
Abstract
Considering the possible adverse effects of thyroid autoantibodies on the brain, the present study aimed to investigate whether there was a difference in mental health difficulties and mindfulness awareness levels between subclinical Hashimoto’s thyroiditis patients with and without levothyroxine (LT4) use. A case-control study was conducted. The Strengths and Difficulties Questionnaire (SDQ) and the Mindful Attention Awareness Scale (MAAS) were used to screen mental health difficulties and mindfulness awareness. Scale scores were compared by performing correlation analysis between the groups with respect to LT4 use and thyroid autoantibodies. Levothyroxine alone does not affect scale results. Higher thyroid peroxidase antibody (TPOAb) titers were positively correlated with the behavioral problems subscale of the SDQ, while awareness level in patients was inversely correlated with higher thyroglobulin antibody (TgAb) levels.
Introduction
Hashimoto’s thyroiditis, also known as chronic lymphocytic thyroiditis, is the most common cause of hypothyroidism in adolescents. 1 It is an autoimmune disease in which autoantibodies (thyroid peroxidase antibody [TPOAb], more commonly, and thyroglobulin antibody [TgAb]) cause chronic thyroid inflammation. More thyroid gland damage is seen in the presence of high levels of antibodies. 2 Apart from the classical findings of hypothyroidism in Hashimoto’s thyroiditis (HT), many psychiatric conditions may arise. The most common psychiatric symptoms in HT are cognitive disorders characterized by a slowdown in mental function, memory disorders, impaired abstract thinking, and mood disorders. 3 In some patients, these findings develop in the later stages of the disease, and in others, they may be the first clinical finding, even if the patients are in the euthyroid phase. Thyroid hormones have an essential role in the development and differentiation of the nervous system by affecting the migration, differentiation, myelination, and synaptogenesis of cells, which continues throughout life. 4 Thyroid hormones also contribute to repairing damage in the central nervous system by positively affecting synaptic plasticity with their neurotrophic effects. 5 Although some inconsistent data exist on the relationship between subclinical hypothyroidism and impaired neuropsychological development, many studies have shown that subclinical thyroid dysfunction may have a negative effect on psychometric tests, which have been shown to be improved with LT4 therapy. On the other hand, the effect of thyroid autoantibodies on brain structure and function is unclear. Although thyroid hormone levels are normalized with LT4 therapy, antibody levels do not completely return to normal. And it is rarely useful to repeat measurements of their levels, which does not influence the treatment given. 6
The present study aimed to investigate whether there was a difference between mental health difficulties and mindfulness awareness levels in HT patients who were euthyroid without the need for LT4 support and in those who were euthyroid under LT4 treatment.
Materials and Methods
Study Population
Acase-control study was conducted. The case subjects consisted of adolescents with HT referred to the pediatric endocrinology outpatient clinic. The health control group was selected using continuous sampling at the same outpatient clinic. Inclusion criteria for the study groups are given in Table 1.
