
Abstract
Family-centered childhood obesity interventions have been found to be effective. We describe the use of telehealth for tailored behavior change support in a family-centered randomized trial. Children of 2 to 12 years with body mass index ≥85th percentile were randomized to Enhanced Primary Care (EPC) or Enhanced Primary Care + Coaching (EPC + C). EPC + C received 6 health coach visits (in-person or by video or phone call) over 1 year. Telehealth modalities included interactive text messaging, video calls, and an online community resource map. There were 360 children randomized to the EPC + C arm; 87% of parents completed ≥1 health coaching contacts. Overall, 93% parents were sent text messages of which 99% responded at least once. About 72% parents were very satisfied with the message content and 97% were satisfied with information provided about community health resources. The high level of participant engagement and satisfaction suggests that telehealth is feasible and acceptable in family-centered childhood obesity programs.
Background
Obesity is a major clinical and public health problem in the United States and worldwide. Despite recent declines in the prevalence among preschool-aged children, childhood obesity is a serious problem putting children at risk for poor health. 1 Without any intervention, children with obesity have a greater than 50% risk of having obesity in adulthood. 2 Family-based behavioral treatments offer a cost-effective and efficient means of intervening. 3 Behavioral interventions have traditionally been delivered in-person, but this can be challenging. The cost and time for patients to attend onsite sessions pose barriers to participation. 4 Telehealth may be a more feasible option for the treatment and management of childhood obesity, and interventions delivered in person have shown no significant difference in weight-related outcomes and satisfaction compared with those delivered using remote digital technologies.5,6
Recently, behavioral interventions have been administered successfully via telehealth modalities. The Health Resources and Services Administration of the US Department of Health and Human Services defines telehealth as “the use of electronic information and telecommunications technologies to support and promote long-distance clinical health care, patient and professional health-related education, public health, and health administration.” Technologies used include videoconferencing, streaming media, and wireless communications. 7 Telehealth can support health care delivery in numerous ways, including delivering inpatient and outpatient care, medical emergency response, educating physicians and patients, conducting medical research, and more generally augmenting the communication between families and the medical professionals who care for their children. 8 With the ever-improving developments in technology, it holds a promising future for delivering health care across a wide population.
In obesity management trials, different modes of telehealth have been used. Randomized controlled trials using interactive text messaging as a method of health coaching to supplement standard care have shown greater weight loss as compared with standard treatment of care.9-12 One obesity management intervention found that greater engagement with text messages correlated with higher weight loss, 13 more improvement in weight-related behaviors, 12 and better study retention. 14 Videoconferencing offers real-time interactions and is another tool being used to deliver health care interventions. When used in weight management trials, it has shown promising results in terms of weight loss, satisfaction, and adherence.15-17 It also offers the advantage of convenience, including less work or school missed for appointments, less travel, decreased financial burden, and more easily accessible health care in rural areas, among others.18-20 Another method of enhancing and tailoring counseling for obesity is to identify neighborhood socioeconomic characteristics and built environment factors that contribute to weight-related outcomes. Geographical information systems (GIS) computer-based mapping tools have been used in obesity studies to identify food establishments and physical activity resources within communities.21-23 These resources can then be shared with patients to support healthy behavior change.
In this study, we examined the use of telehealth technology to support behavior change among parents and children participating in a pediatric weight management intervention. The intervention incorporated the use of interactive text messaging, video calling, and an online community resource mapping tool to coach family behavior change. We hypothesized that incorporating digital technology to provide parents with tailored behavior change support would be feasible, well accepted by parents, and associated with greater family engagement in the interventions.
Methods
The Connect for Health study was a randomized trial that leveraged clinical and community resources and addressed socioenvironmental factors to improve childhood obesity outcomes. Children between 2 and12 years with a body mass index greater than or equal to the 85th percentile who received routine health care at 6 sites of a multispecialty pediatric practice in Eastern Massachusetts were recruited between June 2014 and March 2015 to participate in a 1-year study. Research assistants called parents of children referred to the study by their pediatrician to establish eligibility, obtain verbal consent, and complete a telephone survey. Seven hundred twenty-one children were enrolled out of which 360 were randomized to the enhanced primary care + coaching arm (EPC + C) and 361 children were randomized to the EPC arm. Details of the study design, randomization, and recruitment are described elsewhere. 24 Study activities were approved by the Partners Healthcare Institutional Review Board. The trial has been recorded in clinicaltrials.gov.
