
Abstract
We conducted a cross-sectional online survey among 4 chapters of the American Academy of Pediatrics from July through October 2014 to describe characteristics of pediatricians and practices associated with practice-level responses to alternative immunization schedule requests. Among 374 pediatricians, 58% reported frequent alternative immunization schedule requests and 24% reported feeling comfortable using them. Pediatricians who work in practices that accommodate alternative immunization schedule requests have increased odds of having a high frequency of alternative immunization schedule requests, and beliefs that relationships with families would be negatively affected if they refused requests. Practices that discontinue care to families who request alternative immunization schedules have increased odds of being a private group practice and having a formal office vaccine policy. Pediatricians are frequently asked to use alternative immunization schedules and many are not comfortable using them. Practice-level responses to alternative immunization schedules are associated with characteristics of pediatricians and practices.
Introduction
Immunization is considered 1 of the 10 great public health achievements of the 20th century. 1 Despite the proven safety and effectiveness of immunization for reducing morbidity and mortality related to vaccine-preventable diseases,2,3 vaccine hesitancy (delaying or refusing vaccination despite availability of vaccination services), 4 has been increasing in the United States for the past 20 years.5-9 Vaccine-hesitant parents report many reasons for their hesitancy, including concerns over the number of vaccines given per visit and during the first 2 years of life, and vaccine safety, including beliefs that vaccines can cause learning disabilities like autism.10-13 Vaccine-hesitant parents are increasingly requesting alternative immunization schedules that deviate from the Advisory Committee on Immunization Practices (ACIP) recommended schedule, which is endorsed by American Academy of Pediatrics (AAP).8,9,14 Alternative immunization schedules can lead to population-level underimmunization, significantly increasing the individual risk of acquiring and transmitting vaccine-preventable diseases.15-17
Pediatricians are an important factor in parental vaccine decision making and a trusted source of vaccine information.18-20 As requests for alternative immunization schedules increase, pediatricians face the important decision of how to respond to these requests. The AAP discourages pediatricians from dismissing patients from their practices based solely on parental vaccine refusal, but recognizes that there are situations (high levels of distrust, poor communication) in which pediatricians may encourage families to find another pediatrician or practice.21,22 While a few studies have described characteristics of physicians who dismiss vaccine-refusing families from their practice,23,24 currently no studies identify factors that are associated with a range of specific practice-level responses to alternative immunization schedule requests, including accommodating requests and discontinuing care for families who request alternative schedules. Understanding the factors associated with responses to alternative immunization schedule requests can inform the development of strategies to support implementation of immunization policies in practice settings.
The purpose of this study was to examine a sample of pediatricians to determine: (1) individual attitudes about alternative immunization schedule requests, (2) practice-level responses to alternative immunization schedule requests, (3) willingness to delay certain vaccines, and (4) characteristics of pediatricians and practices associated with specific practice-level responses to alternative immunization schedule requests including accommodating requests and discontinuing care to families.
Methods
Survey Administration
The current investigation draws from an original study, which examined the association between state vaccine exemption laws and pediatricians’ comfort using alternative immunization schedules. A purposive sample of 10 state AAP chapters was approached based on varying state vaccine exemption laws and 4 states (Colorado, Delaware, Hawaii, and Pennsylvania) agreed to participate and invited their members to complete the survey. Six other state AAP chapters did not participate in this survey for varying reasons such as participation in another survey on vaccine hesitancy in their chapter. We conducted a cross-sectional, 28-question online survey from July through October 2014 among members of 4 participating AAP chapters. Surveys were pilot-tested and critically reviewed by 12 pediatricians and infectious diseases physicians.
While all members of the Colorado, Delaware, and Hawaii AAP chapters were eligible to participate in the survey, we randomly sampled and invited 50% of the Pennsylvania member list due to the significantly larger membership in this chapter. Overall, 1493 pediatricians comprised the list-based sampling frame. Respondents were given a $5 gift card as a financial incentive to complete the survey and 2 email reminders were sent to encourage participation. We used REDCap (Research Electronic Data Capture) to build and manage the online survey. 25 The institutional review board at The Children’s Hospital of Philadelphia approved this study.
