
Abstract
Pediatric morbidity due to unintentional poison exposure is a significant burden on public health. We prospectively characterize patterns of unintentional poison exposure in a single pediatric emergency department, using a detailed computerized questionnaire for all unintentional injuries admitted during 2009 to 2017. Out of 71,765 visits due to unintentional injuries, 252 children were admitted due to unintentional poison exposure. Most (198/252, 79%) were between 1 and 3 years of age. The majority of events (209/252, 82.9%) occurred at the patient’s home and 81% (205/255) were classified as exploratory ingestion. In 41/252 (14%) cases, exposure to more than one substance was reported. Most events 231/293 (79%) involved medications and 21% were due to domestic products. Four medications account for 45% of the events (Paracetamol, Salbutamol, Antihypertensive, and Antidepressants). Opioids were responsible for only 1.7%. By, collaboration between government, public health, educational institutions and commercial companies, can the burden of pediatric unintentional poison exposure be reduced.
Introduction
Fatal child poisoning involving drugs and other hazardous household substances has decreased dramatically in the United State (US) in recent decades, down from >200 per year in the early 1970s to an average of < 35 per year in recent years.1,2 This decrease can be attributed to implementation of the poison prevention packaging act, and the introduction of child-resistant packaging (CRP) and education on safe medication storage. 3 However, in certain countries, such as Pakistan, pediatric poisoning mortality can be as high as 11%. 4 Despite such interventions, child morbidity due to unintentional poisoning remains a significant burden on public healthcare worldwide. According to the US records, there are approximately 500,000 calls to poison centers and more than 60,000 pediatric emergency visits annually. The majority of these events occur at home and most involve preschool children (<6 years of age).5-7
The Israel National Poison Information Center published a retrospective analysis of their database of patients <18 years of age during 2007. A total of 15,005 pediatric events were recorded of which only 21% were referred by physicians with the remaining 79% initiated by the public. Most (80.3%) were in preschool children (<6 years), 89% of events occurred at home, and 90% were unintentional poison exposure. Most patients (92%) were asymptomatic or mildly affected with only 1.9% required hospitalization. 8 Following these findings, in 2008, we, in collaboration with Safe Kids Israel Organization (“Beterem”), which is a member of Safe Kids Worldwide, started a prospective study of all unintentional injuries in the pediatric population (0-18 years) admitted to the PED in the E. Wolfson Medical Center. By 2017, despite implementation of CRP requirements, the total number of referrals to the Israel National Poison Center had increased dramatically by ~ 50%, to 22,431 pediatric cases with very similar characteristics in comparison to the previous report, that was published in 2010 8 (Y. Bentur, personal communication, October 2017). These results call for a different approach in order to reduce the incidence of unintentional pediatric poison exposure.
The aim of the present study was to characterize the patterns of unintentional poison exposure in children (0-7 years), who represent the most vulnerable pediatric population. This could help identify prevention priorities and direct intervention strategies specific for this group.
Methods
Data Source
Our study population included children (0-7 years) seen in the PED in the E. Wolfson Medical Center during a 9-year period (January 2009 to December 2017). The hospital serves mid-high socioeconomic status population (cluster 5-8 according to the local authorities’ index conducted by the Central Bureau of Statistics), and it is defined as secondary health center.
As a part of the National Pediatric Injury and Safety Surveillance program in Israel, in August 2008, in collaboration with Safe Kids Israel Organization (“Beterem”), we created a computerized questionnaire designed to collect comprehensive data about all the PED visits in the E. Wolfson Medical Center due to unintentional injuries (age 0-18 years).
The questionnaire, which is based on the WHO recommendations, is completed by the nursing staff upon arrival at the PED of a child presented with unintentional injuries. It contains epidemiological, demographic, and clinical data including the age and gender, place, and mechanism of injury, the body part involved, the circumstances surrounding the injury, and subsequent treatment and outcome. The “Helsinki” ethics committees of the E. Wolfson Medical Center approved the study. No written informed consent was required.
If poison exposure was suspected, the following additional data were recorded: the toxic substance; place and manner of exposure associated with the poisoning; whether the exposure was due to intentional or unintentional ingestion; whether the event was caregiver error or due to exploratory ingestion, time between exposure and arrival at the PED; symptoms and signs; type of medical assistance before admittance to the PED; treatment at the PED (basic life support, GI decontamination, antidote or symptomatic therapy); results of laboratory and toxicology investigations; and patient’s final outcome. Information about whether the poison control center was consulted before or during the PED visit was also recorded.
