
Abstract
The Clinical Effort Against Secondhand Smoke Exposure (CEASE) is an evidence-based framework that increases pediatric providers’ ability to address secondhand smoke exposure of minors. Physician champions at 4 University of California sites conducted regular 1-hour didactic trainings on CEASE principles to pediatric residents as part of a longitudinal curriculum. At the conclusion of the academic year, 111 of 284 residents (39%) completed an anonymous survey. CEASE-trained residents reported significantly higher rates than untrained residents of counseling on smoking cessation (adjusted odds ratio [OR] = 4.50, P = .009), and referring to the smokers’ quitline (adjusted OR 3.6, P = .007) to 50% or more of their patients’ caregivers who smoked. In addition, among CEASE-trained residents, there were significant increases in multiple post-training knowledge and self-efficacy items. Our results show that a brief educational curriculum can be helpful in changing pediatric residents’ attitudes and behavior toward assisting adult caregivers to pediatric patients in smoking cessation.
Introduction
Despite significant advances in smoking cessation efforts in the United States, tobacco use remains a considerable source of morbidity and mortality. 1 Furthermore, much of the progress in reducing smoking rates in the United States has been concentrated in wealthy, privileged populations, leaving underserved populations to bear the brunt of this hazardous exposure. 2 Pediatric patients, including those who do not themselves smoke, are a particularly vulnerable group to smoke and secondhand smoke, as the exposure to tobacco combustion byproducts can lead to the development and exacerbation of a number of cardiopulmonary diseases, chief among them asthma attacks, respiratory infections, ear infections, and sudden infant death syndrome.3-6
When children affected by smoking and secondhand smoke present for medical care, the health care system has a unique opportunity to intervene and break the cycle of nicotine addiction and its downstream effects for both pediatric patients and their accompanying caregivers. Despite the American Association of Pediatrics (AAP) guidelines endorsing tobacco use cessation approaches with patient parents and families at clinical visits, rates of such behaviors remain suboptimal. 7 The Clinical Effort Against Secondhand Smoke Exposure (CEASE) is an evidence-based framework that increases pediatric providers’ ability to address secondhand smoke exposure (SHSE) through 3 effective techniques to curb caregiver smoking. These include screening for SHSE, assisting with quitting through motivational interviewing and prescribing nicotine replacement therapy (NRT), and referring those who smoke to a quitline.8-11 These strategies have successfully been used to decrease smoking rates in caregivers10,12 and are summarized in Figure 1.
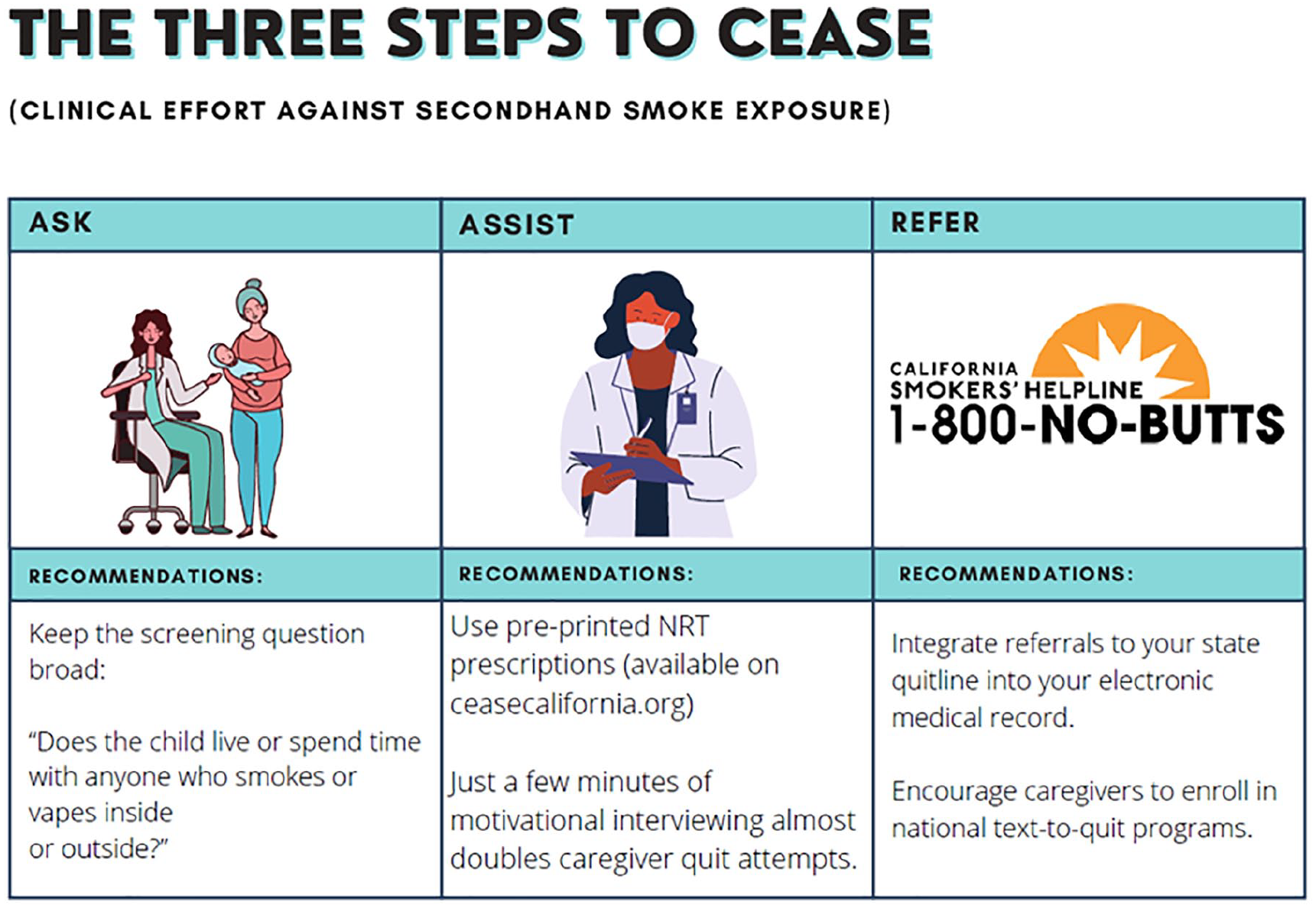
Principals of CEASE (Clinical Effort Against Secondhand Smoke Exposure).
