
Abstract
Introduction. The purpose of this study was to pilot a brief measure of family functioning (Family Assessment Device–General Functioning [FAD_GF]) with caregivers of children aged 2 to 18 years, seen for routine pediatric primary care visits. Methods. This study evaluated the psychometric properties of the FAD_GF in a pediatric primary care sample of 400 families. Confirmatory factor analysis was used to validate the FAD_GF using R, and WLSMV was used to estimate missing variables. Results. The FAD_GF was found to be reliable with this sample, α = .90. The model fit was χ2(54) = 56.44, P = .38, with root mean square error of approximation = .01 and comparative fit index = .99. The 12 items were significantly predicted by family functioning, and family functioning explained more than 20% of the variance in the items, R2 > .25. Overall, 12.6% (n = 46) of families were identified as having clinically impaired family functioning. Discussion. The FAD_GF provides clinicians the ability to make evidence-informed decisions regarding referrals to family therapists.
Introduction
Behavioral and mental health screenings, as well as referrals, are not reaching all children, with only 21% of children diagnosed with a mental illness receiving services. 1 Children with mental health challenges are at increased risk for poor school performance, engagement with the juvenile justice system, and ultimately suicide.2-4 The average delay between behavioral/mental health symptom onset and intervention services is approximately 10 years. 5 The majority of pediatricians perceive a need for behavioral/mental health services, with 50% to 80% of them feeling responsible for identifying child behavioral/mental health concerns. 6 In response to this need, the American Academy of Pediatrics (AAP) is supporting the development of policies to provide early identification and treatment of children’s mental health disorders. 1
One way the AAP is encouraging more comprehensive services, including mental health, is through the adoption of the Child-Centered Medical Home (CCMH). The AAP defines the CCMH as “an approach to comprehensive and high quality medical care” marked by the following characteristics: accessibility, family-centered, continuity, comprehensive, coordinated, compassionate, and culturally effective. 1 Medical homes provide integrated care in which multidisciplinary health care professionals care for the varied needs of children and families. 7 As the lead of the CCMH, pediatricians are encouraged to consider the cultural beliefs, values of communities, and interpersonal family dynamics and relationships. 8 As it pertains to behavioral/mental health, screening for and providing appropriate care can be seen as a core tenet of a CCMH.
According to the AAP, patient- and family-centered care (PFCC) is the provision of care involving the patient and his/her family in health care decision making as equal partners with health care providers, and is an essential component of high-quality medical homes.9,10 As emphasis on the importance of PFCC has increased, researchers have called for more clarity and direction on the practices that constitute PFCC, and appropriate implementation of these practices. 9 As noted by the AAP’s Task Force on the Family, a child’s outcomes— “their physical and emotional health and their cognitive and social functioning—are strongly influenced by how well their families function.” 11 (p1563) To provide family-centered care, more must be understood about a child’s family, and how best to intervene. Theories grounded in family science may help clarify and provide guidance on how to assess and involve family members in pediatric primary care to benefit children’s mental/behavioral health.
Family systems theory (FST)12,13 explains how families structure themselves around various medical and mental health diagnoses and challenges, and more specifically, how family interactions influence compliance with prevention and treatment guidance provided in health care. For instance, children diagnosed with asthma may experience sleep disturbance, which may negatively affect family morning rituals and routines, and subsequently, the quality of family interactions in the morning as the child struggles with fatigue and caregivers struggle with completion of morning routines. Rather than solely targeting the child’s health status, pediatric primary care providers using FST seek to intervene with both the child and family members (the family system) in order to promote positive health (physical and mental) behaviors and habits. Family functioning offers researchers a promising way to quantify dynamic interactions in the family system and the application of FST in clinical settings.