In 8 cases, the children were drowsy upon arrival and there was no initial known exposure to medication or hazardous substances. These patients were queried later when the details about the poison exposure were revealed.
Poison exposure was defined as ingesting or inhaling a potentially toxic substance, and chemical burns resulting from contact with acids, alkalis, or caustic agents. Poisoning or allergic reactions resulting from insect bites or plants, as well as smoke and carbon monoxide inhalation, were excluded from the analysis. The poison exposure cases were categorized according to the type of product or products involved.
Reason for poison exposure was categorized as either exploratory ingestion, refer to those cases in which the child himself mistakenly ingested the drug/household agent, or a caregiver mistakenly gave the toxic material by an inappropriate route or dose. The outcome of each child, that was unintentionally exposed to poison, was documented (data not shown).
Statistical Analysis
Statistical analyses used SPSS V. 23. Chi square tests were performed in order to test the associations between gender and other categorical variables. Independent sample t-tests were conducted in order to test differences in continuous variables (age and hospitalization duration) between groups. The 95% confidence intervals of frequencies were obtained by using the bootstrapping method based on 5,000 resamples.
Results
During the period of this prospective study, there were 203,620 admissions of children aged 0 to 18 years to the PED in the E. Wolfson Medical Center. Out of them, 71,765 visits were due to unintentional injuries. These included 308 patients aged 0 to 18 years who were admitted due to suspected unintentional poison exposure. A total of 252 children (48.8% males, N = 123; 51.2% Females, N = 129), aged under 7 years (M = 2.16, SD = 1.27), met the inclusion criteria and were recruited to the study after being admitted to the PED.
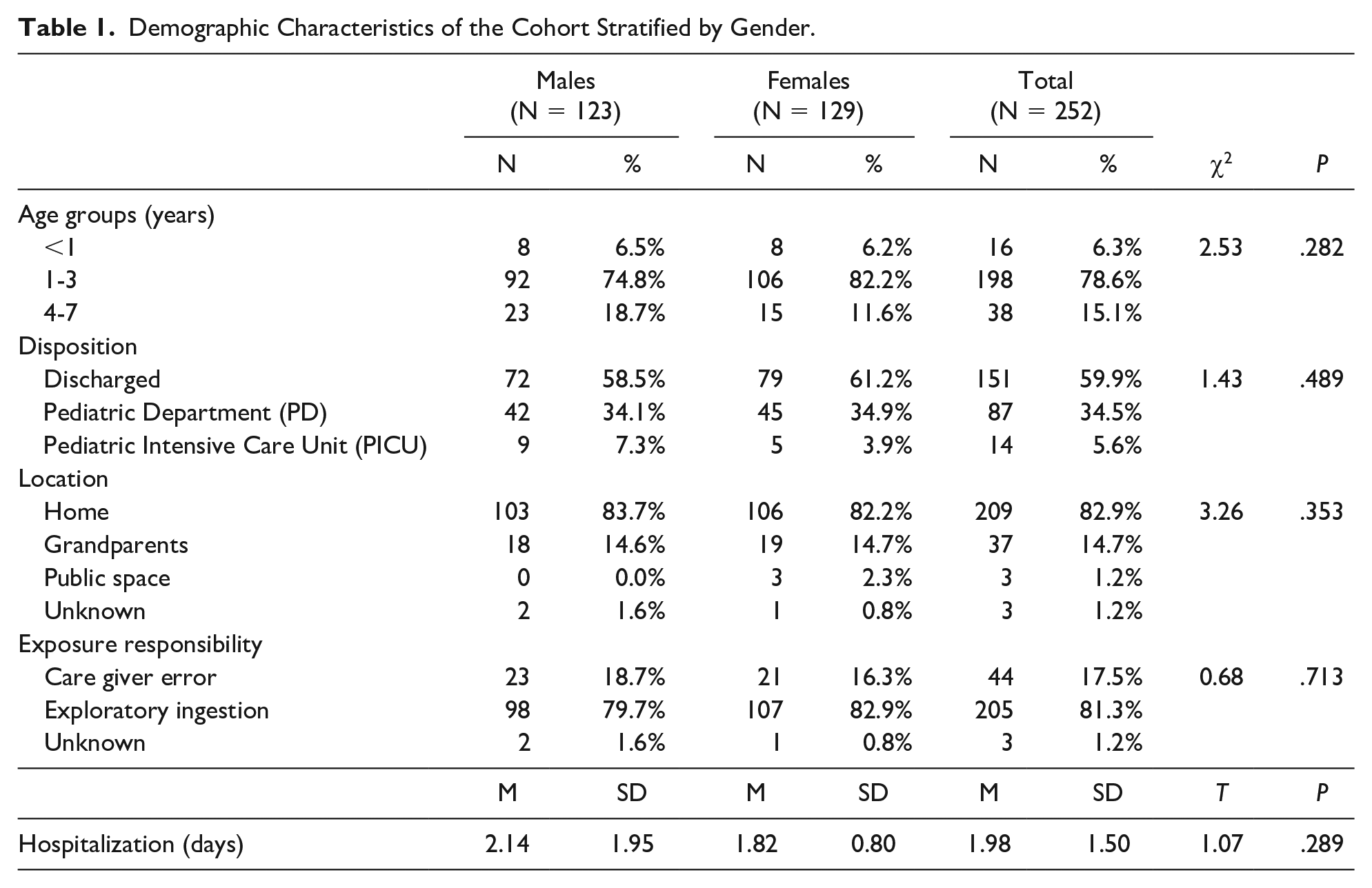
The demographic characteristics presented in Table 1 revealed no significant gender differences. Most of the children, 198/252, 79%)) were between 1 and 3 years old, including 92/123 males (75%) and 106/129 (82%) females.
Demographic Characteristics of the Cohort Stratified by Gender.
The distribution of reason for poison exposure among different age groups is presented in Figure 1. Among 16 children under the age of 1 year, only very few (6.3%) were due to exploratory ingestion, in contrast to 86.4% of incidents among older children, with a peak in the group aged 1 to 2 years. The comparison between the 2 groups yielded a statistical significance (P < .001).
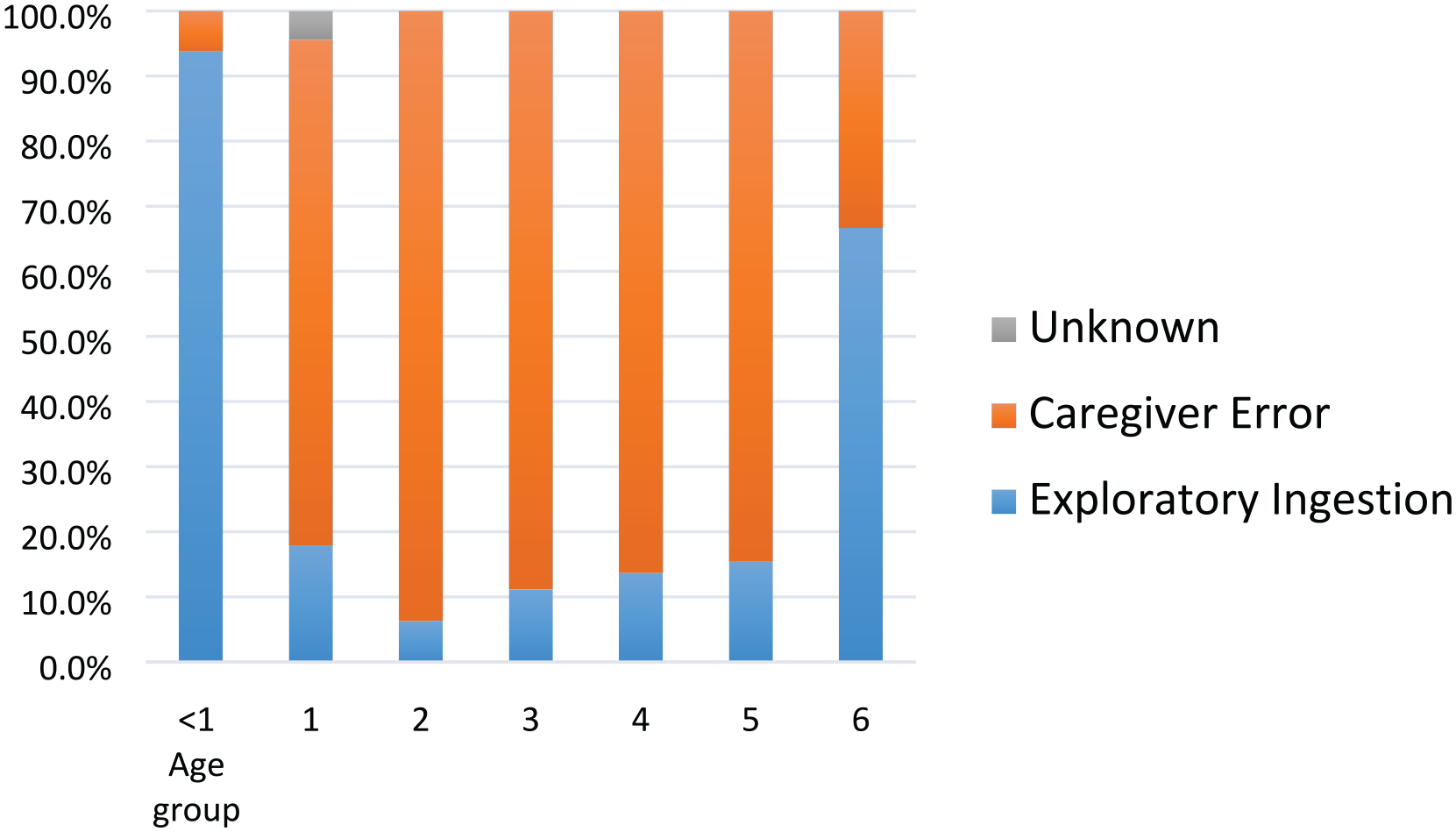
The X axis represents the age group, and the Y axis represents the percentage of responses
Most admissions to the PED (177/252, 70 %) were due to reported poison exposure without apparent clinical manifestations. Other manifestations include drowsiness—26, tachycardia—14, restlessness—13, vomiting—10, ataxia—9, encephalopathy—5, hypotension—4, respiratory symptoms -2 (some patients had more than 1 symptom). The majority of patients (151/252, 60%) were discharged from the PED. The most common treatments in the PED included cardiovascular monitoring—66 (26%), IV fluids—46 (18%), GI detoxification with activated charcoal—38 (15%). The reasons for hospitalization of the 14 patients in the PICU comprised of exposure to CNS depressants– 8, CVS drugs—3, wart solution -1, hydrocarbon solvent—1, potassium permanganate—1. No deaths were recorded.
