
Abstract
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) has a wide pediatric clinical spectrum. Initial reports suggested that children had milder symptoms compared with adults; then diagnosis of multisystem inflammatory syndrome in children (MIS-C) emerged. We performed a retrospective cohort study of hospitalized patients at a children’s hospital over 1 year. Our objectives were to study the demographic and clinical profile of pediatric SARS-CoV-2-associated diagnoses. Based on the clinical syndrome, patients were classified into coronavirus disease 2019 (COVID-19; non-MIS-C) and MIS-C cohorts. Among those who tested positive, 67% were symptomatic. MIS-C was diagnosed in 24 patients. Both diagnoses were more frequent in Caucasians. Both cohorts had different symptom profiles. Inflammatory markers were several-fold higher in MIS-C patients. These patients had critical care needs and longer hospital stays. More COVID-19 patients had respiratory complications, while MIS-C cohort saw cardiovascular involvement. Health care awareness of both syndromes is important for early recognition, diagnosis, and prompt treatment.
Introduction
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) was first identified in Wuhan, China, in December 2019. Since then, it has spread worldwide causing a wide spectrum of illness across age groups. Initially, children were thought to have a mild clinical course. 1 However, in May 2020, reports of a hyperinflammatory syndrome with multi-organ involvement emerged.2,3 The Centers for Disease Control and Prevention (CDC) defined this as multisystem inflammatory syndrome in children (MIS-C), which can result in severe illness requiring hospitalization and intensive care. 4 The virus also causes lower respiratory tract illness similar to adults. Clinicians were therefore met with 1 new pathogen but 2 distinct and serious disease processes. Luckily, we were able to draw from our experiences with Kawasaki disease (KD) and toxic shock syndrome (TSS) to manage MIS-C. In this study, we share a year-long experience with SARS-CoV-2 from an academic children’s hospital in the Midwest. Our objectives were to study the incidence, demographics, clinical characteristics, management, and outcomes of pediatric SARS-CoV-2-associated diagnoses.
Materials and Methods
We conducted a retrospective cohort study of hospitalized patients who met the following inclusion criteria: aged <20 years at admission; admitted between March 1, 2020, and February 28, 2021; and either a positive SARS-CoV-2 reverse transcriptase polymerase chain reaction (RT-PCR) or a positive SARS-CoV-2 serum antibody (immunoglobulin G).
Until June 2020, the definition of MIS-C was not established and availability of serological testing was limited. Therefore, admissions from March to May 2020 were reviewed for the following diagnoses: KD, febrile illness of >5 days, culture-negative sepsis, and vasculitis. Since these cases have syndromic similarities to MIS-C, they were scrutinized to see if they retrospectively meet MIS-C criteria.
Electronic medical records of patients were reviewed to obtain information on demographics, clinical characteristics, management, outcome, and follow-up. The study was approved by the institutional review board.
Once data collection was completed, the clinical syndromes were condensed into 2 groups: the first group consisted of patients who had tested positive for SARS-CoV-2, but did not meet MIS-C criteria, while the second group consisted of patients who met MIS-C criteria. For the purpose of this article, we called these 2 groups coronavirus disease 2019 (COVID-19) and MIS-C, respectively. Statistical analysis was done using IBM SPSS v27.
Results
In a 12-month period, 1277 hospitalized patients were tested for SARS-CoV-2 by RT-PCR. The positivity rate was 8.3% (n = 103). These patients were classified as the COVID-19 group. Twenty-four patients fulfilled the CDC diagnostic criteria for MIS-C. During early months of the pandemic, the number of positive inpatients were <5 per month. COVID-19 hospitalizations increased through the summer and peaked in December 2020. The incidence of MIS-C remained steady throughout the study period, with a peak in January 2021 (Figure 1).
