
Abstract
In this study, we aimed to determine the frequency of symptomatic central venous catheters-associated deep vein thrombosis (CVC-a DVT) among critically ill children with femoral vein implantation in our pediatric intensive care unit (PICU), and to compare the demographic factors, serum electrolyte levels, and types of the infusion treatments performed. A total of 215 patients aged 1 month to 18 years who had femoral CVC implanted between 2019 and 2021 were included in this study. The cases that were clinically symptomatic and had thrombosis diagnosed ultrasonography were accepted as CVC-a DVT (+), and the other cases were considered as CVC-a DVT (-). Of the total 215 cases, 57.2% (n = 123) were female and 42.8% (n = 92) were male. Catheters-associated deep vein thrombosis diagnosis were made in 9.8% of the cases (n = 21). The mean time to diagnose thrombosis in CVC-a DVT (+) cases was 8.33 ± 5.65 days. With regard to gender, age, blood type, intubation status, length of stay on mechanical ventilator, presence of extra hemodialysis catheter, acute and chronic disease status, number of days of PICU hospitalization, and Pediatric Risk of Mortality-3 scoring, no significant differences between CVC-a DVT (-) and CVC-a DVT (+) cases were observed (P > .05). The incidence of thrombosis in refugee cases was found to be significantly higher than in Turkish cases (P = .047; P < .05). There was no statistically significant difference between the groups in baseline, mean, and peak glucose, sodium, and magnesium values and who received magnesium, blood product, inotrope, and 3% hypertonic saline (HTS) infusion (P > .05). No effect of serum glucose, sodium, and magnesium levels on the development of CVC-a DVT was found. Magnesium, blood product, inotrope, and 3% HTS infusion treatments have not been shown to have an effect on the development of CVC-a DVT.
Introduction
Central venous catheters (CVCs) are vascular access tools that can be used for a variety of purposes, including fluid and antibiotic therapy, inotropic infusion, blood product use, and parenteral nutrition in the intensive care follow-up of critically ill children. The use of CVCs is vital, especially in the follow-up of patients in pediatric intensive care units (PICUs), as it is often difficult to provide reliable vascular access in children. Non-tunneled CVCs are placed percutaneously in a deep vein (internal jugular, subclavian, or femoral) and can be used for a long time in acute situations. 1
In addition to the benefits of CVCs, there are also complications that may occur during and after the catheterization procedure. Early complications include arterial puncture, bleeding, nerve damage, and malposition, while late complications include catheter infection, dysfunction, and thrombosis.2,3 One of the most important risk factors for the development of deep vein thrombosis (DVT) in childhood is having a previously placed CVC. 4 In a meta-analysis study, it was reported that CVC-associated DVT (CVC-a DVT) is developed in approximately 20% of children with CVC. 5 It has been suggested that femoral vein CVCs lead to a higher incidence of CVC-a DVT than veins of other regions due to their location. 6
In this study, our primary aim was to determine the frequency of symptomatic CVC-a DVT in patients admitted to our PICU and implanted femoral non-tunneled CVC, and to determine the demographic, clinical, and laboratory findings of CVC-a DVT (+) cases. Second, we aimed to show the effect of serum electrolyte levels and especially effects of infusion therapies given via CVC on the development of CVC-a DVT.
