
Abstract
Publicly insured adolescents and young adults experience significant obstacles in accessing primary care services. As a result, they often present to their medical appointments with multiple unmet needs, adding time and complexity to the visit. The goal of this project was to optimize team work and access to primary care services among publicly insured adolescents and young adults attending an urban primary care clinic, using a previsit screening checklist to identify patient needs and delegate tasks within a care team to coordinate access to health services at the time of the visit. We conducted an interventional quality improvement initiative in a PDSA (Plan-Do-Study-Act) cycle format; 291 patients, 13 to 25 years old were included in the study over an 8-months period. The majority of patients were receptive to the previsit screening checklist; 85% of services requested were provided; nonclinician staff felt more involved in patient care; and providers’ satisfaction increased.
Introduction
Our primary care practice is located in a low-income neighborhood of Boston, and despite convenient location and multidisciplinary services offered, the patient no show rate among our adolescent and young adult age group averages 30%. We find a trend for risky health behavior in this age group, with high rates of sexually transmitted diseases, unplanned pregnancies, and numerous psychosocial stressors in addition to significant comorbid or complex medical diagnoses. As a result, patients frequently present with multiple unmet medical needs than it is ideal to address in the span of a 15- to 30-minutes visit.
With the emergence of puberty, adolescents experience greater autonomy in decision making but at the same time are far more vulnerable to negative influences.1,2 This provides a unique opportunity for health care providers to address and/or reduce risky health behaviors that could otherwise significantly affect their future health outcomes. Guidelines on what should constitute adolescent-specific preventive health services have been established, and provisions in the 2010 Patient Protection and Affordable Care Act (ACA) have been put in place to facilitate access to care for adolescents and young adults.2-4 Despite these measures, disparities in access to preventive services remain among youths. Publicly insured adolescents and young adult patients experience greater obstacles in accessing primary care services partly because of financial and housing insecurity, reliance on public transportation, language barriers, and low educational attainment among their parents.5-8
Thus, timely access to preventive care is of particular importance for low-income adolescents and young adults. Yet primary care practices face challenges in providing timely access because of an imbalance between increase in demands and capacity to provide services.2,9
There is growing evidence that interdisciplinary teamwork, through structured communication and delegation of nonclinical tasks, optimizes workflow, health care delivery, and patient outcomes. Many practices have adopted this model of shared care by expanding the role of administrative staff, medical assistants, and nursing staff.9,10 One of the most successful and well-known examples of this model in health care is the Surgical Safety Checklist. A simple 19-item checklist that has been used in surgical settings demonstrates an increase in teamwork performance and a decrease in morbidity and mortality rate from surgical complications.11-13
To address some of our challenges around workflow and delivery of health services, we hypothesized that the use of a previsit screening checklist in a primary care setting could help a care team anticipate patient needs for services and proactively coordinate access to requested services at the time of the visit. It would enable identification of patient needs prior to the medical encounter and trigger communication within the care team around services requested and delegation of tasks to facilitate access to these services.
We adopted the following aims: (1) promote teamwork during a medical visit through delegation of tasks among care team members and (2) provide same-day access to existing medical services.
