
Abstract
Abusive head trauma (AHT) is a significant cause of morbidity and mortality for infants. Determining when to pursue a complete physical abuse evaluation can be difficult, especially for nonspecific findings or when a child appears clinically well. This retrospective study of 7 cases sought to describe the presentation, evaluation, and diagnoses for infants with abnormal subdural collections identified on cranial ultrasound for macrocephaly, and to determine how frequently AHT is diagnosed. The results of this study showed that while each patient presented due to asymptomatic macrocephaly, the extent of the workup varied greatly. In addition, no infants had suspicious injuries for abuse during the initial evaluation or the year following. In summary, among the 7 patients seen for asymptomatic macrocephaly with possible subdural hemorrhage, there were very inconsistent child abuse workups. There needs to be a standardized clinical guideline for this specific patient population involving a child abuse pediatric evaluation.
Background
Abusive head trauma (AHT) is a significant cause of pediatric morbidity and mortality, affecting approximately 30 out of every 100,000 infants.1,2 The initial presentation of AHT varies widely from infants who are asymptomatic to infants presenting with severe life-threatening symptoms. The more severe the symptoms, the more likely concerns for AHT are to be identified. However, when signs and symptoms are nonspecific, AHT is more likely to be missed, leaving children at risk of recurrent abuse or even death. 3 The American Academy of Pediatrics (AAP) recommends that when physical abuse of an infant is suspected, the child has a complete evaluation, which may include a physical examination, abdominal labs, skeletal survey, and head imaging. 4 When infants present with nonspecific findings, especially in the setting of a relatively well-appearing infant, deciding when to pursue a child abuse work-up can be challenging and inconsistent. Furthermore, without clear guidelines, child maltreatment concerns and evaluations are under the discretion of individual providers, potentially resulting in implicit and explicit biases influencing medical decisions. 5
Macrocephaly is a relatively common finding in infants and toddlers with a very broad differential; on that differential is AHT. 6 For most cases of macrocephaly in a well-appearing infant, the initial step is a cranial ultrasound, screening for any possible intracranial pathology. 7 When that head ultrasound reveals a possible subdural hemorrhage (SDH), AHT becomes more significantly considered as part of the differential.8,9 These cases may be referred to the child abuse pediatrician for a work-up looking for abusive injuries, any previous accidental traumas, or underlying medical causes. This work-up likely involves sending the family to the hospital, a possible admission, blood draws, consultations and imaging, all resulting in cost, time, and increased stress for the family. Failure to do a work-up, however, may result in the child returning to an unsafe environment.
When an infant appears clinically well, medical providers may be hesitant to send them immediately to a higher level of care for a more comprehensive evaluation. One study by Hansen et al looked at children less than 2 years of age with a SDH who were evaluated for child physical abuse. They found that while children with severe symptoms had an almost 90% chance of having another suspicious injury on evaluation, those with mild or no symptoms still had a 60% chance of having another injury. 10 This finding suggests that the absence of severe symptoms should not negate the need for a thorough evaluation. There is no research to date that describes infants with asymptomatic macrocephaly who had a cranial ultrasound which identified subdural fluid collections, and the subsequent evaluation for AHT.
The purpose of this study is to describe the presentation, evaluation and ultimate diagnosis for infants who had a cranial ultrasound completed for macrocephaly when the ultrasound identified concern for SDH. The primary objective is to describe the extent of child abuse evaluations completed for these infants and determine how frequently AHT is diagnosed. The secondary objective is to identify if these infants had any subsequent evaluations for concerns of child abuse during the year following their initial hospitalization.
Methods
All procedures and methods used in this retrospective study were conducted in accordance with ethical principles for research involving human subjects. The study protocol was approved by the Hospital Institutional Review Board (IRB) and followed all applicable guidelines and regulations to ensure the protection of participants’ privacy and well-being. Informed consent was waived by the IRB as the retrospective study involved the analysis of pre-existing de-identified data. Confidentiality was maintained throughout the study, and all data collected were entered and stored on a web-based data storage and analysis tool that is compliant with the Health Insurance Portability and Accountability Act (HIPAA) regulations. Any individual identifiable information was removed to protect their anonymity.
