
Abstract

Background
Actinomycosis is a bacterial infection often missed on diagnosis due to its variable presentation and the nonspecific signs and symptoms. Actinomyces spp are gram-positive, anaerobic, non–acid-fast and filamentous bacteria, found as part of the normal human oral, gastrointestinal, and genitourinary flora. Although rare, infections with Actinomyces spp most commonly occur in the orocervicofacial region. Middle ear and mastoid involvement have rarely appeared in the literature, with a recent review reporting less than 30 cases reported worldwide since 1946. 1
Actinomyces is often difficult to diagnose, but typically requires fulfillment of 2 out of 3 of the following criteria: positive culture, positive histopathology, or sulfur granules visible in the drainage or pus.2,3 As Actinomyces is difficult to grow in culture due to its anaerobic predilection and slow-growing nature, most diagnoses occur through histopathology. We present a case of actinomyces discovered in a 5-year-old male with mastoiditis diagnosed based on histopathology.
Case Report
A 5-year-old male presented to our hospital with a slow-growing painless mass and developing erythema behind his left ear, which was incidentally discovered during a haircut the week prior. The patient had experienced no systemic signs at home, including no fever, malaise, fatigue, upper respiratory symptoms, hearing loss, otorrhea, or otalgia. No medical history of significance was reported, including no history of recurrent otitis media or ear tube placement.
On physical examination, the patient had erythematous, bulging tympanic membrane and tender fluctuant mass behind the left ear with protrusion of the ear. Nontender posterior cervical and supraclavicular lymphadenopathy were also identified. Vital signs were all within normal limits, as was initial complete blood cell count and C-reactive protein drawn in the emergency department. Computed tomography scan of the head revealed coalescent mastoiditis of the left mastoid air cells with focal erosion of the lateral cortical bone and marked thickening of the periauricular soft tissues. An ENT consultation was requested and ampicillin/sulbactam was initiated. The following day, the patient was taken to the operating room for mastoidectomy and ear tube placement. During the surgical intervention, the surgeon noted postauricular abscess in the soft tissue from bone erosion through the mastoid. Also noted, the mastoid air cells were eroded with the presence of granulation tissue and yellow thick purulence with consistency similar to caseation. Middle ear effusion was drained, and tissue and cultures were obtained. Pathology evaluation of the specimen revealed multiple irregular fragments of edematous fibrovascular tissue with marked mixed acute and chronic inflammation. Present within the inflamed stroma were scattered irregular aggregates of granular basophilic material, surrounded by neutrophils (Figure 1). On high power, basophilic purple filamentous structures couple be appreciated (Figure 2). Grocott methenamine silver stain highlighted these filamentous structures, confirming morphologic feature consistent with Actinomyces spp (Figure 3). Culture results remained negative for greater than 1 week before finally returning with growth of Fusobacterium necrogenes, Prevotella bivia, and Bacteroides stercoris.
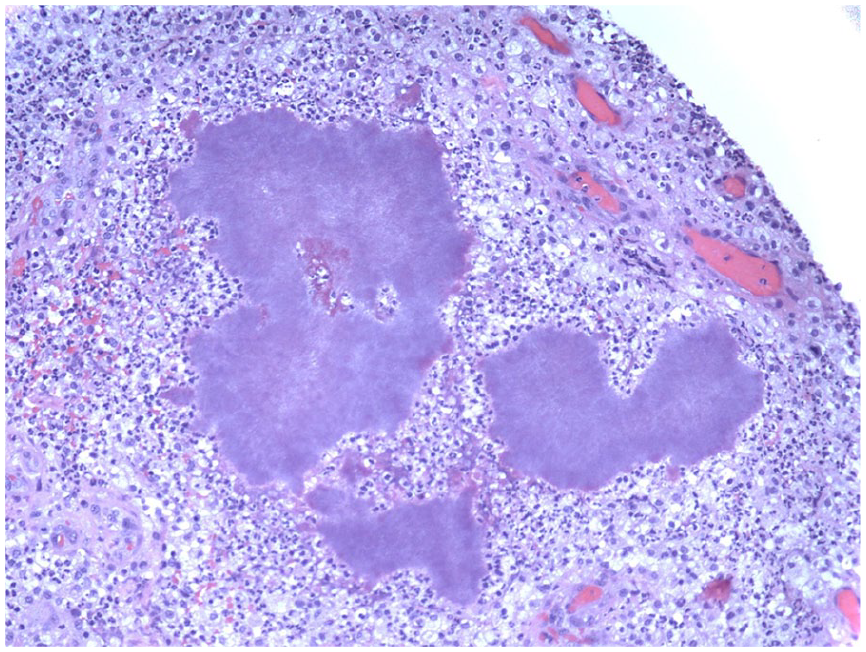
Basophilic (purple) aggregates within markedly inflames fibrovascular stroma (hematoxylin and eosin, 20×).
