
Abstract

Educational Objectives
Recognize spontaneous intracranial hypotension as an etiology of postural headache in patients with Marfan syndrome.
Examine the differences in management strategies for spontaneous intracranial hypotension and postural orthostatic tachycardia syndrome.
Case Report
A 17-year-old woman with Marfan syndrome complicated by scoliosis, mitral valve prolapse, and bilateral lens subluxation presented to the emergency department (ED) with a 2-week history of postural frontal headache. The patient described the headache as “throbbing,” worse in the morning, and at its worst (4-5/10) when she was sitting or standing or upon Valsalva maneuver. She reported subjective palpitations with sitting up and standing, but she otherwise denied changes in vision, photophobia, phonophobia, dizziness, or change in appetite. Her headache only improved when lying supine and was refractory to acetaminophen. She denied fevers, dizziness, syncope, weakness, trouble speaking, or decreased sensation.
Physical examination was notable for tall stature, thin body habitus, arachnodactyly, increased arm-to-height ratio, joint hypermobility, and a loud blowing systolic murmur at the apex. Specifically, her weight was in the 9th percentile and height in the 96th percentile, correlating to a body mass index of 14.8 kg/m2 (0.02th percentile). Initial vital signs showed a heart rate of 64 bpm supine that increased to 120 bpm upon standing with a respective blood pressure change of 99/57 to 88/57 mm Hg. Her neurologic examination was unremarkable, and a fast-brain magnetic resonance imaging (MRI) was negative. Analgesic therapy was administered in the ED without significant improvement.
An electrocardiogram and echocardiogram were stable from previous cardiology visits. Multiple intravenous fluid boluses were administered but she remained symptomatic and began experiencing postural vomiting refractory to antiemetics. Given the ongoing nature of her symptoms and inability to tolerate PO, she was hospitalized for further evaluation. At the time of admission, the primary consideration was postural orthostatic tachycardia syndrome (POTS), and additional intravenous fluids were planned.
Discussion: Hospital Course
Due to lack of improvement in postural symptoms with 48 hours of analgesics and fluid resuscitation and with knowledge that symptom onset had been relatively sudden, consideration was made for a diagnosis of spontaneous intracranial hypotension (SIH). Pediatric neurology was consulted and MRI of the brain, cervical, thoracic, and lumbar spine were completed. A volumetric MRI of the lumbar spine showed prominent dural ectasia and a fluid signal extending from the L5 and S1 nerve root sleeves into the L5 perifacet soft tissues and iliopsoas muscle, concerning for cerebrospinal fluid (CSF) leak (see Figure 1). A follow-up computed tomographic (CT) myelogram of the lumbar spine confirmed the presence of large nerve root sleeve dilations, sleeve cysts, and diverticula in the dura. Contrast leakage was seen around the dilated S1 nerve root sleeve, confirming that this was the origin of the suspected CSF leak (see Figure 2). An autologous epidural blood patch at the site of the suspected leak was performed later the same day. At the time of discharge, her symptoms had completely resolved. She continued to be symptom-free several months following hospital discharge and did not require a second blood patch.
