
Abstract

Case Report
A 15-year-old female presented to the emergency department (ED) with chest pain. One month ago, the patient was noted to have cough, congestion, intermittent fever, and night sweats with a decrease in appetite. She was seen by her pediatrician at that time and sent home with chest wall pain and treated with oral corticosteroids. A week later, the patient’s chest pain had persisted, prompting the patient’s pediatrician to obtain a chest x-ray, which showed large right pleural effusion (Figure 1). Patient was sent to the ED for further evaluation. Patient’s medical history was notable for pityriasis rosea and chronic iron deficiency anemia. The patient had no history of surgeries and no allergies, and her birth history was unremarkable. Her family history was notable for mother with kidney stones and a paternal aunt with type I diabetes mellitus. Review of systems was positive for fever, chills, 10 pounds weight loss (over 1 month), fatigue, congestion, rhinorrhea, cough, shortness of breath, nausea, and headache.
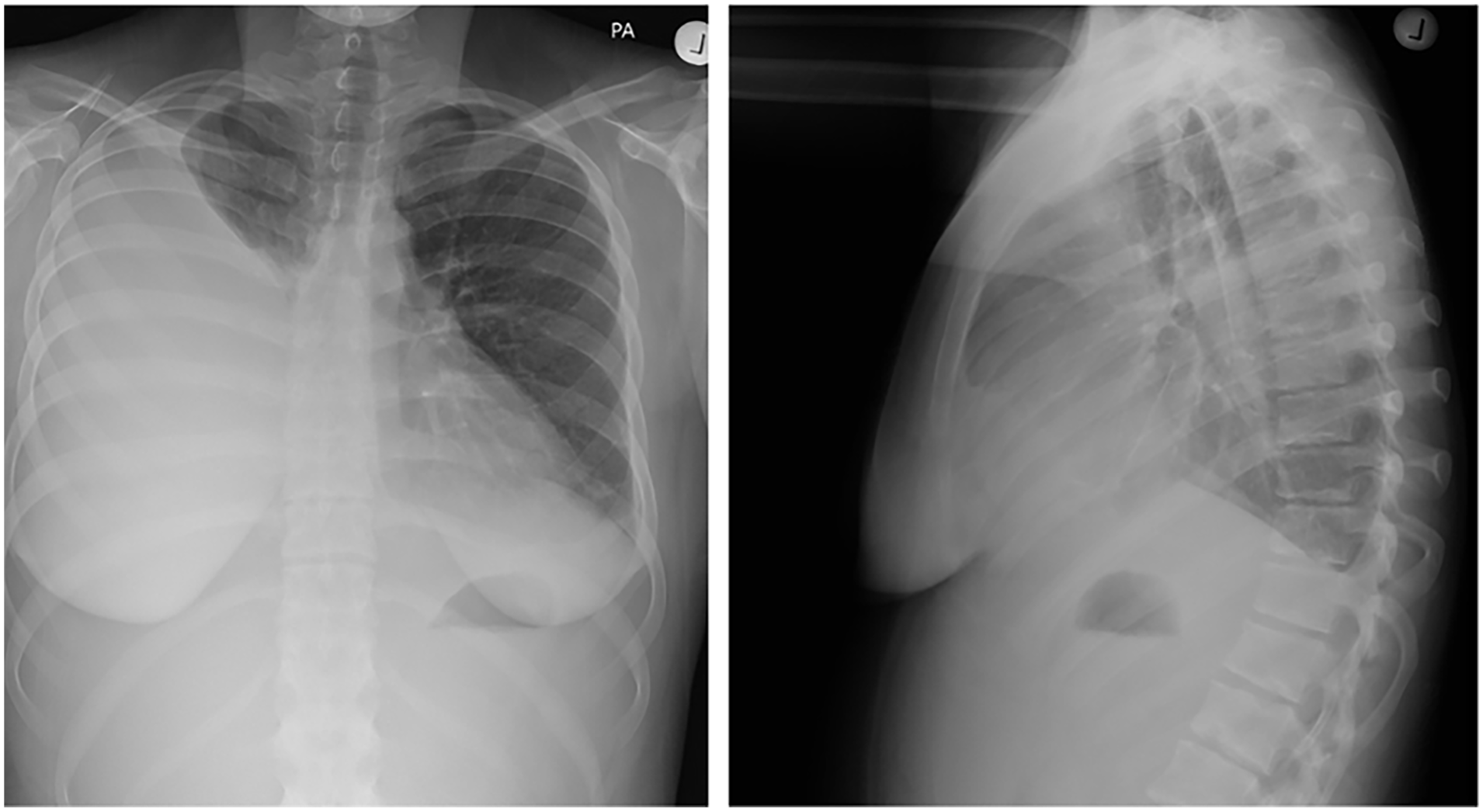
Chest x-ray [anterior posterior (AP) and lateral] completed outpatient by pediatrician showing right pleural effusion.