Methods
Setting
The setting is a primary care pediatrics and adolescents practice owned by a children’s hospital, located in a low-income urban neighborhood of Boston. It serves children, adolescents, and young adults through age 25 years. With 77% of its total population self-identified as Hispanic, the majority of patients are first- or second-generation immigrants of Latino descent. Most are of low-income families, with an income level below the poverty line, and about 74% qualify for Medicaid (Table 1). 14 Since 2013, this practice has engaged in an academic learning collaborative toward a patient-centered medical home transformation, to deliver efficient, high-quality preventive and acute health care to all primary care patients through care teams. 15 The practice has been divided into 2 teams: 1 focused on pediatric care and the other on adolescent care. Each team includes medical providers, nurses, social workers, clinical and administrative assistants, and a nutritionist. Previsit huddles, PDSA (Plan-Do-Study-Act) cycles focusing on workflow, regular care team meetings as well as patients’ and parents’ advisory boards have been key components of this transformation process.16-18
Sample Characteristics. a
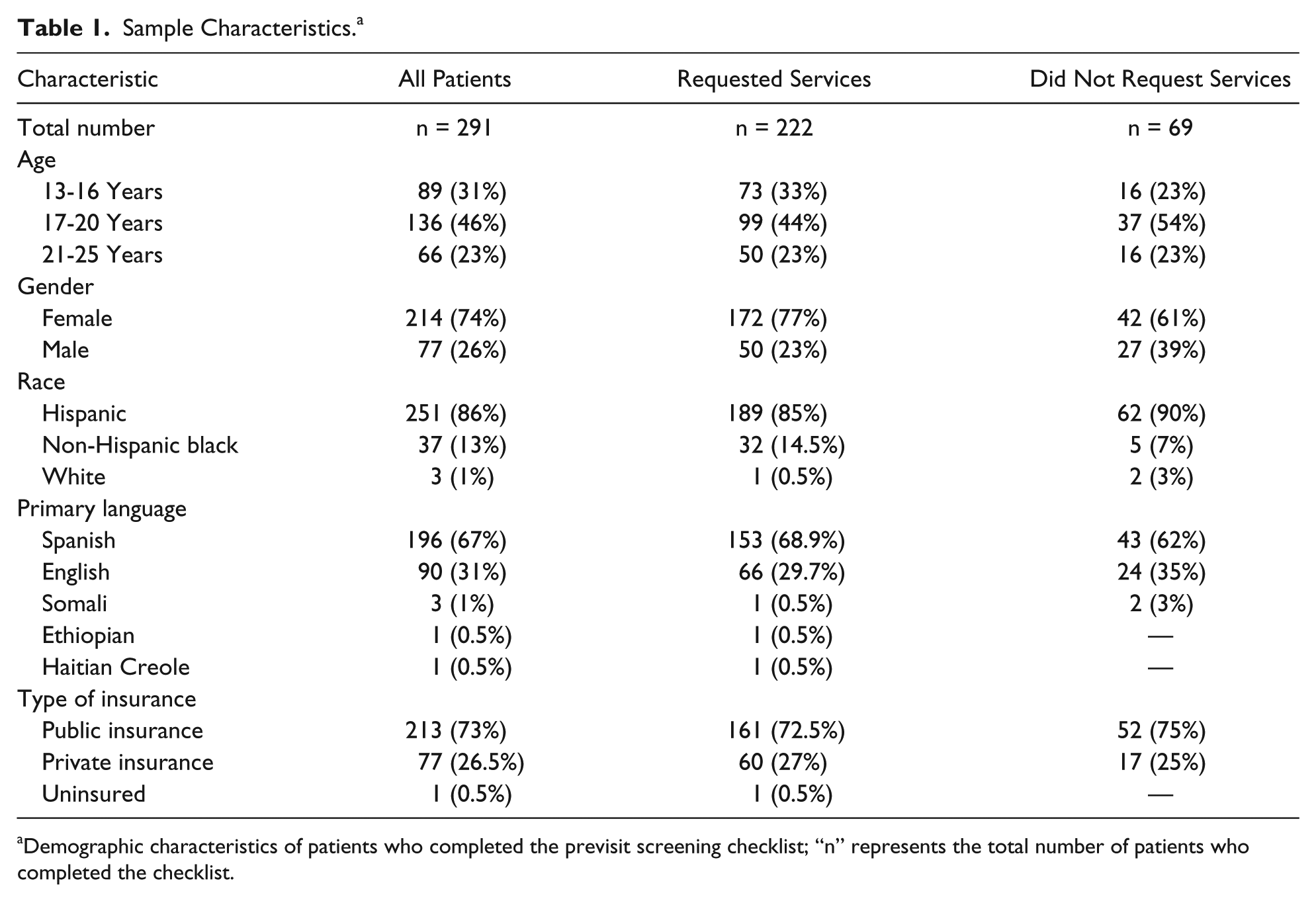
Demographic characteristics of patients who completed the previsit screening checklist; “n” represents the total number of patients who completed the checklist.
Intervention
Description of the Intervention
We created a brief self-administered previsit screening checklist, available in both English and Spanish (Figure 1). It includes 11 questions in a “yes/no” answer format, covering the following areas: nutrition, reproductive health, and social and nursing services (ie, health form completion, prescriptions refills). The checklist is completed by the patient privately during a standard screening process that takes place prior to the medical encounter and is returned to the clinical assistant (CA). The CA reviews patient requests for services and, after a coordinated discussion with the other team members, contacts the appropriate support service.
