
Abstract

Background
Ophthalmologic concerns are common in the pediatric primary or urgent care setting, with more than 70 000 children treated annually in emergency departments in the United States. 1 Complaints can range from allergic conjunctivitis to a foreign body to infection. Of these, corneal ulcers, also known as ulcerative keratitis, carry the potential for long-term morbidity and loss of visual acuity due to scarring and associated inflammatory effects. A full evaluation for corneal ulcers requires the input of an ophthalmologist to determine the depth and extension of the corneal erosion, as well as obtaining cultures to help guide therapy. In the pediatric population, the greatest risk factor has become contact lens usage2 -4; with the most common bacterial pathogens encompassing Staphyloccoccal species and Pseudomonas.3 -6 Other less common infectious etiologies include viruses, such as herpes simplex virus (HSV) in infants, fungal (Fusarium species), or even protozoan (Acanthamoeba). Once the eye and corneal defects have been defined, treatment with fortified antibiotic, antiviral, or antifungal eye drops should be promptly started to prevent further corneal erosion and damage. Here we review a case of a 5-month-old boy who presented with bilateral swollen eyelids and drainage, a relatively common presentation. As his hospital course progressed, new insights were made requiring further evaluation and discussion of additional diagnostic possibilities.
Case Report
A 5-month-old boy presented to the emergency department with his mother after a week of progressive eyelid swelling and drainage. His mother first noticed a change in the shape of his eyes 7 days prior, for which he was brought to an emergency department on day 3 of illness for bilateral purulent eye drainage. There he was diagnosed with conjunctivitis and started on tobramycin eye drops. The swelling worsened despite reported compliance