On arrival to the ED, vital signs included blood pressure of 138/85, pulse 114 bpm, temperature 98.3°F (36.8°C) oral, respiratory rate 22 breaths/min, and oxygen saturation 98% on room air. Physical examination was remarkable for decreased breath sounds on the right tachycardia and cervical adenopathy, with no organomegaly noted. Laboratories showed white blood cells (WBC) of 4.6 bil/L, hemoglobin 10.7 g/dL, mean corpuscular volume 87 fL, and platelets 535 bil/L. Basic metabolic panel included sodium 141 mmol/L, potassium 3.7 mmol/L, chloride 108 mmol/L, bicarbonate 22 mmol/L, glucose 83 mg/dL, blood urea nitrogen 10 mg/dL, creatinine 0.56 mg/dL, calcium 8.1 mg/dL, albumin 1.9 g/dL, and protein total 4.5 g/dL. Other labs included prothrombin time 11.8 seconds, partial thromboplastin time 34.1 seconds, uric acid 3.9 mg/dL, and lactate dehydrogenase 526 U/L. D-dimer elevated at >10 000 ng/ml FEU (fibrinogen equivalent unit). Urinalysis showed >500+ protein, 2+ blood, 6 to 10 red blood cells (RBC).
Computed tomography (CT) chest with intravenous (IV) contrast showed diffuse enlarged axillary lymph nodes bilaterally, right pleural effusion with complete atelectasis of right and middle lower lobes, trace pericardial effusion, and left pleural effusion. There was also concern of possible central filling defect in the right renal vein concerning thrombosis (Figure 2). Renal ultrasound showed a filling defect in the right renal vein consistent with thrombus with evidence of thrombus in the inferior vena cava. The CT abdomen/pelvis with IV contrast showed partial thrombosis of the right renal vein with mild diffuse anasarca. Multiple palpable nodes were noted in bilateral axilla, right supraclavicular, and left posterior cervical chain. Plan for core needle biopsy with thoracentesis was made and the patient was admitted to Pediatric Intensive Care Unit (PICU) where the definitive diagnosis was made on day 4 of admission.