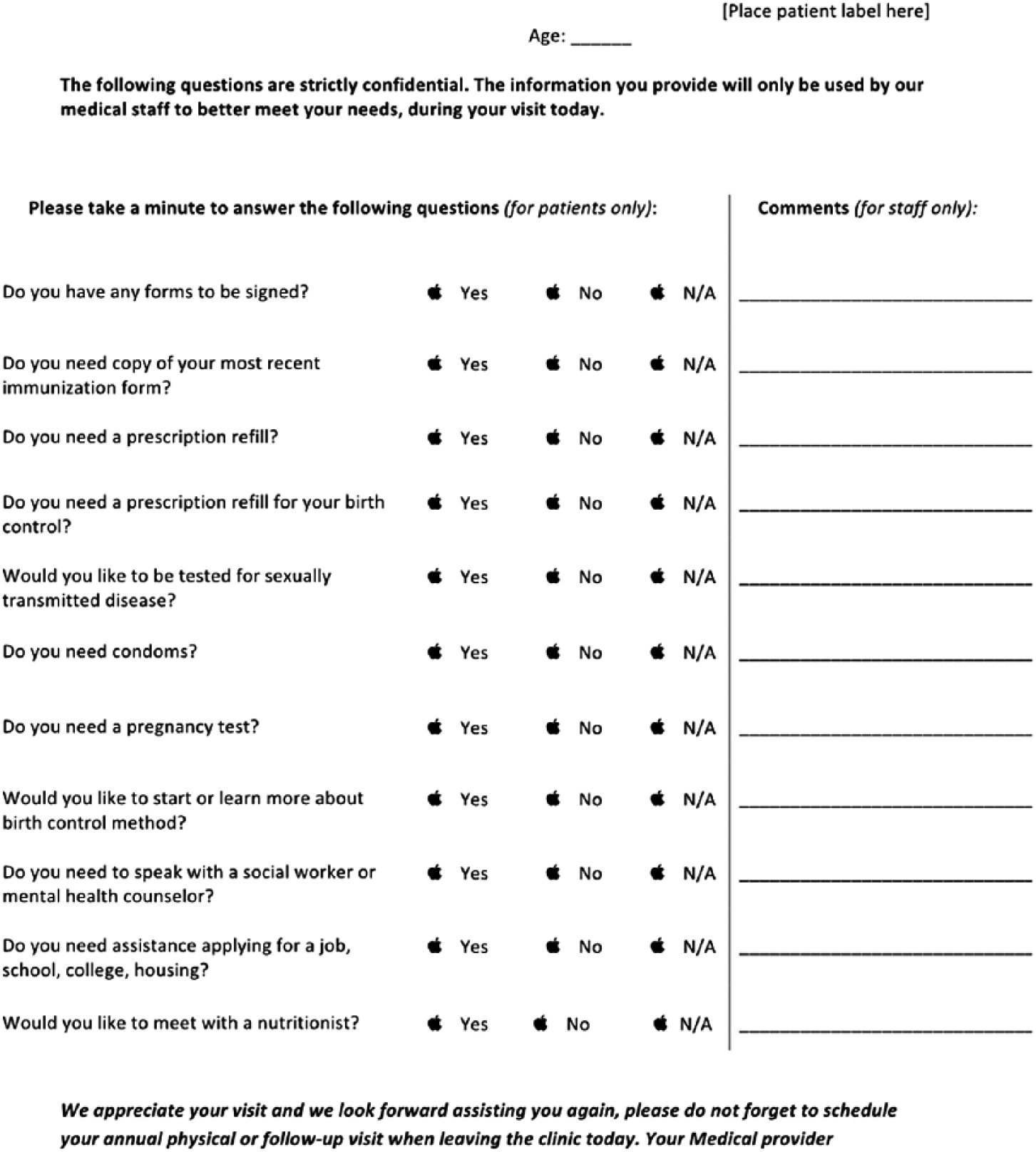
The previsit screening checklist: The figure represents the actual previsit screening checklist in its English version. It includes an 11-item checklist in “yes/no” or “N/A” (not applicable) format to identify patient needs (left-hand side) and a staff communication column (right-hand side).
Improvement Team
Our multidisciplinary project team included the following: 1 physician project leader, 1 adolescent nurse practitioner, 2 registered nurses, 1 CA, and 1 clinical research assistant.