The McMaster model of family functioning is based on tenants of FST. Family systems’ theoretical assumptions emphasized within the McMaster model include the following: (1) all parts of the family are interconnected, (2) individuals must be understood in context of his/her family, (3) family functioning cannot be captured by an isolated understanding of subgroups (ie, parents only) or individual members, (4) family structure and organization influence and determine family members’ behaviors, and (5) family system patterns of behavior influence individual member behaviors. 14 The McMaster model focuses on the following 6 dimensions of family life to understand the complex patterns and behaviors of families: communication, problem solving, roles, affective involvement (or the emotional expression and response of family members), affective responsiveness (or the interest or concern of members for one another), and behavior control. 14 The McMaster model has been adapted into a number of assessment methods including clinical interviews (McMaster Structured Interview of Family Functioning), observational assessments (McMaster Clinical Rating Scale and Mealtime Interaction Coding System), and self-report measures (McMaster Family Assessment Device).
The Society of Pediatric Psychology Task Force rated the McMaster Family Assessment Device (FAD) as a well-established self-report measure due to its consistent test-retest reliability and internal consistency. 15 There are 7 subscales of the FAD that are similar to the 6 dimensions of family life mentioned above: problem solving, communication, roles, affective responsiveness, affective involvement, behavior control, and general functioning. 16 Though the FAD is preferable from cost, training, and efficiency perspectives to direct observation and interviewing, the length of the 60-item survey can be problematic in settings where participants are filling out multiple questionnaires and are time-limited. Byles and colleagues 17 established the reliability and validity of the General Functioning Subscale of the Family Assessment Device (FAD_GF) using the Ontario Child Health study. More recently, researchers have assessed the validity of the FAD_GF 12-item measure against composite scores on the other 6 subscales of the full 60-item FAD, and concluded that the FAD_GF is an acceptable proxy for providing an overall picture of family functioning in both clinical and nonclinical samples. 18 The FAD_GF shows promise as an easily administered assessment in pediatric primary care and with diverse families. 19 A systematic review of the self-report family assessment measures indicated that the FAD had demonstrated strong construct and criterion validity. 20 The FAD has been used with diverse families, including race/ethnicity, 21 education, 22 family structure,23,24 and income.23,25
Families are responsive to their pediatricians providing mental/behavioral health screening; however, the time constraints placed on pediatricians require that they efficiently determine what families can benefit from more intensive services to address family dynamic and relationship needs. A review of universal mental health screening in pediatric primary care revealed that patients responded well to mental health screenings, which were portrayed as universal, confidential, and optimizing patient concerns. 26 Furthermore, Jonovich and colleagues 27 included parent and child mental health screeners in routine well-child visits and found that mental health screeners increased referrals to family and community counseling services. Finally, screening for deficits in family functioning rather than current mental health symptoms in parents and children may offer an opportunity for preventative efforts in families with younger children. Ferro and Boyle 28 found that family functioning mediated the relationship between child chronic health symptoms and child anxiety and depressive symptoms, indicating that family functioning may indicate risk for child mental health challenges prior to symptom onset. Screeners who are able to integrate tenants of FST, are brief, and require minimal training prior to implementation may provide the greatest utility in pediatric primary care. A successful example of this model is the Pediatric Symptom Checklist, 29 a brief, validated measure that accurately screens children for cognitive, emotional, or behavioral problems.30,31 The ease of administering and scoring allows for use in primary care; an elevated score indicates possible psychosocial challenges, and therefore, additional assessment or referral is needed.
Taken together, pediatricians report that they feel responsible for the comprehensive welfare of their pediatric patients and that families may be open to receiving referrals for mental/behavioral health care when executed in a nonjudgmental and open manner. Utilization of a brief family functioning screener, like the FAD_GF, may provide primary care practitioners with a way to identify families who may benefit from additional behavioral health services, such as brief family therapy, to address impaired family dynamics that may affect a child’s health in the short term and long term. The FAD_GF may be an appropriate tool to both assess family dynamics in pediatric primary care and provide a rationale for referral and collaboration with mental/behavioral health providers to address needs related to family functioning.