Inclusion and Exclusion Criteria of Participants in the Study.
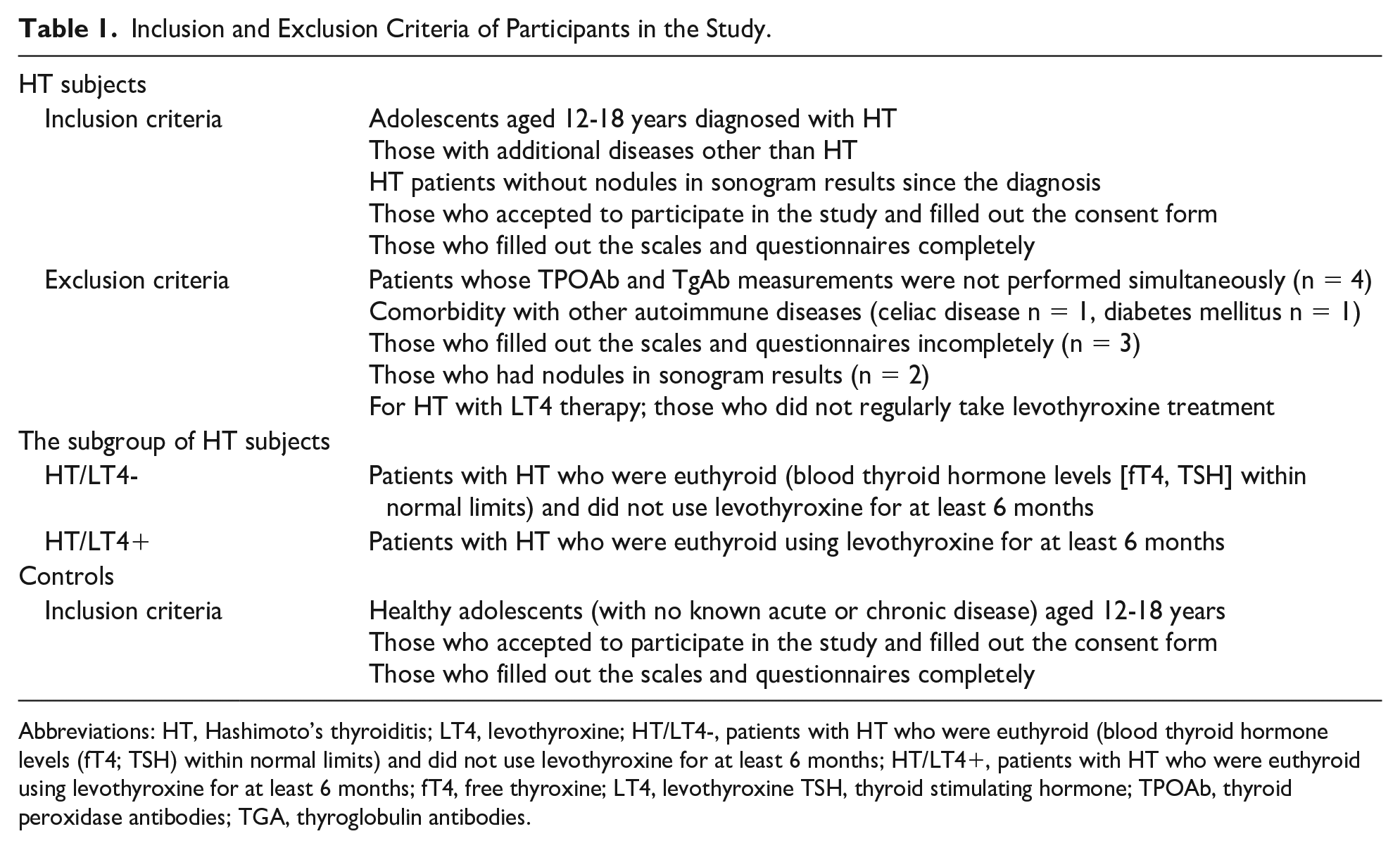
Abbreviations: HT, Hashimoto’s thyroiditis; LT4, levothyroxine; HT/LT4-, patients with HT who were euthyroid (blood thyroid hormone levels (fT4; TSH) within normal limits) and did not use levothyroxine for at least 6 months; HT/LT4+, patients with HT who were euthyroid using levothyroxine for at least 6 months; fT4, free thyroxine; LT4, levothyroxine TSH, thyroid stimulating hormone; TPOAb, thyroid peroxidase antibodies; TGA, thyroglobulin antibodies.
The diagnosis of HT was based on medical history, clinical findings, and serum levels for fT4 and TSH. Serum levels of fT4, TSH, antithyroglobulin antibody, and antithyroid peroxidase antibody were measured using an electrochemiluminescence immunoassay method with a Beckman Coulter DxI 800 analyzer (Beckman Coulter Access kit, Beckman Coulter, Inc. • 250 S. Kraemer Blvd. • Brea, CA 92821 USA). The normal reference ranges for fT4, and TSH applied in our study were 0.69 to 1.2 ng/dL and 0.5 to 4.7 mIU/L, respectively. The measurements of T4 and TSH are detailed in NHANES III.7,8 Thyroid peroxidase antibody (TPOAb) and thyroglobulin antibody (TgAb) titers at the diagnosis were noted from medical records. Patients with serum TSH levels between ≥5 ng/dL and <10 ng/dL with fT4 levels within the normal range for at least the last 6 months were evaluated as mild SCH, and LT4 treatment was not initiated. 9 These patients constituted HT without LT4 therapy. Those with TSH levels >10 mIU/L and fT4 levels within normal limits and those with TSH levels>4.7 mIU/L with fT4 levels<0.69 ng/dL were evaluated as severe SCH and overt hypothyroidism, respectively, and LT4 treatment was initiated. These patients constituted HT with LT4 therapy.
Due to the possibility that abnormal thyroid hormone levels may adversely affect neurocognition, 10 only euthyroid patients were included in the study so that the scale results would not be affected.
Socio-Demographic Data Collection
A self-report questionnaire prepared by the researchers, which included age, gender, height, weight, mode of delivery, birth week, birth weight, educational level of parents, their school grade, and the family’s economic status was used. Parental education level was categorized as less or more than 8 years. School success was asked according to the adolescent’s own description and divided into 3 categories good, medium, or poor. Likewise, the economic situation of the families was divided into 3 parts as good, medium, or poor. The economic status of the families was self-reported and defined by themselves. Anthropometric data were collected at the time of enrollment. Body mass index (BMI) was calculated on the basis of weight in kilograms and height in meters according to the formula kg/m2. Body mass index standard deviation score (SDS), weight SDS, and height SDS were calculated according to age- and sex-specific reference values. 11
The Scales
The participants themselves completed the scales in a separate room next to the endocrinology outpatient clinic. Participants who filled out the scales incompletely were not included in the study.