Intervention
All participants in the study received enhanced clinical care. This included a computerized, clinical decision support alert during primary care visits that identified children with a body mass index greater than or equal to the 85th percentile, and 2 additional clinical decision support tools to assist clinicians in the management of children with overweight or obesity.24-26
Enhanced Primary Care Group
Participants randomized to the EPC group received monthly educational text messages that contained links to publicly available resources to support behavior change. We also emailed the EPC participants a resource guide to places in the community that support healthy living.
Enhanced Primary Care + Coaching Group
In the EPC + C arm, families received individualized health coaching. This included 6 study visits conducted in-person, by video call, or by phone. Health coach visits focused on behavior change through the identification and management of childhood obesity risk factors, providing family-centered care through motivational interviewing style counseling, and shared decision-making. Study health coaches were trained by the senior health educator (SP) and assessed regularly for consistency across visits. Details of this training and quality assurance protocol have been described elsewhere. 24 Health coaching was supplemented by twice-weekly text messages and referrals to community resources that support nutrition and physical activity. These resources were identified by a community resource map developed by the study team using GIS.
Health coaches worked with families to identify social and environmental contextual factors that support behavior change. They guided parents through goal-setting around obesity-related behaviors, shared educational materials and community resources, and discussed potential barriers to achieving goals and ways to overcome them. Following the visit, intervention materials to support the behavior change goals, and tailored to the child’s age, were mailed or emailed to the family. Communication was most often between the health coach and parent, but children were encouraged to participate when deemed appropriate by the parent.
Technology
Text Messaging
