
Abstract
Background. Ocular extraintestinal manifestations (O-EIMs) are one of the most well-known EIMs in patients with inflammatory bowel disease (IBD). This study aimed to identify the frequency of O-EIMs in children with IBD, referred to Mofid Children’s Hospital, Tehran, Iran, during 2014 to 2019. Methods. Children with IBD, younger than the age of 18 years, who were referred to an ophthalmologist, were included in this study. Results. Ninety-six patients with IBD were examined. Four patients had ocular manifestation of IBD. Two patients had complications due to treatment of IBD. The mean age of the patients was 11.25 ± 4.17 years (range: 5.5-17 years). The O-EIMs included 3 (50.0%) cases of anterior uveitis, 1 (16.7%) case of episcleritis, and 2 (33.3%) cases of posterior subcapsular cataract. Conclusion. O-EIMs are important in children with IBD. Therefore, it is recommended that annual screening for ocular complications be performed in all children with IBD.
Background
Inflammatory bowel disease (IBD) is a chronic inflammatory disease of the gastrointestinal tract with an unknown etiology. It includes Crohn’s disease (CD), ulcerative colitis (UC), and unclassified IBD. 1 This disease involves many other body organs, even before the gastrointestinal manifestations occur. Various extraintestinal manifestations (EIMs) affect approximately 16% to 24% of pediatric patients.2,3 Ocular EIMs (O-EIMs) are one of the most well-known EIMs. 4 The overall prevalence of O-EIMs in adults is estimated at 2% to 6%. However, the prevalence of ocular EIMs in children seems to be lower than adults, ranging from 0.7% to 1.8%.2,5-8
Both adults and children with CD are exposed to a higher risk of O-EIMs.8,9 The ocular manifestations of IBD include episcleritis, scleritis, and different types of uveitis. Other rare, but potentially severe ocular manifestations in patients with IBD include retinal vascular disease, optic neuritis, orbital myositis, and keratopathy. 8 So far, very limited studies, mostly case studies, have been conducted on pediatric populations with IBD. Therefore, there is a need for extensive research to increase our knowledge about the O-EIMs of IBD and to find new control strategies. This study aimed to identify the frequency of O-EIMs in children with IBD to prevent the development of permanent ocular complications by initiating appropriate treatment.
Methods
Children with IBD younger than the age of 18 years, who had undergone ophthalmologic examinations, were included in this study. They were referred to the subspecialty clinic of gastroenterology, liver, and nutrition of Mofid Children’s Hospital in Tehran, Iran, from September 15, 2014, to August 15, 2019. The patients’ clinical records were reviewed to extract data, including demographic data, disease type, duration of disease, steroid use, and disease activity, using the UC and CD activity indices. The laboratory tests included erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP). The ophthalmological examinations included eye movements, pupil assessments, cover tests, slit-lamp biomicroscopy, and fundoscopy. Visual acuity was not tested with regard to age and cooperation. The severity and type of uveitis, cataract, glaucoma, band keratopathy, cystoid macular edema, retinal involvement, vasculitis, papillitis, and orbital inflammation (myositis, lacrimal gland inflammation, and nonspecific inflammation) were recorded by the ophthalmologist. This study was approved by the Ethics Committee of Shahid Beheshti University of Medical Sciences.
Results
A total of 156 patients were diagnosed with IBD in this study. Sixty patients did not undergo eye examinations at the onset of diagnosis or during the disease course. In this study, 96 patients with IBD were examined, including 50 (52.1%) patients with UC and 46 (47.9%) patients with CD. Overall, 59 (61.5%) children were male, and 37 (38.5%) children were female. The mean age of the patients was 8.98 ± 4.56 years (range: 0.9-17 years). Six cases showed ocular complications, indicating a 6.2% prevalence of ocular involvement in these children. Of 6 patients with ocular complications, 4 (66.7%) were boys and 2 (33.3%) were girls. The mean age of these patients was 11.25 ± 4.17 years (range: 5.5-17 years). Also, the mean age of patients at the time of diagnosis was 4.67 ± 2.16 years (range: 3-9 years).