Mindful Attention Awareness Scale (MAAS)
MAAS is a 15-item scale designed to assess a core characteristic of mindfulness, namely, a receptive state of mind in which attention, informed by a sensitive awareness of what is occurring in the present, simply observes what is taking place. The MAAS is a 6-point Likert-type scale consisting of 15 items. Each item is scored between 1 (almost always) and 6 (almost never). Internal consistency was found to be α = 0.82 (n = 327) in the student sample and α = 0.87 (n = 239) in the general adult sample. The scores range from 15 to 90, with higher scores indicating a greater level of mindfulness. Mindful Attention Awareness Scale test-retest results were also quite high (r = 0.81). Internal consistency α = 0.78 (n = 100), a test-retest result of 0.83 (n = 78), internal consistency α = 0.80 (n = 78), and a test-retest correlation result of 0.86 were found in adult sample studies. 12 High scores on the scale indicate high mindfulness. The Turkish validation of the scale was performed by Özyeşil et al in 2011. The Cronbach’s alpha internal consistency coefficient of the scale was found to be .80. 13
Strengths and Difficulties Questionnaire (SDQ)
SDQ is used to detect mental health difficulties. It is a brief behavioral questionnaire that consists of 5 subscales, each containing 5 items. The scales measure emotional symptoms, conduct problems, hyperactivity-inattention, peer relationship problems, and prosocial behaviors. Respondents indicate on a 3-point Likert-type scale to what extent a symptom applies to them, using the options “Not true,” “Somewhat true,” or “Certainly true.” Each of the subscales consists of 5 items and scale scores ranging from 0 to 10. A higher score is indicative of more problems for all subscales, except for the prosocial scale, where higher scores correspond to fewer difficulties in prosocial behavior. The total score is calculated by summing the scores of the subscales except for the prosocial behavior score. The resulting score ranges from 0 to 40 and is counted as missing if one of the four-component scores is missing. The internal consistency coefficient Cronbach’s α was adequate for the SDQ total difficulties scale (α = 0.78) and for the subscale emotional problems (α = 0.73), but low for hyperactivity-inattention (α = 0.69) and prosocial behaviors (α = 0.63), and poor for peer problems (α = 0.57) and for conduct problems (α = 0.47). 14 Turkish validation of the scale was adapted into Turkish by Güvenir et al in 2008. 15
Ethical Consideration
The study was approved by the local ethics committee of Çanakkale Onsekiz Mart University Faculty of Medicine Hospital Ethics Committee and conducted in accordance with the principles of the Declaration of Helsinki (2011-KAEK-27/2019-E.1900172607). Participants were recruited for the study after informed consent was obtained from both them and their parents.