In the EPC + C group parents received twice-weekly text messages to support behavior change. The messages were delivered through a web-based platform supported by Mobile Commons, a mobile technology vendor. Text messages were sent on a schedule based on initiation of health coach contact, over approximately 1 year. The messages included (1) self-monitoring messages to help parents track their child’s health-related behaviors (sleep, physical activity, sugary drink intake, fast food consumption, screen time, and social and emotional well-being) and (2) skills training messages that delivered tips and encouraged families to work toward the targeted goal for each behavior. When parents replied to the self-monitoring message, they immediately received an automated, age-specific response that provided feedback on how their child was doing on that particular behavior, as well as motivational support to help them achieve the recommended goal (Figure 1). In order to avoid participants getting accustomed to similar messages sent on a regular basis, there were 73 different response options to be sent out depending on the question and the parent response. The overall design of the text message campaign in the EPC + C group was based on that developed for the Study of Technology to Accelerate Research (STAR) and is described in detail elsewhere. 27
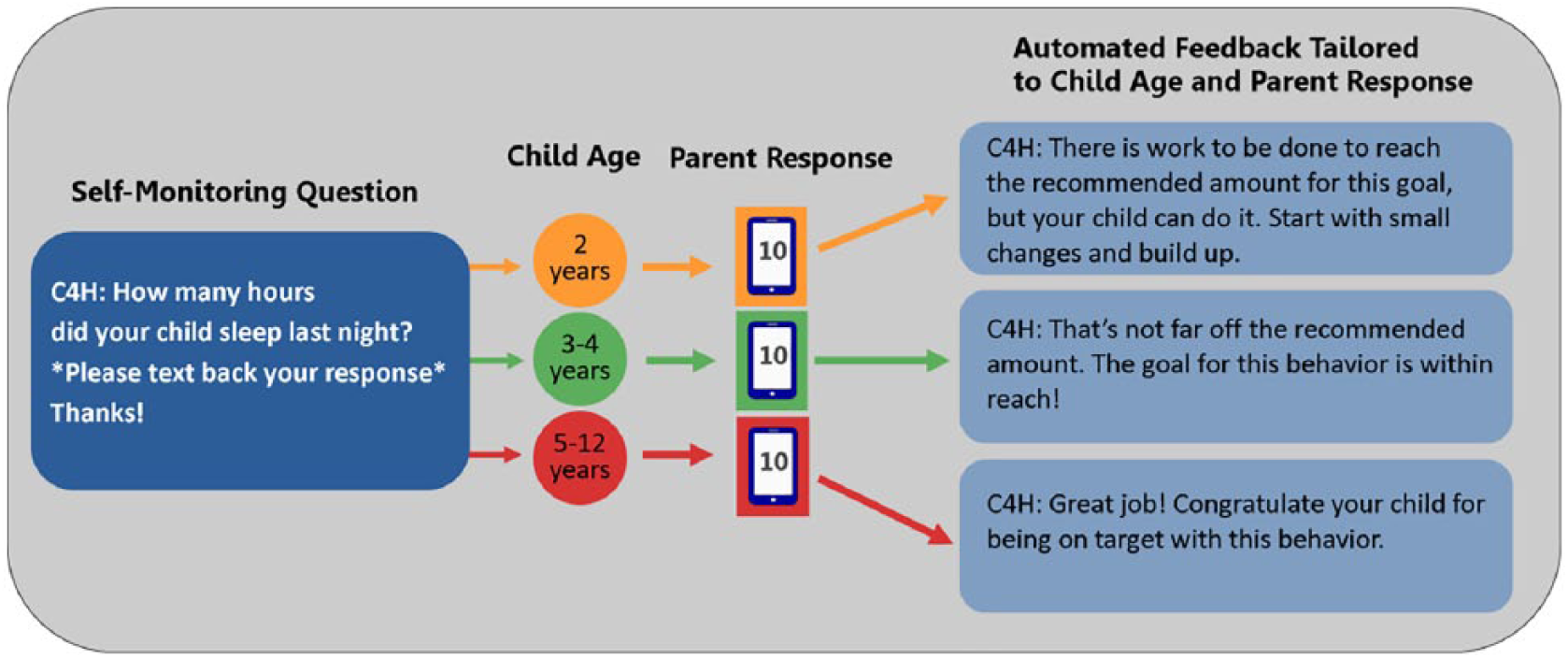
Interactive text messaging with automated tailored, age-specific feedback.
The Connect for Health text message campaign sought to build on the success of the STAR campaign and further improve on it. In addition to focusing on sleep, physical activity, sugary drink intake, fast food consumption, and screen time, the Connect for Health campaign included self-monitoring questions and educational information on social and emotional wellness. This improvement emerged from our qualitative work with “positive outlier families,” defined as the families of children who achieved healthier weight-related outcomes despite living in an obesogenic neighborhood. 28 Positive outlier families and our Parent and Youth Advisory Board emphasized the importance of getting support around their child’s social and emotional well-being. 24 The Connect for Health text message campaign also tailored the automated feedback responses to the child’s age. A parent’s reply to a health-related behavior question generated an automated response that reflected the recommended guidelines for their child’s age group (Figure 1).
The Connect for Health text campaign in the EPC + C group also provided information about available local community resources for physical activity, such as YMCAs and Boys and Girls Clubs, and healthy food establishments like farmers markets and supermarkets. Another notable addition to the Connect for Health text message program was that parents in the EPC group also had the option of receiving text messages. These parents were generally sent one message a month for the duration of the intervention year. Messages included links to publicly available resources to support behavior change, but no self-monitoring, individualized feedback, or tailored or direct support of any kind. Parents in both groups who declined text messages were given the option of being sent the messages by email.