Study Measures
Many of the measures were adapted from a survey instrument developed by Wightman et al. 9 Additionally, the definition of alternative immunization schedules, which was provided to respondents at the start of the survey, was adapted from Wightman et al. 9 and defined as schedules that delay one or more immunizations or not immunizing for reasons other than established medical precautions and contradictions. The recommended immunization schedule was defined for the 6-, 12-, and 15-month ages as follows: at 6 months receipt of vaccines for hepatitis B (1 dose), Haemophilus influenzae type B (Hib) (2 doses), inactivated poliovirus (IPV) (2 doses), rotavirus (2 doses), diphtheria–tetanus toxoids–acellular pertussis (DTaP) (3 doses), and pneumococcal conjugate vaccine (PCV) (3 doses); at 12 months receipt of varicella vaccine (1 dose); and at 15 months receipt of measles-mumps-rubella (MMR) vaccine (1 dose). The birth dose of hepatitis B vaccine was excluded for this study due to varying policies related to administering the birth dose to newborns in the hospital or during the first week well-visit.9,26-29
Dependent Variables
The outcomes of interest were practice-level responses to requests for alternative immunization schedules. Pediatricians were asked, “How does your practice respond to parents who request to delay or refuse a vaccine?” Responses included (1) response depends on family, (2) sign declination form, (3) dismiss family from the practice, (4) parent education, (5) accommodate requests when possible, and/or (6) refer to another practice. Pediatricians were able to choose more than one response to this question because pediatrician’s responses may depend on the circumstances in which alternative immunization schedules are requested (relationship with family, specific vaccines refused or delayed). The main outcome of interest was related to clinical policies that restrict or permit access to health services based on vaccinations status, 30 for which we created 2 dichotomous variables: (1) accommodate or not and (2) discontinue care or not. The accommodate variable includes pediatricians who said that their practice exclusively accommodates all requests for alternative immunization schedules. The discontinue care variable includes pediatricians who said that their practice (1) exclusively refers families to another practice for requesting alternative immunization schedules, (2) exclusively dismisses families for requesting alternative immunization schedules, and (3) uses a combination of dismissal and referral of families to another practice for requesting alternative immunization schedules. We combined responses for dismissal and referral into one variable since both are clinical policies that restrict access to health services at a pediatric practice based on vaccination status.
Independent Variables
The key independent variables for this study were: (1) pediatrician attitudes toward alternative immunization schedule requests and (2) characteristics of practices related to alternative immunization schedule requests. Attitudinal measures included comfort using alternative immunization schedules and perceptions of how using alternative immunization schedules would impact their relationship with families and medical peers, respectively. Based on an instrument from Wightman et al., 9 attitudinal measures were assessed on a 5-point Likert-type scale and dichotomized into agree (strongly agree/agree) versus disagree (neutral/disagree/strongly disagree) for analyses.
Characteristics of practices related to alternative immunization requests included frequency of alternative immunization schedule requests and presence of a formal office vaccine policy. Frequency of alternative immunization requests was measured on a 5-point Likert-type scale and dichotomized into high frequency (always, frequently, or sometimes) or low frequency (rarely or never) for analyses based on an instrument from Wightman et al. 9 To measure presence of office vaccine policy, pediatricians were asked, “Which choice best describes your practice’s approach to having an immunization policy?” Responses included (1) formal written policy distributed to parents; (2) formal policy within practice, but not distributed to parents; (3) no formal policy, but set of shared guidelines; or (4) no formal policy or set of shared guidelines. For analyses, we dichotomized presence of an office vaccine policy into formal office vaccine policy (response options 1 and 2) and no formal office vaccine policy (response options 3 and 4).
Control Variables
Control variables were included in the analyses that represented the organizational context of practices which prior literature have suggested may be associated with responses to alternative immunization schedule requests. Variables included (1) practice setting, 23 (2) patient load, 24 (3) parental educational attainment, 31 and (4) years of pediatric work experience. 24 For analyses, all control variables were dichotomized. Practice setting was dichotomized into private group practice compared to all other types of practice settings (health maintenance organization–based practice, hospital-owned group practice, etc). 23 Pediatrician patient load was measured by the number of patients 2 years or younger seen per week and dichotomized into high patient load (greater than 40 patients 2 years or younger seen per week) compared with lower patient load (fewer than 40 patients 2 years or younger seen per week). Parental educational attainment was measured by the estimated percentage of college-educated parents in the practice and dichotomized into high proportion of college-educated parents (more than 50%) compared lower proportion of college-educated parents (50% or less). Finally, we dichotomized years of experience into working more than 20 years in pediatrics compared to working less than 20 years.