Purpose
The purpose of this study is to pilot a brief family functioning screener, using the FAD_GF subscale in pediatric primary care practices among a sample of diverse caregivers of pediatric patients aged 2 to 18 years. The results from this study will allow researchers to further determine how the assessment of family functioning could be included within pediatric primary care visits, and long-term may provide a way to identify families who could benefit from on-site mental/behavioral health and/or family therapy referrals and services.
Methods
Procedures
Following institutional review board approval, a convenience sample of 400 participants was recruited from 2 pediatric primary care clinics (Columbus, Ohio). To be eligible for the study, participants had to speak/read English, identify as the primary caregiver or parent of a patient between the ages of 2 and 18 years, and be over the age of 18 years. Every consecutive family meeting our inclusion criteria had an equal opportunity for enrollment while the research assistant was there, 2 days per week, for the duration of the study from September 6, 2016, to December 6, 2016. Of the 423 families recruited to participate, 23 families declined (5%), citing concerns around time constraints. Written consent was obtained from eligible caregiver participants. Participants completed the paper-and-pencil survey containing an investigator-created demographics form and the FAD_GF while they were waiting to see their provider. Caregivers were instructed to complete the survey for one of their children if multiple children over the age of 2 years were present at the visit. Participants were compensated for their time completing the survey with local retail gift cards.
Measures
Demographics
The investigator-created demographics questionnaire contained caregiver and child age, gender, education, and race/ethnicity. It also contained child’s insurance status, height and weight, medical diagnoses, caregiver marital status and employment, languages spoken in the household, family income, and home ownership.
Race
Caregiver and child race were collapsed into 3 categories: Caucasian, African American, and Other. Other was used due to the low participant response as American Indian/Native Alaskan and Asian. Participants were able to self-identify as one or more races.
Child Insurance
The insurance variable was examined as both a categorical and dichotomous variable, with the varied options (traditional health insurance [Fee for service where you choose your doctor and most fees are covered], Medicaid, Medicare, None, and Other) being collapsed into traditional and government-assisted insurance. None and Other were dropped from analysis due to their small sample sizes (n = 5, 1%; n = 36, 9.1%) for the dichotomous variable, but Other was included as a separate category in categorical analysis.
Education
The education variable was examined as both a categorical (less than high school, high school/graduate diploma, college degree/graduate, graduate degree [eg, master’s, doctorate, etc], and other) and dichotomous variable, with the levels of education collapsed into at or above a bachelor’s degree and below a bachelor’s degree.
Income
Caregiver reported income was transformed from a categorical category (below $25 000; $25 000-$49 000; $50 000-$74 000; $75 000-$99 000; and $100 000 and above) into a dichotomous category, which placed families at or above the poverty line. Families who reported an income of <$50 000 of the poverty line were coded as 0 and those above $50 000 as 1.
FAD_GF Subscale
The FAD_GF is a 12-item scale that asks participants to identify with varying statements on a Likert-type scale from 1 to 4, ranging from 1 as strongly agree to 4 as strongly disagree. Scores of 1 indicate the healthiest family functioning, while scores of 4 indicate the least healthy family functioning. The responses to the 12 items are summed for the total score and averaged to determine the clinical cutoff. A score <2.00 indicates healthy functioning, whereas ≥ 2.00 indicates impaired functioning. 16
Statistical Analysis
Analyses were conducted through IBM SPSS (version 24) and R. Descriptive statistics were generated in SPSS for all demographic variables. ANOVA (analysis of variance) and independent t tests were used to assess mean differences on the FAD_GF. Chi-square tests were run to assess mean differences between demographic categorical variables and participants below and above the family functioning cutoff score. Confirmatory factor analysis was conducted in R to assess the validity of the FAD_GF.
