
Abstract

Introduction
The hepatopulmonary syndrome (HPS) is characterized as the triad of liver disease, pulmonary gas exchange abnormalities leading to arterial deoxygenation, and evidence of intrapulmonary vascular dilatations.1,2 The prevalence of HPS in adults is 4% to 29%; however, its prevalence and outcome in children is unknown. 3 There is currently no effective medical treatment. Liver transplantation is considered to be the definitive treatment. 1
Case Summary
An 11-year-old girl, born of third degree consanguineous marriage, was diagnosed with Wilson’s disease at the age of 9 years. She was on pyridoxine, penicillamine, and zinc chelation therapy and was admitted with complaint of fever, vomiting, loose stool, decreased oral intake, and decreased urine output. On examination, higher mental functions were normal and vital signs were stable with blood pressure within normal limits. Palmar erythema and grade III clubbing were present, with dusky hue of lips and face (see Figures 1 and 2). SpO2 was 86%, not associated with respiratory distress. There was no evidence of Kayser-Fleischer ring on naked eye and slit lamp examination. On systemic examination, she had hepatomegaly (liver: 5 cm below right subcostal margin) with span of 10 cm, firm in consistency, and splenomegaly of 6 cm firm in consistency. In view of clinical presentation, dengue was suspected; intravenous fluids were given and infusion rates were increased in view of hemoconcentration. Despite adequate fluid therapy, hemoconcentration still persisted. Routine laboratory investigations were suggestive of persistent polycythemia, thrombocytopenia, and leucopenia with hemoglobin 16 to 17 g/dL, hematocrit 50% to 60%, and platelet 50 000 to 70 000/µL (Table 1). However, serology for dengue was negative. The investigations are as follows.

Grade III clubbing.