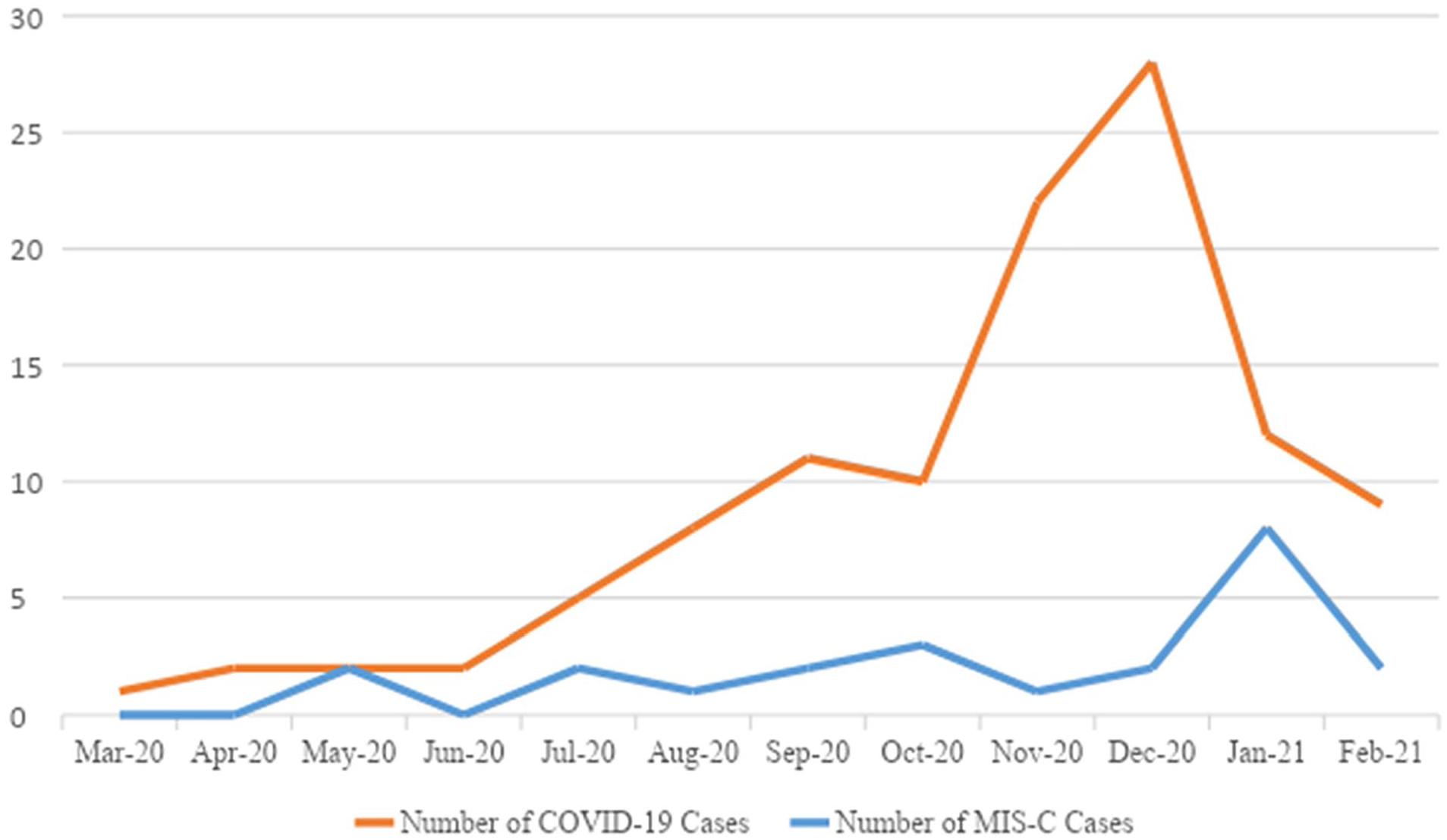
Trend of COVID-19 and MIS-C admissions.
The mean age of patients in both groups was similar (9.4 ± 6.5 years in COVID-19 vs 8.1 ± 4.9 years in MIS-C). The youngest child with MIS-C was 18 months old. About 25% to 35% of patients in both cohorts had preexisting comorbidities, mostly respiratory and neurological.