Data Analysis
Data were examined with the Shapiro-Wilk test to determine whether it had a normal distribution. Results are presented as mean ± standard deviation, median (interquartile range), or frequency and percentage. Normally distributed data were compared with independent samples t-test or one-way analysis of variance (ANOVA). Kruskal Wallis and Mann Whitney U tests were used for non-normally distributed data. The Bonferroni correction was used to adjust for multiple comparisons where appropriate. The Pearson correlation was used for the comparison between HT patients. Categorical variables were compared using Pearson’s chi-square test and Fisher’s exact test between groups. P < .05 was considered the significance level. Statistical analyses were performed with IBM SPSS ver.23.0 (IBM Corp. Released 2015. IBM SPSS Statistics for Windows, Version 23.0. Armonk, NY: IBM Corp.).
Results
The study included 86 adolescents with HT and 63 healthy adolescents as controls. The HT subjects and the control groups were composed of 86% girls and 73% girls, respectively. The median age of the HT subjects was 15.35 years, and 14.70 years for the control group. The sociodemographic data of the participants, together with the statistical results, are summarized in Table 2.
Sociodemographic Characteristics and Anthropometric Parameters of the Participants.
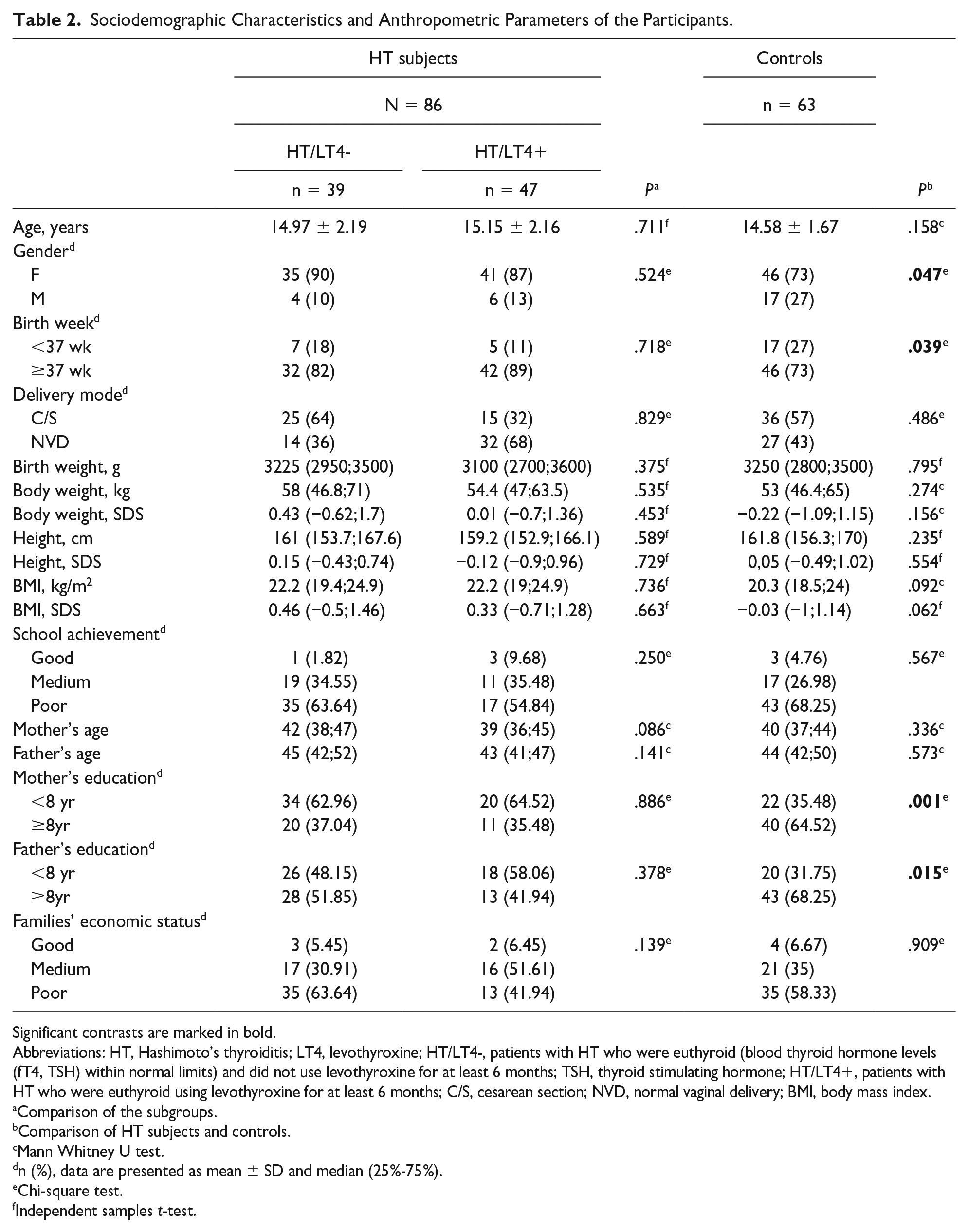
Significant contrasts are marked in bold.
Abbreviations: HT, Hashimoto’s thyroiditis; LT4, levothyroxine; HT/LT4-, patients with HT who were euthyroid (blood thyroid hormone levels (fT4, TSH) within normal limits) and did not use levothyroxine for at least 6 months; TSH, thyroid stimulating hormone; HT/LT4+, patients with HT who were euthyroid using levothyroxine for at least 6 months; C/S, cesarean section; NVD, normal vaginal delivery; BMI, body mass index.
Comparison of the subgroups.
Comparison of HT subjects and controls.
Mann Whitney U test.
n (%), data are presented as mean ± SD and median (25%-75%).
Chi-square test.
Independent samples t-test.
While no difference was found between MAAS scores in the groups, SDQ total score was found to be statistically significantly higher in the health control group (P < .001). Emotional symptoms and conduct problem subscale scores of the scale were found to be higher in the healthy control group (each resulted in P < .001). Scale score comparisons between the groups are given in Table 3.
Comparison of MAAS and SDQ Scale Scores.
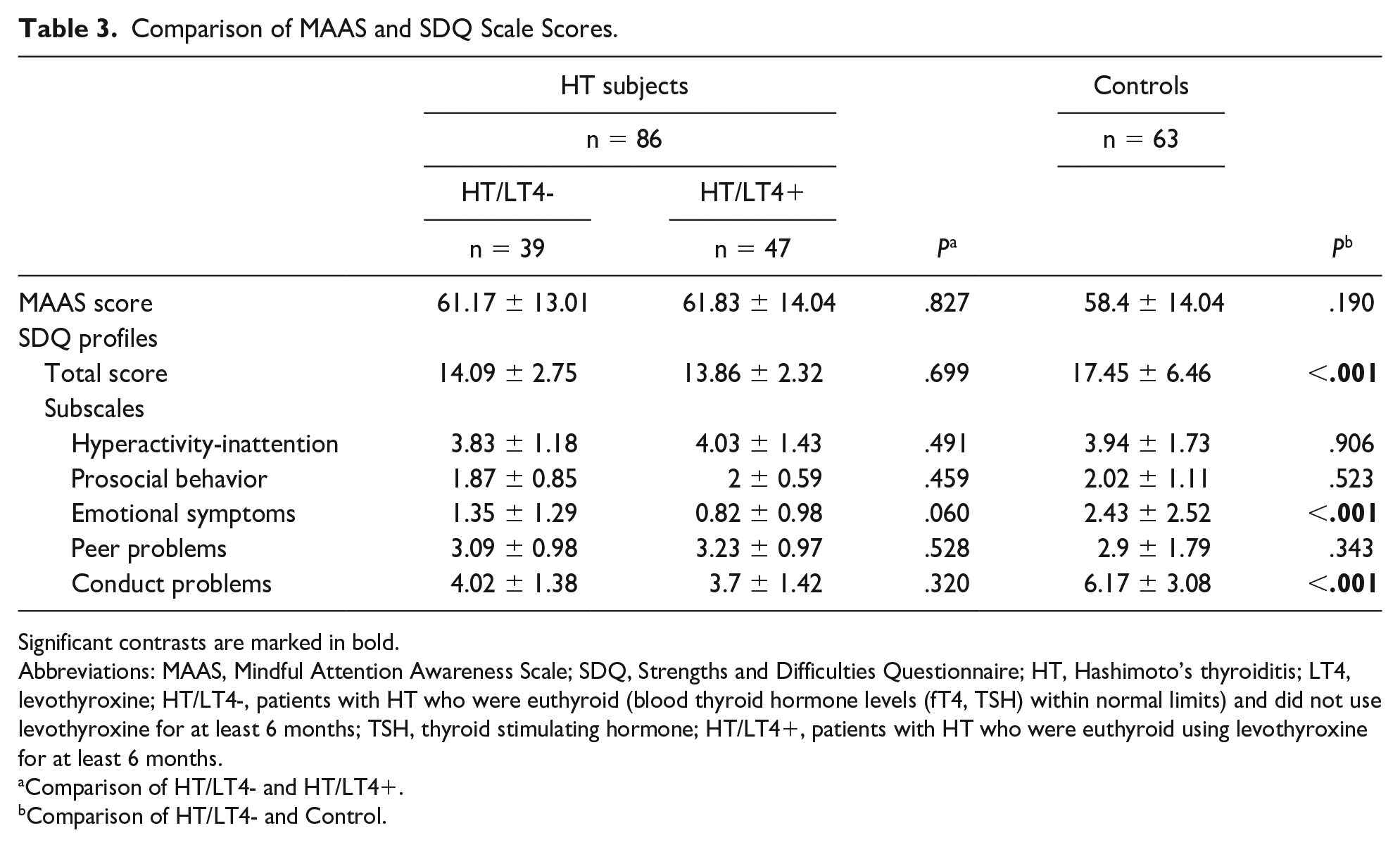
Significant contrasts are marked in bold.