Despite these encouraging findings, resident training programs do not require training in smoking cessation counseling and techniques.13-16 As such, we aimed to evaluate whether a curriculum for teaching pediatric residents the CEASE framework would result in self-reported behavior change, increased knowledge, and improved self-efficacy with the subject matter of smoking cessation advice and NRT prescription.
Methods
Study Population, Exposure/Outcome Description
Physician champions at 4 University of California sites (University of California, San Francisco, Los Angeles, San Diego, and Davis) conducted regular didactic trainings on CEASE principles between July 2017 and June 2019. The curriculum involved standard CEASE digital training materials developed by one of the study authors for training pediatric practices in the state of California 17 that were used as the primary basis for presentations. Specific training topics include tobacco use screening techniques, motivational interviewing approaches, directed practice in writing pre-printed NRT prescriptions, and referral strategies to both state and national smokers’ quitlines.
At the end of the 2019 academic year, all pediatric residents at the 4 study sites were asked to complete a voluntary, online, retrospective Qualtrics survey to assess their behavior, knowledge, and self-efficacy around helping caregivers quit smoking. To assess behavior, residents were asked to indicate the number of caregivers whom they had counseled to quit smoking, prescribed NRT for, and referred to the California Smokers’ Helpline. We also assessed self-knowledge on the second- and third hand effects of smoking. To assess self-efficacy, we inquired about self-confidence in screening for SHSE, talking with caregivers about the importance of smoking cessation, using motivational interviewing for smoking cessation, making referrals to the California Smokers’ Helpline, and providing NRT prescriptions. The complete assessment tool is available as Supplementary Material 1. We compared both residents who reported having undergone the CEASE curriculum with those who indicated that they had not been exposed to the CEASE curriculum. The study was reviewed by the institutional review board (IRB) of the sponsoring institution and determined to be exempt (IRB # 17-22373).
Statistics
Deidentified baseline demographic characteristics of study participants including institution and level of training (ie, postgraduate year [PGY]) were collected with the initial survey (Table 1). These trainee characteristics were described using counts, percentages, means, medians, standard deviations, and interquartile ranges. The SHSE knowledge and self-efficacy at performing interventions to facilitate smoking cessation were separately assessed using 10-point Likert scales. Univariate comparisons between groups were conducted using the chi-square and Wilcoxon rank-sum tests. To determine whether CEASE training was associated with increased likelihood of prescribing and counseling behaviors, we further constructed logistic regression models that were adjusted for trainee PGY and clinical site. P values <.05 were considered statistically significant. Survey data were captured and stored in a secure online Qualtrics survey database (Provo, Utah). Statistical analyses were performed using the Stata 12 software package (StataCorp, College Station, Texas).
