
Abstract

Case Report
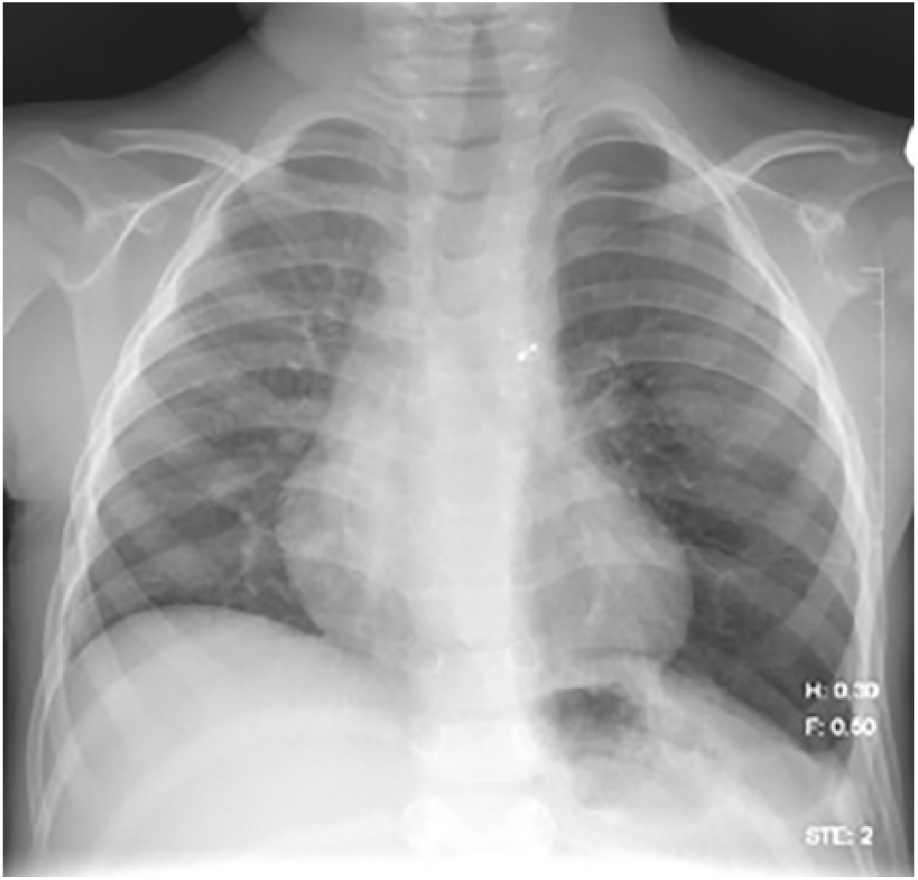
A 20-month-old male presented to his pediatric clinic for a well-child visit. His mother reported that he was doing well besides a cough which had been present for 2 to 3 months and had worsened after a recent upper respiratory tract infection. On further questioning, the mother stated that he had also experienced some nasal congestion and constipation. Occasionally, she noticed that he had “fast breathing.” She denied fever, wheeze, stridor, decreased activity, and vomiting. He had been eating well with no difficulty taking liquid or solid food. Past history was significant for congenital diaphragmatic hernia (CDH; Bochdalek’s type), repaired on the fourth day of life. He also had a history of pulmonary hypertension, which had been well controlled with sildenafil. He did not have a history of recurrent wheezing and there was no family history of asthma. On physical examination, the patient appeared to suffer from poor weight gain, charting in the 5.46th percentile on the growth curve. The patient’s lungs were found to be clear to auscultation with no wheezes. He was playful and not in acute distress. After administering age-appropriate vaccinations, the decision was made to refer the patient to pediatric pulmonology for reestablishing specialty care and evaluation of his chronic cough. At the pulmonology clinic, only a week following, the patient exhibited mild occasional tachypnea with a respiratory rate up to 40 breaths per minute, minimal subcostal retractions, and an oxygen saturation of 98%. The child was playful and active. Auscultation revealed mild end-expiratory wheezes bilaterally and air entry was slightly decreased on the left side. Cardiac examination was unremarkable. The abdomen was flat and nontender, and the extremities did not exhibit any clubbing, cyanosis, or edema. Because of the patient’s significant past medical history, a 2-view chest X-ray was obtained to evaluate his cardiopulmonary status. The chest X-ray (Figure 1) revealed herniation of bowel into the left lung base with a shift of the cardiothymic silhouette and trachea to the right.