Video Calls
Video calls were offered as an alternative option for participants in the EPC + C group who had the technology available and were interested in doing their health coach visits face-to-face, but not at the health center. We used Vidyo, a password protected, HIPAA-compliant software provided free of cost to the families (Figure 2), for all video calls. Vidyo can be downloaded and used on most personal computers, tablets, or smartphones, as long as they have a camera, microphone, and Internet connection. This made it an accessible option to most participants, given the high rates of cell phone and computer ownership among the general population. 29
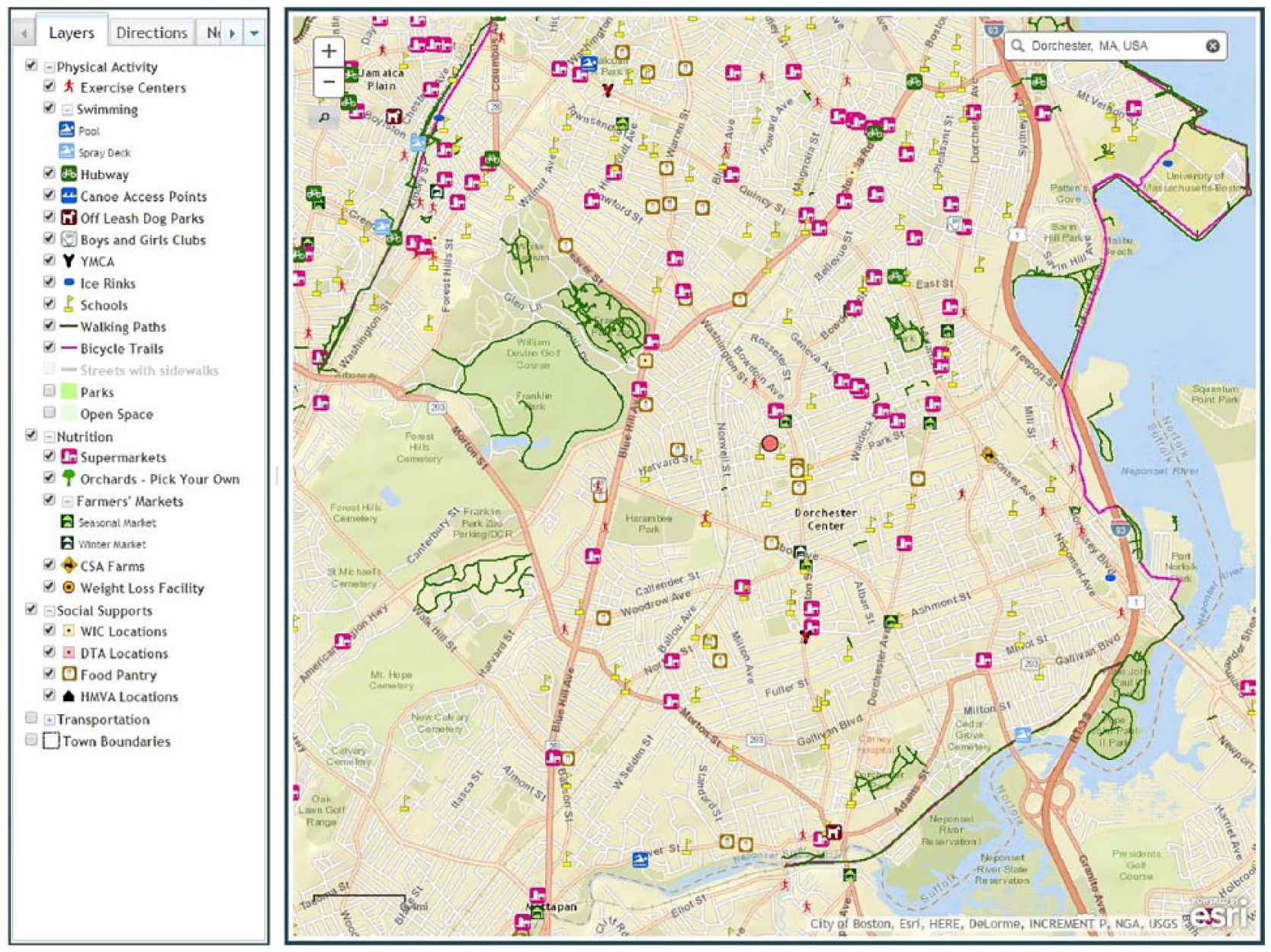
GIS mapping tool to locate neighborhood resources that support healthy living (farmers markets, supermarkets, fitness centers, parks, etc).
Community Resources
To further tailor the intervention, health coaches identified resources to support healthy eating and physical activity, as well as social support services, using an online community map developed for the study using GIS software. 30 Health coaches shared the map with families during the first study visit, and at follow-up visits as appropriate. Depending on the modality of the visit, the map was shown in person or through screen sharing, or referenced in conversation if on the phone. The map was created based on information gained from the positive outlier parent interviews, community stakeholders, and built environment specialists as to what was most important to include. At the visits, the health coaches mapped the distance from the participants’ residential address to built environment variables and they identified the nearest available trails, parks, playgrounds, open spaces, recreation centers, gyms, exercise programs, pools, farmers markets, and grocery stores and reviewed relevant findings with the participant (Figure 3). As a nontailored approach to sharing resources, we emailed the EPC group a general guide to resources for healthy living based on the location of their health center and surrounding communities.
Vidyo: free, password-protected, HIPPA-compliant software, compatible with most computers, tablets, and smartphones.