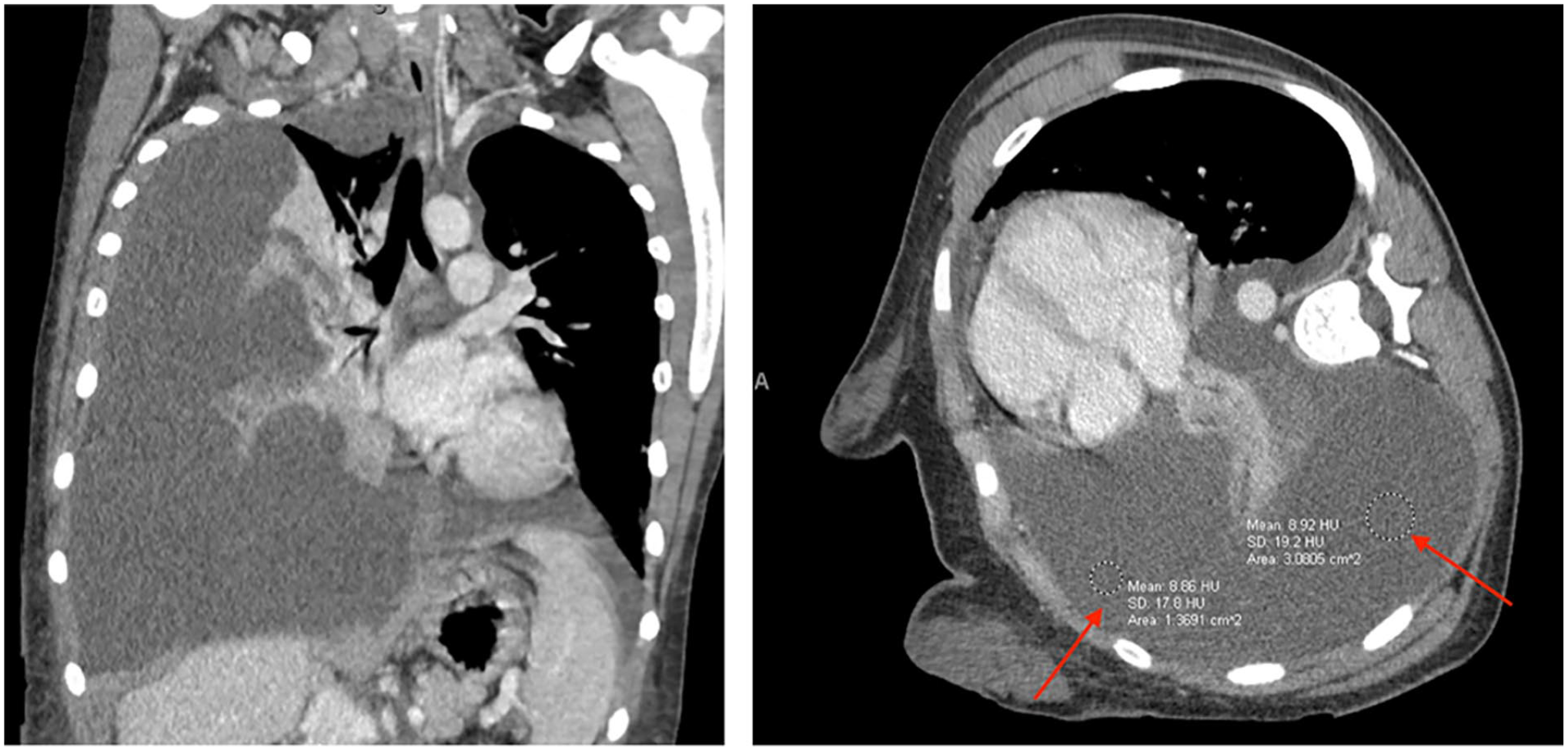
Chest computed tomography with intravenous contrast showed diffuse enlarged axillary lymph nodes bilaterally, redemonstration of right pleural effusion, trace left pleural effusion, and concern for possible central filling defect in right renal vein.
On arrival to the PICU, vital signs included blood pressure of 150/82 mmHg, pulse 107 bpm, temperature 98.3°F (36.8°C) oral, respiratory rate 22 breaths/min, and oxygen saturation 94% on room air. Patient was sedated and right thoracentesis was performed with 2.8 L serous fluid drained. Biopsy of supraclavicular nodes was obtained. Thoracentesis identified a transudative effusion with results as follows: yellow, clear, RBC <2,000, WBC 286, lactate dehydrogenase 178 U/L, glucose 82 mg/dL, triglycerides 57 mg/dL, culture: no polymorphonuclear neutrophil (PMN), no epithelial cells, no organisms, and total protein 2 g/dL (Figure 3). In the PICU, echo showed normal flow, ejection fraction of approximately 66% with normal systolic function.