Out of 6 patients, 5 (83.3%) were diagnosed with UC (mean activity score: 68 ± 8.), and 1 (16.7%) was diagnosed with CD (activity score: 75). Four out of 6 patients (66.6%) had other underlying diseases, including amyloidosis (n = 1), arthritis with erythema nodosum (n = 1), spondyloarthropathy (n = 1), and central venous thrombosis (n = 1). The O-EIMs included 3 (50.0%) cases of anterior uveitis (2 cases of symptomatic uveitis and 1 case of asymptomatic anterior uveitis), 1 (16.7%) case of episcleritis, and 2 (33.3%) cases of posterior subcapsular cataract.
In terms of the therapeutic approach, 2 patients with posterior subcapsular cataract were prescribed high-dose systemic steroids (>15 mg) for more than 2 years. Human leukocyte antigen B27 (HLA-B27) was positive in 3 (50%) cases. All 3 patients with anterior uveitis were HLA-B27 positive. The mean ESR and CRP were 79.67 ± 25.67 and 53.33 ± 36.92 mg/L, respectively. All 6 patients showed elevated ESR and CRP. The clinical and laboratory data of children with ocular manifestations are summarized in Table 1.
Clinical and Laboratory Characteristics of Children With IBD and Ocular EIMs.
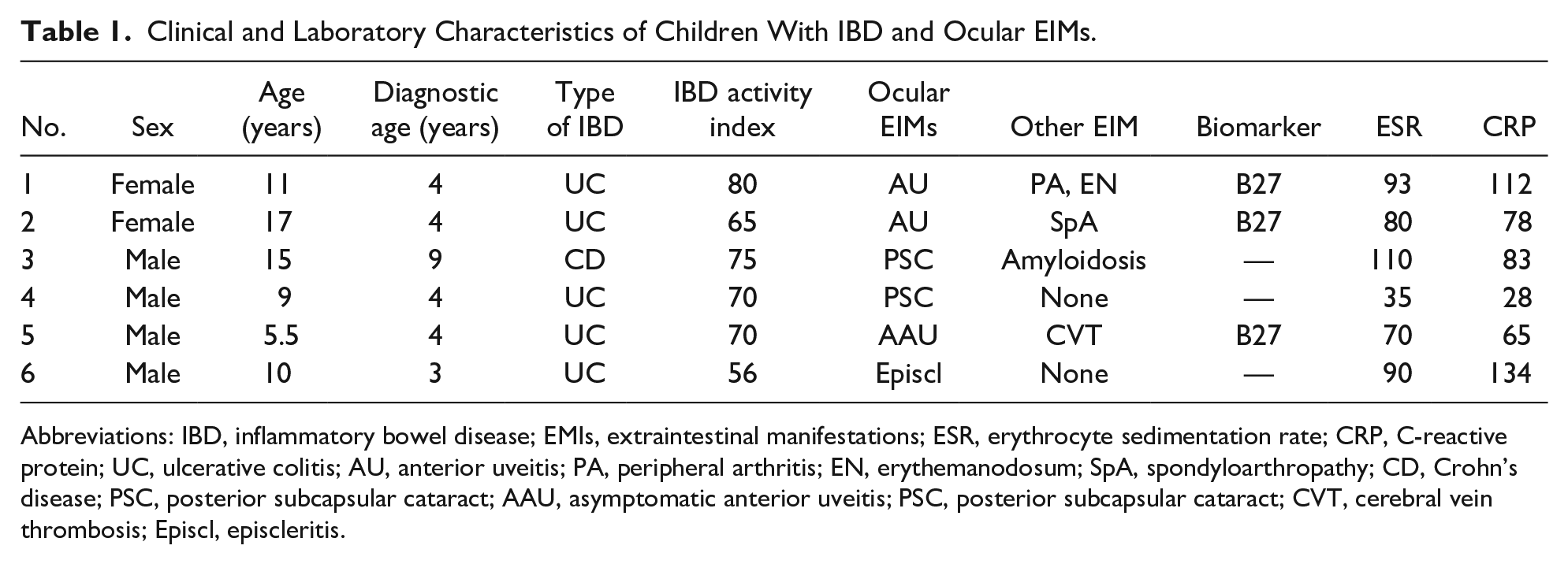
Abbreviations: IBD, inflammatory bowel disease; EMIs, extraintestinal manifestations; ESR, erythrocyte sedimentation rate; CRP, C-reactive protein; UC, ulcerative colitis; AU, anterior uveitis; PA, peripheral arthritis; EN, erythemanodosum; SpA, spondyloarthropathy; CD, Crohn’s disease; PSC, posterior subcapsular cataract; AAU, asymptomatic anterior uveitis; PSC, posterior subcapsular cataract; CVT, cerebral vein thrombosis; Episcl, episcleritis.