Results
Demographic information for children and caregivers can be found in Table 1. Caregiver participants predominately identified as females (77.7%), with a mean age of 38.18 years (SD = 7.96; range = 21-69 years). The majority of participants identified as Caucasian (81.5%), followed by African American (13.7%), Asian (1.0%), Biracial or Multiracial (1.3%), and Other (2.5%). Few respondents identified as Hispanic (3.3%). The sample reported high educational attainment, with 74% of the sample attaining at least a college degree. Most of the sample identified as employed (75.6%) and reported that they were currently married (77.9%). While our sample was similar to a nationally representative sample with respect to racial diversity, there was a biased representation of families by education, income, and insurance status. Caregivers in our sample were more likely to have attained a college degree (sample = 74.6%; US = 30%; and Ohio = 26.7%), more likely to have an income above the federal poverty line (sample = 81.7%; US = 87.3%; and Ohio = 85.4%), and more likely to have an insured child (sample = 98.8%; US = 89.9%; and Ohio = 93.4%) than known state and national prevalence. 32
Sample Demographics a .
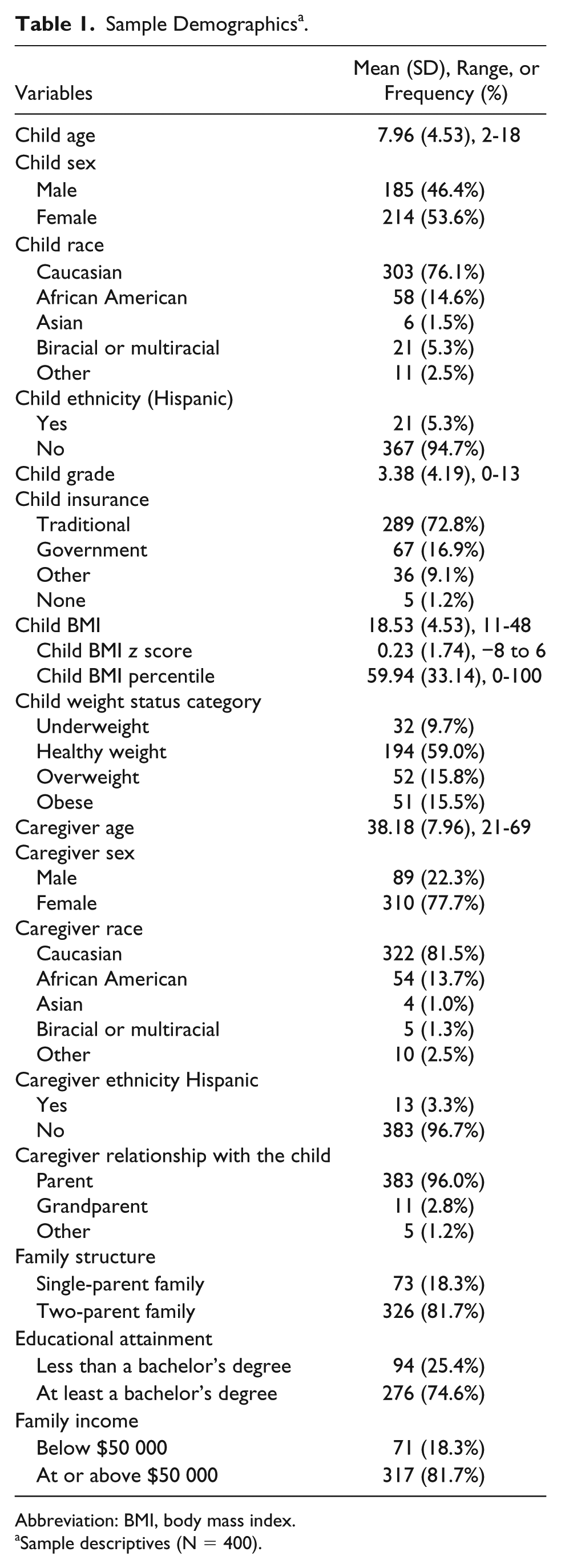
Abbreviation: BMI, body mass index.