Materials and Methods
A total of 215 patients who were admitted to the tertiary 8-bed PICU of our hospital during the 2-year period (2019-2021) were included in this retrospective study. Ethics committee approval was obtained from a local ethics committee and the study was conducted in accordance with the Declaration of Helsinki. All of the cases were between 1 month and 18 years of age, and the non-tunneled CVC was placed in the femoral vein. During the study period, all procedures were performed under intensive care conditions without ultrasonography (USG) by the PICU team blindly. Percutaneous technique was used for catheterization under sterile conditions. The size of the selected CVC was decided by the PICU team according to the age and body measurements of the case. Generally, we insert a 4f CVC in infants between 1 month and 1 year, 5f in preschool age group, 5.5f in school age group, and 7f in adolescent age group. Patients in which the CVCs that were placed in a deep vein other than the femoral vein or placed permanently, had a catheter infection, and CVCs were placed outside the intensive care conditions were excluded from the study. Additionally, in critically ill children, urinary output was monitored by an urinary catheter. No anticoagulation therapy was given to any patient prior to catheter placement. However, routine care (washing with a mixture of unfractionated heparin mixed with 0.9% isotonic saline at a ratio of 1/1, twice a day) was performed in each case in accordance with the standard practice principles accepted for our unit. After CVC placement, the cases were followed up for extremity swelling, edema, redness, or catheter dysfunction. Ultrasonography and Doppler USG were performed in cases with clinical symptoms. Ultrasonography was performed by an experienced radiologist under intensive care conditions on the day the symptoms were diagnosed. The difference between the day of insertion of the catheter and the day of thrombosis was recorded. Thrombosis was diagnosed by ultrasonographic visualization of thrombus or absence of intraluminal blood flow by Doppler USG. Patients with clinical symptoms and detection of thrombosis by USG were grouped as CVC-a DVT (+), and all other cases as CVC-a DVT (-).
The data of the cases were obtained from the hospital records retrospectively. Age, gender, ethnicity, blood type, presence of acute and chronic disease, length of stay in PICU, intubation status, length of stay on mechanical ventilator, onset of thrombosis after catheter placement, laboratory parameters (glucose, sodium, magnesium), treatments applied, and Pediatric Risk of Mortality-3 (PRISM-3) score were recorded. For the laboratory parameters, the baseline levels at the time of admission to the PICU, peak values during the intensive care follow-up, and as the mean levels, all values during the total intensive care stay were recorded. Infusion of magnesium, blood product, inotrope, and 3% hypertonic saline (HTS) were recorded as the treatment protocol. Due to the retrospective nature of the study, informed consent was not obtained either from the patients or their relatives.
Statistical Analysis
Number Cruncher Statistical System (NCSS) 2007 (Kaysville, Utah, USA) software was used for statistical analysis. Descriptive statistical methods (mean, standard deviation, median, minimum, maximum, frequency, and percentage) were used to evaluate the data. The distribution of the quantitative to the normal distribution was tested with the Shapiro-Wilk test and graphical examinations. Independent sample t-test was used for the comparison of normally distributed quantitative variables of 2 groups, and the Mann-Whitney U test was used for comparisons of 2 groups with non-normally distributed quantitative variables. Pearson chi-square test, Fisher’s exact test, Fisher-Freeman-Halton exact test were used to compare qualitative data. P < .05 was considered statistically significant.
Results
Our study was carried out on 215 cases, 57.2% (n = 123) were female and 42.8% (n = 92) were male. The ages ranged between 1 and 212 months, with a mean age of 50.23 ± 53.11 months. The distribution of the descriptive features of the cases is indicated in Table 1. Catheters-associated deep vein thrombosis was detected in 9.8% of the cases (n = 21). Thrombosis in CVC-a DVT (+) cases was diagnosed within the period between 2 and 25 days, with a mean period of 8.33 ± 5.65 days. The evaluation of the cases according to the presence of thrombosis is shown in Table 2. Accordingly, gender, age, blood type, intubation status, length of stay on mechanical ventilator, presence of extra hemodialysis catheter, presence of acute and chronic disease, length of stay in PICU, and PRISM-3 scoring did not significantly differ between CVC-a DVT (+) and CVC-a DVT (-) cases (P > .05). In the evaluation made according to the ethnic origin of the cases, the incidence of thrombosis in refugees was found to be significantly higher than in Turkish cases (P = .047; P < .05).
The Distribution of the Descriptive Features of the Cases.