Discussion
IBD is a systemic inflammatory multisystem disease that is not limited to the gastrointestinal system, even in UC. In recent years, gastroenterologists have paid more attention to the EIMs of this disease. One of the reasons is the better control of gastrointestinal manifestations, along with the management of EIMs. Detection of O-EIMs is also particularly important in some cases, as it may change the treatment strategy.3,5 Studies on O-EIMs in children with IBD are very scarce and scattered. Routine eye examinations by ophthalmologists in children with IBD at the disease onset and later in the follow-up are not strictly recommended. Therefore, further studies, similar to the present one, may provide new guidelines for ophthalmologic examinations at regular intervals.
The prevalence of ocular involvement in children (0.7% to 1.8%) seems to be lower than adults (2% to 6%).2,5-8 In the present study, 96 patients with IBD were examined. Six (6.2%) cases showed ocular manifestations. Four cases were related to IBD complications, indicating a prevalence of 4.2% for ocular involvement in these children. The O-EIMs included anterior uveitis (n = 3), episcleritis (n = 1), and posterior subcapsular cataract (n = 2). In this regard, studies by Dimakou in Greece and Castro in Italy have reported prevalence rates of 0.62% and 1.3% for ocular complications, respectively10,11; however, the type of O-EIMs is unclear in these studies. Another study evaluated O-EIMs in 94 children with IBD. The prevalence of ocular manifestations was 7.4%, and the prevalence of ocular complications related to IBD was 1.06%. 7 Moreover, Saadah et al evaluated O-EIMs in 96 children with CD in Saudi Arabia, where 2 patients showed O-EIMs (2.08%). 12 Other cohort studies have also reported ocular complications in form of EIMs. In a study by Jose et al, 24 (1.5%) out of 1649 patients <18 years with IBD had ocular EIMs. 2
There are different types of uveitis (anterior, intermediate, and posterior). Anterior symptomatic uveitis and anterior asymptomatic uveitis are the most common types of IBD. Nevertheless, the exact prevalence of anterior uveitis is not defined. In the present study, anterior uveitis was the most common O-EIM. Two patients had symptomatic uveitis, and 1 had asymptomatic anterior uveitis, with prevalence rates of 2.08% and 1.04%, respectively. The 3 patients with UC were positive for HLA-B27. Also, these patients had an active intestinal disease with high inflammatory markers. Uveitis was improved with the step-up treatment protocol (azathioprine dose tapering and administration of biologic agents) for each of the 3 patients. In less recent studies, the high prevalence of subclinical uveitis (4.1% to 23.1%) was reported in children.13-15 According to a study by Jose et al, uveitis was the most common O-EIM in children with IBD. Iritis was detected in 16 patients, uveitis in 1 patient, and papilledema/corneal infiltrates in 7 patients. 2 Also, in a study by Naviglio et al, the prevalence of asymptomatic uveitis was 1.06%. 7 In adult patients, anterior uveitis was also predominant. 16
The most important corticosteroid-induced complications include posterior subcapsular cataract and increased intraocular pressure that need to be considered in children with IBD. Our 2 patients with posterior subcapsular cataract were under high-dose systemic steroid therapy (>15 mg) for more than 2 years. Immediate change of the treatment plan and substitution of steroid with biologic therapy were performed accordingly. In the 1-year follow-up, cataract had improved. Moreover, Malgarinos et al reported the case of a 25-year-old patient with exacerbation of the clinical symptoms of UC, who had received high-dose corticosteroid therapy for 2 years. Almost 2 weeks after starting the prednisolone treatment, he developed preterm posterior cataracts. Therefore, it was not possible to establish a safe dose or a specific duration of treatment with corticosteroids to prevent the development of cataracts. 17
In the study by Naviglio et al, one patient had posterior subcapsular cataract, associated with a long history of corticosteroid therapy. 7 Therefore, it seems reasonable to incorporate ophthalmological evaluations, including the measurement of intraocular pressure in children undergoing long-term systemic corticosteroids. On the other hand, episcleritis was only reported in a case report. 18 This patient was diagnosed with UC when he was 3 years old. Episcleritis was seen at the time of disease flare when he was 10 years old. Intravenous methylprednisolone was initiated, and 3 weeks later, episcleritis was improved.