Additional Study Measures
Sociodemographic characteristics of pediatricians were measured, including gender (male, female) and race/ethnicity (white, black, Asian, Hispanic, other). We also measured the variation of the implementation of office vaccine policies across pediatricians within their practice (very consistent, fairly consistent with some variation, great deal of variation, not applicable—work in a solo practice). Attitudes toward the number of immunizations in the recommended ACIP schedule and the willingness of pediatricians to delay certain vaccines were also measured.
Statistical Analysis
Univariate analyses were used to describe sample characteristics and survey responses. We used multivariate logistic regression to test the associations of the outcome variables (practice-level responses to alternative immunization schedule requests) with the key independent variables (pediatrician attitudes toward alternative immunization schedule request and practice characteristics). We tested both bivariate and multivariate models to obtain unadjusted and adjusted odds ratios to examine the relationship between the dependent and key independent variables.
The final two multivariable models controlled for the organizational context of practices and estimated adjusted odds ratios (aORs) for (1) pediatricians who work in practices that accommodate alternative immunization schedule requests and (2) pediatricians who work in practices that discontinue care for families who request alternative immunization schedules. We used backward stepwise elimination procedures in the logistic regression models to eliminate the least significant predictor in the model sequentially. Estimates were checked at each step to ensure that other variables were not affected by dropping the least significant variable. The final 2 models for specific practice-level response to alternative immunization schedule requests resulted in factors that were significant at P < .05. All analyses were conducted in SPSS 22 (IBM Corp, Armonk, NY).
Results
Study Sample
A total of 420 pediatricians responded to the survey (27% response rate). We excluded pediatricians who did not practice in primary care and did not administer vaccines as part of their clinical practice (n = 46), resulting in a final analytic sample of 374 pediatricians.
Pediatrician Attitudes and Practice-Level Responses to Alternative Immunization Schedule Requests
The majority of pediatricians who completed the survey were female (63%), white (77%), worked in a private group practice (41%) and had practiced for more than 20 years (40%) (Table 1). Among the respondents, 43% of pediatricians reported having a formal office vaccine policy and 85% reported that the implementation of an office vaccine policy across providers within their practice was very/fairly consistent (Table 1). Many pediatricians (58%) reported frequent requests for alternative immunization schedules and 61% believed that if they did not agree to use alternative immunization schedules it would negatively impact their relationship with families (Table 2). Almost all respondents were supportive of immunizations and the ACIP-recommended immunization schedule—only 4% of pediatricians strongly agreed/agreed that there are too many immunizations given at one visit and only 2% agreed that there are too many immunizations overall (Table 2).
Characteristics of Participating Pediatricians and Practice Characteristics (N = 374). a
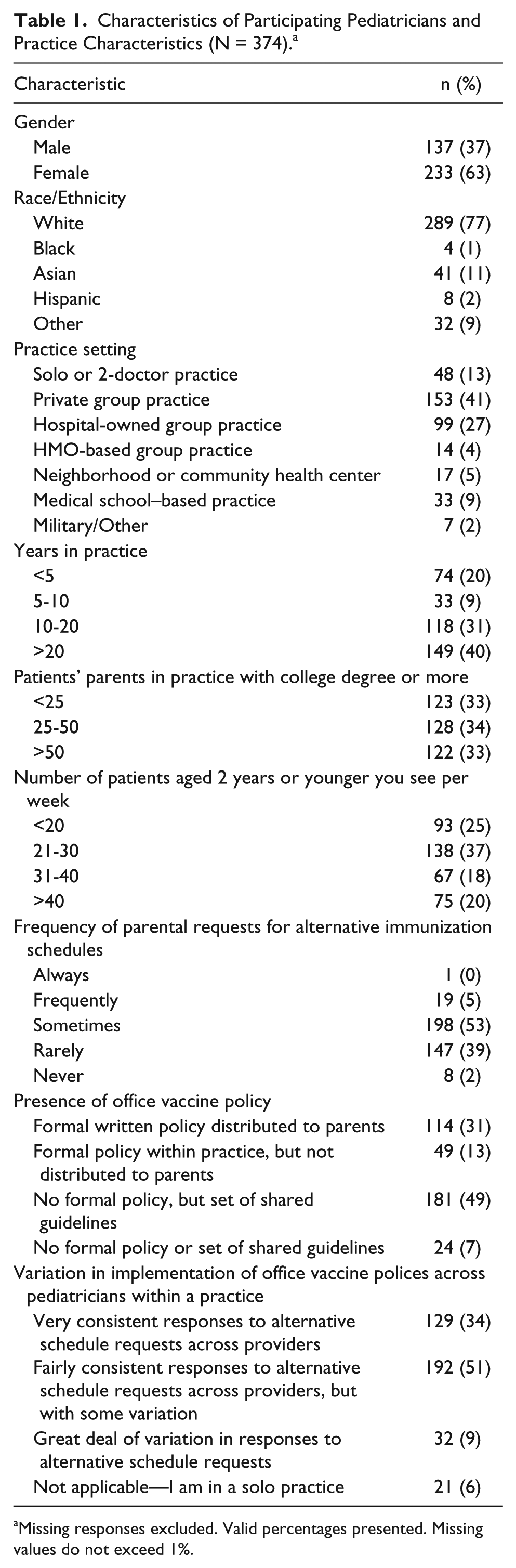
Missing responses excluded. Valid percentages presented. Missing values do not exceed 1%.