Measures
We asked the parents of children in both groups to complete 2 surveys: a baseline survey after consent was obtained and a follow-up survey at the end of the 1-year intervention. Survey questions collected demographic information and child health behaviors. The outcomes assessed in the follow-up survey at 1 year included parents’ satisfaction with the content of text messages and their satisfaction with the information about community resources for physical activity and nutrition. Parents who met with a health coach by video call were also asked about reasons they would recommend a video visit to others, satisfaction with the use of the technology, and about any technical problems they encountered during video call visits. Parents who did not complete a video call were asked about reasons for not using the technology. The specific questions asked to parents in the intervention arm were the following: (1) How satisfied were you with the content of the Connect for Health text messages/emails? (2) How satisfied were you with the information you received about resources in your community as part of the Connect for Health study? (3) Have you completed at least one video call with your health coach? If no . . . Why didn’t you meet by video call? (4) During your video visits, did you experience any technical problems? (5) What, if any, are the reasons you would recommend a video visit with your health coach to a friend or family member? We also assessed several process measures including visit completion, visit completion mode, and participation in the text message campaign.
Statistical Analysis
Descriptive statistics (means and standard deviations for continuous measures and percentages for categorical measures) were calculated for participant characteristics at baseline and for participant satisfaction at 1-year follow-up.
Results
Characteristics of Study Participants
A total of 721 participants were enrolled in the Connect for Health study, out of which 360 were randomized to the EPC + C group. Baseline parent and child characteristics of participants in the EPC + C arm at intake is shown in Table 1. The mean (SD) age of the enrolled children was 8.1 (3.0) years. Nearly all parents owned a cell phone (99%), and 91% who owned a cell phone reported to text once a day or more.
Baseline Characteristics of Study Participants in the Enhanced Primary Care + Coaching Group.
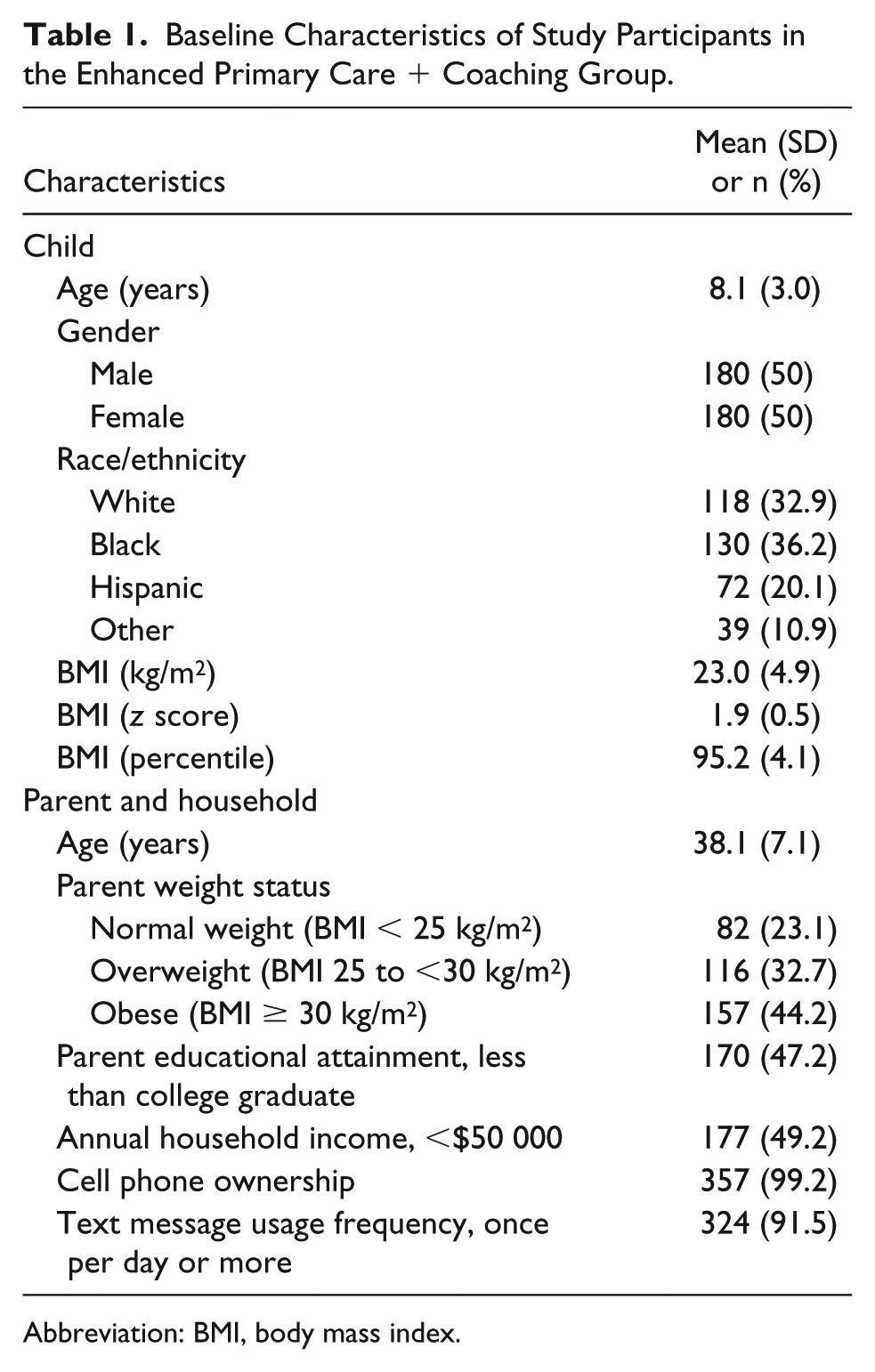
Abbreviation: BMI, body mass index.