The O-EIMs in the present study were more frequent in UC than CD (10% vs 2.17%), which is similar to the results of a cohort study by Greuter et al (25% vs 12.8%). 3 Generally, the O-EIMs can affect both CD and UC, whereas in a meta-analysis by Ottaviano et al, children with CD were at a higher risk of O-EIM than UC children, with an odds ratio of 2.7. 8 However, in other studies, the O-EIMs were more common in CD than UC.5,6,10,11,19 Also, in adult patients, the O-EIMs were more common in CD than UC. 20
The time of O-EIM emergence is unclear in children. Not all our patients were evaluated by an ophthalmologist at the time of diagnosis of IBD. However, in 6 patients with O-EIMs, the median duration of the disease was 5.5 years. Greuter et al reported a median uveitis onset of 7 years after IBD diagnosis. 3 The O-EIMs may also occur before the onset of gastrointestinal symptoms. According to a study by Jose et al, the prevalence of uveitis increases over time. 2 However, according to a study by Herzog et al, there was no significant relationship between the rate of uveitis and age at onset of diagnosis, which may indicate that the onset age of IBD did not increase the risk of uveitis. 21 Also, the ocular complications in 2 studies on French children with UC were almost similar at the onset of diagnosis (1.77% and 1.3%, respectively). However, in the follow-up, it was significantly increased (3.54% and 7.6%, respectively).22,23
Few studies have examined the association of O-EIMs with disease activity. In the present study, 5 patients had UC with moderate to severe activity. One of the patients had CD with moderate activity. Inflammatory markers, including ESR and CRP, were high in all patients. Because of the small sample size, it is not possible to conclude any relationship between the O-EIMs and disease activity. Uveitis is not classically associated with intestinal disease activity, while in a study by Vavricka et al 1 on adult patients, uveitis in CD had a significant association with disease activity.
The most common diagnosis of uveitis is HLA-B27-associated uveitis worldwide. 24 Acute unilateral anterior uveitis is usually a form of uveitis, associated with HLA-B27.25,26 Three of our patients were positive for HLA-B27, and all of them had UC. Two of these patients had acute unilateral anterior uveitis, and one had asymptomatic anterior uveitis; also, one of the patients had spondyloarthropathy. Generally, HLA-B27 exposes patients to different types of spondyloarthropathy, ranging from IBD to anterior uveitis. The proposed mechanism behind this association is change of the gut microbiome or dysbiosis. 27 In this regard, Daum et al reported one known HLA-B27-positive case of CD with asymptomatic uveitis. 13 On the other hand, there are IBD patients with HLA-B27-negative anterior uveitis. All of these findings suggest that HLA-B27 positivity may be important in small subgroups of patients with spondyloarthropathy and IBD, but not in all patients. 8
Conclusion
The O-EIMs are important in children with IBD. Therefore, it is recommended that annual screening for ocular complications be performed in all children with IBD. Children undergoing long-term systemic corticosteroid therapy should be followed-up more closely, as they are at a greater risk of ocular complications. It is also suggested that health care providers, as well as parents and caregivers, be educated about the increased risk of ocular complications in children with IBD.
Author Contributions
PR: Contributed to conception and design; contributed to acquisition; drafted manuscript; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
FAG: Contributed to design; contributed to analysis; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
ME: Contributed to conception; contributed to acquisition; drafted manuscript; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
VJP: Contributed to conception; contributed to interpretation; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
MM: Contributed to design; contributed to acquisition; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
RZ: Contributed to design; contributed to acquisition; drafted manuscript; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Written informed consent was obtained from the child’s parents (father) for the publication of this case series, including any data contained within.