Abbreviations: MAAS, Mindful Attention Awareness Scale; SDQ, Strengths and Difficulties Questionnaire; HT, Hashimoto’s thyroiditis; LT4, levothyroxine; HT/LT4-, patients with HT who were euthyroid (blood thyroid hormone levels (fT4, TSH) within normal limits) and did not use levothyroxine for at least 6 months; TSH, thyroid stimulating hormone; HT/LT4+, patients with HT who were euthyroid using levothyroxine for at least 6 months.
Comparison of HT/LT4- and HT/LT4+.
Comparison of HT/LT4- and Control.
As TPOAb levels increased in the HT subjects, hyperactivity-inattention and conduct problem scores were found to decrease (r = -0.219; P = .04, r = -0.249; P = .02). It was determined that the MAAS score decreased with the increase in TgAb level (r = -0.273; P = .01). Thyroid autoantibody levels were similar in patients who received or did not receive LT4 (P = .111). The mean duration of HT in the HT without LT4 therapy group was 21.67 ± 18.65 months and 27.6 ± 19.65 months in the HT with LT4 therapy group (P = .046). The total SDQ score decreased as the disease duration increased in HT with LT4 therapy (Table 4).
Correlation Analysis Between HT Duration and MAAS and SDQ Scores.
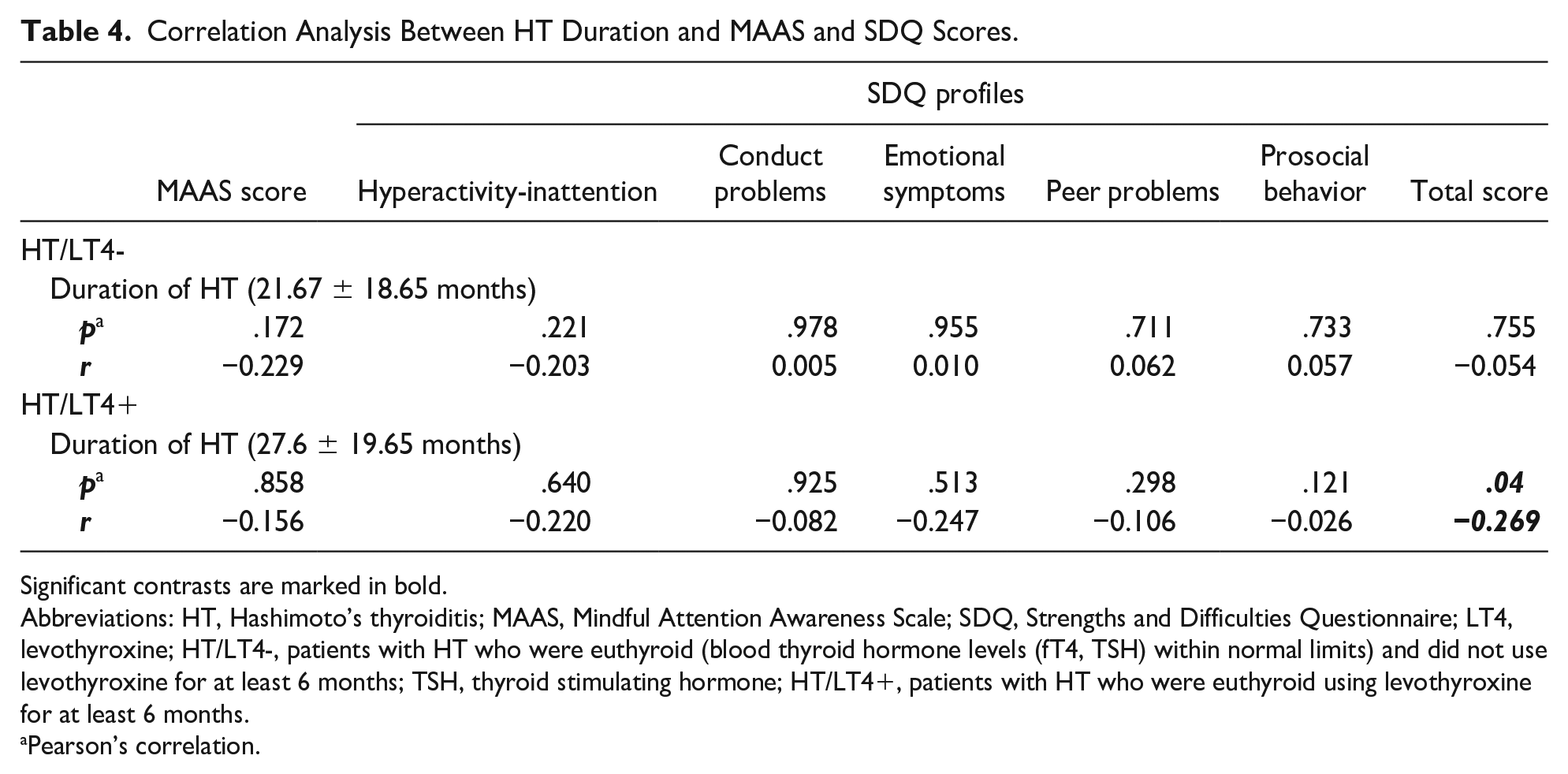
Significant contrasts are marked in bold.