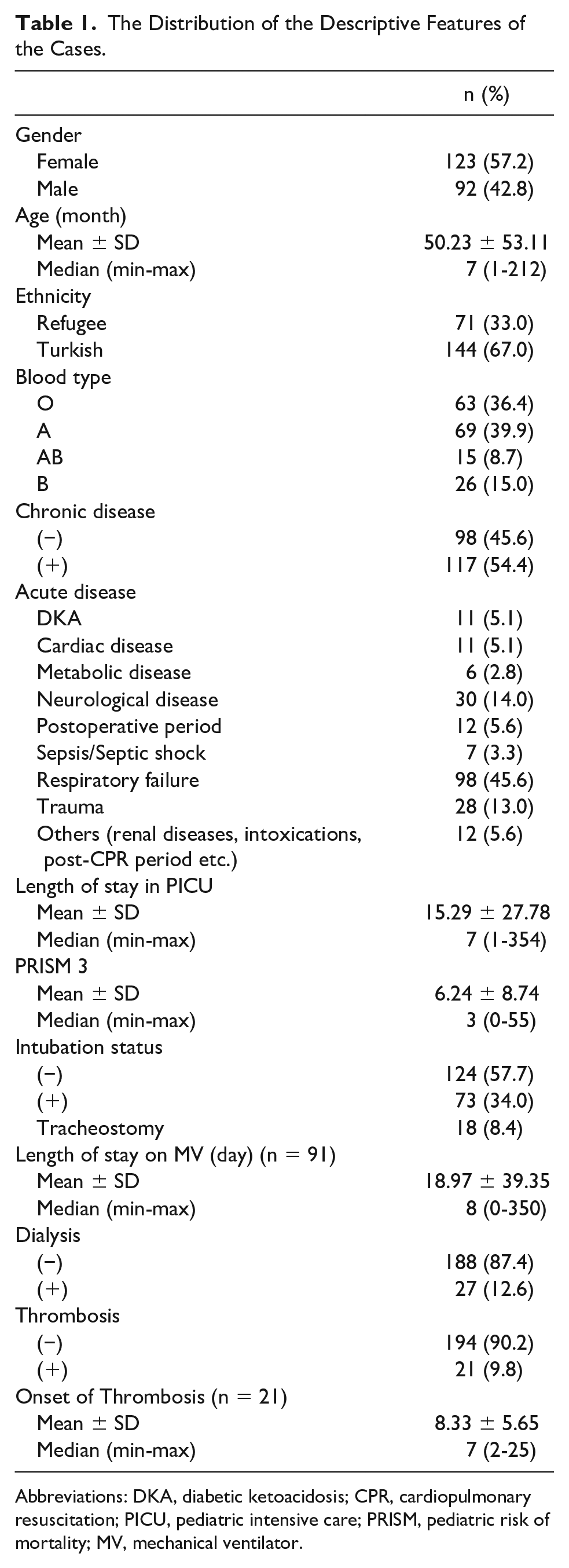
Abbreviations: DKA, diabetic ketoacidosis; CPR, cardiopulmonary resuscitation; PICU, pediatric intensive care; PRISM, pediatric risk of mortality; MV, mechanical ventilator.
The Evaluation of the Cases According to the Presence of Thrombosis.
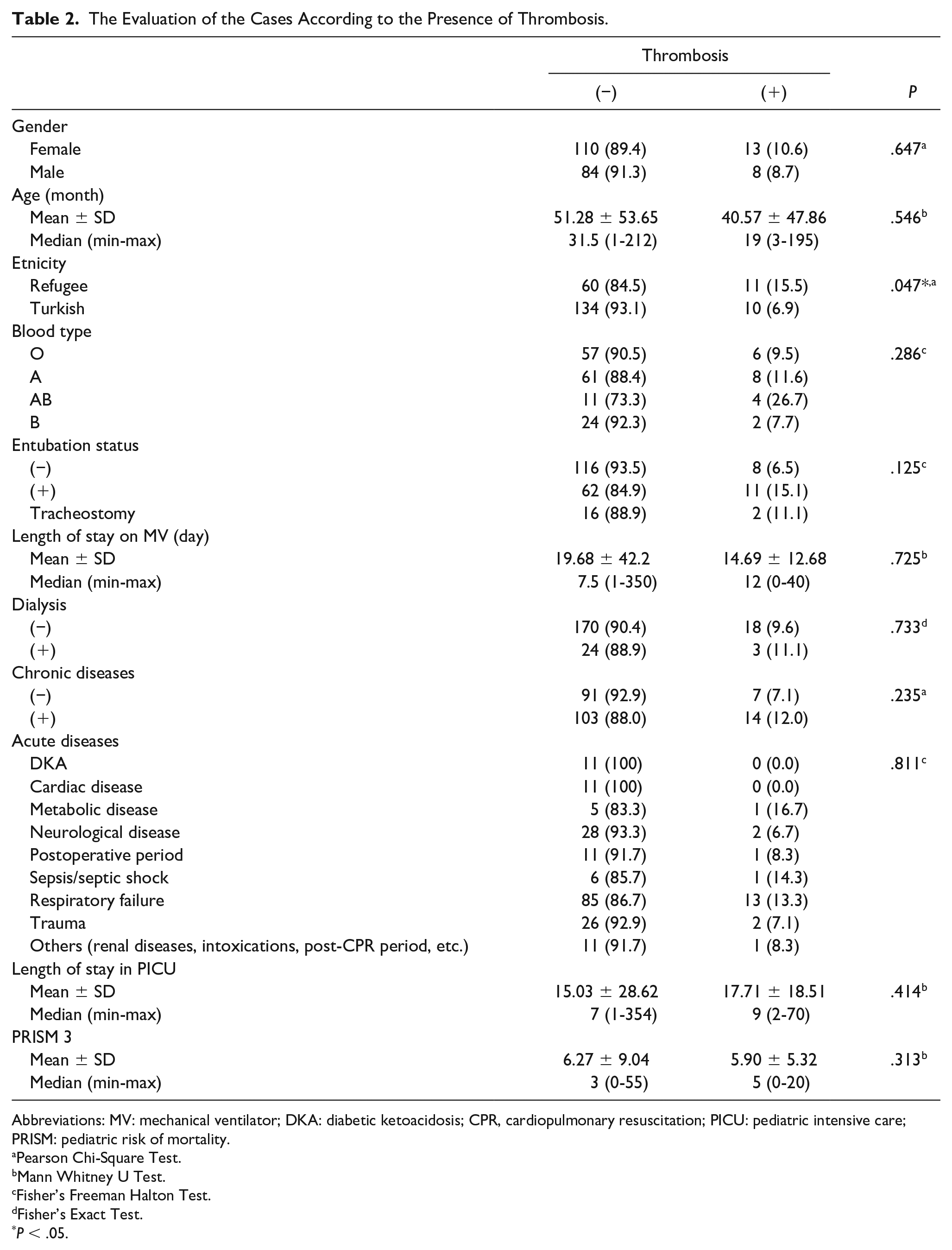
Abbreviations: MV: mechanical ventilator; DKA: diabetic ketoacidosis; CPR, cardiopulmonary resuscitation; PICU: pediatric intensive care; PRISM: pediatric risk of mortality.
Pearson Chi-Square Test.
Mann Whitney U Test.
Fisher’s Freeman Halton Test.
Fisher’s Exact Test.
P < .05.
The comparison of laboratory values according to the presence of thrombosis is shown in Table 3. The results revealed no statistically significant difference between the initial, mean, and peak glucose, sodium, and magnesium levels of the groups (P > .05). The evaluations made according to the infusion treatments applied to the cases are reported in Table 4. Our results revealed no significant differences in the development of thrombosis between the cases who received magnesium, blood product, inotrope, and 3% HTS infusion and those who did not receive any infusion therapy (P >.05).
The Comparison of Laboratory Values According to the Presence of Thrombosis.