Participant Demographics.
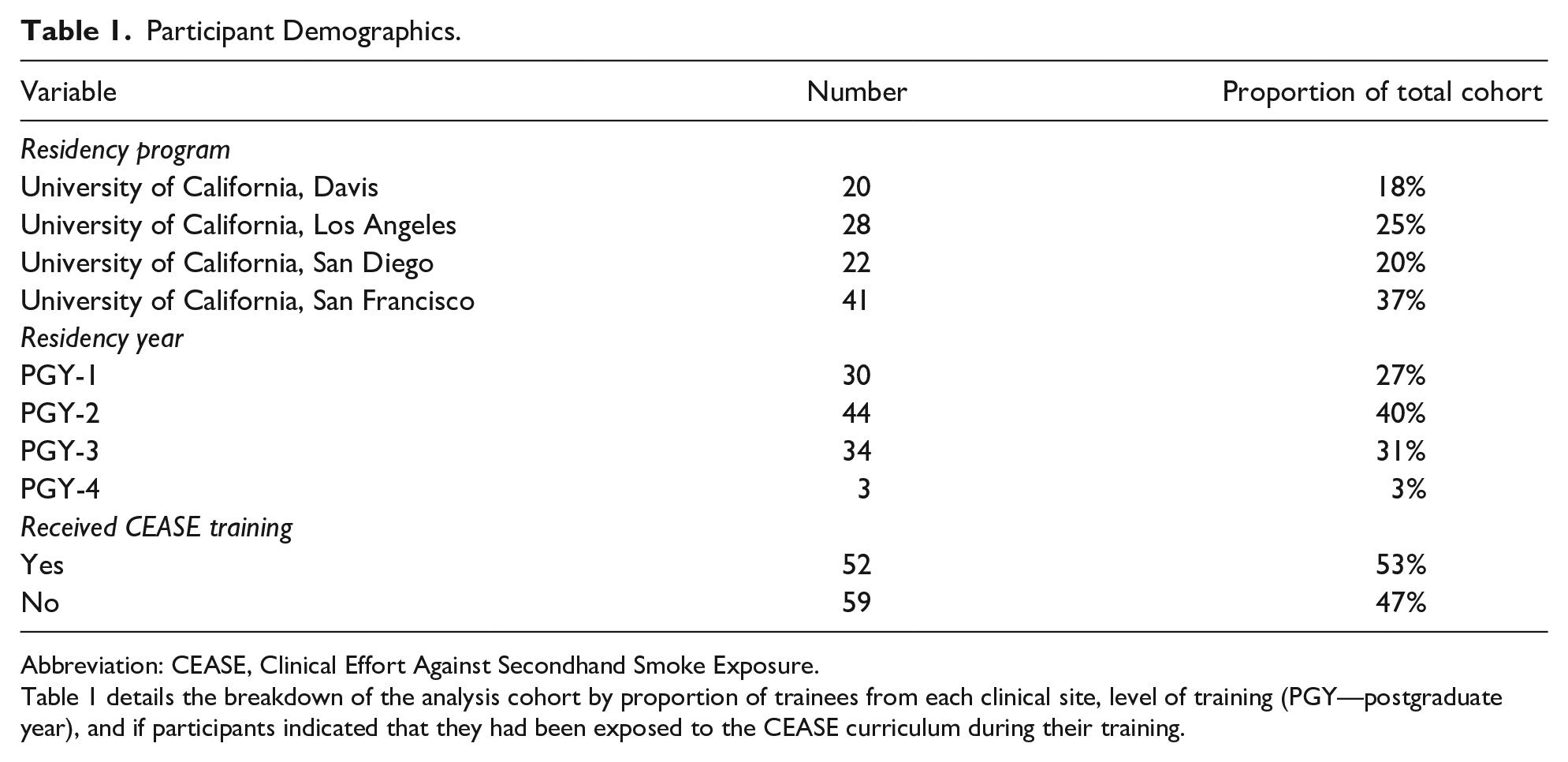
Abbreviation: CEASE, Clinical Effort Against Secondhand Smoke Exposure.