Study of the Intervention
The previsit screening checklist was created with input of the improvement team based on most frequently requested services; questions were refined with input of the advisory boards. We conducted 3 independent key-informant semistructured interviews of our Parent and Youth Advisory Boards (YABs) as well as medical staff (nurses, CAs, and providers) to assess needs and acceptance of the checklist prior to conducting our intervention. Quantitative and qualitative approaches through iterative PDSA cycles were used to evaluate the intervention. Our improvement team met regularly during this process and provided feedback related to the use of the previsit screening checklist.
Measures
In addition to project team feedback, specific measures were used to evaluate our intervention.
Process measure was defined by the number of unique patients who completed the previsit screening checklist during an adolescent and young adult health visit.
Outcome measure was defined by the number of requests per unique patient provided with same-day access to a service, as identified on the previsit screening checklist. This measure reflected that a certain degree of communication did occur among support staff to coordinate requests and provide access to services. Staff were invited to communicate verbally or in writing about the action taken on each service requested on the checklist.
Analysis
Completed previsit screening checklists and patient medical records review were used to determine access to services. Basic quantitative data analysis was applied to identify frequencies of requested services and trend in the population sample.
Ethics
This study was approved as a quality improvement initiative by our department and was, thus, exempted from review by the institutional review board. All data collected were anonymously stored and used for our process evaluation.
Results
Phase 1: Key Informants’ Semistructured Interviews
Members of our YAB provided feedback on the previsit screening checklist content and whether or not it met their needs. They believed that it read well, questions were clear, and it covered the topics most useful to youth. They felt that the checklist was helpful in reminding teens to ask the doctor questions, encouraging shy or embarrassed patients to bring up uncomfortable topics, and informing youth about the services available in the clinic. They also stressed the importance of keeping this previsit screening process confidential from parents, stating that “youth would not be as honest and may not request for services that they need if they were to complete the checklist in presence of their parent.” YAB members reported that teens do not receive enough information about reproductive health outside of the medical setting, stating that “sexual education is not mandatory in their schools.” Consequently, the majority of YAB members felt that “teens should be given the opportunity to discuss reproductive health issues at every visit” and the previsit screening checklist would support that as well.
Members of our Parent Advisory Board (PAB) provided feedback on the previsit screening checklist, expressing strong reservations in regard to the reproductive health questions. PAB members were divided about these questions. About half of them viewed the checklist as “dangerous,” expressing that youth already received enough information regarding sexual health from schools and felt that addressing this again with a doctor would result in “information overload” and may lead youth to believe that engaging in sexual activity is “the norm.” They were also concerned about the appropriateness of the reproductive health questions for youth younger than 15 years and felt more comfortable with male patients being offered the checklist rather than female patients. About half of the PAB members thought that adolescents were often uncomfortable expressing their reproductive health needs and that the previsit screening checklist would facilitate access to these services. These parents stated that “teens will do what they want anyway and this information should therefore be made available to them” and that adolescent confidentiality must be maintained for this process to work.
Staff interviews revealed a positive perception of the previsit screening checklist and high acceptance as a useful tool to support coordination of health services. They felt that questions were easy to read, adequately covering key services provided in our clinic, emphasizing the need for such a tool to bring the desired services to “the top of youth’s minds” and to “let the patients know what is available.”
Phase 2: Planned Intervention
We evaluated whether this checklist supported care team collaboration to provide timely access to services. Over the 8-month study period, a total of 291 unique patients 13 to 25years old, received the previsit screening checklist during an adolescent well visit, and 76% (n = 222) requested services (Table 1). The majority of the patients requesting services were female patients (214) in contrast to 77 male patients (Table 1). Patients were allowed to request more than 1 service per form. A total of 464 requests were made during the entire study period. Female patients accounted for the majority of the requests, making 82% of all requests (n = 382) in comparison to 18% (n = 82) made by male patients, yielding an average of 1.64 requests per male patient in contrast to an average of 2.19 requests made per female patient. Of the 464 requests made across all service areas, 85% (n = 395) were provided access to the requested services at the time of the medical visit (Table 2, Figure 3).