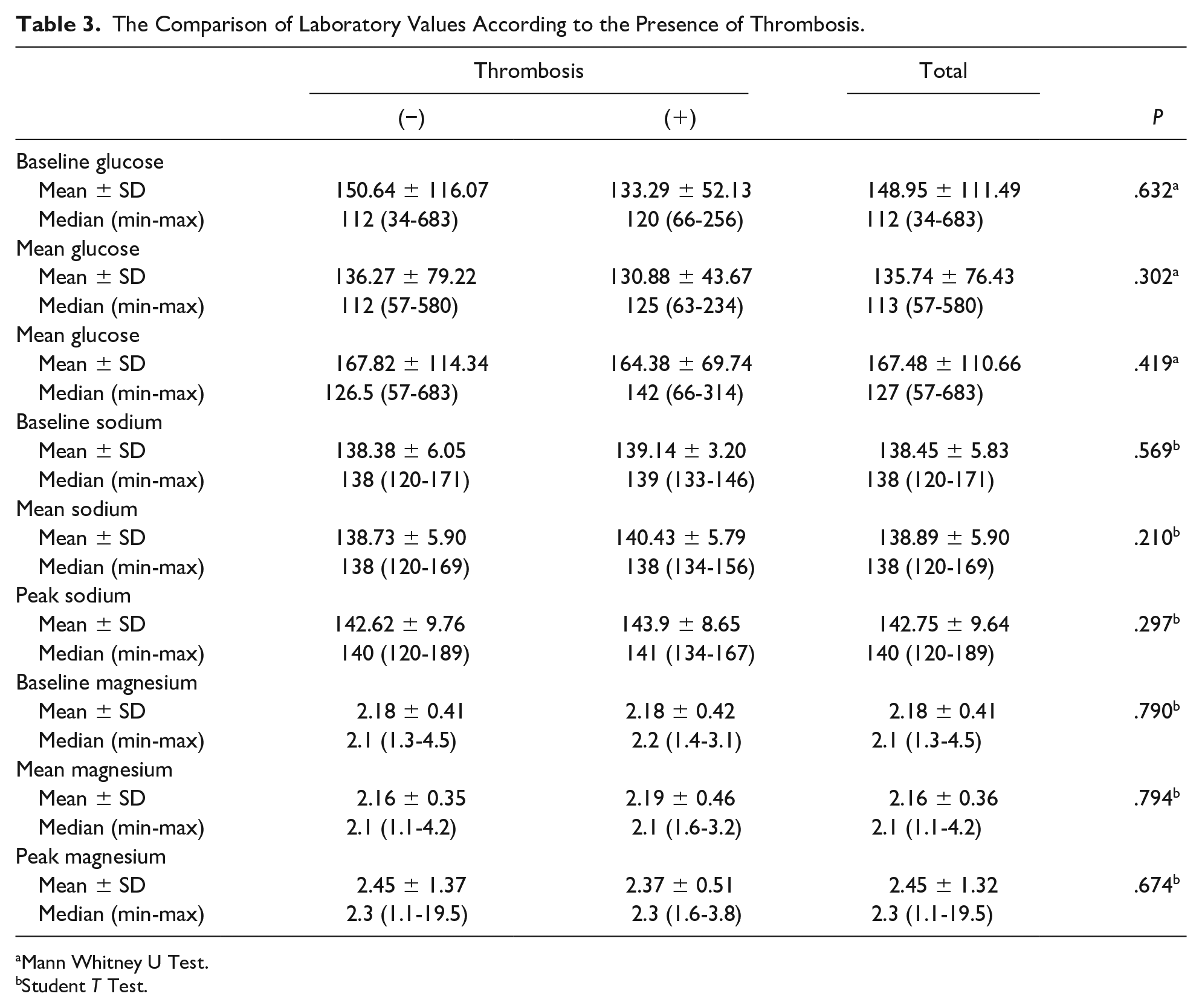
Mann Whitney U Test.
Student T Test.
The Evaluations Made According to the Infusion Treatments Applied to the Cases.