Sample descriptives (N = 400).
There was a relatively even split of children by sex with 46.5% of the sample identified as male and 53.6% female. The mean child age was 7.96 years (SD = 4.53), the range was 2 to 18. Participants identified their children as Caucasian (76.1%), African American (14.6%), Asian (1.5%), Biracial or Multiracial (5.3%), and Other (2.5%). Only 5.3% of children in the sample were identified as Hispanic. Children were predominately insured by traditional insurance (72.9%), followed by government insurance including Medicare/Medicaid (16.9%) and Other (9.0%). Approximately 1% of the sample reported having no health insurance. The majority of families reported an income at or above $50 000 per year (81.7%), with 43% of families with an income at or above $100 000 per year. Families were predominately homeowners (74.6%) with an average of 4.3 people (SD = 1.09), including the caregiver participant, living in the home.
The average total score on the FAD_GF was 16.83 (SD = 4.74), and the range was 12 to 32. The majority of the sample scored below the clinical cutoff for “general functioning,” indicating healthy functioning; 12.8% of families, or 46 families, were at or above the cutoff, indicating that they are experiencing impaired family functioning.
General Functioning Subscale Confirmatory Factor Analysis
A confirmatory factor analysis was estimated using R. 33 Missing data were handled using the LaVaan package with diagonally weighted least squares with robust standard errors (WLSMV).34,35 The initial model was χ2(54) = 56.44, P = .38. There was good model fit as indicated by an insignificant χ2 value; the root mean square error of approximation was .01, the standardized mean square residual index was .05, and the comparative fit index was .99. All of the 12 items were significantly predicted by the latent factor of family functioning. The latent factor family functioning explained more than 40% of variance of all items except item 2, “In times of crisis we can turn to each other for support,” R2 = .34; item 4, “Individuals are accepted for what they are,” R2 = .25; and item 10, “We are able to make decisions about how to solve problems,” R2 = .28 (Table 2).