Services Requested, by Gender, on the Previsit Screening Checklist. a
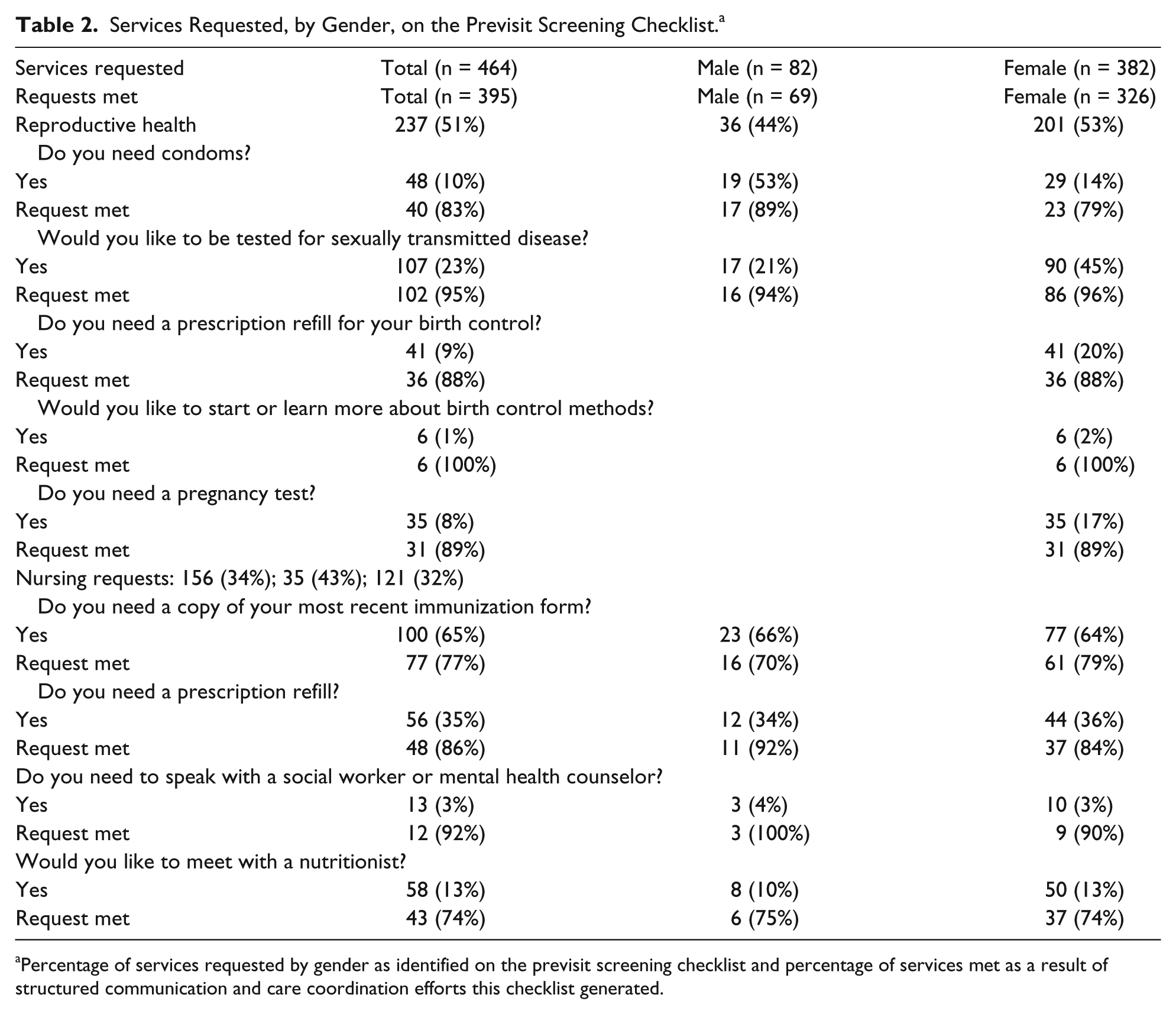
Percentage of services requested by gender as identified on the previsit screening checklist and percentage of services met as a result of structured communication and care coordination efforts this checklist generated.
Among the services requested, reproductive health services accounted for 51% of all the requests made across gender (Table 2). For female patients, reproductive health services included pregnancy testing, contraception refill or initiation, screening for sexually transmitted infection (STI), and requests for condoms. For male patients, reproductive health services included requests for STI screening or requests for condoms. STI screening included testing for Chlamydia trachomatis and Neisseria gonorrhoeae and/or HIV. Among female patients (n = 172), 201 requests for reproductive health services were made. Reproductive health service requests for female patients had high completion rates (91%), with 100% of requests for birth control initiation met, followed by 96% of STI screening requests met (Table 2). In comparison, reproductive health services among male patients (n = 82) accounted for 44% (n = 36) of all requests made in this group. About 92% of all reproductive health services requested were met in this group (Table 2).