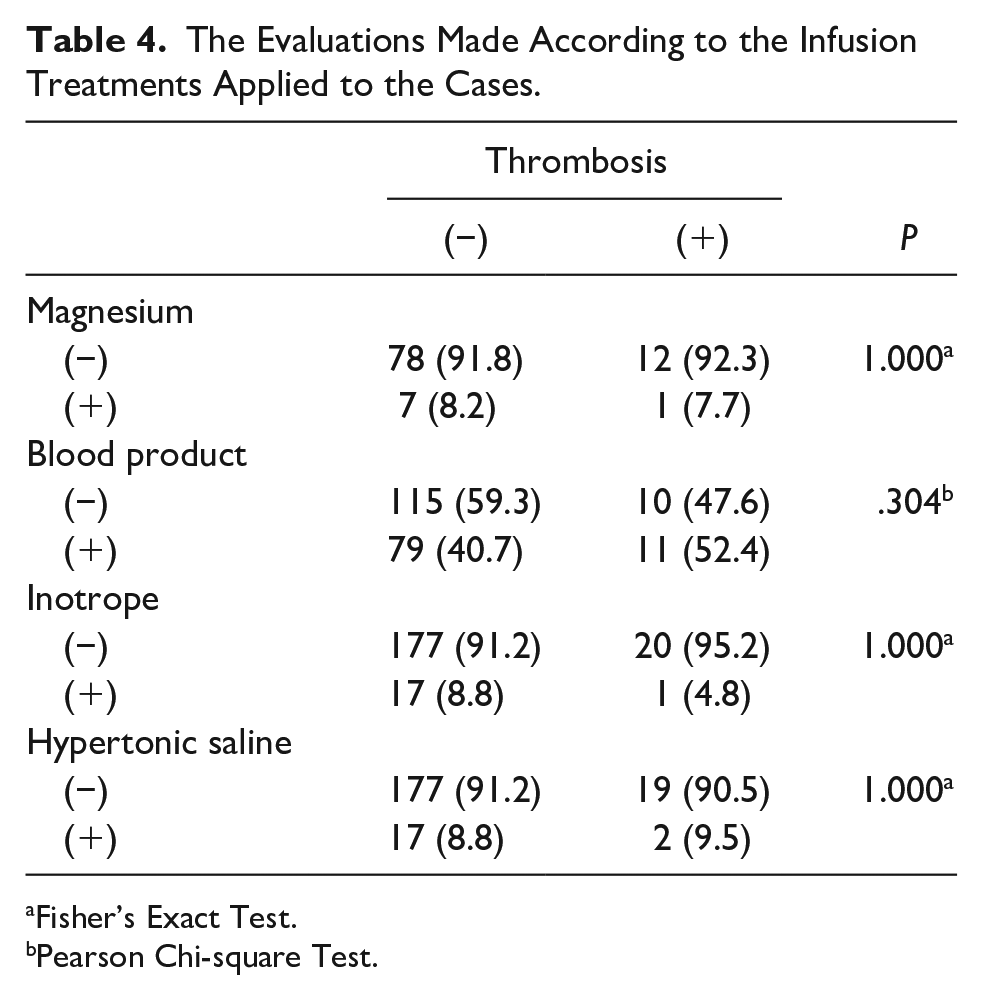
Fisher’s Exact Test.
Pearson Chi-square Test.
Discussion
In this study, the frequency of symptomatic CVC-a DVT was found to be 9.8%. The femoral vein is frequently used for CVC in children as it possesses a low risk of insertion-related complications, mostly does not require USG, and can be performed quickly in emergency situations. In the literature, the frequency of CVC-a DVT among critically ill children with femoral CVCs were reported ranging between 8% and 44%.7-10 The difference in rates is related to the diagnosis of asymptomatic cases by performing studies prospectively on CVC-a DVT, or whether only symptomatic cases are handled retrospectively. In our study, the incidence of CVC-a DVT was within the reported limits in literature but closer to the lower limit. This may be due to the heparin flushing process we used to ensure catheter patency, which is a standardized protocol that we performed in our unit but is not a general written policy. Since this procedure is applied in the same way in all cases, we do not think that it has an effect on other rates.
There is no evidence of timing of the development of CVC-a DVT in critically ill patients. Two prospective studies have reported that DVTs begin to develop within the first day and first week after CVC placement.8,10 Dubois et al, 11 however, could not report the timing of CVC-a DVT in their study. In our study, the onset of DVT to be symptomatic was between 2 days at the earliest and 25 days at the latest, with an average of 8.33 ± 5.65 days, which was in line with the literature.