The sex distribution varied between cohorts. While we saw an almost equal distribution in the COVID-19 group (50.5% male), a male predominance was noted in the MIS-C group (58% male). The highest prevalence of both syndromes was seen in the Caucasian population (63% of COVID-19 and 54% of MIS-C).
Among those who tested positive by RT-PCR, 67% were symptomatic including isolated anosmia. Asymptomatic individuals were those screened prior to surgery and behavioral health placement. The symptom profiles of both diagnoses were starkly different (Figure 2). While fever was the most common presenting symptom (>90%) for both, MIS-C patients had longer mean duration of fever than COVID-19 group by 2.0 ± 0.1 days, and a higher mean maximum recorded temperature (38.7 ± 0.6 °C vs 39.4 ± 0.5 °C in COVID-19). Oro-mucosal involvement was common in MIS-C patients, whereas COVID-19 patients predominantly had respiratory and gastrointestinal symptoms. Interestingly, >25% of MIS-C patients experienced encephalopathy with hallucinations.
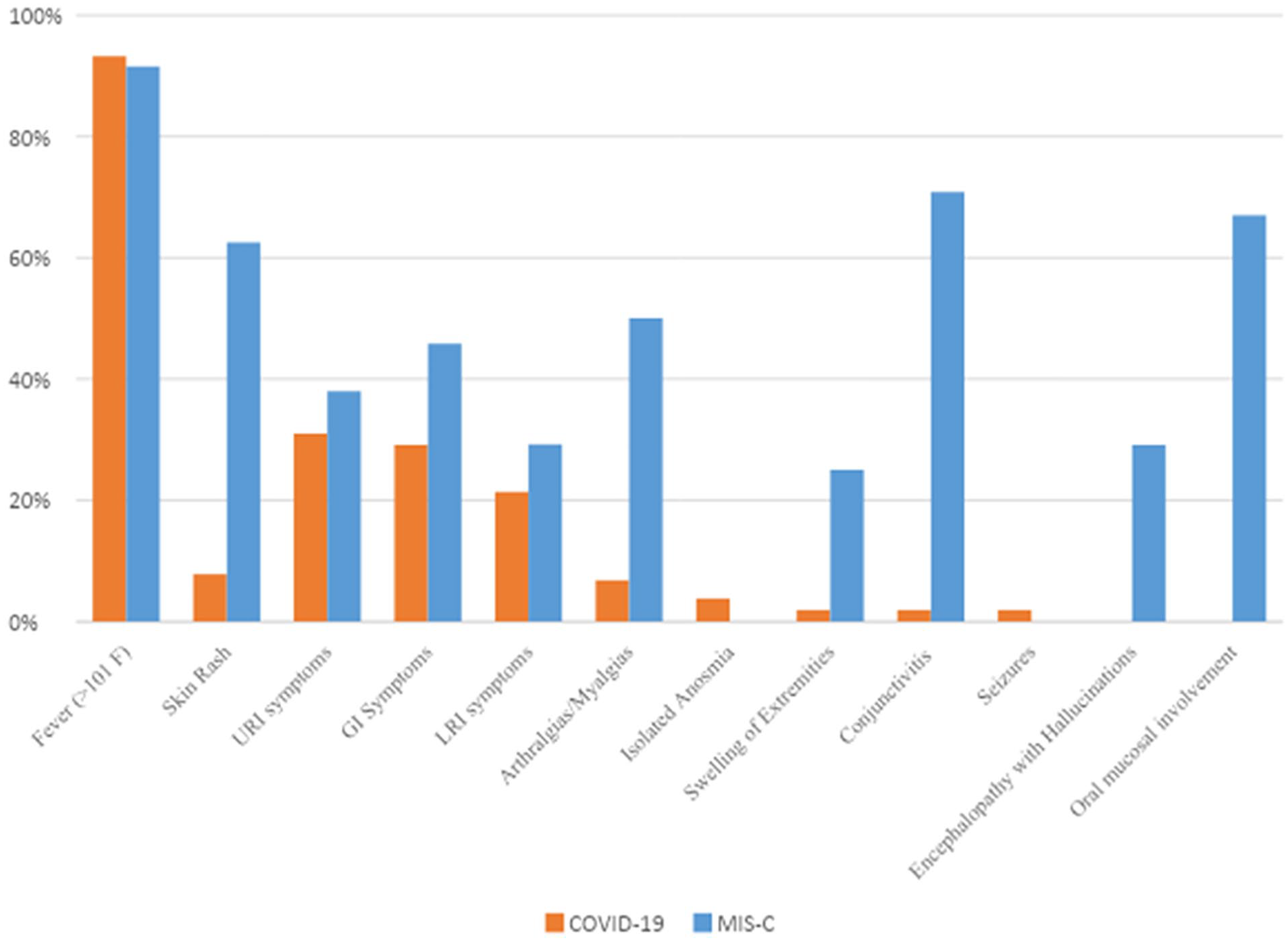
Comparison of symptom profiles.