Among the children hospitalized in the PD or PICU, 84/101 (83%) were discharged within 1 to 2 days. However, we found a significant difference between the duration of hospitalization in the PD and PICU (P = .003).
Most poison exposure events occurred in the patient’s home (82.9%, N = 209) and 81% (205/255) were classified as exploratory ingestion. No gender differences were found in the distribution of location of poison exposure, or in exploratory ingestion (Table 1).
Table 2 shows the distribution of 293 drugs/household agents that the children had unintentionally were exposed to. Among our cohort 41/252 (14%) patients were exposed to more than one substance. The toxic agents include combination therapy drugs such as antihypertensive and diuretics, cough medications and paracetamol, vitamins and iron, vitamins and homeopathic supplements, and antihistamines and pseudoephedrine, as well as a variety of domestic products. The majority (231/293; 79%) of the unintentional poisoning exposures were due to medications and only 21% were due to domestic products. Cleaning products included bleach—9, cleaners—6, laundry—5, others—5. Cosmetic/Personal care products included: soaps/shampoos—8, nail products—5, hair products—5, solvents/alcohol/ oil—4, and creams/ointment—4. Other products included pesticides—8, cannabis—2, and kerosene—2.
Distribution of 293 Unintentional Poison Exposure Drugs/Household Agents Among 252 Preschool Children.