Table 1 details the breakdown of the analysis cohort by proportion of trainees from each clinical site, level of training (PGY—postgraduate year), and if participants indicated that they had been exposed to the CEASE curriculum during their training.
Results
Of 284 total pediatric residents (39%), 111 residents at all 4 clinical training sites completed the survey; of the respondents, 53% recalled receiving CEASE training. There was relatively comparable representation of study participants by institution and PGY year (Table 1).
Behavioral Outcomes
Per self-report, CEASE-trained residents had significantly higher rates than untrained residents of (1) counseling on smoking cessation (90% vs 71%, P = .01), (2) referring to the smokers’ quitline (66% vs 43%, P = .02), and (3) offering NRT prescriptions (31% vs 12%, P = .02) to 50% or more of their patients’ caregivers who smoked (Table 2). The effect persisted after controlling for PGY year and clinical site—Residents trained in CEASE were 4.5 times as likely to have counseled patient caregivers who smoke in half or more of their encounters, odds ratio (OR) for CEASE-trained vs untrained: 4.50, P = .009. They were also 3.6 times as likely to have referred patient caregivers to the smokers’ quitline (OR = 3.60, P = .007) in half or more of their encounters (Table 3).
Trained vs Untrained Pediatric Residents’ Smoking Cessation Assistance Behaviors.
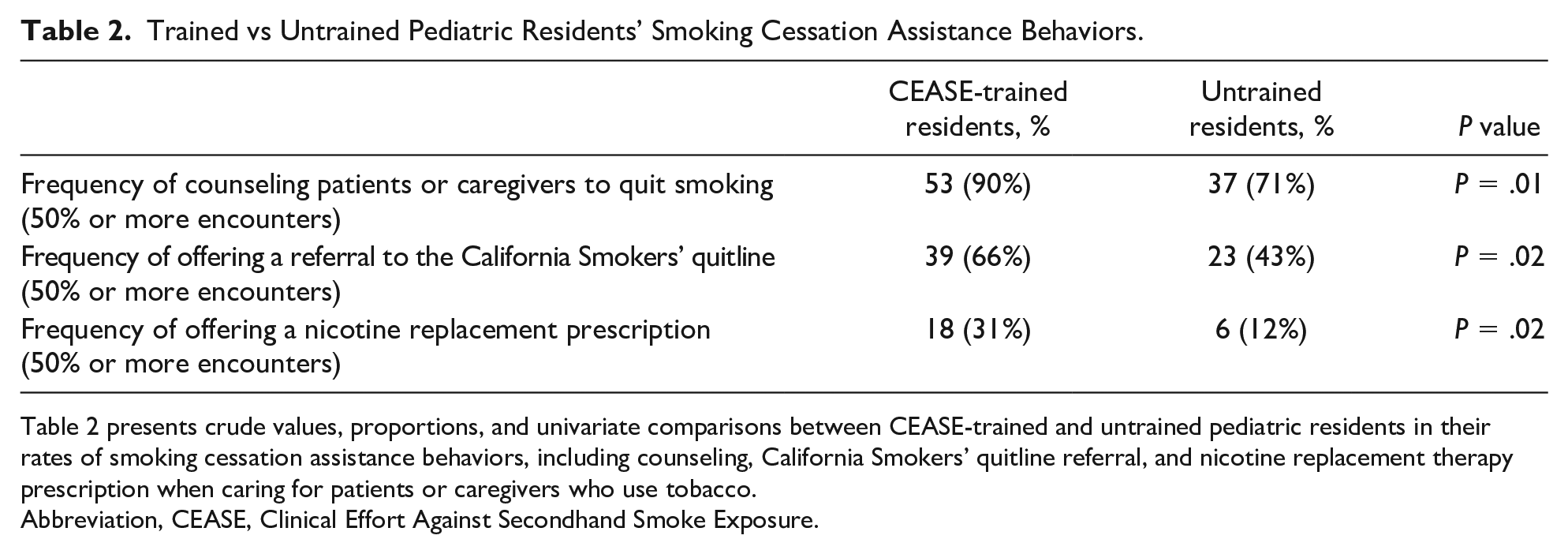
Table 2 presents crude values, proportions, and univariate comparisons between CEASE-trained and untrained pediatric residents in their rates of smoking cessation assistance behaviors, including counseling, California Smokers’ quitline referral, and nicotine replacement therapy prescription when caring for patients or caregivers who use tobacco.