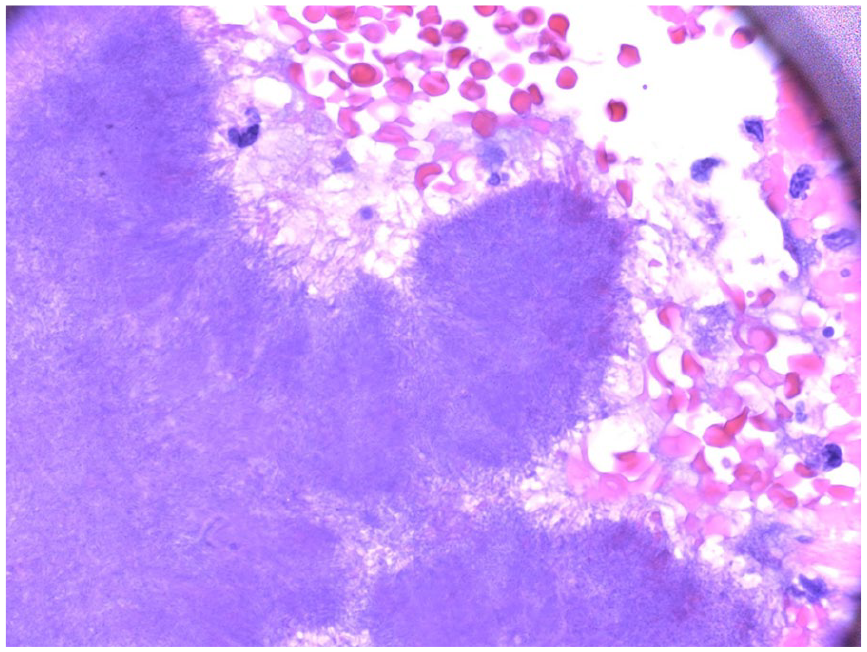
Vague filamentous structures around the periphery of the basophilic aggregates (hematoxylin and eosin, 100× oil).
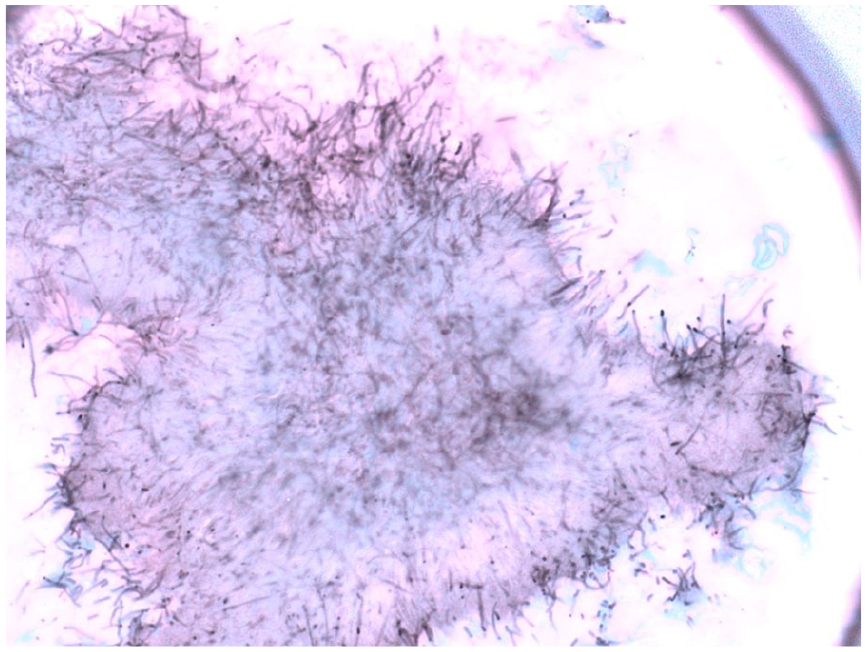
Grocott methenamine silver (GMS) stain demarcates and highlights the filamentous structures (GMS, 100× oil).
Since Actinomyces often occurs in immunocompromised patients and is increasingly reported in those with chronic granulomatous disease, we also obtained testing for neutrophil oxidative burst to test NADPH oxidase function, which returned normal.
After debridement, the patient remained in hospital to receive a total of 1 week of intravenous ampicillin/sulbactam, before being discharged home on high-dose oral amoxicillin (80-90 mg/kg/day) for a 6-month course, tapered to 50 mg/kg/day during the final month of treatment. The patient was followed closely with our Infectious Disease and ENT clinics.