Subject Recruitment
The study was completed at the state’s only Level I Pediatric Trauma Hospital, which is a large referral site for the entire state.
Patients were identified by a board-certified Pediatric Radiologist (J.C.) and a board-certified Child Abuse Pediatrician (C.B.) using the Imaging Radiology Information System with subsequent review of the medical records. Infants less than 12 months of age who underwent a cranial ultrasound due to macrocephaly between January 1, 2013, and December 31, 2019 were identified from the data set. They were included in the study if the ultrasound revealed an abnormal subdural collection. The medical record was then reviewed, and infants were excluded if they had severe neurological symptoms (ie. seizures and altered mental status), or if the cranial ultrasound was completed for a reason other than macrocephaly.
Record Review
After inclusion in the study, 3 reviewers (G.J., B.S., and C.B.) independently completed a detailed review of the medical records, and information was collected including demographic information, family and personal medical history, presenting neurological symptoms, examination findings, medical or surgical interventions, consultation notes, and any final diagnoses including level of concern for child abuse.
The medical record was then reviewed for the year following their initial cranial ultrasound to determine if future diagnoses or concerns for child abuse were identified.
Results
Review of the Radiology data set identified 1011 cases of infants who had a cranial ultrasound with the primary indication of macrocephaly. One hundred and sixty-three (163) of these cranial ultrasounds were identified as abnormal, of which 139 were excluded due to medical indications (ex. extracorporeal membrane oxygenation (ECMO), germinal matrix bleed, choroid plexus cyst, hydrocephalus, and Chiari II malformation) in addition to macrocephaly. Of the remaining 24 abnormal cranial ultrasounds for macrocephaly, 7 were identified as having possible subdural collections.
Demographic information and case descriptions can be found in Table 1. Most children were male (5/7), had public insurance (4/7), were non-Hispanic White (4/7), and were asymptomatic (7/7), though one infant had a history of recent fussiness which was attributed to a recently diagnosed ear infection. All of the children had cranial ultrasounds for macrocephaly, which identified concerns of SDH. The child abuse pediatric team was contacted for 6 of the 7 infants and completed a consult on 5 of them. The child abuse pediatric consultation was canceled for one child (case 4) after additional imaging (head computed tomotography (CT)) was completed, which identified enlarged subarachnoid space with no evidence of SDH.
Case Descriptions.
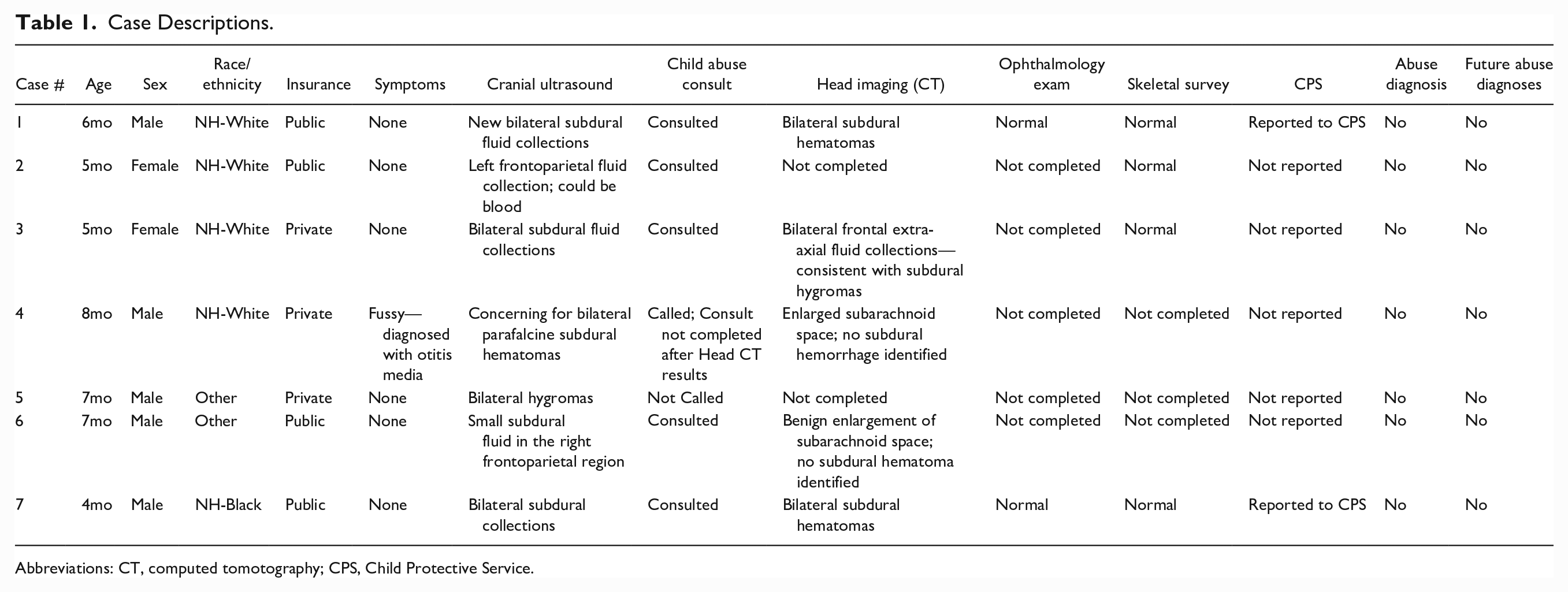
Abbreviations: CT, computed tomotography; CPS, Child Protective Service.