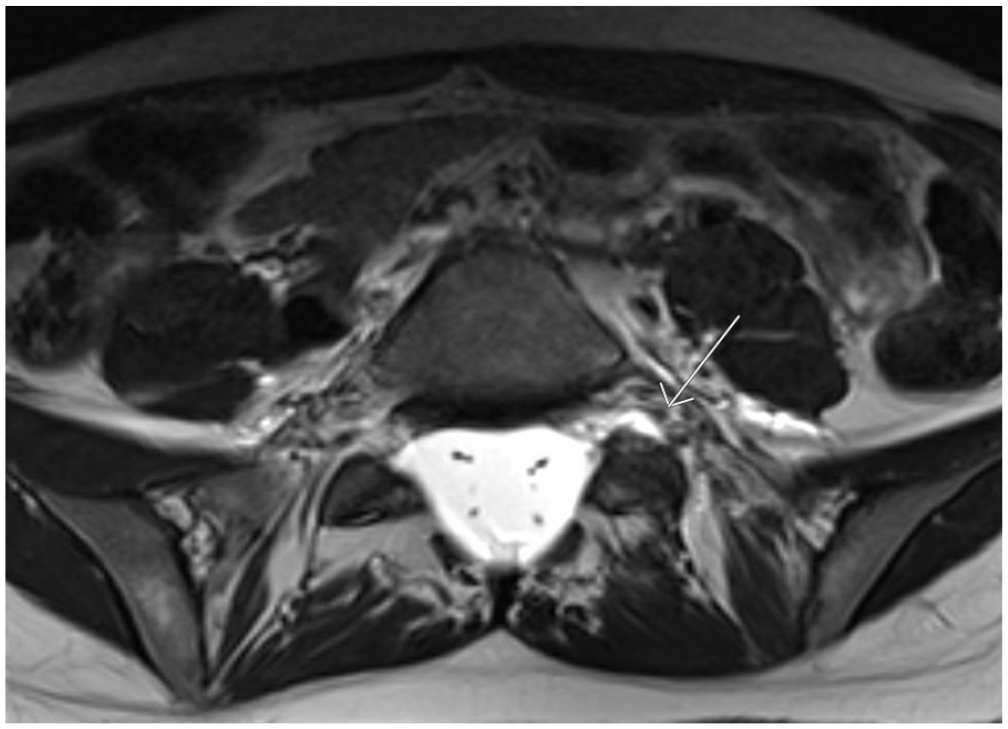
Magnetic resonance imaging of the lumbar spine demonstrating a fluid signal extending from the left L5 and S1 nerve root sleeves into the perifacet tissues and to the left iliopsoas muscle concerning for site of cerebrospinal fluid leak.
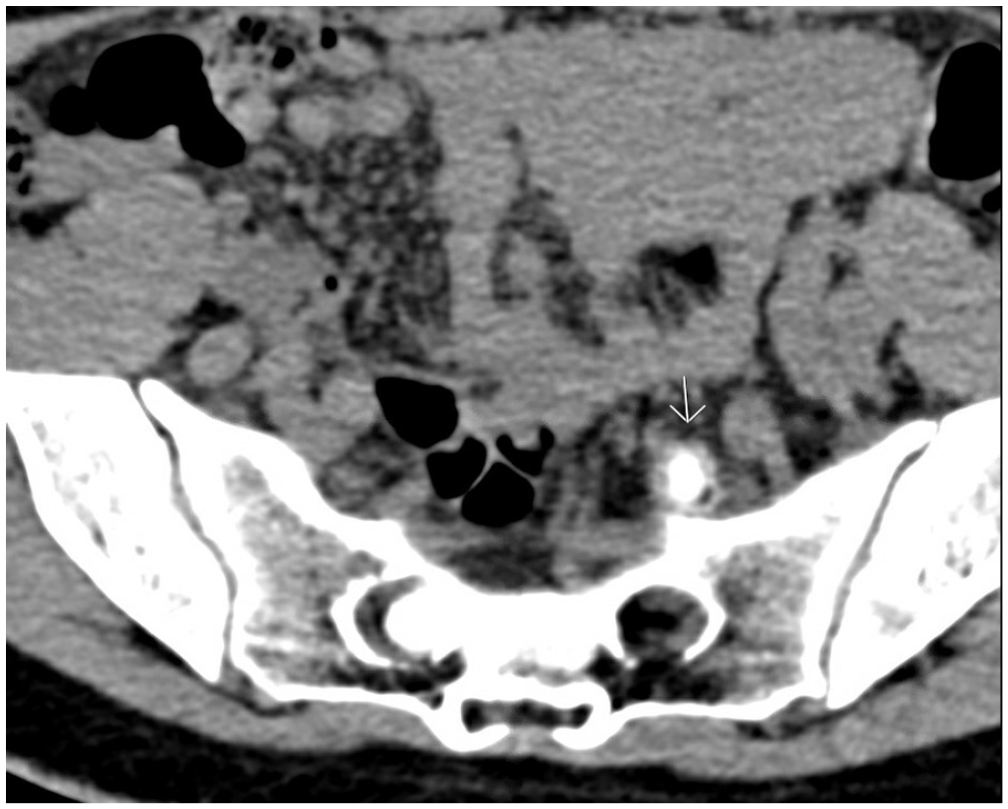
Computed tomographic myelogram of the lumbar spine, which shows and area of contrast surrounding the dilated left S1 nerve root sleeve, confirming the focus for a cerebrospinal fluid leak.