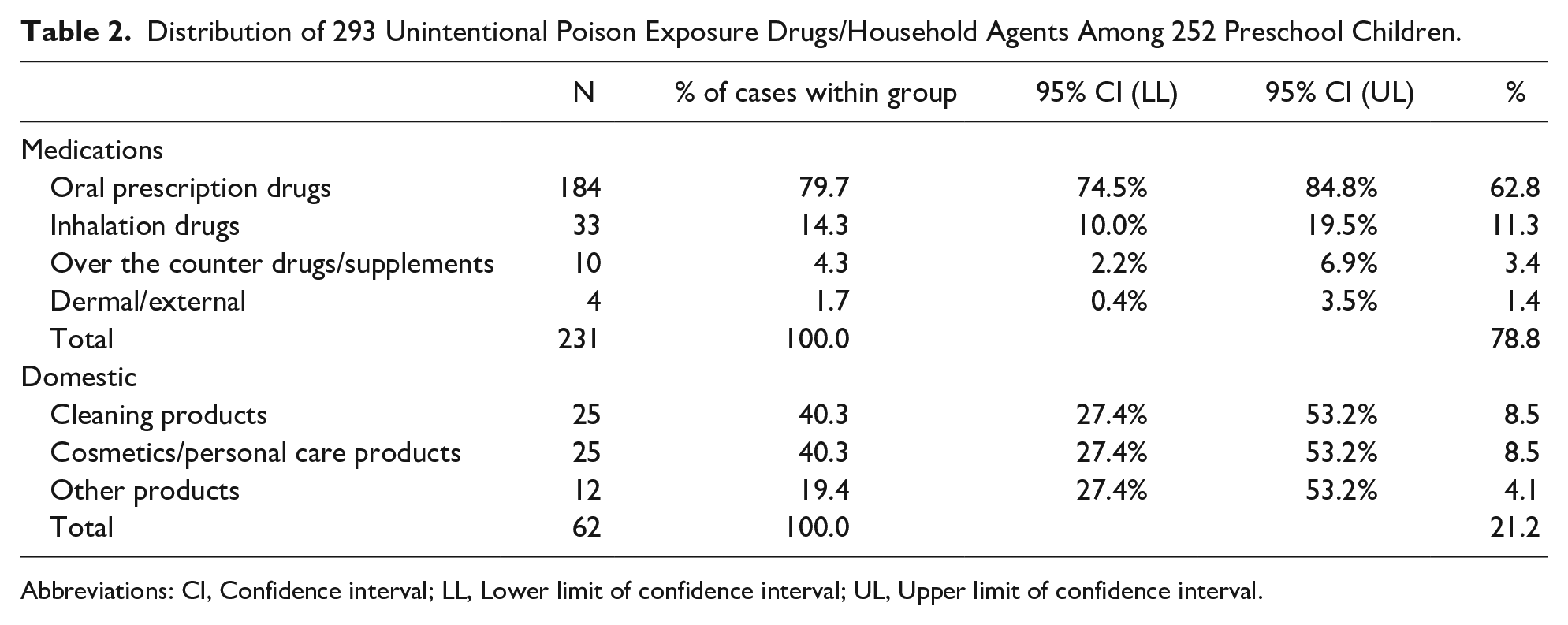
Abbreviations: CI, Confidence interval; LL, Lower limit of confidence interval; UL, Upper limit of confidence interval.
The most common form of exposure to poisoning agents was ingestion, which was the route involved in 96% (281/293) of all cases. Inhalation was responsible for only 3% (9/293) of the poisonings, and skin/eye injuries comprised only 1% (3/293) of the cases.
The results presented in Table 3 demonstrate that only 4 groups of medications account for 76% of the events and 4 single medications account for 45% of the events.
Distribution of 231 Medications Involved in Unintentional Poison Exposure.