Practice-Level Responses and Pediatricians’ Attitudes to Alternative Immunization Schedule Requests (N = 374). a
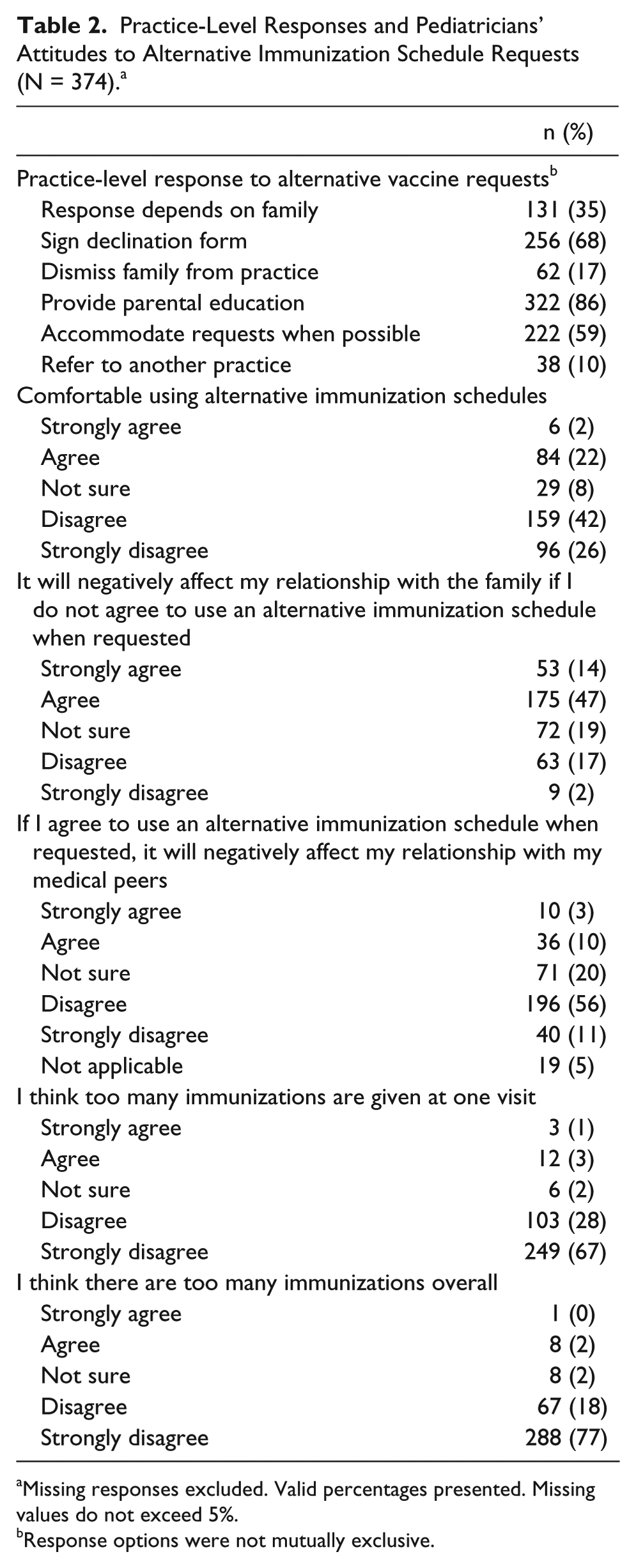
Missing responses excluded. Valid percentages presented. Missing values do not exceed 5%.
Response options were not mutually exclusive.