Laboratory parameters between the 2 groups also showed a considerable differences, although none were statistically significant. The white blood cell count and inflammatory and hypercoagulability markers were several-fold higher in the MIS-C group (Table 1).
Comparison of laboratory results, multi-system involvement and medical management of COVID-19 and MIS-C cohorts.
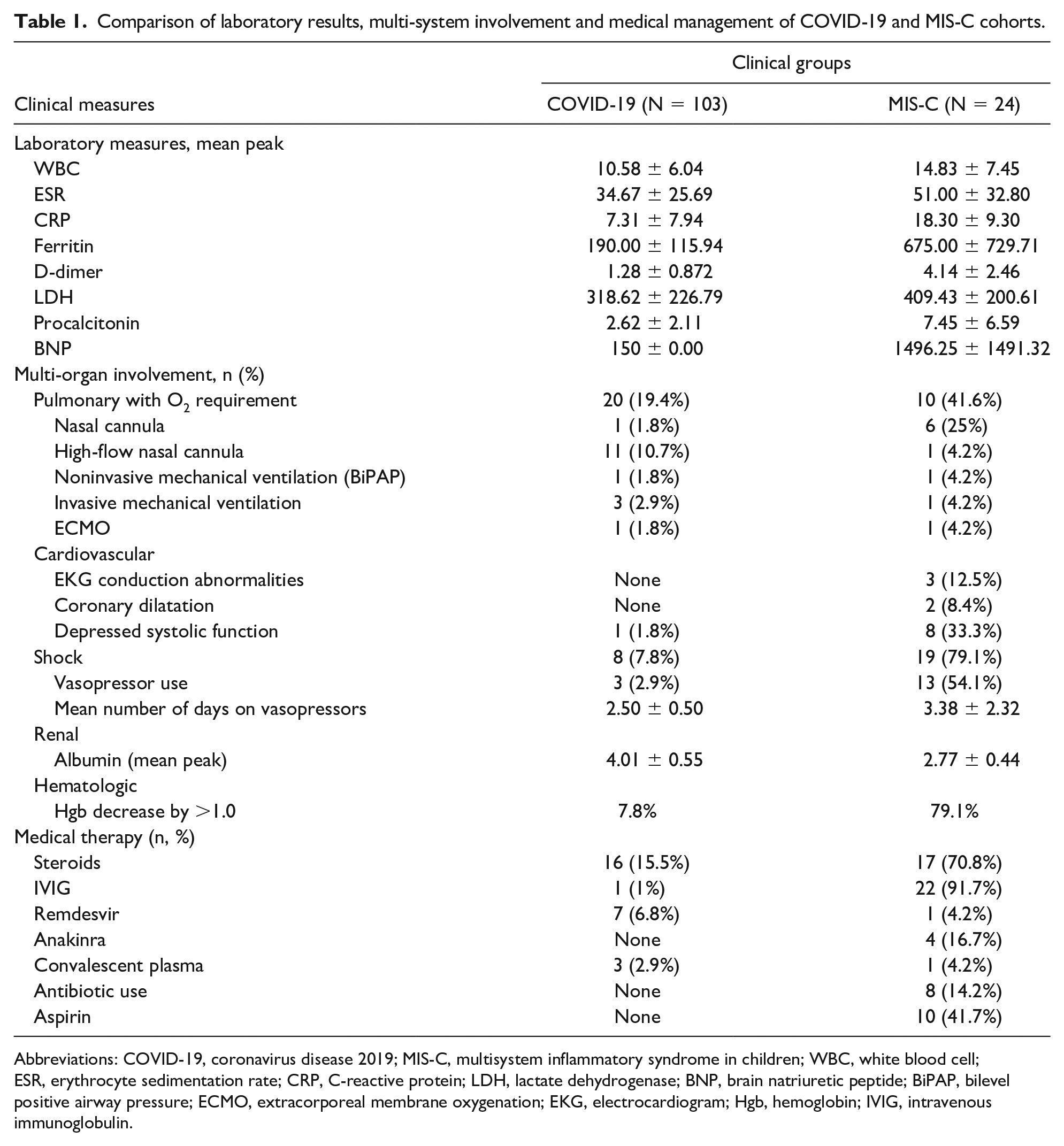
Abbreviations: COVID-19, coronavirus disease 2019; MIS-C, multisystem inflammatory syndrome in children; WBC, white blood cell; ESR, erythrocyte sedimentation rate; CRP, C-reactive protein; LDH, lactate dehydrogenase; BNP, brain natriuretic peptide; BiPAP, bilevel positive airway pressure; ECMO, extracorporeal membrane oxygenation; EKG, electrocardiogram; Hgb, hemoglobin; IVIG, intravenous immunoglobulin.
Patients requiring intensive care were 3-fold higher in the MIS-C versus the COVID-19 group (66% vs 19%, respectively). The difference in organ system involvement between both cohorts was statistically significant (P < .05). Respiratory involvement was common in the COVID-19 cohort, with most patients (65%) managed with noninvasive ventilation. Cardiovascular involvement was predominant in the MIS-C cohort. Rhythm abnormalities included first- and third-degree atrioventricular block. One case had junctional rhythm and elevated troponin without ST-segment elevation, raising concerns for myocardial involvement. A COVID-19-positive patient was diagnosed with Henoch-Schoenlein purpura. There were 4 cases of KD who were sero-positive for SARS-CoV-2, but did not meet MIS-C criteria.