On follow-up visits, wound site appeared clean and well healing, and mass had not returned. The patient had no additional signs of infection, including no fevers, ear pain, hearing loss, headaches, vomiting, or diarrhea. The only complication was mild scar hypertrophy of the surgical site, which improved with steroid injection by ENT during his third month of treatment. The patient remained without recurrence of infection of ear or surgical site and without hearing complication.
Discussion
Actinomyces was first discovered in 1878 by Israel. Actinomyces is a branching, filamentous gram-positive anaerobe found as a normal inhabitant of human oral flora. It is estimated that more than 90% of children have Actinomyces dwelling within their oropharynx by 1 year of age. 4 Actinomycosis, or infection by Actinomyces spp, most commonly occurs in the orocervicofacial region and typically occurs after a dental procedure or trauma in the oral region allowing the bacteria to enter the tissue, often in the setting of poor dental hygiene. Actinomycosis also presents more commonly in those with history of recurrent otitis media infections,5,6 and more often in men than women. Although this illness has been found to affect people of all ages and genders worldwide, it is predominantly a disease of adults. 4 Actinomycosis also occurs more commonly in those with immunocompromised states, including diagnoses such as chronic granulomatous disease. 7
Throughout the literature, orocervicofacial Actinomyces ranges in onset, from an indolent, slow-growing painless mass to a subacute, painful mass developing abscesses and draining sinus tracts. Typically, actinomycosis is not limited by anatomical barriers and fascial planes. Infection of the middle ear is hypothesized to occur by 3 possible routes: direct spread from the nasopharynx to the Eustachian tube (most likely), direct infection of the external auditory canal, or hematogenous spread.1,2,5
As mentioned above, actinomycosis is often difficult to diagnose and, thus, often goes improperly treated for a prolonged time. Though a positive culture is the gold standard for diagnosis, cultures for Actinomyces return negative in about 50% of cases. 7 Most commonly, diagnosis is made from histopathology showing abundant granulation tissue, and yellow-white, round granules with gram-positive, branching filaments oriented radially around the granules, as was found in our case. Granules may even be visible to the naked eye and found within pus and drainage. Our case additionally highlights the importance of obtaining pathology sample. The aid in diagnosis should the culture return negative, or should results not return for multiple days to weeks. Between 75% and 95% of the time, infections are polymicrobial, found in conjunction with other normal oropharyngeal bacteria including Bacteriodes, Eikenella, Fusobacterium, Prevotella, Haemophilus, Staphylococcus, and Streptococcus. 8 Like Actinomyces, many of these bacteria, which were found in our patient after monitoring cultures for over 1 week, are slow-growing, highlighting the need to follow cultures for extended duration of time.
Harvey et al first reported in the literature in 1956 that prolonged antimicrobial coverage with penicillin and surgery are the gold standard treatment of actinomycosis. 9 The greatest utility of surgical intervention may lie in breaking up the granulomatous regions to aerate the tympano-mastoid surface and, thus, disrupt the anaerobic environment in which the infection thrives.5,10 Many reported cases have conversely been successful with antimicrobial coverage alone, and one review found successful treatment without recurrence in up to 90% of cases. 11 For those with penicillin allergy, macrolides, tetracyclines, clindamycin, lincomycin, rifampin, and chloramphenicol have additionally shown treatment efficacy. The optimal duration of therapy is unclear, with recommended oral antibiotic courses ranging from 6 weeks to 18 months.9,12 Our patient was symptom and infection-free after 6-month course of therapy, though we cannot be sure if the treatment may have been equally as efficacious for an even shorter course of treatment as patient was symptom-free from the beginning.
Conclusion
With a mass in the orocervicofacial region, Actinomyces must remain on the differential diagnosis. Additionally, even with a negative culture, Actinomyces cannot be excluded. Pathology should be obtained in these cases to further evaluate for Actinomyces. Though penicillin is determinedly the treatment of choice, no consensus exists for optimal treatment duration. Most of the literature seems to agree that surgical debridement in addition to prolonged course of penicillin is most effective in preventing recurrence.
Author Contributions
S. Rosie Gellman is a resident on the Infectious Disease treatment team. She drafted the majority of the case report.
Andrew Milera is a resident on the hospital medicine treatment team who provided insight into the hospital course. He helped contribute to the drafting and editing process and approved the final manuscript.
Thomas S. DeNapoli is the pathologist who initially reviewed tissue samples to help make the correct diagnosis for the patient. He contributed through pathology review and providing high-definition slides and description for the case report. He approved the final manuscript.
Lisa M. Buckmiller is the ENT surgeon who operated on the patient. She contributed to the review of the manuscript, editing the manuscript, and surgical aspects of mastoiditis included in the report.
Luis A. Castagnini was the attending on the Infectious Disease treatment team who helped with initial literature review and provided treatment and follow-up for the patient throughout the course of the illness. He contributed to the editing of the case report and the final manuscript.
All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.