Abbreviation, CEASE, Clinical Effort Against Secondhand Smoke Exposure.
Effect of Training on Prescribing and Counseling Behaviors.
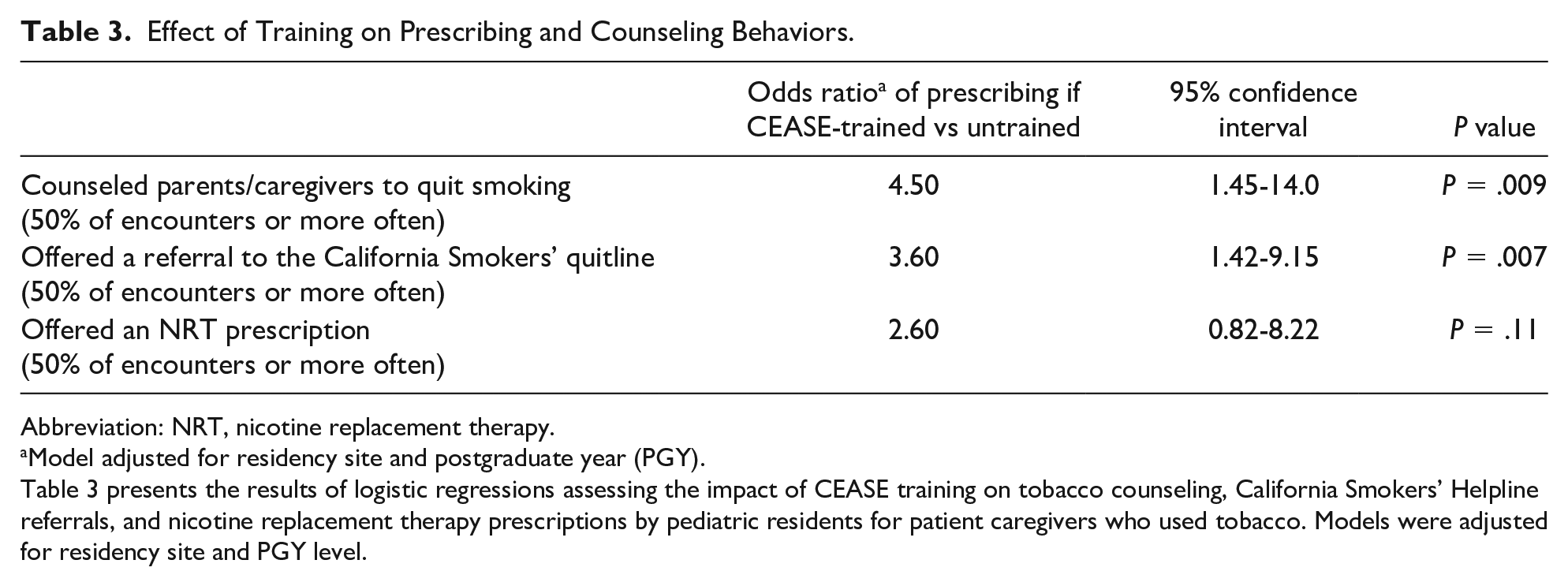
Abbreviation: NRT, nicotine replacement therapy.
Model adjusted for residency site and postgraduate year (PGY).
Table 3 presents the results of logistic regressions assessing the impact of CEASE training on tobacco counseling, California Smokers’ Helpline referrals, and nicotine replacement therapy prescriptions by pediatric residents for patient caregivers who used tobacco. Models were adjusted for residency site and PGY level.
Knowledge and Self-efficacy Outcomes
Among residents who indicated they had received CEASE training, there were significant increases in post-training knowledge and self-efficacy items (Table 4). Mean scores on the 10-point Likert assessment scales improved from before CEASE and after CEASE training. These included knowledge of the health effects of second- and thirdhand smoke exposure (mean score for the cardiorespiratory effects of SHSE 2.78 vs 3.65, P < .01; noncardiorespiratory effects 2.12 vs 3.03, P < .01), disparities in risk of SHSE among children (2.71 vs 3.48, P < .01), consequences of third hand smoke exposure for children (2.9 vs 2.94 P < .01), and screening patients for SHSE (5.47 vs 7.62, P < .01). In addition, there were significant improvements in comfort witheaking to patients’ caregivers on the importance of smoking cessation (5.21 vs 7.72, P < .01), using motivational interviewing techniques to discuss smoking cessation (5.37 vs 7.72, P < .01), making referrals to the Smokers’ Helpline (3.76 vs 7.44, P < .01), and providing caregivers NRT prescriptions (2.82 vs 6.06, P < .01).