Chest X-ray showing recurrence of herniated bowel into left hemithorax with mediastinum shift.
Final Diagnosis
Recurrance of CDH.
Hospital Course
The patient was hospitalized and evaluated by pediatric surgery for hernia repair. After further evaluation, the patient was referred to another facility for CDH repair. He recovered well and was discharged without any complications. Follow-up at the pediatric pulmonology clinic after repair revealed a well child with resolution of tachypnea, chest pulling, and wheezing. Repeat chest X-ray at the clinic (Figure 2) showed the surgical correction of herniated bowel with appropriate positioning of the cardiothymic silhouette.
Chest X-ray showing resolution of Bochdalek’s hernia after surgical repair.
Discussion
A common presentation of an uncommon problem is challenging, especially in a busy patient care setting. In this case report, we demonstrated a case of recurrence of CDH in a child presenting with mild and nonspecific respiratory and gastrointestinal signs and symptoms. Although this patient’s complication was promptly identified and resolved, we have demonstrated that the presentation of recurrence can be quite insidious.
CDH is a rare condition often presenting in the newborn period with symptoms of respiratory distress and cyanosis. It occurs in 1 out of 2500 births with a mortality rate of 35%. 1 There are 3 different types of CDH, the most common of which is Bochdalek’s hernia. This type accounts for 70% of CDH and is caused by a defect in the pleuroperitoneal folds during the embryonic period. The other types of CDH are Morgagni-type hernia, an anterior herniation through the foramen of Morgagni (27% of cases), and septum transversum-type, a central herniation, which is the rarest (2%-3% of cases). 2 In all types, the intestines herniate into the thorax encroaching upon the space in which the lung or lungs should be developing. As a result, pulmonary hypoplasia and persistent pulmonary hypertension are almost always present in patients with CDH, and these complications pose significant morbidity and mortality in and after the newborn period. 1 The diaphragmatic defect is usually diagnosed by ultrasound in utero and so is swiftly and surgically repaired after birth.
Recurrence of a diaphragmatic hernia can often be overlooked due to nonspecific or even asymptomatic presentations of patients. 3 However, a missed diagnosis can have fatal consequences. Therefore, the purpose of this case report is to advise physicians to have a high index of suspicion for recurrence, if a patient with a past medical history of CDH presents even with seemingly benign respiratory or gastrointestinal symptoms. Recurrence of CDH is not common, occurring at a rate of about 12.9%. Risk factors of recurrence are those that reflect the severity of the hernia such as home oxygen requirement and use of a prosthetic patch for repair. 3 Our patient’s initial hernia was, in fact, repaired with a prosthetic patch, which is usually used for hernias too large for primary suturing.
Although presentation of CDH at birth includes symptoms of respiratory distress with a scaphoid abdomen and cyanosis, presentation of recurrence varies with severity and organ system. A review of case reports shows that the clinical spectrum of late-presenting and recurrent CDH can range from no symptoms, found incidentally, to cardiac arrest. 4 Although our patient’s recurrence was resolved without significant morbidity, previous case reports reveal the severity of possible consequences. One report demonstrates 2 patients who were diagnosed and treated for suspected lower lobe pneumonia after presenting with symptoms such as tachypnea and cough. The late diagnoses in these patients ultimately lead to the death of one of the infants. 5 Another case report shows children who were initially diagnosed with pneumonia, pleural effusion, or lung abscess. Only after autopsy were these children found to have been suffering from recurrent CDH. 6
Not only can patients with recurrent CDH present with respiratory symptoms, but they can also present with gastrointestinal symptoms. 4 Similar to our case, patients can have a seemingly benign symptom such as constipation or failure to thrive; however, patients can also present with a complication as serious as bowel strangulation or perforation. Cases of bowel strangulation and necrosis in CDH have been reported, which presented initially with only abdominal pain and vomiting. 7
Conclusion
Because of the rarity of recurrence of CDH, recognizing presenting signs and symptoms can be challenging. Unfortunately, late diagnosis and repair can have fatal consequences. As demonstrated in this case report, patients with recurrence can present with symptoms mistaken for a less serious etiology. Therefore, physicians should practice a high index of suspicion for recurrence when evaluating a patient with a past medical history of CDH. As seen in our patient, early recognition and prompt repair can avoid morbid consequences and yield a happy and healthy child.
Author Contributions
SE contributed to analysis, drafted the initial manuscript. SK contributed to conception and design, critically revised the manuscript, gave final approval.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.