
Abstract

Case Presentation
The patient is a 20-year-old female with a history of seasonal allergies and mild intermittent asthma. She presented to the emergency department with 2 months of a constellation of symptoms, including intermittent fevers, pleuritic chest pain, recurrent productive cough, decreased appetite, hoarseness, dysphagia, and weight loss. These symptoms began acutely and worsened over time. Her fevers did not have any regularity to onset or temporal pattern, and she did not have any concerning infectious exposures or recent travel.
She was evaluated several times for persistent symptoms, including a 2-week admission to a neighboring hospital. During this hospitalization, she underwent extensive rheumatologic, infectious, and oncologic/hematologic workup including computed tomography (CT) sinus, chest, and abdomen/pelvis; echocardiogram; bone marrow biopsy; and white blood cell scintigraphy, all of which were unremarkable. Symptoms eventually improved with steroid burst, and she was discharged on a steroid taper. Her symptoms returned with tapering of steroids, and thus she presented to this emergency department. Of note, the day prior to presentation, she developed new erythema and swelling of her right pinna.
On arrival, she was afebrile, tired-appearing, and tachypneic with splinting. Initial examination demonstrated decreased aeration at left lung base, tenderness to palpation along costochondral margins of anterior chest, erythematous and swollen right external pinna that was tender to palpation (see Figure 1), and bilateral tympanic membrane effusions. Laboratory evaluated demonstrated persistently elevated inflammatory markers and negative ANCA testing. CT chest showed new tree-in-bud opacities in the left lower lobe with mildly enlarged left hilar lymph nodes.
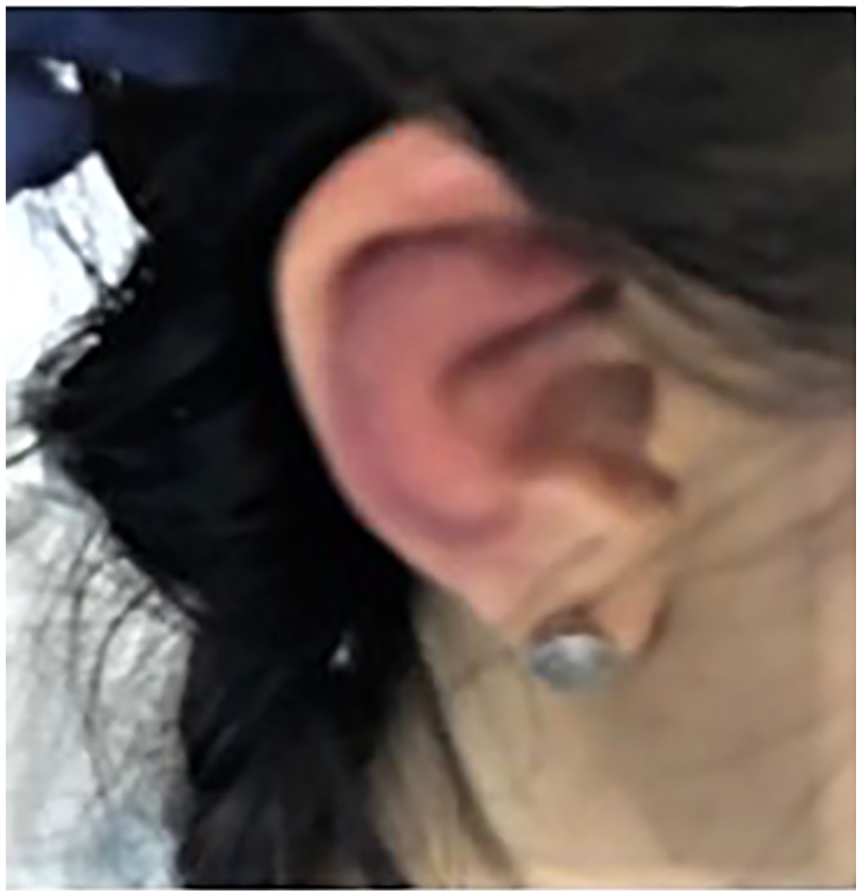
Right external pinna on initial examination.