Central cyanosis and vacuous smile.
CBC Trends.
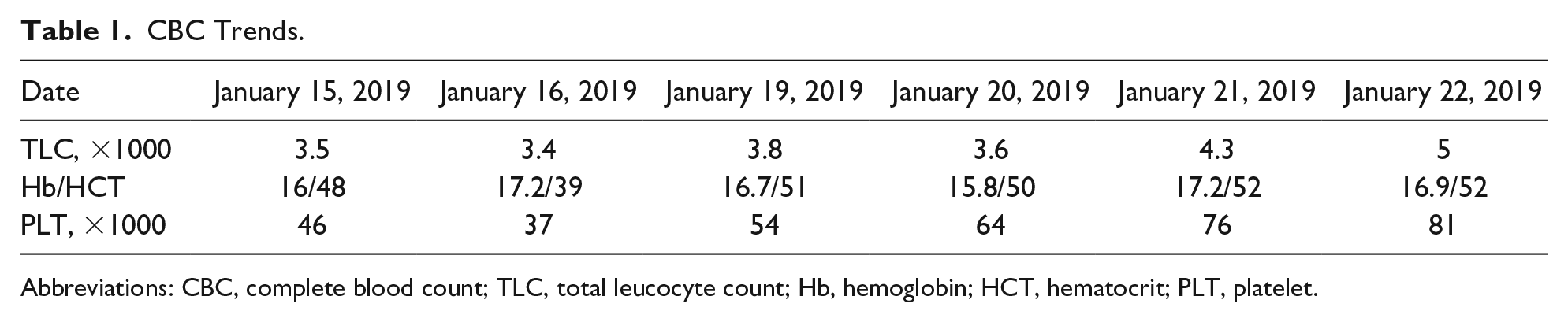
Abbreviations: CBC, complete blood count; TLC, total leucocyte count; Hb, hemoglobin; HCT, hematocrit; PLT, platelet.
Attributing bicytopenia to penicillamine toxicity, penicillamine was stopped and complete blood count monitored. 4 Polycythemia still persisted. It was observed that the child was comfortable with SpO2 of 85% to 90% and bluish lip discoloration with no respiratory distress or postural dyspnea. Saturation did not improve with supplementary oxygen; however, orthodeoxia was noticed. Arterial blood gas done on 2 consecutive days, which were suggestive of severe hypoxemia with PaO2 of 50.72 mm Hg and 47.7 mm Hg, respectively. The gradient showed P(A-a)O2 of 64.5 mm Hg (severe grade). 5 Bubble 2-dimensional echo showed severe grade intrapulmonary shunt. Abdominal ultrasound and hepatoportal Doppler scans revealed liver parenchymal disease, cholelithiasis, and mesenteric collaterals. Upper gastrointestinal endoscopy did not show any significant finding. Chest and abdominal computed tomography scans with contrast were done, to rule out cardiovascular and pulmonary causes of hypoxemia, which showed mesenteric collaterals. Computed tomography pulmonary angiography showed that pulmonary vasodilation could not be ruled out. The child was diagnosed as a severe case of hepatopulmonary syndrome type II with P(A-a) gradient ≥15 mm Hg and a PaO2 between ≥50 mm Hg and <60 mm Hg on room air, labeled as a candidate requiring liver transplantation. Macroaggregated albumin scan could not be done due to financial constraints. Prognosis and requirement of liver transplantation in near future was explained to parents and family.
Discussion
Hepatopulmonary syndrome is a rare but serious complication of chronic liver disease, and current knowledge in pediatric HPS is mainly based on case reports or small series of case reports. Three mechanisms are thought to play a role in the impaired oxygenation of venous blood as it flows through the pulmonary circulation: ventilation/perfusion mismatch, intrapulmonary shunting, and limitation of oxygen diffusion. 6 The current treatment of these conditions is extrapolated from that in adults and is not sufficiently evidence based. 6 At present, there are no specific effective medical therapies. General measures include providing symptomatic relief, improving quality of life and exercise capacity, and facilitating liver transplantation if indicated. In patients with chronic hypoxemia and PaO2 <60 mm Hg, continuous supplemental oxygen to maintain the O2 saturation above 88% is indicated because chronic hypoxemia impairs quality of life and may contribute to mortality in HPS.
Staging of the severity of HPS is important because severity influences survival and is useful in determining the timing and risks of liver transplantation. 7 A classification of the severity of HPS (Table 2) based on oxygenation abnormalities in 4 stages is proposed.
Classification of Hepatopulmonary Syndrome Based on Oxygenation Abnormalities.
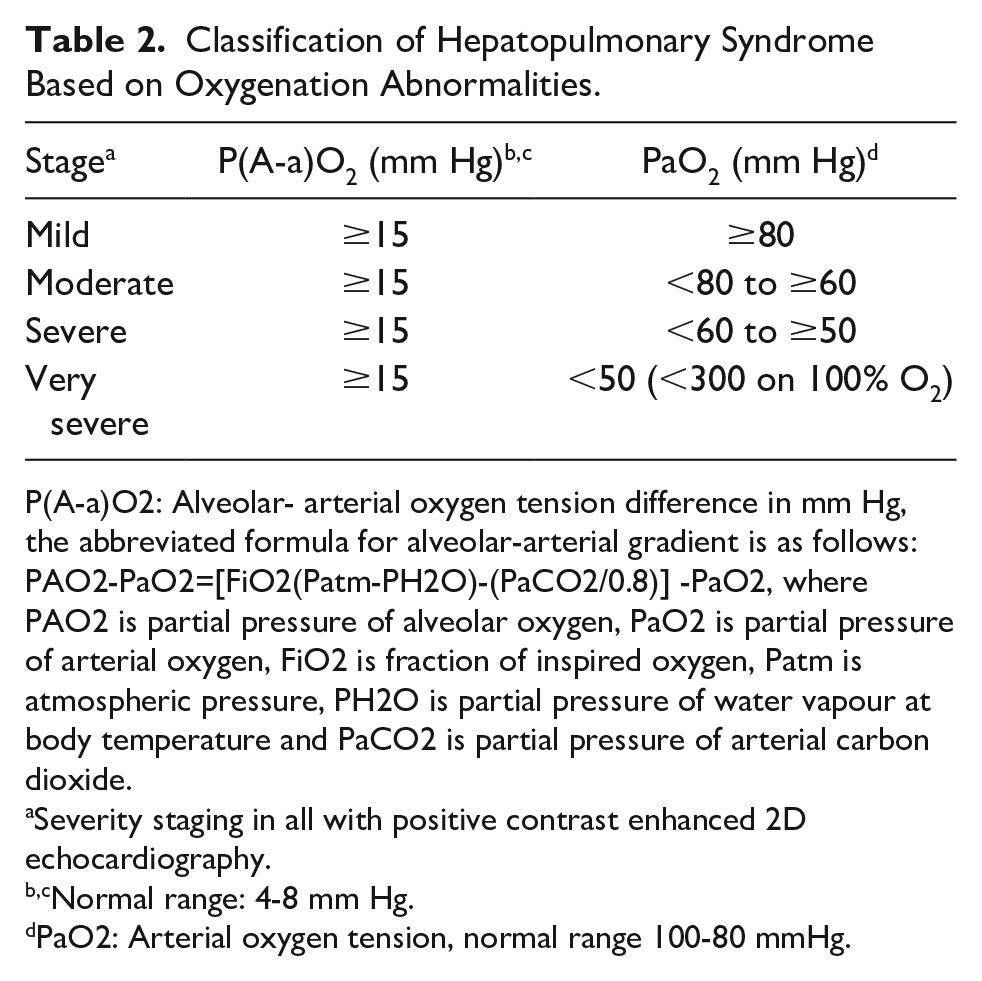
P(A-a)O2: Alveolar- arterial oxygen tension difference in mm Hg, the abbreviated formula for alveolar-arterial gradient is as follows: PAO2-PaO2=[FiO2(Patm-PH2O)-(PaCO2/0.8)] -PaO2, where PAO2 is partial pressure of alveolar oxygen, PaO2 is partial pressure of arterial oxygen, FiO2 is fraction of inspired oxygen, Patm is atmospheric pressure, PH2O is partial pressure of water vapour at body temperature and PaCO2 is partial pressure of arterial carbon dioxide.
Severity staging in all with positive contrast enhanced 2D echocardiography.
Normal range: 4-8 mm Hg.
PaO2: Arterial oxygen tension, normal range 100-80 mmHg.
Liver transplantation reverses the intrapulmonary vascular shunting and hypoxemia present in HPS over a variable period of time. 1 Poor outcome of patients with HPS without liver transplantation, as well as improved outcome and resolution of HPS after liver transplantation, has led to a reevaluation of the role of liver transplantation in HPS. Thus, progressive hypoxemia (PaO2 <60 mm Hg) because of HPS, which responds poorly to medical management, is now considered as an indication for liver transplantation. Liver transplantation results in complete resolution of gas exchange abnormalities in the vast majority of patients with HPS. 8
It is, therefore, suggested that a multicenter, multinational registry be developed for childhood HPS. The role of liver transplantation needs to be more clearly defined and applied to update the pediatric end-stage liver disease.
Author Contributions
SB and SS contributed to preparation of first draft/design. SB and PK contributed to collection of data and literature search. Conceptualization, acquisition, analysis and interpretation of data, critical revision of the manuscript for important intellectual content contributed by SS, SB, PU, PK, they also gave the final approval.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.