Of the 5 children for whom a child abuse pediatric consultation was completed, 4 of the 5 had a head CT, 4 of the 5 had a skeletal survey, 2 of the 5 had a dilated eye exam, and all 5 had bleeding labs obtained. None of the children were diagnosed with a bleeding diathesis and none of the children were diagnosed with child abuse. Child Protective Services was contacted for 2 of the 7 children, 1 (case 7) whose initial skeletal survey identified concerns for possible rib fractures (which were excluded on follow-up skeletal survey) and 1 (case 1) with newly identified bilateral subdural collections on serial ultrasounds for increasing head circumference. None of the children re-presented with concerns of abuse within a year of their initial evaluation.
Discussion
The presenting symptoms for AHT vary widely, which results in identifying affected children extremely challenging. As noted by Jenny et al, 3 when infants have significant symptoms such as respiratory failure or seizures, providers are more likely to identify concerns for AHT; however, with less-obvious symptoms of AHT, it may be missed. Hansen et al 10 found that in cases of suspected child physical abuse with SDH found on cranial imaging, symptom severity was associated with a higher likelihood of identifying concurrent suspicious injury. Interestingly, Hansen et al 10 also identified that less-severe symptoms were still associated with concurrent suspicious injury, suggesting that minimally symptomatic or asymptomatic patients should still have an evaluation for other injuries. In a paper on macrocephaly and subdural collection, Caré explains that the role of screening infants with subdural collections or SDH, especially in the presence of enlarged subarachnoid spaces, for additional concerning injuries remains undefined. 8 This study is the first to look at infants with subdural collections identified on cranial ultrasound for macrocephaly and describes their subsequent evaluation for AHT.
The AAP recommends a skeletal survey and a thorough physical examination when physical abuse is suspected in a child less than 2 years of age. In cases of suspected AHT, this evaluation also includes head imaging and a dilated eye exam with Ophthalmology. 4 When an outpatient provider orders a cranial ultrasound for macrocephaly and a subdural collection is identified in an otherwise well-appearing infant, the decision to pursue a further evaluation for child physical abuse relies upon the ordering provider or radiologist identifying the SDH as concerning for possible physical abuse and then prompting further evaluation. In our review of the last 7 years of cranial ultrasounds at a large tertiary pediatric hospital, only 7 cases had a SDH identified on cranial ultrasound completed for macrocephaly, which implies this may be an unusual occurrence.