Among pediatricians in this sample, 24% reported feeling comfortable using alternative immunization schedules. However, when pediatricians were asked to report practice-level responses to alternative immunization requests, 51% of pediatricians reported exclusively accommodating requests while 8% reported exclusively dismissing families and 2% reported that they exclusively refer families to another practice. Additionally, 2% of pediatricians reported both dismissing and referring as a response to alternative immunization schedules requests. In response to alternative immunization schedule requests, the majority of pediatricians provide education to vaccine hesitant parents (86%), and document delays or refusals by having parents sign a declination form (68%), while 35% of respondents stated that their response was dependent on the family.
Willingness to Delay Vaccines
Pediatricians were more willing to consider using alternative immunization schedules for hepatitis B vaccine, rotavirus vaccine, and varicella vaccine compared to DTaP, Hib vaccine, and PCV (Table 3). The 3 vaccines that pediatricians were the most comfortable delaying for more than 4 months were hepatitis B vaccine, IPV, and varicella vaccine. In contrast, the 3 vaccines that pediatricians were least comfortable delaying for more than 4 months were Hib vaccine, DTaP vaccine, and PCV.
Pediatrician Willingness to Consider Alternative Immunization Schedules and Length of Time Comfortably Delaying by Specific Vaccine (N = 374). a
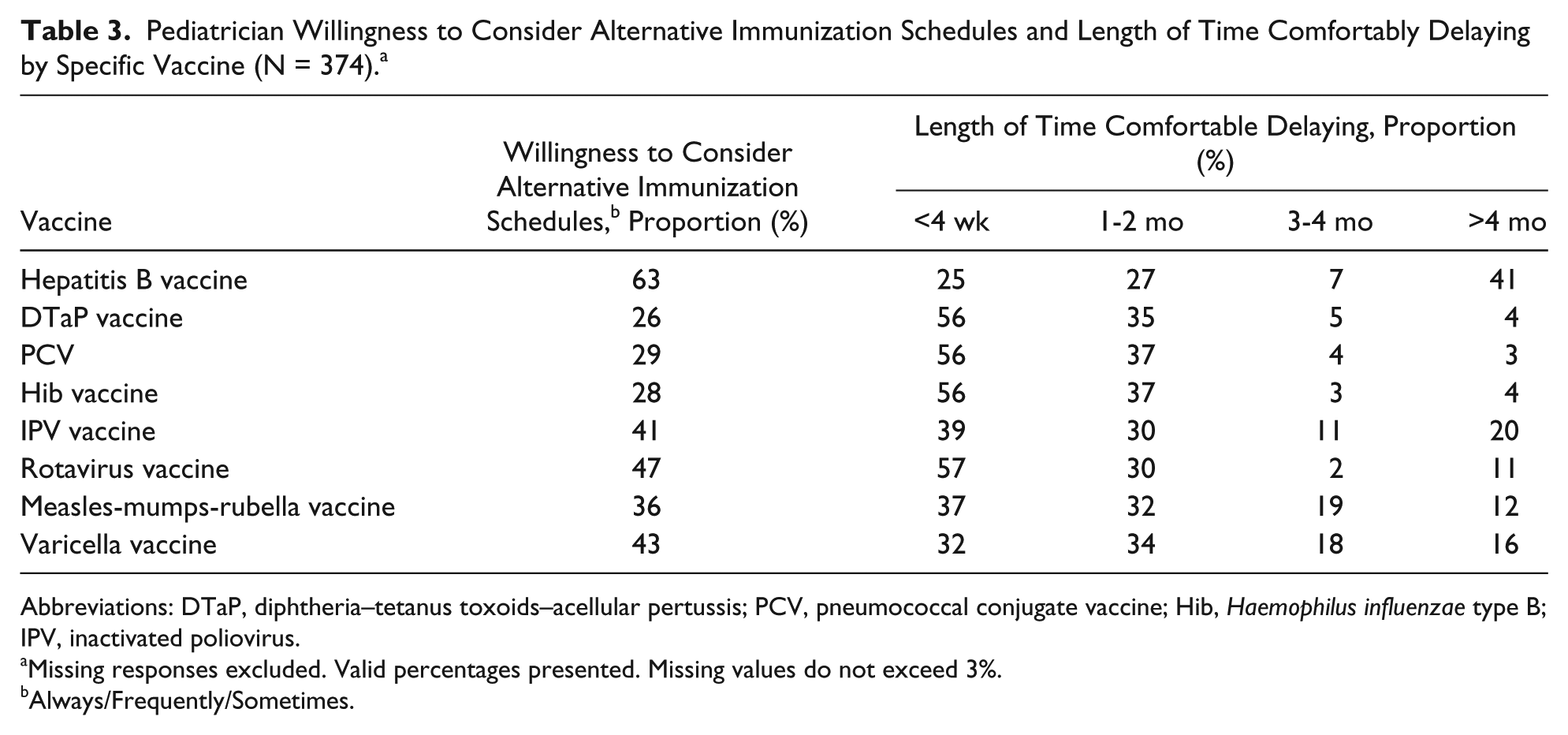
Abbreviations: DTaP, diphtheria–tetanus toxoids–acellular pertussis; PCV, pneumococcal conjugate vaccine; Hib, Haemophilus influenzae type B; IPV, inactivated poliovirus.