General Functioning Subscale of the Family Assessment Device Full Model a .
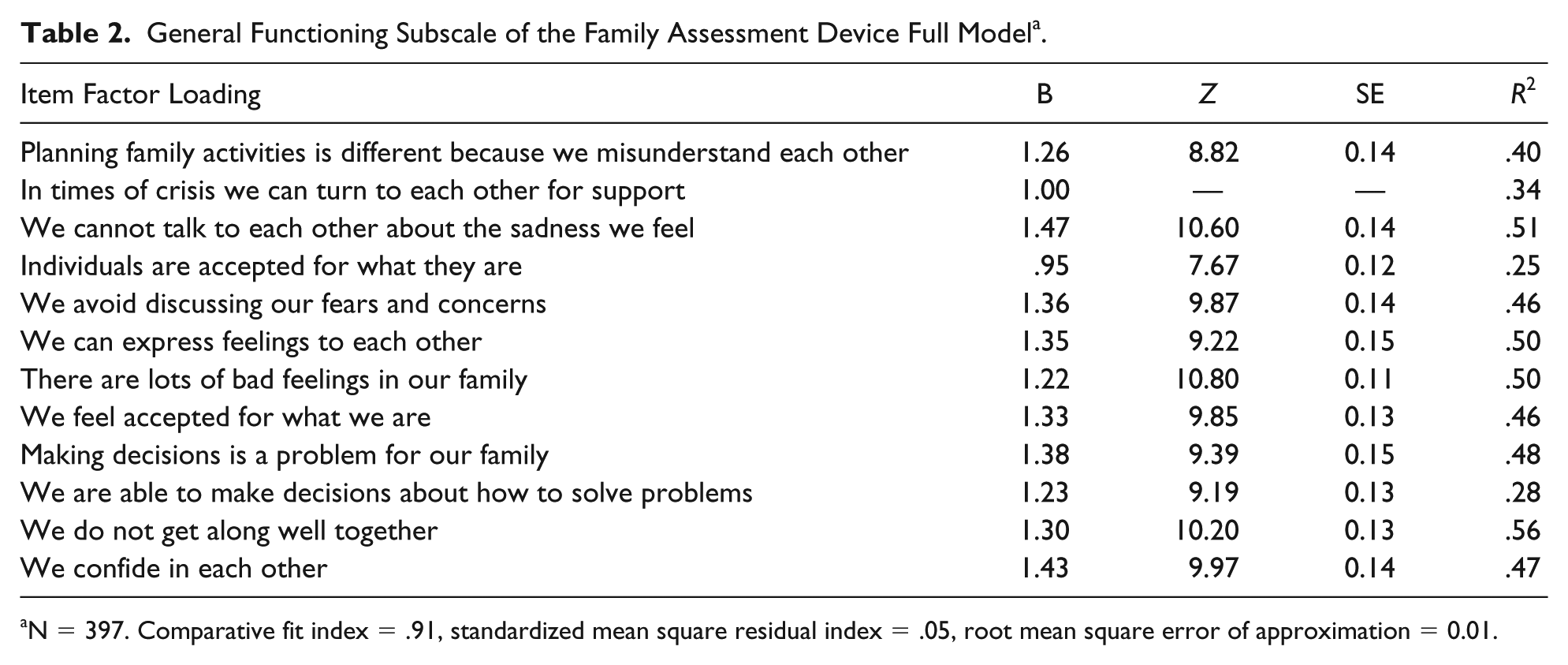
N = 397. Comparative fit index = .91, standardized mean square residual index = .05, root mean square error of approximation = 0.01.
General Functioning and Demographic Variables
There were limited significant relationships between FAD_GF total score and clinical cutoff score and demographic variables, apart from child age and caregiver education. The FAD_GF total score was used as a continuous variable in analysis while the clinical cutoff score was a dichotomous variable (below clinical cutoff, at or above cutoff). Variables that were assessed that were not statistically significant include caregiver race/ethnicity, marital status, employment, family income, child gender, child insurance, child race/ethnicity, and child height and weight.
A χ2 test of independence was performed to examine the relationship between caregiver education attainment and the FAD_GF clinical score, with caregiver educational attainment dichotomized (below a bachelor’s degree, at or above a bachelor’s degree). The relationship between the variables was significant, χ2(2, N = 341) = 4.43, P = .04 (Table 3). Child age was positively and significantly correlated with family functioning (r[357] = .119, P < .05), where caregivers of older children reported experiencing higher impairment in family functioning as a total score, without including the clinical cutoff. Furthermore, there was a significant difference in the age of children who scored at or above the clinical cutoff for impaired family functioning, where caregivers who reported higher family functioning impairment had older children (mean = 8.96, SD = 4.46) compared with caregivers who reported lower impairment had younger children (mean = 7.57, SD = 5.02; t[355] = −1.94, P = .05). Family annual income was marginally correlated with the FAD_GF total score (r[358] = −.09, P = .09), where caregivers who reported lower family income were more likely to have a higher score on the FAD_GF, or a higher level of impairment in family functioning.
Caregiver Educational Attainment and Family Functioning a .