Nursing services were the second most frequently requested services after reproductive health (Figure 2). Nursing services included requests for completion of specific health forms or a printed copy of annual physical forms and prescription refills (excluding birth control refills for female patients). Unless verbal communication within the care team occurred at the time these services were provided, it was difficult to track completion. In response to this, a written staff communication section was added to the previsit checklist, with staff members leaving notes to indicate whether or not a request was fulfilled (Figure 1); 32% (n = 121) of all female patients’ requests (n = 382) were for nursing services, compared with 43% (n = 35) among male patients (Figure 2). Approximately two-thirds of nursing requests by both female and male patients were for health forms completion or printed copy of last annual physical forms (Table 2). Assuming undocumented tasks were uncompleted, we estimate that 79% (n = 61; 95% CI = 78.18%-80.26%) of requests by female patients for health or immunization forms were met, compared with 70% (n = 16; 95% CI = 65.62%-73.48%) among male patients (Table 2). Again, assuming that requests with a missing documentation were unmet, 84% (95% CI = 82.45%-85.73%) of prescription refill requests for females and 92% (95% CI = 87.17%-96.17%) for males were completed (Table 2).
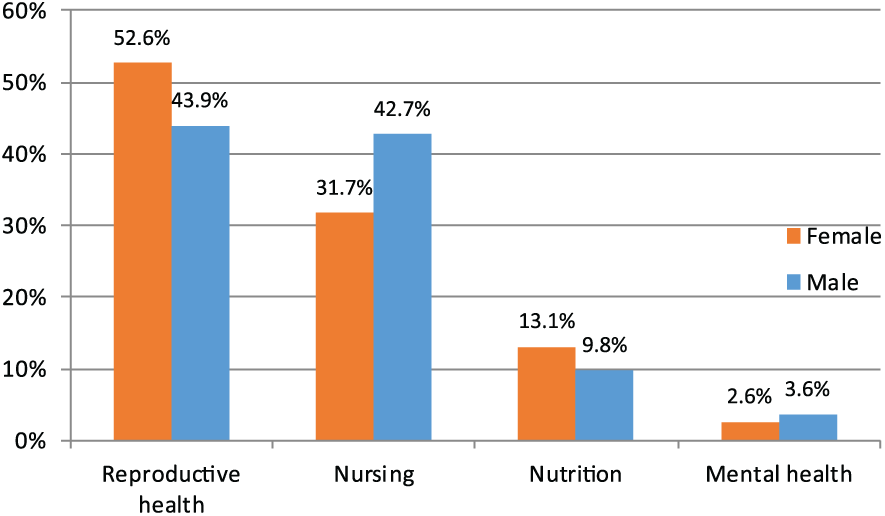
Categories of preventive health services requested by male and female patients, in percentage.
Nutrition counseling services were less frequently requested, particularly among male patients, representing only 10% (n = 8) of all requests made by male patients (n = 82) compared with 13% (n = 50) of requests made for nutrition services among female patients (n = 382; Table 2 and Figure 2). Of the 58 nutritionist services requests, 26% (n = 15) accessed nutrition services at the time of their medical visit; 52% (n = 30) opted to schedule an appointment at a later time; and 22% (n = 13) chose not to schedule an appointment for a later date when same-day appointment was not available. Overall, 74% (n = 43) of all requests for nutrition counseling (n = 58) were met: 75% for male and 74% for female patients (Table 2).
There were overall fewer requests for social work and mental health services; only 3 male patients and 10 female patients requested these services over the 8-month study period. However, almost all (92%) patients requesting social services referral had their needs met (Table 2).
Staff Feedback Regarding Clinic Workflow
Staff involved in this project reported that the coordination of services requested sometimes led to increased patient wait time. This would occur most frequently when the CA to provider ratio was too low to meet high demands. When increased waiting time was a barrier to access services, patients were advised to schedule a visit at a later time for the particular services they requested, although many were also willing to wait after completing the visit with their medical provider.