The treatment modalities are listed in Table 1. Antivirals and convalescent plasma were used to treat COVID-19. Although treatment guidelines for MIS-C by the American College of Rheumatology were not established early in the pandemic, all cases were managed similarly that is based on severity of the illness and disease manifestations. First-line treatment being intravenous immunoglobulin and aspirin, second-line being steroids and anakinra reserved for severe refractory disease. All patients with MIS-C were discharged on low-dose aspirin for 4 weeks.
Most patients recovered well and were discharged home. The mean duration of hospitalization was longer in the MIS-C cohort by 4.2 days. All but one patient with MIS-C had good outcomes, irrespective of disease severity or management modalities. There was one death in the MIS-C cohort in a 13-year-old boy who presented in respiratory distress requiring mechanical ventilation then extra-corporeal membrane oxygenation. He died on day 2 of hospitalization from carotid dissection and decannulation following an episode of agitation. His only comorbidity was obesity (body mass index = 41.3 kg/m2).
We had limited follow-up data on the COVID-19 cohort. Since most MIS-C patients (62%) followed-up with our Rheumatology and Cardiology clinics, we had access to their data. In all 15 patients, periodic echocardiograms showed restored ejection fraction and no coronary artery aneurysms. Inflammatory markers had also normalized and aspirin was discontinued. At 6 weeks after discharge, 3 post-MIS-C patients described persistent symptoms including myalgia, fatigue, and “brain fog.”