Participant Enrollment, Engagement, and Satisfaction
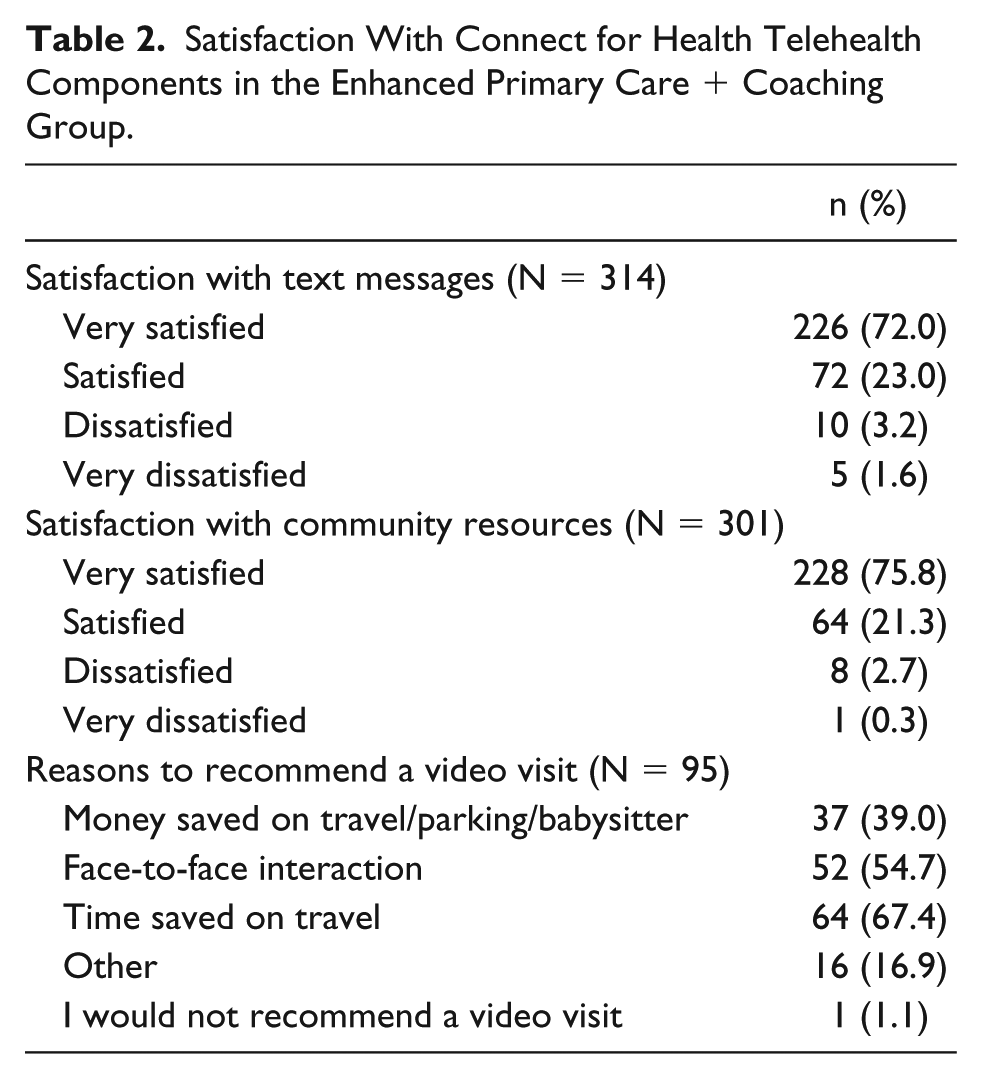
Of the 360 participants in the EPC + C group, 336 (93%) enrolled in the text message program. The rest opted to be sent the messages by email, with the exception of only one participant who declined both texts and emails. Of the total participants who requested texts, 99% responded to at least 1 self-monitoring question and 61% responded to more than half of the 46 text questions sent. At the end of the intervention year, 314 (87%) participants completed the follow-up survey. Of those, 72% reported being very satisfied and 23% satisfied with the content of the text messages.