Discussion
Our key informant interview process was crucial in adopting the previsit screening checklist in its current version (Figure 1). Our YAB members clearly voiced the need for such a tool to inform patients of what services were available to them in real time and as a facilitator for adolescents to address their health care needs and access timely preventive services. However, PAB members were divided around the appropriateness of reproductive health questions, which seemed to be influenced by cultural differences, whereas on the other end, YAB members expressed challenges accessing health services, particularly around reproductive health, and stressed the importance of keeping confidentiality around previsit screening process as reported in the existing literature.19-24
The previsit screening checklist was easily incorporated in the clinic workflow. It promoted a culture of teamwork by eliciting real-time communication around patient medical needs and delegation of tasks to meet these needs. The staff felt more involved in the care of patients, and increased teamwork led the provider to focus on the medical aspects of the visit. One concern raised by the staff was whether the previsit screening checklist was leading to overuse of certain services, citing as an example a perceived “high number of pregnancy test” requests. Although it is impossible to identify if patients requested this service because it was suggested, it is important to note that we were able to meet 89% of these requests (Table 2), thus allowing either prevention or addressing risk of a potential unexpected pregnancy.25-27
The implementation of the previsit screening checklist was at times hindered by staffing and clinic flow issues. We conducted several PDSA cycles to address this. Among ideas generated, one included limiting the type of visits during which the form was deployed (well visits vs problem-focused visits). This was helpful in balancing demand versus access when faced with limited capacity to provide access (Figure 3). During busy clinic hours, communication among staff was more difficult to maintain, leading to confusion among team members around what request has been fulfilled. In response to this, another PDSA was implemented and involved the addition of staff communication line next to each item on the checklist (Figure 3). This allowed the provider as well as the rest of the team to be aware of action taken to coordinate care, thus helping maintain communication, avoid duplicating efforts, and support tracking of the intervention.
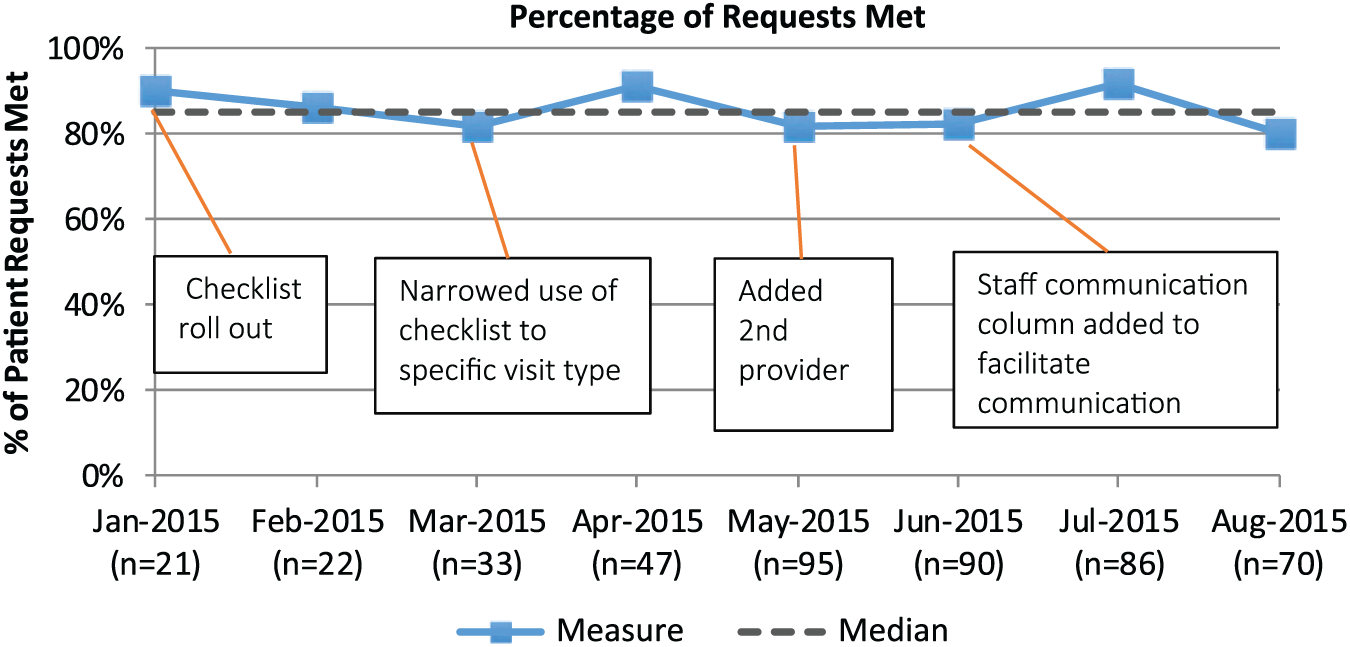
The run chart describes the different tests to change we conducted to meet patient’s request for preventive health services and same-day access to these services. The Y-axis represents the percentage of services met as identified on the previsit screening checklist. The X-axis represents the total number of services requested using this checklist. Patients were allowed to request more than 1 service.