with treatment. When he did not open his eyes for 2 days, his mother brought him to another emergency room for a second opinion. Prior to this he was a previously healthy infant born full term via Cesarean-section for nonreassuring fetal heart tones to an 18-year-old woman. His mother had a distant history of a treated Chlamydia infection, but no other reported sexually transmitted infections. There was also a maternal history of bipolar disorder and depression per chart review. The mother was the patient’s main caregiver with occasional assistance of the maternal grandparents.
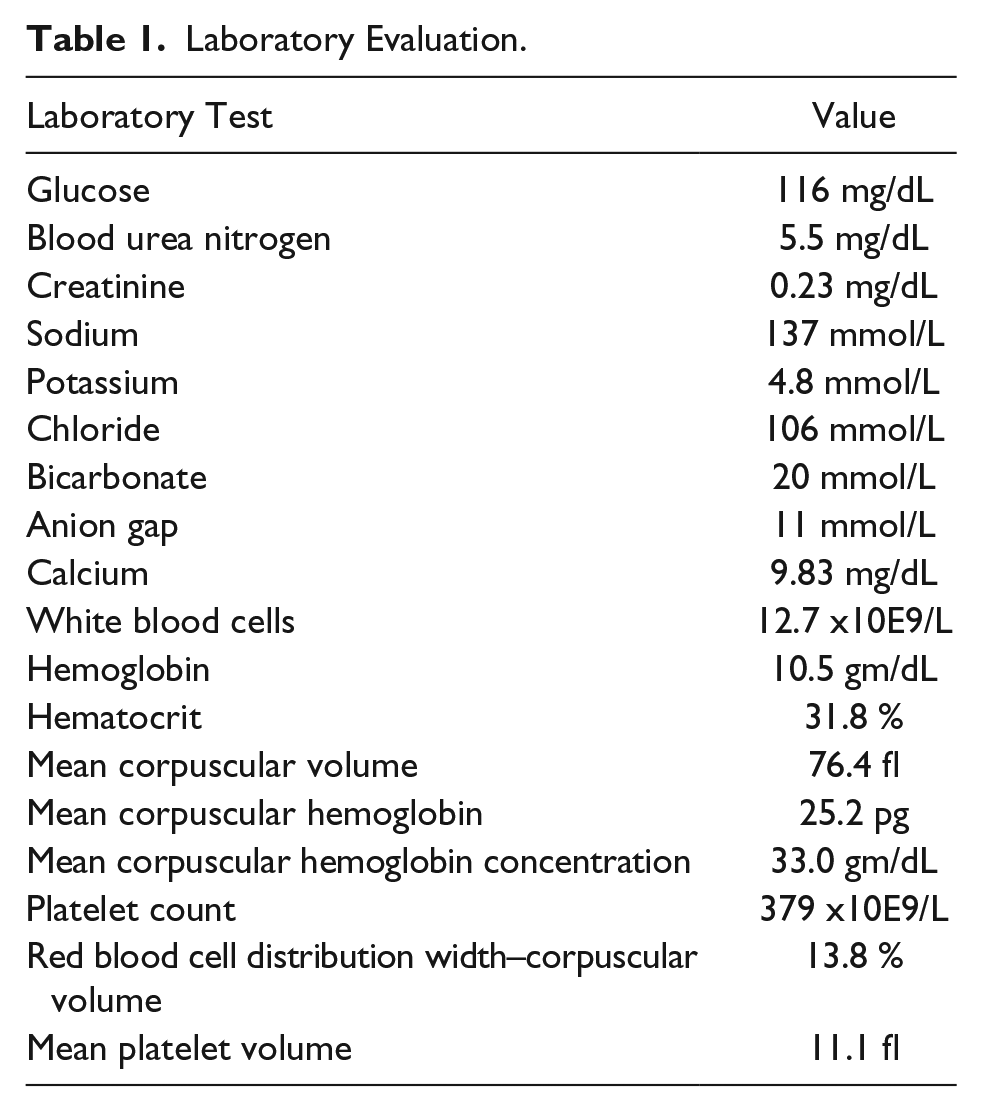
At presentation, he was afebrile, with bilateral periorbital edema, right worse than left, and purulent drainage from both eyes. A complete blood count and basic metabolic panel were sent, with the results contained in Table 1. A computed tomography scan of the sinuses and orbits was done with intravenous contrast, which showed preseptal cellulitis of the right eye and air in the anterior chamber of the right globe concerning for a corneal ulcer (Figure 1). Given these findings, he was started on clindamycin (40 mg/kg/d) and ophthalmology was consulted. Because of periorbital edema, his examination was limited despite use of an eyelid speculum, but he had fluoroscein uptake consistent with bilateral large corneal ulcers. Bacterial and fungal cultures were sent from both eyes, and he was started on fortified vancomycin (25 mg/mL) and fortified tobramycin (15 mg/mL) eye drops every hour. There was no reported history of trauma or mechanism of injury, so it was assumed on admission that this was due to unintentional self-injury from his fingernails.
Laboratory Evaluation.
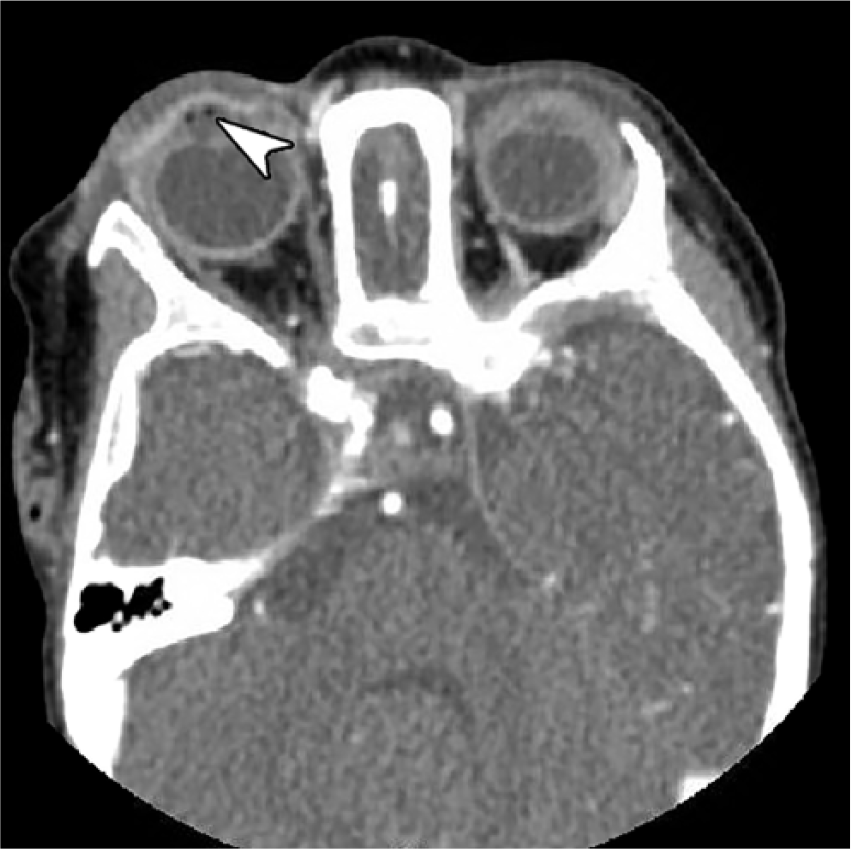
Computed tomography scan of the sinuses and orbits with intravenous contrast showing air in the anterior chamber of the right chamber (white arrowhead), concerning for a corneal ulceration.
