
Abstract
Compared with the Finnegan Neonatal Abstinence Scoring System (FNASS), the Eat, Sleep, Console (ESC) approach reduces pharmacotherapy and length of stay (LOS) for neonatal opioid withdrawal syndrome (NOWS) infants. The independent outcome contribution of ESC is unknown as the approach combines ESC assessment with additional management changes. Our objective was to evaluate ESC assessment’s independent impact on outcomes compared with FNASS. We conducted a retrospective cohort study of in utero opioid-exposed infants ≥35 weeks gestation managed with FNASS versus ESC. Outcomes included pharmacotherapy initiation, LOS, length of pharmacotherapy, and emergency department visit/readmissions. Among 151 FNASS and 100 ESC managed infants, pharmacotherapy initiation (P = .47), LOS for all infants (P = .49), and LOS for pharmacologically treated infants (P = .68) were similar. Length of pharmacotherapy did not differ (P = .84). Emergency department evaluation/NOWS readmission was equally rare (P = .65). Using equivalent models of care, comparison of ESC and FNASS assessment tools showed no difference in NOWS outcomes.
Introduction
The national opioid crisis has led to increased opioid use during pregnancy. Maternal opioid use disorder more than quadrupled from 1.5 to 6.5 per 1000 delivery hospitalizations between 1999 and 2014. 1 A parallel increase in neonatal opioid withdrawal syndrome (NOWS) followed from the rise in fetal opioid exposure.2,3 Infants with NOWS often have prolonged hospital stays resulting in high hospital utilization and costs exceeding a half-billion dollars per year.4-6 The Finnegan Neonatal Abstinence Scoring System (FNASS), the most frequently used NOWS assessment tool, influences this length of hospitalization as it guides the duration of both inpatient observation and pharmacotherapy.7,8 The FNASS score is limited by its subjective assessment of 21 clinical signs which can lead to poor inter-rater reliability. While the FNASS score describes NOWS symptomatology, it does not reflect whether symptoms interfere with normal function. This treatment of symptoms rather than functional impairment may drive opioid-exposed infants’ disproportionate hospital utilization.
Recent studies suggest FNASS leads to unnecessary opioid replacement therapy for withdrawal compared with the Eat, Sleep, Console (ESC) approach.9,10 The ESC approach combines a 3-item function-based assessment reflecting whether NOWS severity affects an infant’s ability to eat, sleep, and console with nonpharmacologic care optimization and parental education, support, and empowerment. In comparison with FNASS, the ESC approach reduced pharmacotherapy initiation by 50% and shortened length of stay (LOS) without increasing readmissions. Subsequent studies of ESC approach implementation in pediatric and neonatal intensive care units (NICU), including a recent cluster-randomized controlled trial, showed significant decreases in pharmacotherapy initiation and LOS as well.11-19
In all prior publications, ESC assessment was always one component of a larger NOWS model of care change including increasing nonpharmacologic care, converting to as-needed morphine, or changing admission to inpatient pediatrics.9,11-20 It is unclear whether the ESC approach was successful because of the ESC assessment tool itself, additional care components, or a combination.
Our objective was to evaluate whether a change to the ESC assessment tool alone could safely reduce initiation of pharmacotherapy and decrease LOS compared with FNASS.
Methods
Study Design
We used a retrospective cohort design to compare outcomes of in utero opioid-exposed infants from the same centers managed using ESC (February 2020 to August 2021) versus FNASS assessment (April 2018 to December 2019).
Study Setting
This study was conducted in the 2 level III NICUs and 4 level II NICUs with the highest NOWS incidence within our regional health care system. All 6 NICUs have an open-bay design preventing rooming-in at the bedside.
Except for the assessment tool, the NOWS management guideline across all 6 sites was unchanged over the study period. This regional guideline included prenatal consults, nonpharmacologic care optimization, a standardized methadone initiation, escalation and weaning protocol, 21 clonidine adjunctive therapy, breakthrough morphine, and standardized discharge criteria (Figure 1).