Abbreviations: HT, Hashimoto’s thyroiditis; MAAS, Mindful Attention Awareness Scale; SDQ, Strengths and Difficulties Questionnaire; LT4, levothyroxine; HT/LT4-, patients with HT who were euthyroid (blood thyroid hormone levels (fT4, TSH) within normal limits) and did not use levothyroxine for at least 6 months; TSH, thyroid stimulating hormone; HT/LT4+, patients with HT who were euthyroid using levothyroxine for at least 6 months.
Pearson’s correlation.
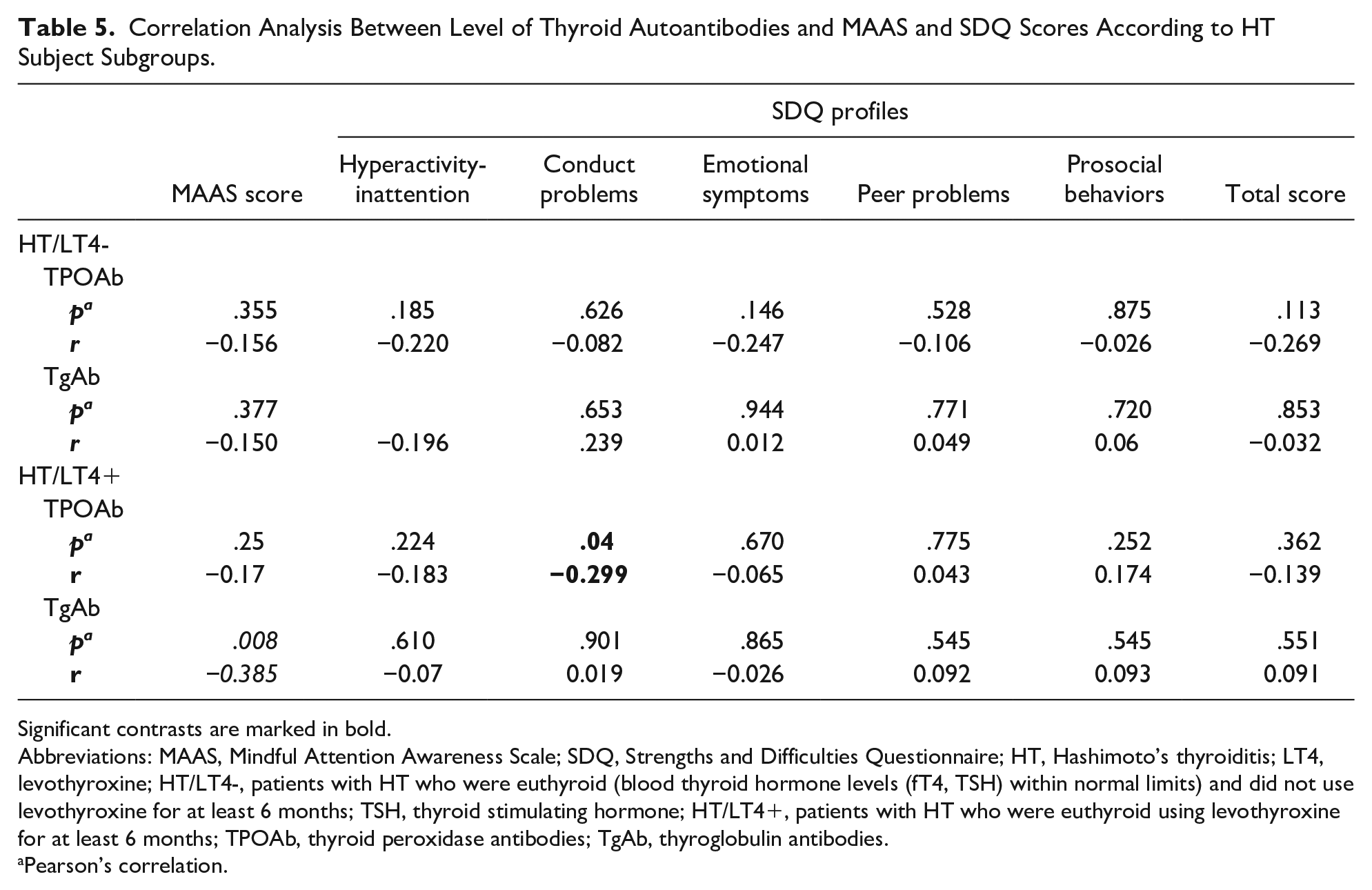
There were no patients in the study for whom both antibodies were negative. All patients were positive for 1 or 2 antibodies. In the HT subjects, the number of patients with only TPOAb positivity was 25 (29%), the number of patients with only TgAb positivity was 7 (8%), and the number of patients with both positive antibodies was 54 (63%). When the thyroid autoantibody distribution of the patients in the HT with LT4 therapy group was examined, 58% (n = 27) of the patients were positive for both antibodies and exclusively TPOAb positivity (36%, n = 17) was higher than TgAb positivity (6%, n = 3). No difference in SDQ or MAAS scores was observed between HT patients with or without LT4 treatment in the rate of antibody positivity (Table 5).