On the second day, his eyelid edema had improved, and repeat examination by ophthalmology was notable for large epithelial defects over the inferior 40% of the bilateral corneas, without evidence of mucoid drainage and no corneal clouding. No dendrites were observed. Because of the nature of the injury, ophthalmology relayed concerns that chemical exposure was a primary consideration. Antibiotic eye drops were spaced to every 3 hours. Further history was obtained regarding potential chemical exposure, and no instances were reported, nor any other mechanisms to explain pattern of injury. Because of concerns for abuse, social work and child protection were consulted, and a skeletal survey was obtained, which was negative. As there were inconsistencies in the time course of events provided by his mother to social work and child protection, the decision was made to notify child protective series. On hospital day 2, the examination was significantly improved, with the corneal defects only 15% to 20% of the inferior aspect of the corneas. The palpebral conjunctiva of the inferior lids continued to have changes consistent with a chemical exposure. The corneal defect resolved the next day, and the infant was discharged home to complete a 7-day course of clindamycin and with vancomycin and tobramycin eye drops every 6 hours until his follow up with ophthalmology. One eye culture eventually grew Staphylococcus epidermidis, while all other cultures remained negative. Follow-up visit with ophthalmology demonstrated no residual defect and normal visual acuity on induced tropia test.
Discussion
In retrospect, there were many warning signs that this was an unusual presentation of ulcerative keratitis. Both of the infant’s eyes were affected, raising concerns for an exposure at birth, such as HSV, although the patient being born via C-section makes this significantly less likely. 7 The purulent drainage raises concerns for chlamydial ophthalmicus neonatorum, which is also a diagnostic consideration in an infant under a year, but this would be a delayed presentation. 3 The most common cause of ulcerative keratitis in the industrialized world is contact lens use,2 -4 which would not be present in an infant this young. The next most common cause would be trauma.4,5 A 1999 study of pediatric ulcerative keratitis in India with a relatively young patient population (mean age of 4.8 years), none of whom wore contact lenses, found that while trauma was the most common etiology, systemic illness and preexisting eye disease were also significant risk factors. 5 None of these factors were present in our patient. Fungal causes are worth considering in patients with subacute onset of symptoms, but these are significantly less common than bacterial or viral etiologies, and only encompass 5% to 10% of corneal infections in the United States. 8 A 2006 study in India comparing corneal ulcers among 3 different age groups, found that the pediatric population (defined as age 16 years or younger) had a significantly lower rate of fungal infections compared with the control (18-64 year old patients) and geriatric (65 and older) groups. 9
Ocular trauma is a broad term that encompasses many potential etiologies. Blunt trauma or retained foreign bodies may be apparent from the history, but in older patients, enquiring about occupational or hobby exposures can assist with the diagnosis. Any tasks relating to manufacturing or construction raises the possibility for debris to come in contact with the eye, especially if the patient was not wearing protective eyewear. Young men in particular have the highest incidence of occupational eye injury, thought to be due to a disregard for safety measures. 2 Such instances require an examination of the upper eyelids via eversion to evaluate for a foreign body, in addition to fluorescein staining. In a child that is not ambulatory, trauma is a dubious explanation though.