The study intended to deliver 6 health coaching contacts, including an introductory phone call followed by 5 structured visits conducted by phone, video call, or in-person. The initial phone contact was completed by 98% of parents. Following that call, 87% of parents completed at least 1 visit. For the first health coaching visit, 23% of the visits were conducted by video call, 69% by phone call, and 8% were in person. Subsequent visits were by phone or video call only. For the second visit, 80% of visits were conducted by phone and 20% by video call, whereas for the third visit, 84% were phone calls and 16% were video calls. For both the fourth and fifth visits, 86% percent of visits were phone calls and 14% were video calls.
Video calls were used as a mode of health coaching visit at least once by 28% of parents. Of those who used it, 98% reported that they would recommend this method of communication for health coaching visits. Parents found video calls beneficial for saving time on travel (67%), promoting face-to-face interaction (55%), and saving on babysitter, parking, or travel expenses (39%). While the majority of the parents (65%) did not report any problems with video call visits, a few reported problems with downloading the software (4%), logging into the software (11%), remaining connected during the visit (19%), being heard (9%) or being seen (6%) during the video call. For parents who never completed a video call (72%), 23% felt phone visits would be easier, 19% reported not having a compatible device to use with Vidyo, and 5% were not comfortable using the technology. Nine percent of the parents who did not meet by video call reported having tried Vidyo and encountered technical difficulties that prevented them from completing the visit using that technology.
The GIS community resource map was shared with the EPC + C group parents during the first health coaching visit and at subsequent contacts as needed. The majority of parents were very satisfied or satisfied with the information provided about community health resources (97%). Table 2 summarizes the satisfaction of the parents with the different telehealth modalities in the Connect for Health EPC + C group.
Satisfaction With Connect for Health Telehealth Components in the Enhanced Primary Care + Coaching Group.
Discussion
In this study, we used 3 modalities of telehealth (interactive text messaging campaign, video call, and community resource map using GIS technology) to enhance a randomized trial to reduce childhood obesity. We found that that incorporating digital technology to provide parents with tailored behavior change support is feasible, well accepted by parents, and associated with greater family engagement in the interventions.
Telehealth has the potential to be a feasible, cost-effective, and wide-reaching option for weight management programs.31,32 Studies using telehealth to manage obesity have shown an overall improvement in the well-being and treatment satisfaction of participants, and positive effects on eating behaviors, physical activity, and decreasing screen time.5,33 As guided by prior research, the use of telehealth in our study incorporated the components recommended for a technology-based weight management intervention that included self-monitoring, counselor feedback and communication, social support, and an individually tailored, structured program. 34 Digital technology was used to support communication with patients by (1) making face-to-face visits more accessible through video calls, (2) allowing self-monitoring of behaviors via text message to further encourage change, and (3) as a reference tool in the form of neighborhood mapping to identify community resources that can support healthy behavior change. Our findings indicate that parents were generally satisfied with the use of tailored behavior change tools supported by telehealth technologies. This suggests that the addition of telehealth modalities in a pediatric weight management intervention is both feasible and acceptable.