CVCs placed in the jugular and femoral veins were evaluated in a prospective study conducted in 189 patients who were followed up especially for cardiac problems in the PICU, and age, number of CVC days, and Pediatric Index of Mortality-2 (PIM-2) score were not found to be associated with CVC-a DVT. 12 In our study, there was no statistically significant difference in the incidence of thrombosis with regard to gender, age, blood type, intubation status, length of stay on mechanical ventilator, presence of extra hemodialysis catheter, diagnosis of acute and chronic disease, length of stay in PICU, and PRISM-3 scoring. Other studies have found that individuals with non-O blood type had a higher risk of thrombosis due to higher factor VIII and Von Willebrand factor levels.13,14 In our study, although we did not analyze a correlation between thrombosis incidence and levels of coagulation factors and thrombosis was detected more in pediatric cases with A blood group, the incidence of thrombosis did not correlate with any blood types (P > .05). Gray et al 15 found longer hospital and intensive care unit stay in the DVT (+) group in their study including 333 patients under the age of 1. Similarly, Sandoval et al 16 found that children with DVT had longer in intensive care stay. In our study, length of stay in PICU of DVT (+) cases did not significantly differ from DVT (-) cases (P > .05). In a prospective study conducted in the general pediatric population, similar to our study, the presence of CVC-a DVT did not affect the length of stay in the PICU and did not increase the risk of mechanical ventilation. 17 However, in the same study, male gender was found to be a significant and independent risk factor for CVC-a DVT development (P = .049). Although female gender was more common in our cases, there was no statistical difference between genders in terms of thrombosis development (P > .05). While some studies have found a higher risk of femoral DVT, especially in the younger group, in our study, age did not make a difference in terms of thrombosis development (P > .05).8,10
In our study, the only significant difference between demographic data was seen in ethnic origin. Due to the location of our intensive care center, 1/3 of our cases consisted of refugees. In the study, the incidence of thrombosis in the refugee group was found to be statistically significantly higher than the Turkish population (P = .047; P < .05). Due to its geographical location, our country has become a country preferred by a large number of refugees in recent years, as it is on the route of international migration routes. During the time when the study was done, among the all cases which were admitted to our PICU, the rate of refugees was 56%, while this figure was 38% in general pediatric unit, and in neonatal intensive care unit (NICU) this figure was 47%. Life conditions, social status, and economic conditions may vary between refugees and Turks. These variations may give rise to the possibility on getting serious diseases in refugees. As a result of this, this situation might be responsible for making DVT development higher. Although we could not screen for the genetic factors that cause thrombosis due to the retrospective nature of our study, we think that genetic factors may also contribute to this situation. The effect of genetic factors, which are responsible for the development of thrombosis, is shown on the patients who are suffering from cancer. 18 Deficiency in protein C, S, and antithrombin III; mutation of factor V Leiden and prothrombin G20210A; the existence of antiphospholipid and anticardiolipin antibody; and activated protein C resistance are the most common hereditary risk factors for CVC-a DVT. 19 Previous studies reported that all these factors alone or in combination are associated with DVT in children. 20 Beside that the KIDCAT (KIDs with Catheter Associated Thrombosis) study showed that prothrombotic conditions do not have a significant effect on the development of CVC-a DVT. However, the researchers indicated that they performed this study only on patients with heart disease and placed a CVC for short-term perioperative care. 21
In a study of critically ill children, it was shown that the risk of clinically significant DVT is increased in the cases where blood glucose is >150 mg/dL. 22 Therefore, it is known that the risk of CVC-a DVT is high in children treated for diabetic ketoacidosis (DKA). In a series of 154 pediatric patients with DKA in whom femoral CVC was placed for 81, DVT was detected in 4 patients. 23 A total of 11 cases were diagnosed with DKA among our cases, and symptomatic DVT did not develop in any of them. We attributed this to the fact that the first treatment of DKA cases was carried out in the emergency department and that they came to the PICU with a slightly more moderate blood glucose levels. On the other hand, the fact that we did not prefer catheter placement due to the risk of thrombosis in patients with DKA led to low number of cases in this group. When we compared all the cases, the baseline, mean, and peak glucose levels did not differ statistically between the DVT (+) and (-) groups. Therefore, we could not obtain a borderline blood glucose level for the development of thrombosis. In the literature, a blood product transfusion within 24 hours after CVC is placed has been shown to increase the development of thrombosis. 24 In our series, the numbers in the groups who received blood product transfusion and who did not receive were close to each other, and both groups had similar rates in terms of thrombosis frequency. Other infusion treatments within the scope of our study were used in the acute period. Blood products, on the other hand, can be used in PICUs as a chronic choice in addition to emergency treatment in long-term hospitalized patients. In our study, the timing of blood product transfusion treatments could not be confirmed due to study limitations.