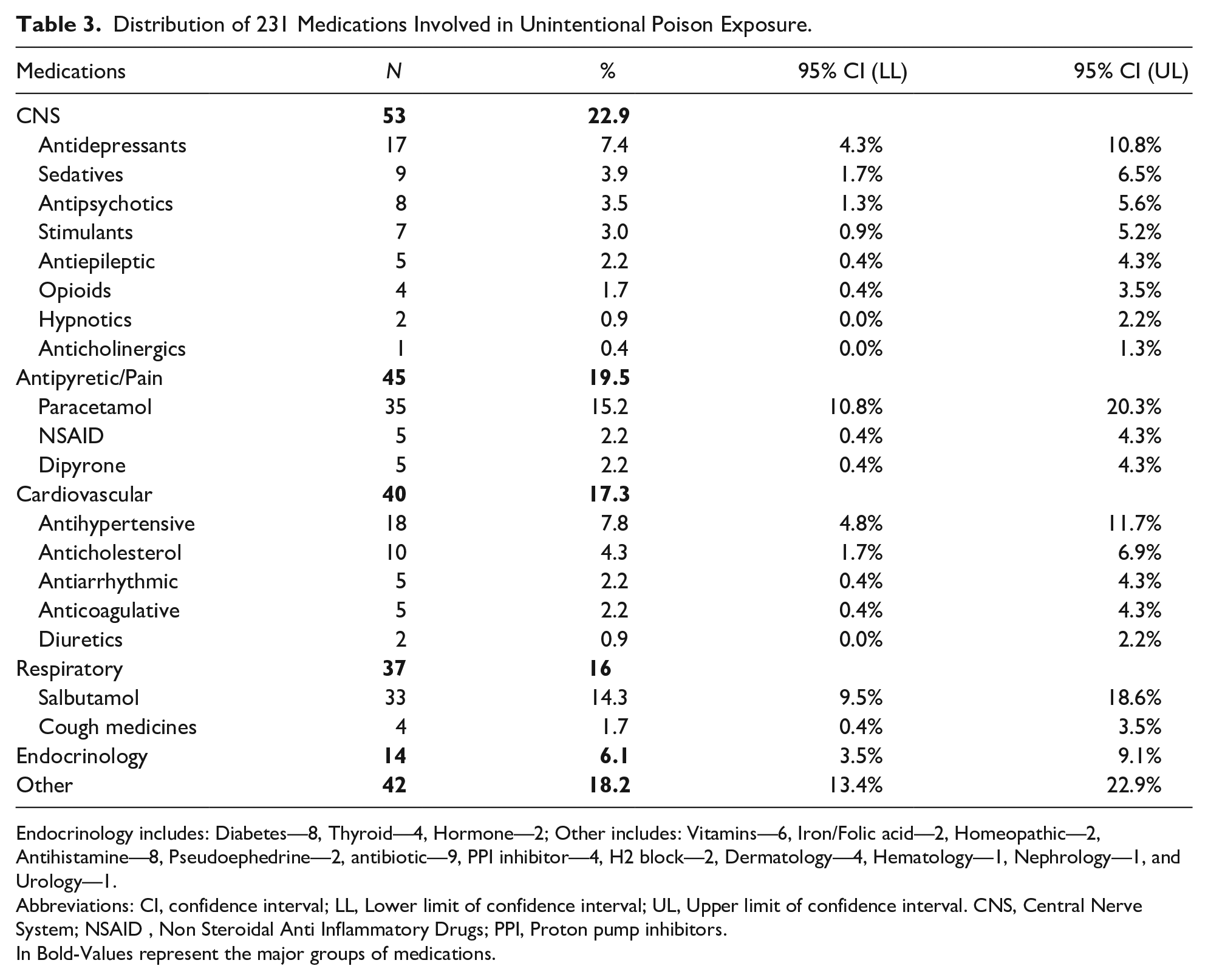
Endocrinology includes: Diabetes—8, Thyroid—4, Hormone—2; Other includes: Vitamins—6, Iron/Folic acid—2, Homeopathic—2, Antihistamine—8, Pseudoephedrine—2, antibiotic—9, PPI inhibitor—4, H2 block—2, Dermatology—4, Hematology—1, Nephrology—1, and Urology—1.
Abbreviations: CI, confidence interval; LL, Lower limit of confidence interval; UL, Upper limit of confidence interval. CNS, Central Nerve System; NSAID, Non Steroidal Anti Inflammatory Drugs; PPI, Proton pump inhibitors.
In Bold-Values represent the major groups of medications.
Of note, there were 33 cases that involved Salbutamol for inhalation. In 28 cases it was mistakenly taken orally, and in 5 patients an error was made in the cumulative inhalation dosage.
Discussion
In our 9-year prospective study, we characterized 252 unintentional poison exposure cases among children (0-7 years), admitted to a single PED in E. Wolfson Medical Center, in Israel. We found that most of them were between 1 and 3 years of age. The majority of events occurred at the patient’s home and were classified as exploratory ingestion. Four medications account for 45% of the events (Paracetamol, Salbutamol, Antihypertensive, and Antidepressants).