Telehealth interventions also have great potential because they are deliverable via widely accessible devices such as smartphones, tablets, and home computers. According to a 2016 survey, 90% of adults in the United States reported using the internet at least occasionally and 77% of adults reported owning a smartphone. 29 With rapidly increasing rates of electronic device ownership, telehealth weight management interventions offer a promising way to reach a greater number of individuals at a lower cost. We observed a high level of participant engagement and satisfaction with our interactive text messaging campaign. The high response rate suggests that text messaging can be used as a method for boosting self-monitoring, which is an important component in a technology-based weight management intervention. 34 This has been shown in previous studies as well.9,12,27
Telehealth also offers a convenient approach to meet with a multidisciplinary weight management team without the need to travel to a health center. This in turn can lead to greater program adherence to an intervention and successful long-term weight control. 35 According to participant survey responses, meeting health coaches by video call saved money and time. It also allowed for face-to-face interaction, which may foster greater trust and establish a stronger relationship to support behavior change. Video calls may also reduce the likelihood of missing study visits, leading to decreased attrition rates, a common barrier to success in pediatric obesity programs. 36
Our intervention was strengthened by the use of telehealth to support behavior change. It enhanced the tailored nature and family-centeredness of our intervention by allowing for personal preferences in mode of communication with health coaches, age-specific automated feedback to parent responses to text messages, and the identification of neighborhood-specific resources to share with families. The study was also strengthened by having been informed by qualitative data collected from positive outlier patients and their families to inform our study practices. 24 This helped us better understand the ways an intervention can best support parents as they work to help their child with behavior change and weight management.
Studies have shown that human support and a personalized approach is important for enhancing engagement and outcomes in telehealth interventions.34,37 To this end, while using digital technology to support our participant communication, study participants met with trained health coaches regularly who counseled and motivated them to set goals and develop strategies to achieve positive weight-related outcomes. At follow-up visits, health coaches checked in with parents on progress toward goals, barriers encountered, and the use of community resources previously discussed. These conversations strengthened rapport and encouraged patient engagement and adherence.
As with any other technology-based intervention, the use of telehealth has limitations. While using text messaging is generally low cost, some cell phone plans charge for texts sent and received. Since this may have deterred some people from enrolling in our text message campaign, we offered our messages via email as an alternative option, which some participants requested. Another limitation was that there was no way of knowing if participants actually received all the text messages we sent. However, 99% of participants who were sent texts responded to at least 1 of them, which indicates messages were received. And finally, our text messaging campaign was only in English. This limits the generalizability to a non-English-speaking population. In Connect for Health, being comfortable reading and speaking English was an eligibility requirement, but the ability to communicate in and translate study components to other languages would be beneficial for future studies. Video calls offer great potential for provider and patient communication. However, technical issues can arise, such as difficulties in downloading or using the software, device incompatibility, quality of the video image or audio transmission. Some participants may also have concerns about sharing personal health-related information over the Internet, despite Vidyo being password-protected, HIPAA-compliant software. As such, Vidyo offers greater security than video calls via programs like Skype or FaceTime, but it is less commonly used, which may pose a barrier to patient use.
A final potential limitation is that while we validated the resources included in our mapping tool prior to the start of the study, using it over time would require additional resources to ensure it remains accurate and up to date. The benefits of a mapping tool may also not be generalizable to a population outside the area studied.
Conclusion
This study aimed to use telehealth technology to deliver and support behavior change by the use of interactive text messaging, meeting health coaches by video calling, and a GIS community resource mapping tool. High patient engagement and reported satisfaction with the above-mentioned telehealth modalities is encouraging and suggests telehealth as a feasible tool to provide high quality care for children with obesity.
Author Contributions
NB made the initial draft of the manuscript and assisted in data analysis. SNP also assited in making the initial draft of the manuscript. CMH assisted in reviewing and revising the manuscript. MWG carried out the data analysis. EMT conceptualized and designed the study and reviewed and revised the manuscript.
Footnotes
Acknowledgements
The authors would like to thank the providers and staff at Harvard Vanguard Medical Associates for their ongoing collaboration in pediatric obesity research efforts. We would like to thank the Connect for Health clinical research coordinators and health coaches for their assistance with the study. We thank the parents and children who serve on our advisory boards and offered their input to help shape the intervention. And lastly, we thank our community partners, Cooking Matters and multiple Massachusetts YMCAs, for making their resources available to study participants.
Authors’ Note
All statements in this report, including its findings and conclusions, are solely those of the authors and do not necessarily represent the views of the Patient-Centered Outcomes Research Institute, its Board of Governors, or Methodology Committee. Natasha Bala is now affiliated with SUNY Downstate Medical Center, Brooklyn, NY, USA.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported through a Patient-Centered Outcomes Research Institute Award (IH-1304-6739). Dr Taveras was also supported by a K24 grant (DK10589) from the National Institutes of Health. The funding sources for this study had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.