Given her ear findings and hoarseness, the otolaryngology team performed a biopsy of her right external pinna and performed bedside laryngoscopy, the latter of which showed hemorrhagic and edematous left true vocal cord. They also noted mild saddle nose deformity on examination as well (see Figure 2). Given chest CT, a bronchoscopy was performed on hospital day 3, which was significant for edematous airways throughout, with moderate to severe tracheomalacia with severe bronchomalacia.

Saddle nose deformity.
Final Diagnosis
The aforementioned findings, coupled with a positive anti-type II collagen antibody test and pinna biopsy findings, clinched the diagnosis of relapsing polychondritis. Relapsing polychondritis is a rare autoimmune disease affecting cartilage that can have a delayed diagnosis at presentation given the nonspecific signs and symptoms. It is primarily a clinical diagnosis based on observed effects on multiple organs that contain cartilaginous components, including nose, auricular pinna, eyes, heart, and the tracheobronchial tree. 1 This disease pathogenesis is not fully understood but is known to involve both humoral and cell-mediated immune process. 2 As it can be difficult to diagnosis, it can also be difficult to treat. Steroid therapy is the mainstay option, with a range of other treatments depending on severity of disease and systems involved, though no standardized therapy exists. 1
Hospital Course
Her course was complicated by hypercarbic respiratory failure after bronchoscopy requiring intubation for 1 day. Intravenous steroids were initiated after bronchoscopy, with transition to oral prednisone after several days. Given the severity of airway findings, additional immunosuppression with methotrexate and infliximab was started. Her symptoms gradually improved on this regimen, and she was discharged in stable condition with close pulmonology and rheumatology follow-up.
Since her hospitalization, her symptoms have improved, though do worsen with steroid taper leading to concern that infliximab treatment is not sufficient, and her primary team is considering transitioning to tocilizumab.
Discussion
Relapsing polychondritis is a rheumatologic process that involves both humoral and cell-mediated immune processes, most notably with detectable autoantibodies to types II, IX, and XI collagen, with type II the most likely target given it is the base for almost all cartilage found in the body. 2 The patient had positive anti-type-II collagen antibodies, which further supported the diagnosis.
The prevalence of respiratory involvement in relapsing polychondritis is estimated to be 20% to 50%, with about half of patients having respiratory symptoms at diagnosis. 3 Mild forms of the disease can be treated with nonsteroidal anti-inflammatory drugs, but more severe forms require steroid therapy and immunosuppressants. 4 As can be seen with our patient, she required not only prednisone but also 2 other immunosuppressive agents given the severity of her disease. Biologic agents, such as infliximab, have demonstrated efficacy in inducing remission in patients with relapsing polychondritis, but studies are limited given rarity of this disorder. 2
Other diseases that can mimic her presenting symptoms include external otitis with her inflamed ear, in addition to other systemic diseases with overlapping symptoms including sarcoidosis and reactive arthritis. 5 A significant imitator of relapsing polychondritis is granulomatosis with polyangiitis, particularly given her saddle nose deformity and respiratory involvement. 5
Conclusion
This case underscores the importance of every aspect of a physical examination, as her finding of erythematous and swollen external pinna is what directed the team’s differential toward the diagnosis of relapsing polychondritis initially. Those patients without ear and nose involvement have been reported to be up to 5.6 times more likely to have a diagnostic delay over 1 year compared with those with these organs involved. 6 Though this patient did not have quite this long of a delay, her nonspecific array of symptoms did lead to not only some diagnostic delay but also a vast amount of testing and interventions in order to elucidate this disease. In this patient’s case, it is possible that earlier recognition of the importance of her ear findings could have led to deferring bronchoscopy for less invasive evaluation such as advanced imaging, avoiding emergent intubation.
Author Contributions
AR: Contributed to conception and design; contributed to acquisition, analysis, and interpretation; drafted manuscript; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
KA: Contributed to conception; contributed to acquisition and analysis; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
EJ: Contributed to conception and design; contributed to acquisition, analysis, and interpretation; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
The patient gave verbal and written approval for this case report.