Missing responses excluded. Valid percentages presented. Missing values do not exceed 3%.
Always/Frequently/Sometimes.
Factors Associated With Practice-Level Responses to Accommodate or Dismiss/Refer
Table 4 shows the unadjusted and adjusted odds ratios that estimate two practice-level responses to alternative immunization schedule requests: accommodate and discontinue care. After adjustment, believing that refusing alternative immunization requests would negatively affect the relationship with families (aOR 2.02, 95% CI 1.27-3.20), and working in a practice with a high frequency of requests for alternative immunization schedule requests (aOR 1.69, 95% CI 1.07-2.68) was significantly associated with greater odds of accommodating alternative immunization schedule requests. After adjustment, believing that refusing alternative immunization requests would negatively impact the relationship with medical peers (aOR 0.42, 95% CI 0.21-0.83) and having a formal office vaccine policy (aOR 0.40, 95% CI 0.25-0.63) was significantly associated with lower odds of accommodating alternative immunization schedule requests.
Characteristics of Pediatricians and Practices Associated With Practice-Level Responses to Accommodate or Dismiss/Refer Families for Requesting Alternative Immunization Schedules (N = 346).
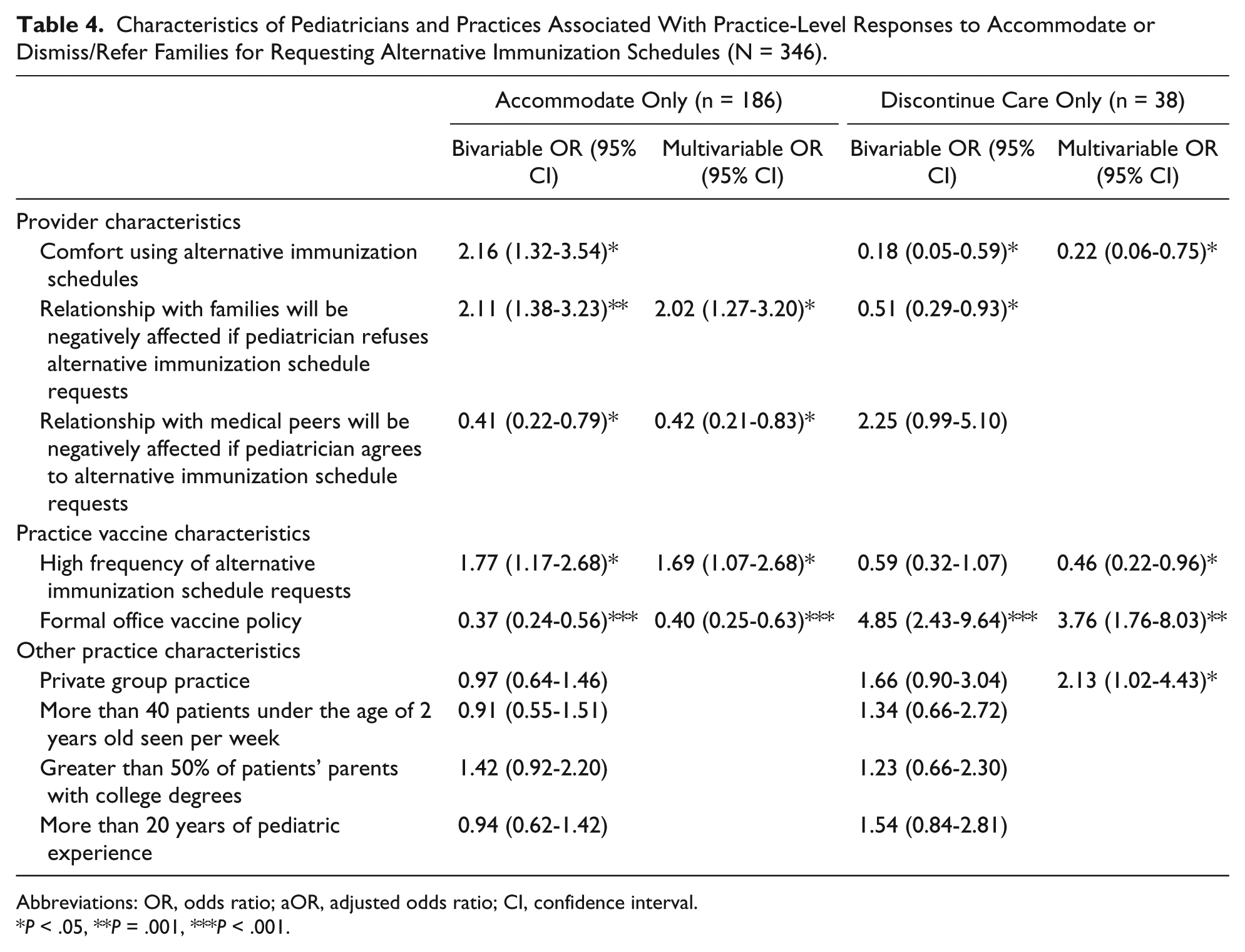
Abbreviations: OR, odds ratio; aOR, adjusted odds ratio; CI, confidence interval.
P < .05, **P = .001, ***P < .001.
In contrast, after adjustment, feeling comfortable using alternative immunization schedules (aOR 0.22, 95% CI 0.06-0.75) and working in a practice with a high frequency of alternative immunization schedule requests (aOR 0.46, 95% CI 0.22-0.96) were significantly associated with lower odds of discontinuing care. Working in a private group practice (aOR 2.13, 95% CI 1.02-4.43) and having a formal office vaccine policy (aOR 3.76, 95% CI 1.76-8.03) was associated with greater odds of discontinuing care. While high frequency of alternative immunization schedule requests was not significant in the bivariate analysis, it became significantly associated with lower odds of discontinuing care in the multivariable model. Similarly, working in a private group practice was not significant in the bivariate analysis, but it became significantly associated with greater odds of discontinuing care in the multivariable model.
Discussion