The previsit screening checklist process was facilitated by the fact that patients were scheduled to arrive 30 minutes prior to their medical encounter to allow time for standard visit screening and nursing assessment, thus providing extra time for coordination of services. Most services were already physically integrated in our clinical areas and most had an open visit template, allowing for same-day access. Our reproductive health services perfectly illustrated this model with the highest completion rate for requested services (Figure 2). Although nutrition services are integrated in the clinic, they operate on a mixed visit template, allowing a few slots to be booked in advance, which at times conflicted with the need for same-day access. This difference may explain the smaller percentage of immediate access to nutrition services in contrast with other services (Figure 2). To preserve clinic workflow and access, patients who were not able to be seen at the time of their visit were encouraged to schedule a nutrition visit at a later time.
Coordination of services in this pilot project was made possible with a limited number of provider visits and medical staff using the previsit screening checklist. In addition to staffing and workflow hurdles, absence of baseline data has been another limitation to claim success with confidence and bring this project to a larger scale within our practice. Because of the nature of this initiative, it was challenging to find preexisting measurable markers that could reliably reflect team work and be applied to our process evaluation.
Although there are many variables in the way patients access preventive services during a primary care visit and no easy one to track access to those services, we were able to observe a 20% average increase in reproductive health counseling visit note type per month from 184 to 223, across the entire practice, during the first 3 months following the introduction of the previsit screening checklist. Reproductive health services were the most frequently requested services and also the ones with the highest percentage of access to services provided, when using the previsit screening checklist. This demonstrates that a previsit screening checklist can optimize teamwork and increase patient access to preventive services and, thus, supports our hypothesis.
Although it is unclear whether our improvement process may have undermined unadjusted variables contributing to its success, the use of a previsit screening checklist does provide a framework that supports a culture of communication and empowers nonclinical staff to take action. This truly represents a cultural change, in a work environment that is traditionally very provider centric. When used in a primary care setting, a previsit screening checklist allows teams to untangle themselves from their routine and problem solve through structured communication, which ultimately enhances health care delivery. From a patient perspective, it not only promotes timely access to preventive services, as for adolescents and young adults in this case, but it also supports patient engagement in decision making, which is associated with better health outcomes in this age group.1,2
Despite established guidelines and provisions in the ACA, access to basic medical care, as for many Americans, is still a challenge for a number of adolescents and young adults.2,28 In this quality improvement project, 29 we tested a novel approach to optimize access to preventive services by empowering nonclinician staff to take on more tasks and proactively coordinate patient access to services. We encountered challenges in our process when the ratio of support staff to provider was low to coordinate patient requests. Allocating more resources to care coordination growth by supporting new skill sets training (ie, care team coordinator, health coaches) and implementing a reimbursement system for care coordination will increase primary care capacity, workflow efficiency, and health care access, as demonstrated in this quality improvement initiative, using a simple 11-item previsit screening checklist.
Author Contributions
SHA-R conceptualized the project, interpreted data, drafted and revised the manuscript. STJ contributed to data collection, data analysis, the initial drafting of the manuscript and its revision. MM performed data analysis and contributed to thorough manuscript revision. PG provided substantial contribution to the project and reviewed the manuscript. KR contributed to initial data collection and reviewed the manuscript. AE-B provided guidance for this project, critically reviewed and revised manuscript.
Footnotes
Acknowledgements
The authors would like thank Elizabeth R. Woods, MD, MPH, for her time, suggestions, and thoughtful review of this article. The Boston Children’s Hospital Primary Care at Martha Eliot Leadership and Staff for their support. The authors confirm that the manuscript has been read and approved by all named authors there are no other persons who satisfied the criteria for authorship that are not listed. We further confirm that the order of authors listed in the manuscript has been approved by all of us. Preliminary results related to the project described in this manuscript has been previously presented as a poster at the Society of Adolescent Health Medicine annual meeting. This manuscript has otherwise not been previously published and is not under consideration for another publication. The authors have no conflict of interest to disclose.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was made possible with the support of the Harvard Medical Faculty Teaching Compensation.