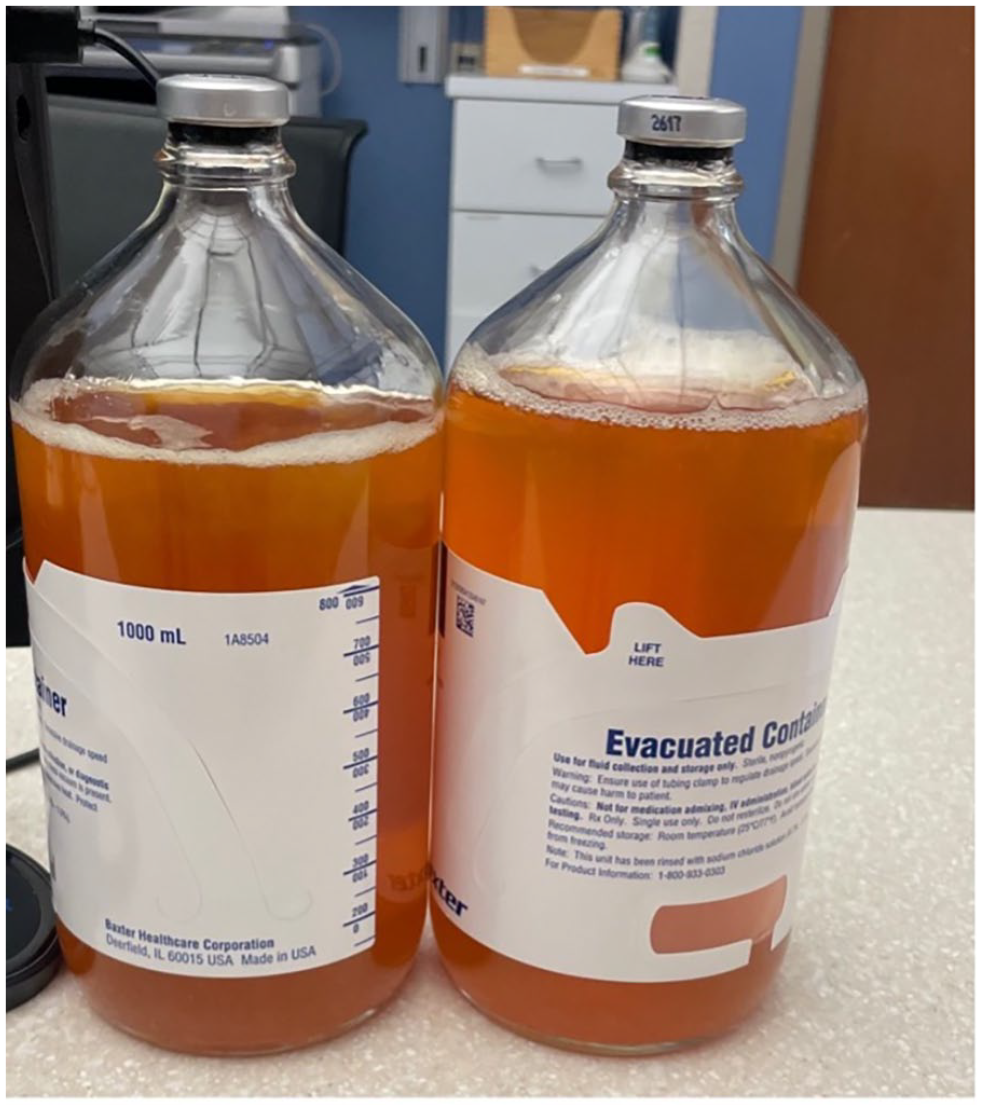
Thoracentesis-identified pleural fluid.