In our PICU, an infusion of 3% HTS is used for the treatment of severe traumatic brain injury (TBI) or another process with brain edema. Webster et al 25 found that the use of 3% HTS and a serum sodium level >160 mmol/L in children with severe TBI were associated with DVT. However, they also stated that treatment with 3% HTS is not a risk factor for DVT, and that the hyperosmolar state experienced by critically ill children may be associated with thrombotic complications. In our study, 3% HTS treatment was applied to 19 patients, while DVT was detected in 2 cases, and 3% HTS infusion treatment was not found to be associated with the development of thrombosis. Coritsidis et al 26 showed that while HTS treatment was given to 96 of 205 TBI cases, they reported no significant change in the incidence of DVT after 48 hours in the HTS group. The baseline, mean, and peak sodium levels of our cases did not differ between DVT (+) and (-) cases. We think that both the low number of cases and the fact that we did not calculate the 3% HTS dose cumulatively led to this result. It has been noted that infusion of inotropes typically at a slow and continuous rate promotes stasis in parallel, which in turn leads to catheter occlusion. 9 In a study using peripherally inserted central catheters lines, it was shown that simultaneous use of heparin infusion led to less cloth in the lines in the case group receiving continuous inotropic infusion. 27 Thrombosis developed in only one of 17 cases in which inotropic infusion was administered in our study, which was not statistically significant. In our PICU, patients hospitalized with status asthmaticus (SA) are treated with magnesium infusion in the acute period. Eight of our patients hospitalized for respiratory failure were diagnosed with SA, and magnesium infusion therapy was applied to these patients. The relationship between serum magnesium level and thrombosis was demonstrated in a study including a middle-aged male population, where serum magnesium level was not associated with future risk of venous thromboembolism. 28 In our study, there was no statistical difference between baseline, mean, and peak magnesium levels of DVT (+) and (-) cases. There was no difference in thrombosis in the magnesium infusion group.
The limitations of our study can be summarized as follows. Due to its retrospective nature, we could not have a comprehensive data analysis on all CVCs placed. The cases included in the study was from a single center, so our results may not be valid for other centers. Only cases with percutaneous non-tunneled femoral CVCs were included in the study, and those who were symptomatic were included. We considered other cases as DVT (-) and this may have led to missing some cases. We relied on USG as the imaging method, we did not need to do venography. Since we referred the cases to hematology outpatient clinics after discharge, it was not possible to record their long-term results. While other infusion therapies were used in the acute period after CVC insertion, we could not guarantee this for blood products, so the results for blood products on the timing of infusion were unclear. We did not focus on acute and chronic diseases because we divided the cases into 2 groups as DVT (+) and (-), which resulted in the small number of cases when evaluating laboratory parameters and infusion treatments.
In conclusion, critically ill children followed in the PICU are at risk for the development of CVC-a DVT. This risk is determined by the characteristics of the patient, the characteristics of the CVC, and the catheterization process itself. Clinical conditions such as hyperglycemia and hypernatremia, which have been shown in the literature as having an effect on the development of CVC-a DVT, and 3% HTS, blood product and inotropic infusion treatments were not found to have a significant effect on the development of thrombosis in our study. Likewise, no effect of serum magnesium level and magnesium infusion therapy on the development of thrombosis was detected. However, prospective, multicenter studies with higher number of cases are needed on this subject in order to make an evidence-based decision.
Author Contributions
Contributed to conception and design: U.K.B.; Contributed to conception: A.O., S.O.; Contributed to acquisition: U.K.B.; Contributed to analysis: A.O.; Contributed to design: S.O.; Contributed to acquisition and interpretation: M.Y.B.; Drafted manuscript: U.K.B., A.O., S.O.; Critically revised manuscript: U.K.B., A.O., M.Y.B.; Gave final approval: U.K.B., A.O., M.Y.B., S.O.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Ethics committee approval was obtained from a local ethics committee for the study.
Patient Consent
Due to the retrospective nature of the study, informed consent was not obtained either from the patients or their relatives.