Correlation Analysis Between Level of Thyroid Autoantibodies and MAAS and SDQ Scores According to HT Subject Subgroups.
Significant contrasts are marked in bold.
Abbreviations: MAAS, Mindful Attention Awareness Scale; SDQ, Strengths and Difficulties Questionnaire; HT, Hashimoto’s thyroiditis; LT4, levothyroxine; HT/LT4-, patients with HT who were euthyroid (blood thyroid hormone levels (fT4, TSH) within normal limits) and did not use levothyroxine for at least 6 months; TSH, thyroid stimulating hormone; HT/LT4+, patients with HT who were euthyroid using levothyroxine for at least 6 months; TPOAb, thyroid peroxidase antibodies; TgAb, thyroglobulin antibodies.
Pearson’s correlation.
Discussion
Relationship Between HT and MAAS
There was no statistical difference between the MAAS scores of the groups in the study. However, it was noted that the mean MAAS score of the patient group was slightly higher than that of the healthy group. Having a chronic illness may raise awareness in some ways. Mindfulness awareness is the state of being aware of the events occurring in the current time period and teaches one how to deal with negative thoughts and emotions by embracing their presence rather than trying to avoid or judge them. In many studies, it has been found to reduce anxiety, stress, and depression in individuals with chronic physical and mental health conditions. 16 The level of mindfulness awareness has been found to be negatively affected by the presence of chronic disease. 17 In contrast, in our study, although there was no statistical difference, MAAS levels in the patient group were higher compared to the controls. However, this result may not give clear and robust information since mindfulness may be related to many different parameters, such as temperament, education level, and previous life experiences. Additionally, it is also elusive to explain that the mean score of awareness in the control group was lower than the mean score in the patient group. Therefore, we think that it would be beneficial to conduct mindfulness assessments periodically in the adolescent age group while they are healthy, even before a disease develops.
Relationship Between MAAS and Thyroid Autoantibodies
We found no relationship between TPO-Ab levels and mindfulness levels, but it was observed that the level of mindfulness decreased with increasing TgAb levels. This effect of TgAb on MAAS was found to be significant in the HT subjects for those using LT4. As a biomarker of thyroid dysfunction in autoimmune thyroid disease, TPOAb is more significant than TGAb, which is used in clinical practice. 18 Therefore, we did not expect any strong correlation between TgAb and scale scores in our study compared to TPOAb. On the other hand, dividing the HT subject group into 2 groups according to LT4 use, no statistically significant difference in mindfulness scores was found between the subgroups, but patients with exclusively TPOAb positivity who did not use LT4 had better mindfulness scores. We thought that the use of LT4 in the presence of TPOAb might decrease mindfulness with a possible interaction. Knowing the MAAS scores of HT patients before LT4 treatment may provide clearer information about causality, with a better inference. This observation may create new study ideas on the subject and mashed light on future studies. The interaction between LT4 replacement and thyroid autoantibodies has not yet been investigated. Since LT4 treatment is essential, especially for hypothyroid HT, it cannot be thought that there is a major negative interaction between them. However, according to our study data, an inverse relationship at the sub/molecular level seems possible. Alternatively it may show that LT4 can improve the clinical symptoms of HT, but since the antibodies in the blood remain together with a complex immune environment in the brain, it does not help the negative effects of these antibodies on the brain.