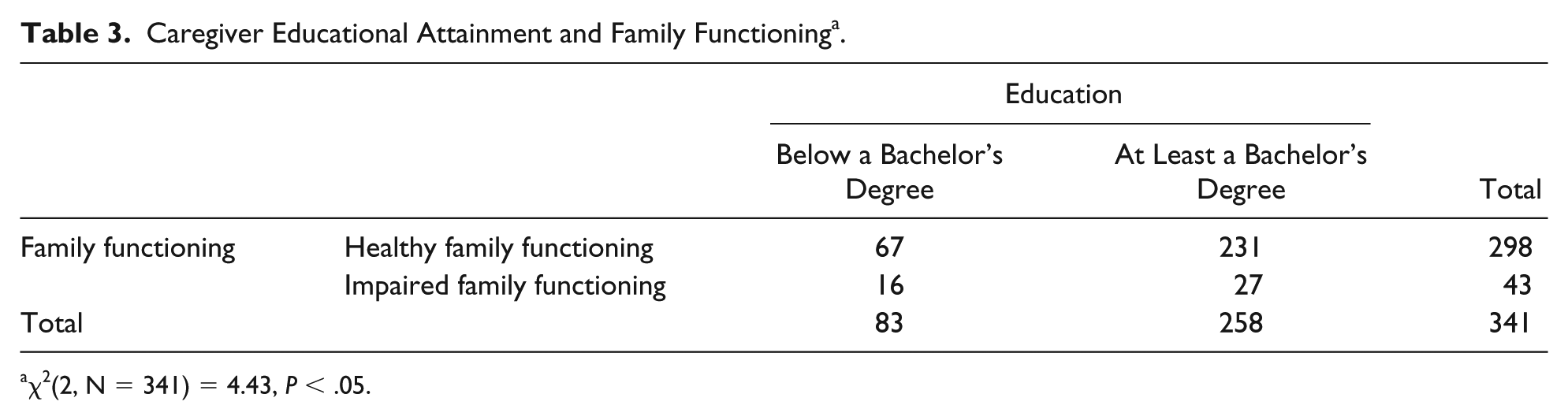
χ2(2, N = 341) = 4.43, P < .05.
Discussion
The purpose of this study was to pilot the FAD_GF in a pediatric primary care sample of caregivers of children aged 2 to 18 years. Overall, the FAD_GF was found to be reliable and valid for use with this population. The fit indices of the confirmatory factor analysis indicated that the model had good overall fit. These findings support the latent variable of family functioning, adding to the existing body of literature indicating construct validity for family functioning. However, while most items had factor loadings above .4, item 2, “In times of crisis we can turn to each other for support,” item 4, “Individuals are accepted for what they are,” and item 10, “We are able to make decisions about how to solve problems,” had factor loadings below .4. Boterhoven and colleagues 22 tested the validity of using an abbreviated form of the FAD_GF compared with the established FAD_GF in a sample of parents answering questions about their child’s health. Their abbreviated 6-item scale only included the positively oriented items from the FAD_GF (2, 4, 6, 8, 10, and 12). They found that the 6-item scale was as effective as the established FAD_GF 12-item scale. 22 The authors hypothesized that the positive items of the FAD_GF would have higher reliability than the negative items. However, in analysis of our sample, the negative items in the FAD_GF had higher factor loadings than the positive items. For those wishing to use an abbreviated measure, briefer than 12 items, additional research is needed to discern which items are appropriate for inclusion. The theoretical and clinical origins of the McMaster Model of Family Functioning: Family Assessment Device and the General Functioning subscale support the use of the both positive and negative items to gain a more comprehensive picture of the family, despite potentially lower psychometric properties resulting from keeping the items together in a single scale.
Overall, caregiver, child, and family demographic variables were not significantly associated with the FAD_GF, with the exception of child age and caregiver educational attainment. The lack of significance between demographic groups (ie, race/ethnicity, gender, and insurance status) demonstrates the strength of the FAD_GF as a measure to assess impaired family functioning among diverse families. Further research is required to assess for whom this measure is appropriate.
Within this study, families with higher impairments in family functioning had older children. Similarly, Herzer and colleagues 19 found that families with older children were at risk for impaired family functioning in a sample of children diagnosed with a chronic illness and healthy peers. They posited that challenging family dynamics may have more time to manifest as children age, given that older children and adolescents begin to assert autonomy and test boundaries. Furthermore, as children age they may begin to have different priorities from their parents related to time spent with family versus friends, and the rules and routines in the family. Future research should determine how both parent and child perspectives of family functioning change as children progress through developmental stages. This inquiry could answer questions such as “Do parents of young children who report healthy family functioning continue to report healthy functioning as their children age? “Do parents regardless of reports of family functioning when their children were younger, have lower reports of family functioning when their children become adolescents?” “What is the congruence between parents and children’s reports of family functioning in primary care as children age?” “Are parents and adolescents more likely to be less congruent in their reports of family functioning compared with parents and children?”