This is the first study to examine the range of pediatricians’ responses to requests for alternative immunization schedules as they relate to existing practice policies around continued access to care. We found that pediatricians are frequently asked to use alternative immunization schedules and that the factors which impact their decision to accommodate, refer or dismiss families for requesting alternative immunization schedules are complex. Many pediatricians do not feel comfortable using alternative immunization schedules but despite this, we found that the majority of pediatricians will accommodate such requests and believe that not agreeing to an alternative schedule will negatively impact their relationships with families. Our results align with a recent study among a nationally representative sample of pediatricians and family physicians which found that while physicians may not support alternative immunization schedules they agree to requests because they believe it will build trust with families and believe that if they do not agree to these schedules that families would leave their practice. 32 About one-third of our sample (35%) reported that their response to alternative immunization schedules depended on the family, which suggests that pediatricians tailor their responses based on the situation or relationship with the family. Furthermore, our finding that pediatricians were willing to delay certain vaccines over others also points to their willingness to compromise with parents who request alternative immunization schedules. This study suggests that pediatricians, despite feeling uncomfortable, will use alternative immunization schedules to maintain relationships with families.
Our results show that certain characteristics of pediatricians and their practices are associated with both accommodating and discontinuing care. Practices that discontinue care for families who request alternative immunization schedule requests had greater odds of having a formal office vaccine policy while practices that accommodate alternative immunization schedule requests had lower odds of having a formal office vaccine policy. Additionally, we found that the majority of pediatricians reported that the implementation of an office vaccine policy across providers within their practice was very/fairly consistent suggesting that pediatricians within a practice generally respond to alternative immunization schedule requests in the same way. This also suggests that formal office vaccine policies may be an important factor related to how pediatricians respond to alternative immunization schedule requests.