Residents’ Attitudes and Knowledge Before and After CEASE Training.
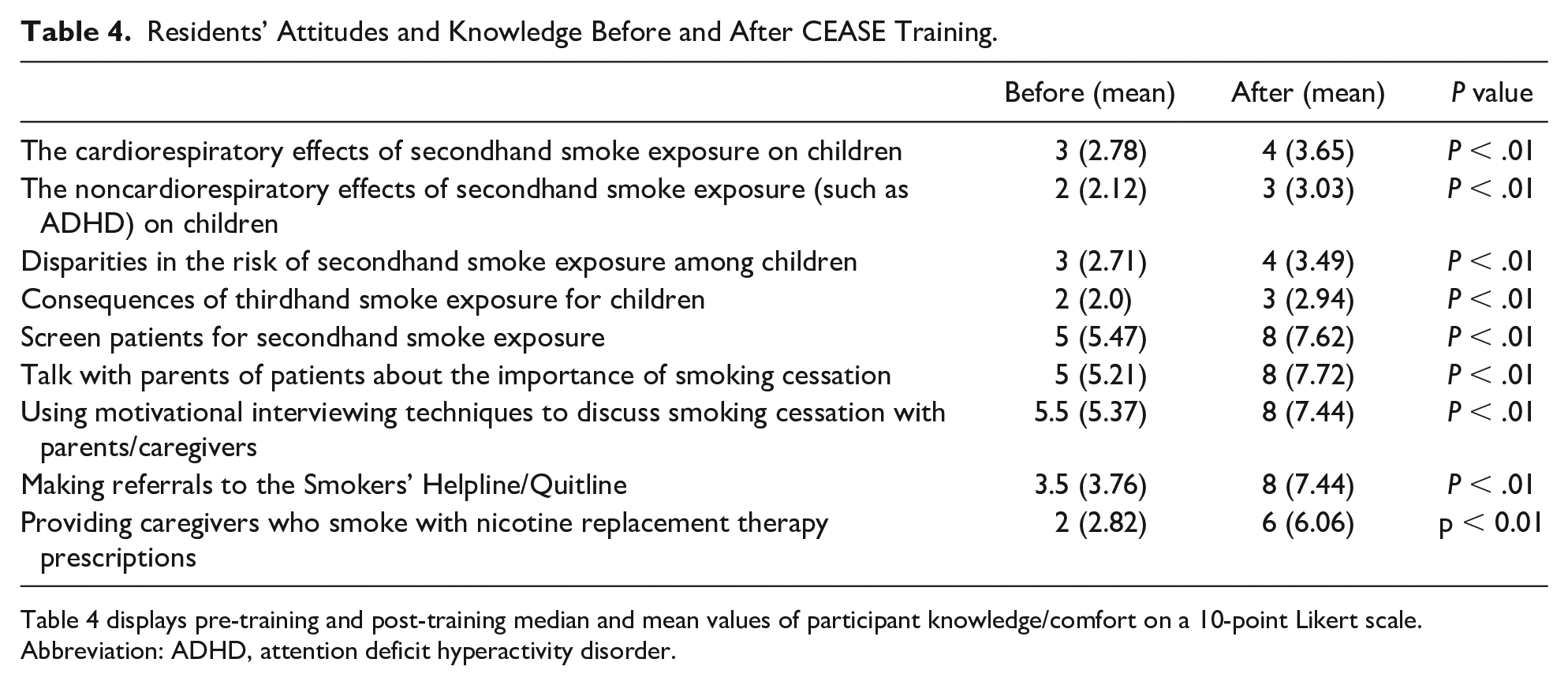
Table 4 displays pre-training and post-training median and mean values of participant knowledge/comfort on a 10-point Likert scale.
Abbreviation: ADHD, attention deficit hyperactivity disorder.
Discussion
Given the importance of combating smoking behaviors in both pediatric patients and their adult caregivers, the CEASE program presents a promising framework for physician education and intervention to protect children and their adult caregivers from the deleterious effects of tobacco smoke. Our present study demonstrates increases not only in housestaff comfort with clinical behaviors such as counseling caregivers on smoking cessation and referring them to quitlines, but also in prescribing NRT to these families. Furthermore, CEASE-trained residents reported increases in knowledge of the medical and socioeconomic impacts of SHSE as well as in screening, approaching, counseling, and referring adult caregivers who smoke to appropriate cessation resources.