In our sample, both lower caregiver educational attainment and family income were positively associated with lower family functioning. Limited research has been done to assess these 2 demographics variables and their association with family functioning.23-25 Georgiades and colleagues 24 found that education was significantly associated with family functioning, where lower education was associated with lower functioning. They also found associations with socioeconomic status (SES) and family functioning where families with higher SES reported high levels of family functioning. 24 However, Herzer and colleagues 19 failed to separately report associations with education and family functioning, despite reporting associations with lower SES. This may indicate a preference to examine overarching family sociodemographic variables rather than individual characteristics of caregivers. Using the FAD, Banovcinova et al 25 found a significant association between poverty and impaired family functioning. Finally, using the FAD_GF, Beiser and colleagues 23 found that impaired family functioning mediated the relationship between family poverty status and child behavioral and emotional problems in a sample of Canadian children. Further research is necessary to understand the mechanisms through which variables related to SES, like caregiver educational attainment and family income, and impaired family functioning may be related. It may be that SES as a whole is a stronger predictor of family functioning, or that individual predictors like caregiver educational attainment are more meaningful predictors.
Limitations
The cross-sectional nature of this study precludes any longitudinal or causal interpretations of findings. This sample was not nationally representative; however, the state in which this study was conducted has demographics that mirror those of national demographics. Although there were families with incomes below the federal poverty line, 43% of families in this sample had incomes at or above $100 000, indicating that there was likely underrepresentation for lower income families. Our study was not perceived as a part of routine care, but as supplemental to the mandatory forms of the clinic. Families who refused to participate reported perceived time constraints around the survey, with some running late to their appointment or anticipating a quick visit and opting to only complete the forms provided by the medical staff. Wissow and colleagues 26 reported increases in acceptability of mental health screeners that were presented as universal. Patient participation and acceptance of the measure may increase if provided to all patients by health care staff rather than external researchers. The presence of research staff may indicate to patients that this screening is optional and not adopted by the plurality of the medical community. While the FAD_GF was reliable (α > .9), there were 3 items with lower psychometric properties, as indicated through the confirmatory factor analysis. These items may lessen our ability to detect impairments in the total family functioning score. Finally, this study only sought one familial perspective, from the attending caregiver, regarding family functioning, and may have subsequently missed the benefits of having multiple perspectives of family functioning, such as that from additional caregivers, older children, or other significant individuals in the child and family’s life.
Future Directions and Implications
The findings of this study, coupled with the prior research on the FAD_GF, indicate that the FAD_GF has high internal consistency, does not distinguish between families of various demographic backgrounds, has ease of implementation, and is able to discern between clinically impaired and healthy family functioning. Nearly 13% of families were at or above the clinical cutoff for family functioning, indicating a need for intervention for families in pediatric primary care. Given the shift to family-centered care, measures to assess the overall family emotional environment are needed, and the FAD_GF holds great promise as brief, reliable, and valid tool in pediatric primary care. Finally, future research should explore associations of general family functioning and relevant demographic variables in pediatric primary care settings in order to better understand for whom and how this measure is helpful, and how to use the FAD_GF to base mental/behavioral health on and off-site referrals for those families with impaired family functioning.
Author Contribution
CAVF and KJP contributed to study conception and design and data acquisition and analysis. All co-authors contributed to data interpretation and drafting and revising the manuscript. Access to the data was provided by the Ohio Academy of Pediatrics.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The second author (Pratt) funded the study through internal funds from The Ohio State University, College of Education and Human Ecology, Department of Human Science.