We found that among our sample, working in a private group practice was associated with increased odds of discontinuing care for families who request alternative immunization schedules. This is similar to a recent study by O’Leary et al. 23 that found that physicians in private practices were more likely to dismiss families than physicians who practiced in a community, hospital-based or health maintenance organization–based practices. Among our survey respondents, we found that there was no significant association between pediatricians who worked more than 20 years and odds of dismissal/referral or accommodation. Similarly, a nationwide survey among a sample of AAP members, found that there was no significant association between pediatricians’ years of experience and odds of dismissal. 24
Since our study adapted questions from Wightman et al., 9 we had the opportunity to compare our results from Wightman’s sample of primary care pediatricians from Washington State to other regions of the country. Our results indicate both consistencies and differences between our sample and Wightman’s sample concerning attitudes and willingness to consider alternative immunization schedules for certain vaccines across difference samples of pediatricians. For example, in both studies, pediatricians were least willing to consider delaying the DTaP vaccine, Hib vaccine, and PCV. This suggests that pediatricians prioritize vaccines that protect against diseases that are still common or that are more likely to have severe sequelae. 9 In contrast, Washington pediatricians were more comfortable using alternative immunization schedules (61%) compared to our study sample (24%). Furthermore, Washington pediatricians had higher frequencies of alternative vaccine requests (77%) compared with this study’s sample (58%). Washington state has 1 of the 10 highest rates of unvaccinated children aged 19 to 35 months in the United States. 31 Therefore our results compared with prior work may be indicative of the regional and temporal variation in attitudes and practices concerning alternative immunization schedules.
This study has several limitations. Due to the cross-sectional nature of this study, we could not establish any causal relationships. Therefore it was unclear whether pediatricians who accommodate alternative immunization requests were more comfortable using these schedules because they believed that alternative immunization schedules are as effective as the recommended schedule or because these requests have become routine. However, because these results indicate that the vast majority of pediatricians in our sample are supportive of the ACIP recommended schedule, it is possible that their comfort with these requests may be related to the frequency of requests they receive. A previous multistate survey of healthcare providers showed that those who held unfavorable opinions related to vaccines (less confidence in vaccine safety and benefits to individual and community) had a greater likelihood of having unvaccinated children in their practice.33,34 This may suggest that parents choose healthcare providers with vaccine beliefs that align with their own. Similarly, it is unclear whether practices that discontinue care to families who request alternative immunization schedules have a lower frequency of requests because they have a formal office vaccine policy, which may be communicated to parents within their community. Future studies should explore the direction of these relationships.
The sampling methodology and low response rate may limit the generalization of these findings. Since this was a convenience sample, data may not be representative of all AAP chapter members within sampled states or among pediatricians in the United States. Additionally, there was potential for nonresponse bias due to sampling since we were unable to measure whether respondents differed in a meaningful way from non-respondents, which may also limit the generalizablity of this study. However, literature suggests that nonresponse bias may not be as critical in surveys of physicians compared to the general population. 35 Despite these limitations, this is the first study that describes characteristics of pediatricians and practices associated with accommodating alternative immunization schedule requests and adds to the limited literature characterizing pediatricians and practices based on dismissal policies related to alternative immunization schedule requests.
This study is unique as it examines specific practice-level responses to requests for alternative immunization schedules, including the decision to accommodate requests and discontinuing care to families who request alternative immunization schedules while previous studies have only focused on pediatricians’ individual responses to such requests or dismissing families for refusing all vaccines. Understanding how pediatricians respond to alternative immunization schedule requests is complex and in order to gain a better understand of this complexity future studies should explore the multiple factors that may impact their responses, such as characteristics of patients and parents (socioeconomic status, family history of autism, etc), as well as those of pediatric practices (practice location, financial stability of practice, etc).
Our results show that pediatricians and practices respond to alternative immunization schedule requests in many different ways including accommodating requests, referring to another practice or dismissing families, and that both pediatrician and practice characteristics are associated with these responses. The results of this study have the potential to inform strategies to increase adherence to the ACIP recommended immunization schedule including creation of formal office vaccine policies, which can support pediatricians’ communication with families.
Author Contributions
All authors participated in the study design, data synthesis and analysis, and interpretation of the results. SM drafted the manuscript. All authors reviewed and edited the manuscript and approved the final version.
Footnotes
Acknowledgements
We gratefully acknowledge the American Academy of Pediatrics, including the Executive Directors of the Colorado, Delaware, Hawaii, and Pennsylvania state chapters and their members who participated in this survey. We also thank the Vaccine Education Center at the Children’s Hospital of Philadelphia. Lastly, we acknowledge the following individuals for thier support and guidance: Caitlin Fasano, Kathleen Noonan, Dr Michael Yudell, Dr Renee Turchi and Dr Paul Offit.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.