Our findings come at a time where professional societies have recognized addressing smoking cessation in pediatric patient parents and family members, but also acknowledged low rates of such behaviors among pediatricians. 7 For example, longitudinal surveys of AAP members showed low rates and little change in pediatricians’ tobacco-quit strategy discussions with patients’ parents between 2004 and 2010 (10% to 14% in providing educational materials, 11% to 16% in referral to quitlines or cessation programs). 18 Although there are a number of reasons for these suboptimal values, national surveys have identified previous training as a major motivating factor in inspiring high levels of self-efficacy for pediatrics to screen and counsel parents.19,20
Thus, it appears that there is both efficacy and appetite for educating pediatric providers in smoking cessation of patient caregivers. Residency appears to the be ideal time for such training, and indeed, pediatric residency program directors who reported having undergone tobacco prevention and control education were significantly more likely than their untrained peers to include such topics in their housestaff instructional curricula. 13 Regrettably, the content of most of these reported curricula were limited by focusing on the effects of smoking (instead of interventions to address it), not incorporating active learning techniques, failing to evaluate trainee self-efficacy, and not involving NRT prescription. 13 It is in this setting that we propose CEASE as an ideal standardized curriculum to fill this role, as it addresses all of the above shortcomings of existing educational programs while reporting overall efficacy in assisting adult family members of patients to quit.10,11
Limitations
The present study has a number of limitations worth noting. First, as the study was not a randomized controlled trial, there exists potential for bias regarding housestaff who chose to participate in our intervention vs those who chose not to or did not find themselves in positions to participate in CEASE training. Although we adjusted our primary analysis for clinical training site and training level, there may be additional unmeasured covariates with impact on our outcome such as pre-residency knowledge of smoking behaviors and personal experiences with family tobacco use. Second, the analysis was not designed to capture long-term cessation rates in caregivers. Last, the training was aimed at the resident pediatrician level—as such, our results may not be generalizable to trainees in other specialties, trainees of other levels (eg, medical students, fellows), or those training to become allied health professionals (eg, physician assistants, nurse practitioners, pharmacists). Expansion of the CEASE curriculum to these valued members of the care team will allow us to assess their impact therein.
Conclusion
CEASE-trained residents reported higher comfort levels and frequency of performing secondhand smoke screening, prescribing NRT, and referring caregivers who smoke to the quitline.
Author Contributions
Study concept and design: Valerie Gribben, Amanda Kosack, Cambria Garell, Jyothi Marbin; Acquisition of data: Valerie Gribben, Amanda Kosack, Cambria Garell, Ulfat Shaikh, Maria Huang, Jyothi Marbin; Analysis and interpretation of data: Valerie Gribben, Jennifer Rasmussen, Kathleen Tebb, Andrew Chang Drafting of the manuscript: Valerie Gribben, Andrew Chang; Critical revision of the manuscript: Valerie Gribben, Amanda Kosack, Cambria Garell, Ulfat Shaikh, Maria Huang, Andrew Chang, Jennifer Rasmussen, Kathleen Tebb, Jyothi Marbin; Statistical analysis: Jennifer Rasmussen, Andrew Chang; Obtained funding: Jyothi Marbin.
Supplemental Material
sj-pdf-1-cpj-10.1177_00099228221113783 – Supplemental material for Impacts of a Multicenter Medical Education Curriculum for Training Pediatric Residents on Tobacco Cessation for Adult Caregivers of Pediatric Patients
Supplemental material, sj-pdf-1-cpj-10.1177_00099228221113783 for Impacts of a Multicenter Medical Education Curriculum for Training Pediatric Residents on Tobacco Cessation for Adult Caregivers of Pediatric Patients by Valerie Gribben, Amanda Kosack, Cambria Garell, Ulfat Shaikh, Maria Huang, Andrew Y. Chang, Jennifer Rasmussen, Kathleen Tebb and Jyothi Marbin in Clinical Pediatrics
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by First 5 California and the California Smoker’s Helpline (Grant Number: CFF 7401). The funders had no role in the study design, data collection, analysis, interpretation, writing of the paper, or decision to submit for publication.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.