Lipid panel and spot protein creatinine ratio were added showing elevated cholesterol 259 mg/dL and triglycerides 196 mg/dL. Protein/creatinine ratio was 4.56. Patient was diagnosed with nephrotic syndrome. Anti-nuclear antibody was 1:640. Complement factors were sent resulting in decreased C3 (58) and C4 (8). Pediatric nephrology was consulted and recommended kidney biopsy. Biopsy showed immune complex glomerulonephritis consistent with lupus nephritis class IV (diffuse proliferative). Rheumatology was consulted and the patient was started on IV methylprednisolone, oral mycophenolate mofetil, and plaquenil. Patient was discharged home on day 8 of her hospital stay with outpatient follow-up.
Discussion
Chest pain is a common complaint in adolescents, but is rarely thought to be associated with life-threatening disease in the pediatric population. When approaching a teenager with chest pain, a wide array of etiologies must be considered, including idiopathic followed by musculoskeletal, psychogenic, gastrointestinal, cardiac, and respiratory. 1 Our patient was diagnosed with chest wall pain, which was thought to be secondary to an inflammatory condition, and was discharged home with oral corticosteroids. As of our knowledge, there is no evidence to suggest use of oral corticosteroids for chest wall pain. This may have masked the patient’s underlying etiology of chest pain. As our case demonstrated, there are occasional cases with serious pathology related to chest pain.
Our patient presented from an outpatient clinic with worsening chest pain associated with shortness of breath. Initial workup and examination revealed a pleural effusion. Pleural effusions, an abnormal accumulation of fluid in the pleural space, are less frequent in children and can be caused by a variety of infectious and noninfectious causes. 2 Pleural effusions in children are most commonly infectious, with noninfectious causes being rare. Our patient was diagnosed with lupus in the presence of a pleural effusion. Lupus is an autoimmune inflammatory disease that primarily affects woman and can affect any organ system. 3 It commonly presents with arthralgia, rash, and renal involvement. 4 Pulmonary involvement in lupus is common; however, pleural effusion is a rare first initial presentation of lupus, seen in 1% to 2% of patients. 5
Our patient’s case represents an unusual presentation of lupus in the context of chest pain, which is a common chief complaint that presents to the pediatric ED. Our patient initially presented with a pleural effusion. As with any other life-threatening condition, initial management is in the ED and is directed at ensuring adequate oxygenation and ventilation. Small pleural effusions generally are asymptomatic. As the effusion increases in size, as seen in our patient, symptoms such as chest pain and dyspnea may present with concern for acute respiratory compromise. At this point, a thoracostomy tube placement should be considered to evaluate the etiology of the underlying effusion. 6 In addition to identifying an effusion, it is important to consider life-threatening complications of lupus. Children with lupus often will have an underlying immunodeficiency secondary to loss of tolerance to autoantigens and will be in a hypercoagulable state secondary to loss of proteins such as antithrombin, protein C, and protein S.7,8 In these patients, it is essential to consider broad-spectrum antibiotics, correct any electrolyte abnormalities, and start anticoagulation as needed. It is also important to limit exposure to nephrotoxic agents such as contrast dye used in tests. Our patient received 2 doses of contrast for separate CT images, which should have been avoided in a patient who ultimately was diagnosed with renal disease.
Conclusion
Chest pain in pediatric patients is common and most often benign. We present an unusual case of chest pain in an adolescent girl with a common presentation but a different outcome. The history and physical examination in this case led to further investigation into the cause of the chest pain, ultimately leading to a diagnosis of pleural effusion and lupus. Prompt diagnosis and treatment is important. The cause for chest pain was not initially clear in our patient; however, keeping a broad differential and recognizing key signs of systemic illness were essential to the diagnosis in our patient.
Author Contributions
A.G. contributed to conception, design, analysis, drafting of manuscript and final approval. E.N. and B.J. contributed to conception, design, analysis, revision and final approval of manuscript.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethic Approval/Patient Consent
This case report did not require IRB approval for completion.