This review highlights 7 cases of infants with a similar initial presentation of possible SDH identified on cranial ultrasound completed for macrocephaly, yet with varying extent of a child abuse pediatrics involvement and workup. Of the 7 cases, 1 patient (case 5) had an ultrasound which identified probable long-term “subdural hygromas” and no further evaluation or consultation with child abuse pediatrics was initiated. Subdural hygromas could be the result of previous subdural hematomas, thus this child should have been referred to the Child Abuse team and had additional head imaging. 11
For the remaining 6 cases, child abuse pediatrics was contacted. The child abuse team planned to complete a consultation on all 6 patients. One patient (case 4) was found not have an SDH on further head imaging, so the child abuse team consultation was canceled. Another patient (case 6) had an initial child abuse consultation completed; however, additional studies including an eye examination and skeletal survey were not completed after the head CT did not identify SDH. The other 4 had child abuse evaluations including a skin examination, blood testing, and skeletal survey, which did not identify any additional concerning injuries. Child Protective Services (CPS) was contacted for 2 of the 7 cases in this study. One patient (case 7) had CPS contacted due to an elicited prior history of emesis and difficulty breathing as well as concerns of rib fractures identified on the initial skeletal survey, which was then ruled out after the follow-up skeletal survey demonstrated no fractures. The other (case 1) was reported due to serial ultrasounds for increased head circumference that showed an acute change with newly identified bilateral subdural collections. None of the 7 cases re-presented for physical abuse concerns or were diagnosed with a bleeding diathesis or genetic condition during the year following their initial presentation.
As detailed above, the subsequent evaluations completed for the 7 cases were not uniform despite all having cranial ultrasounds for asymptomatic macrocephaly revealing possible SDH. The inconsistent evaluations may reflect subtle variations in their presentation or imaging, differences between providers, or other factors which may be affected by bias and social factors. The variation in workup is also likely affected by the absence of clear guidelines for this relatively uncommon situation.
To our knowledge, there is no standardized algorithm or workup for cases of asymptomatic macrocephaly with abnormal subdural collection found on cranial ultrasound. Therefore, we propose the following work-up: for infants with asymptomatic macrocephaly who had an abnormal subdural collection found on cranial ultrasound, the first initial step is to complete additional head imaging, either Head CT or Brain magnetic resonance imaging (MRI), to confirm possible SDH. 4 If the confirmatory imaging show possible SDH, the case should be evaluated as a case of possible AHT, thus a standard child abuse work-up should be completed. This work-up should include a child abuse consult, ophthalmology consult, a skeletal survey with 2-week follow-up, abdominal labs screening for occult abdominal trauma and bleeding labs screening for a bleeding diathesis, and a complete skin exam. 4 Work-up completed for other possible causes, such as genetic or metabolic causes, should be considered based on medical and family history.
A limitation of this study is that it is a retrospective chart review performed at a single institution with a small sample size. Future research that includes subjects from multiple sites with a large patient population is warranted to determine the predictability of an AHT diagnosis in patients with asymptomatic macrocephaly, and further, the necessity of a child abuse evaluation in the initial medical workup for this specific patient population.
Conclusion
There are no clear guidelines on how to evaluate asymptomatic infants who are found to have subdural fluid collections or SDH on cranial ultrasound for macrocephaly, leaving room for individual provider discretion, which increases the risk for inequity and bias. This study demonstrates that within one institution, infants received variable evaluations for similar presentations, which supports the importance of creating and implementing clear recommendations. This study also demonstrated that while most infants did not have a complete child physical abuse evaluation, none had concurrent suspicious injuries, and none were diagnosed with child physical abuse. It is also important to note that none of the patients returned in the subsequent year for any injuries concerning child abuse. While the absence of concurrent suspicious injuries does not exclude the possibility of AHT, it supports the possibility for alternative causes of some of these SDH.
Author Contributions
GJ: Contributed to conception and design; Contributed to acquisition, analysis, and interpretation; Drafted the manuscript; Critically revised the manuscript. BS: Contributed to conception and design; Contributed to acquisition, analysis, and interpretation; Drafted the manuscript; Critically revised the manuscript. JAC: Contributed to acquisition; Critically revised the manuscript. CS: Contributed to acquisition; Critically revised the manuscript. JM: Contributed to conception and design; Critically revised the manuscript. CB: Contributed to conception and design; Contribution to acquisition, analysis, and interpretation; Drafted the manuscript; Critically revised the manuscript.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.