Discussion
The knowledge surrounding pediatric COVID-19-related illness has evolved. Since the onset of the pandemic in March 2020, we have studied 127 children with SARS-CoV-2-related diagnoses. Our trend of fewer cases in spring, followed by an increase in summer and peak in late fall, was consistent with national trends. 5 The rise could be attributed to widespread availability of testing, relaxation of social restrictions, and reopening of schools. The peaks of COVID-19 and MIS-C were separated by 4 weeks. Other studies have also observed this lag.3,6 The lag coincides with the development of immunity and supports the hypothesis that MIS-C is a postinfectious syndrome. While the positivity rate in our population was relatively low (8.3%), some states reported rates as high as 34.4%. 7
Other studies observed the male predilection for MIS-C as well (52% male).5,8 However, our percentage of affected males was even higher at 58%. Although our hospital serves racially and ethnically diverse regions, there was a higher distribution of both COVID-19 and MIS-C in the Caucasian population. In contrast, the CDC reported that African American communities were disproportionately affected, but their figures did not include data from Missouri. 9
Acute COVID-19 infection presents like other respiratory viruses, with fever, exanthem, respiratory, and/or gastrointestinal symptoms. MIS-C has syndromic similarities to KD with prolonged fever, oro-mucosal, dermatologic, and systemic involvement. However, classic KD has a different epidemiology, typically affecting younger children (<5 years) commonly of Asian descent. In our study, the mean age for MIS-C was around 8 years and mostly affected Caucasians.
Consistent with its “hyperinflammatory” nature, MIS-C patients had markedly elevated inflammatory markers. Trending these markers in cases of suspected MIS-C could yield insight into disease progression and multi-organ involvement. Shock requiring vasopressor support is a hallmark of severe MIS-C.8,10 This life-threatening complication draws similarities to TSS. MIS-C seems to be a pathological interface of 2 well-recognized conditions, KD and TSS. This rationalized the convergence of both treatment modalities.
Although severe cases of both COVID-19 and MIS-C were seen, children responded well to prompt initiation of treatment and recovered well. We had only one death in the MIS-C cohort. The cause of death was hemorrhagic shock and not directly related to the disease.
Six weeks after recovery from MIS-C, 3 patients reported symptoms consistent with “long-haul/long COVID-19” like fatigue and chronic headaches. This term describes long-term sequelae of COVID-19 and resembles myalgic encephalitis/chronic fatigue syndrome. 11 These patients were treated symptomatically with academic accommodations at school. There is a case series of post-COVID-19 pediatric patients with “long COVID-19.” 12 Our study is the first to describe this syndrome in post-MIS-C patients.
There are limitations to our study. First, being a single-center study, the findings may not be generalizable. Second, our sample size is smaller compared with regions that grappled with a larger outbreak. However, ours is one of the few studies documenting the pediatric SARS-CoV-2 experience in the Midwest.
Since MIS-C is postulated to be an antibody-mediated immunologic phenomenon to prior COVID-19 infection, it would be interesting to observe for MIS-C-like presentations in vaccinated children. Future research should explore clinical syndromes like “long-haul COVID.”
In conclusion, our study of the pediatric spectrum of SARS-CoV-2 infections substantiates that most children contract mild forms of the infection and recover well; however, there is a small but significant risk of critical illness. While full recovery can be expected in both conditions, further long-term follow-up studies will be needed.
Footnotes
Acknowledgements
The authors would like to thank Howard Williams for his contribution.
Author Contributions
MK: Contributed to conception and design; contributed to acquisition, analysis, or interpretation; drafted the manuscript; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
LD: Contributed to conception and design; contributed to acquisition; drafted manuscript; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
HS: Contributed to acquisition; drafted the manuscript; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
AD: Contributed to conception and design; drafted manuscript; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
AM: Contributed to conception and design; drafted the manuscript; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
AT: Contributed to conception and design; drafted manuscript; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval was obtained from the Saint Louis University institutional review board (IRB) as well as the SSM Cardinal Glennon Children’s Hospital IRB.