Chemical trauma is another important consideration, and could be due to sprays or splashes, delivered intentionally or unintentionally. In this patient, the presumed cause was an aerosolized agent that was able to make contact with the eyes and cause the corneal erosion. There are many agents in the typical household capable of such an injury, from cleaning substances to insect repellant to perfumes and cologne. Such injuries typically resolve over the course of a few days, but steps must be taken to ensure that secondary infection does not occur and that the injury has time to heal.
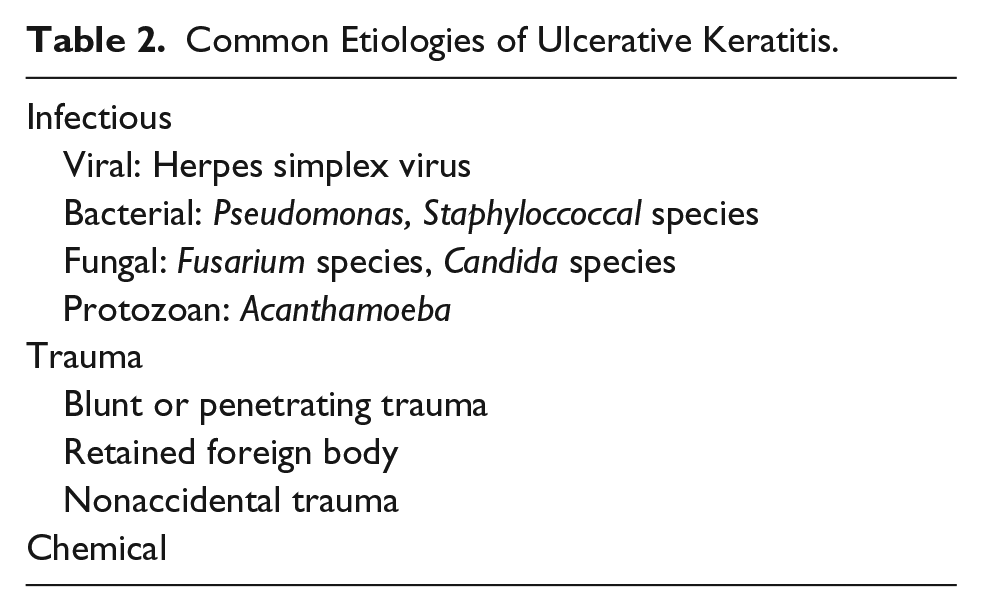
Until ocular culture results are available, standard treatment involves either monotherapy with fluoroquinolone eye drops,2,8 or combined therapy with a fortified aminoglycoside and a fortified cephalosporin.3,6 Therapy in the first 48 hours is frequent, initially occurring every 15 to 30 minutes, and then every hour for the first day or two, before being spaced out further. HSV keratitis is best treated with topical antivirals such as trifluridine or ganciclovir gel, although oral solutions of acyclovir can be used in children to ensure compliance.6,8 An antibiotic drop is typically included as well to ensure no bacterial superinfection. 8 Fungal ulcers are treated with topical natamycin 5% initially, followed by topical amphoteracin B or systemic therapy if there is a poor response or concerns for invasion beyond the anterior chamber of the eye. 8 Causes of corneal ulcers are summarized in Table 2.
Common Etiologies of Ulcerative Keratitis.
This case highlights a number of aspects in the care of infants presenting with ocular symptoms concerning for ulcerative keratitis. A careful history, including birth, occupational, and chemical exposures can not only assist in the diagnosis but also aid in guiding treatment. The involvement of an ophthalmologist is vital to ensure accurate interpretation of fluoroscein results and for recommendations on treatment and further studies. When there are atypical findings, such as bilateral symptoms in an otherwise healthy and immobile infant, further diagnostic possibilities should be considered, such as inadvertent or intentional chemical exposures or abuse. While this infant ultimately did well and the precise etiology of his symptoms remains unknown, early treatment and recognition is crucial to preserve vision.
Author Contributions
Both authors contributed equally to the research and writing of this brief report.
Footnotes
Acknowledgements
The authors would like to thank the patient’s family for allowing us to use their child’s presentation for this brief report.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.