In our study, poison exposure rates were similar between girls and boys, of all age groups, with similar end results (hospitalization in the PD or PICU, or discharge home) to other studies, conducted in the United States and Australia.9,10
The majority of our patients involved children between the ages of 1-3 and were classified as exploratory ingestion. Children younger than 1 year old comprised only 6.3% of cases and the vast majority of them were due to caregiver errors (i.e. wrong dosing). Our results indicate that the chances of unintentional poison exposure in the older subset were 117.50 higher than in the younger age. This trend was compatible with similar findings in young children below 6 months. 11
The hospitalization rate in our study was 41.5%, which is much higher than the 13.3% hospitalization rate for all National Electronic Injury Surveillance System (NEISS)-reported injuries involving children 5 years of age and younger. 5 The Israeli National Poison Center reports that 78.6% of calls to the telephone service center of the Poison Center, were made by the public, with most patients directed to remain at home for observation and only 9.9% of calls, resulting in referral to PEDs. Of these, only 1.9% of cases resulted in hospitalization. 8 It might be reasonable to assume that more severe cases come directly to the PED, so that the Poison Center acts as a filter for the milder cases, and prevents unnecessary admissions to the PED. Similar buffering effect of a regional poison center was found by Chafee-Bahamon and Lovejoy. 12 In recent research from the United States on poisoning-related visits, it emerged that 57.6% of the referrals to the PED were based on caregiver judgment, and only 42.4% were triaged by a poison control center. A total of 46.6 % of self-referrals to the PED proved to be redundant according to the criteria established by the control center. 13 Since regional poison control centers report a higher rate of medical appropriateness, in terms of justified PED referrals, 14 this may explain the difference in the hospitalization rate in our study.
In several cases, it took days until poison exposure was suspected and recognized, while wasting diagnostic and therapeutic resources. The children in this group were admitted to the PICU/PED suffering from unclear conditions, such as impaired consciousness, and therefore required intense investigations and treatments.
In our study, 79% of poison exposures were caused by medications, and 21% by domestic products, as similarly reported in a study done in the United States. 15 In a Spanish study on poisoning in all pediatric age groups that included both intentional and non-intentional cases, 5.9% of poisonings were due to alcohol exposure, and 1.5% were due to exposure to illicit drugs. 16
The 2 most common drugs involved in poison exposure in our cohort are Paracetamol and Salbutamol. These drugs are frequently used in the pediatric medicine. Paracetamol is protected with a CRP. However, Salbutamol was only packed with CRP in 2017, after our study was completed. We speculate that the introduction of CRP will make a significant difference to the Salbutamol poisoning rates since most of our cases were due to drinking the medication (by the child without parental guidance), and only a minority of cases were the result of an inappropriately high frequency of inhalations, given by the parents. Similarly, a study in Spain, reported that the most common drugs implicated in poisonings of children under 10 years of age were Paracetamol, followed by cough and cold medications. 16 The two other medications that were frequently involved in poison exposure were Antidepressant and Antihypertensive drugs. These sub-groups contain multiple medications frequently prescribed mainly for adult use. Our results emphasize the importance of placing medications out of the reach of children.
It seems that medication consumption is a matter of geography. The high prevalence of Opioid consumption in the U.S. results in a high exposure of children to Opioids, and consequently, Opioids are a common cause of poisoning in the pediatric population in the United States.17-19 Since adult consumption of Opioids is infrequent in Israel, it is not unexpected that Opioids were responsible for poison exposure in only 1.7% of our children.
The strength of our study includes the following: being a prospective study, based on computerized data and the length of the study. However, there are some limitations including that is based on a single-center data and the cohort is relatively small.
In summary, our study revealed that unintentional poison exposure in the pediatric population in our area remains a significant health problem. We believe that the burden of this problem may be reduced by improving regulations and inspection, raising the public’s awareness, introducing appropriate legislation and increasing the involvement of government institutions such as the Ministry of Health, public health foundations, and education institutions, as well as commercial companies.
Author Contributions
HWA: contributed to conception and design; contributed to acquisition, analysis, and interpretation; drafted manuscript; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
B-HAD: contributed to conception and design; contributed to analysis; drafted manuscript; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
YD: contributed to acquisition, analysis, and interpretation; drafted manuscript; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
GM: contributed to conception and design; drafted manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
IB: contributed to conception and design; drafted manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
DT: contributed to conception and design; drafted manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
AO: contributed to conception and design; drafted manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
ID: contributed to conception and design; contributed to acquisition, analysis, and interpretation; drafted manuscript; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.