Case Discussion
Marfan syndrome is an inherited autosomal dominant connective tissue disease caused by a defect in the fibrillin-1 protein affecting 1 in 5000 people in the United States. 1 Spontaneous intracranial hypotension is a rare but documented complication of Marfan syndrome. The diagnostic criteria for SIH provided by the International Headache Society are as follows: low CSF pressure (<60 mm CSF) and/or evidence of CSF leakage on imaging; headache that develops in temporal relation to the low CSF pressure or CSF leakage or led to its discovery; and headache not better accounted for by another International Classification of Headache Disorders, Third Edition (ICHD-3) diagnosis. 2 Dural ectasia is the progressive dilation of the dural sac, leading to thinning of the meninges, structural compromise, and eventual formation of small meningeal diverticula prone to CSF leakage over time.3,4 Dural ectasia is a major manifestation of Marfan syndrome according to the revised Ghent criteria, 5 though symptoms are most often absent to mild (low back pain, headache, leg pain). 6 As Marfan syndrome affects connective tissue, patients are at a higher risk of weakened dura. Subsequently, even normal physiologic pressures of CSF flow can lead to progressive dural ectasia which increases the risk for spontaneous CSF leak upon minor unrecognized trauma to the area. 7
Spontaneous intracranial hypotension typically presents with orthostatic headache but can also include vomiting, diplopia, tinnitus, photophobia, and hyperacusis, 8 similar to symptoms of POTS, another common complication in patients with connective tissue disorders.9,10 Postural orthostatic tachycardia syndrome is an increasingly common diagnosis in adolescent women, 11 and individuals in this population may be at increased risk of misdiagnosis. Some studies have shown that POTS may also cause orthostatic headache, though the mechanism behind this is not well understood.12,13
The overlap in symptoms between SIH and POTS in patients with Marfan syndrome presents a diagnostic challenge and has opposite approaches in management. The mainstay of treatment for POTS is conservative including regular cardiovascular training, hyperhydration, and increased salt intake, 14 whereas first-line treatment for SIH includes bed rest, activity limitation, and the option of blood patch for severe cases. 3 It is therefore important to consider whether additional imaging is warranted to rule out SIH in high-risk patients, as misdiagnosis could not only exacerbate symptoms but also delay treatment with blood patch intervention. Brain MRI is the most sensitive single imaging test for diagnosing SIH and should be performed first if this diagnosis is suspected. Magnetic resonance imaging may show signs of low CSF, such as dural enhancement, brain sagging, venous distension, or pituitary engorgement. Spinal CT myelography is considered the gold standard for detection of spinal CSF leakage and is often used to confirm the diagnosis. 3 A possible algorithm for workup of SIH from an imaging standpoint is as follows: complete neuro-axis MRI; if negative, complete neuro-axis CT myelogram; if negative, dynamic CT myelogram with or without digital subtraction myelogram. If imaging is still negative but there is a strong clinical suspicion, consideration can be given to empiric large volume blood patch, followed by a second blood patch if there is no improvement of symptoms.
Final Diagnosis
Spontaneous intracranial hypotension secondary to spontaneous CSF leak.
Conclusion
This patient demonstrates a case of dural ectasia leading to spontaneous CSF leak and subsequent SIH. This is a rare complication of Marfan syndrome and other connective tissue disorders that have an increased risk for spinal meningeal weakening. We recommend including SIH in the differential diagnosis for patients with Marfan syndrome who present with symptoms of intracranial hypotension, such as postural headache and nausea refractory to supportive care. In the case of our patient, relief was achieved following a single autologous epidural blood patch procedure, but it is not uncommon for patients to have a relapse of symptoms requiring repeated intervention. Given the overlap in symptoms but opposing approaches to management between SIH and POTS, it is crucial to consider both diagnoses as part of a thorough workup of orthostatic headaches in adolescent patients with connective tissue disorders.
Footnotes
Acknowledgements
We thank Justin Chetta, MD, who provided radiology reads and images.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Victoria Delk has nothing to disclose; Hannah Ballock has nothing to disclose; Sarah Mennito has nothing to disclose; Umakanthan Kavin discloses the following: Pfizer shareholder.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Written informed consent was given by both patient and guardian for publication of this case report and for the individual’s data to appear in this report.