Relationship Between HT and SDQ
SDQ total scores were found to be significantly higher in the healthy group. This difference seems to be associated with the statistically higher scores of the subscales of the emotional symptoms and the conduct problems. During adolescence, with the aim of searching for one’s own identity, the individual’s relationship with the family, peers, and the environment gains a different dimension than before adolescence. 19 While adolescence itself carries a risk in terms of problems in relationships, the sadness of having a chronic disease and being away from schools, friends and the struggle to cope with the disease can cause additional difficulties. 20 Moreover, social functioning may be impaired by the stigma associated with illness. However, in our study, SDQ scores were higher in the healthy group, contrary to our expectations. The possibility of higher pre-disease scores should also be considered. In this study, it was seen that emotional symptoms and conduct problem subscales had an effect on this difference. Many independent factors that are not directly related to the adolescent can also affect the scores. Analyzing the sociodemographic data in terms of possible reasons for this, the only difference observed between the groups was that the education levels of both parents were higher in the healthy group. We thought that this result might indicate that families are not able to spare enough time for their healthy children from their own work or business. However, the idea that the parents of patients may be more sensitive and constructive on the same issue may arise. In addition, the absence of patients with additional comorbidities in the study may have contributed to this. From another perspective, patients with chronic diseases go to the hospital more often than healthy people. Moreover, depending on the quality of the interviews with the patient and their families in the hospital, patient and family perspectives on the disease and perspectives on life may change and they may display more positive, more mature behaviors and attitudes with these experiences. The higher SDQ scores for control subjects may be due to the fact that they did not have similar experiences. And another possible reason is that this may also be a reflection of today’s challenging conditions. Therefore, by adding SDQ to standard screening programs for healthy adolescents, it may be possible to take a healthier step into adulthood with condition detection and early or appropriate interventions.
Relationship Between SDQ and Thyroid Autoantibodies
According to their antibody presence classification, HT patients without LT4 therapy showed no statistically significant difference in SDQ scores. On the other hand, HT patients with LT4 therapy had a negative correlation between TgAb levels and MAAS, while the SDQ conduct problems subscale had an inverse correlation with higher TPOAb levels. While some previous studies investigating the relationship between thyroid autoimmunity and psychiatric disorders support this relationship, others do not.21-23 Since there is no consensus on this issue, drawing a conclusion with our results seems complicated. More solid results can be obtained in future studies to be carried out with more participants. 23 In our study, while other subscales of SDQ were not associated with TPOAb titer level, hyperactivity, inattention, and conduct disorder, subscale scores were low.
Effects of LT4
There was no significant difference in the scores of both scales in the group that received LT4 treatment compared to the group that did not. However, we found that the total SDQ score decreased in the group receiving LT4 as the duration of HT increased. Many studies have been conducted to determine predictive factors for progression from euthyroidism or SCH to overt hypothyroidism or improvement over time, but no clear conclusions have been reached.24-26 Furthermore, the definition of SCH, as well as indications for LT4 therapy, differ between authors. 27 Although there was no significant difference, the SDQ total score was lower in the patient group using LT4 in the study. As expected, the patients in this group had a longer duration of HT compared to the patients who did not use LT4 and a lower SDQ total score was negatively related to this duration. Although there was no difference between LT4 users and non-users in terms of thyroid autoantibody titers in the study, we found that the SDQ total score decreased as the disease duration increased in patients using LT4. We thought that this result might be related to the long-term chronic effects of thyroid autoantibodies on the brain. Some studies reported that almost all patients required LT4 therapy during follow-up, while other studies found that 25%–50% of those with thyroid dysfunction at baseline had normalized thyroid function over time.26,28-30 We found that MAAS scores were not correlated with LT4 use. However, it was noted that as TgAb levels increased, MAAS scores decreased. Thyroid peroxidase antibody usually becomes positive first in HT, and TgAb becomes evident in the later stages of the disease, when clinical characteristics develop, and the need for LT4 emerges. 31
Conclusion
We observed that high TPOAb titers, which are predicted to be associated with adverse outcomes, were positively correlated with SDQ scores in our study. We thought that this association did not indicate a protective role of TPOAb, but could be a result of disease duration and adaptation to the disease. The MAAS and SDQ scale results were correlated with HT antibody titers, not LT4 treatment. A higher TgAb titer in HT patients receiving LT4 therapy was inversely correlated with mindfulness awareness, while a higher TPOAb titer was negatively correlated with the SDQ conduction problems subscale.
Limitations
The results should be interpreted in the context of several limitations, including a relatively small sample size with some conditions stated from now on, which could contribute to the study but were not evaluated. First, self-report scales may be sensitive to socially desirable responses. Second, we used only the youth-self-report version of the scales. It would be more appropriate to also use the parent-report and teacher-report versions of the scales together. Although not statistically significant in socio-demographic characteristics between patients and controls (Table 2), the lack of an exact match may be another study limitation that may have somewhat affected the results.
Although the presence of thyroid autoantibodies was used as a biomarker in the diagnosis of HT, up to 10% to 15% of patients with HT may have none of these antibodies. 32 On the other hand, TPOAb and TgAb positivity can be detected in disease-free populations. 33 Since autoantibodies were not tested in the healthy control subjects, our study was limited in this regard.
It was surprising that SDQ scores were higher in the healthy group in this study. One of the limitations of the study was that the SDQ scores of the patients were not known before the disease. The possibility of higher pre-disease scores should also be considered.
Author Contributions
MEU: Contributed to conception and design; contributed to analysis; drafted the manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy. NK: Contributed to conception and design; contributed to analysis; critically revised the manuscript; drafted the manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy. OK: Contributed to conception and design; contributed to analysis; critically revised the manuscript; drafted the manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy. TK: Contributed to conception and design; contributed to analysis; drafted the manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.