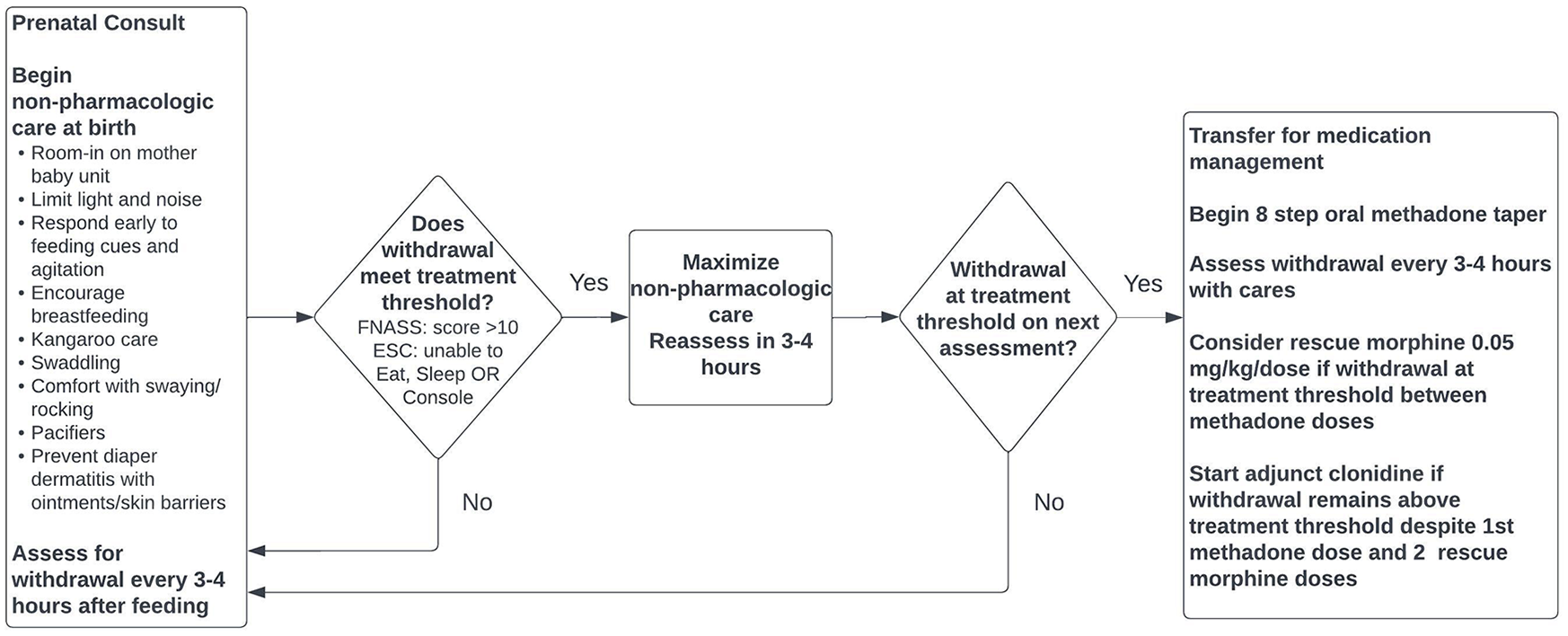
Regional neonatal opioid withdrawal syndrome management guideline for FNASS and ESC cohort.
Study Population
From April 2018 to December 2019, infants at risk for NOWS from opioid exposure during the month preceding delivery were evaluated by FNASS. To achieve score reliability, nurses completed the Finnegan Interrater Reliability Program. Infants were admitted to the mother baby unit where parents, family caregivers, and nurses optimized nonpharmacologic care by rooming-in, minimizing environmental stimuli, responding early to infant hunger and irritability cues, and using comforting techniques. Mothers receiving opioids through a treatment program were encouraged to breastfeed. The FNASS assessment was done every 3 to 4 hours following feeding. Opioid replacement therapy criteria included 2 FNASS scores >10 or a single score >14 despite nonpharmacologic care optimization. In 5 study sites, infants needing pharmacotherapy transferred to the NICU. In one site, infants needing pharmacotherapy transferred to a private pediatric unit room.
From February 2020 to August 2021, infants at risk for NOWS were evaluated by ESC assessment. Staff at all centers completed the same ESC training module. Following birth, these infants roomed-in on the mother baby unit with parents and nurses optimizing nonpharmacologic care. The ESC assessment was done every 3 to 4 hours following feeding. After ESC, an FNASS assessment was also completed but not used to guide management. If an infant could not eat, sleep, or console on 2 occasions despite nonpharmacologic care optimization, they transferred for methadone management to the same NICU/Pediatric unit as in the FNASS period.
All infants born at ≥35 weeks gestation at the 6 study centers from April 2018 to August 2021 were screened for eligibility. We included infants at risk for NOWS who had FNASS or ESC assessments for withdrawal. We defined “at risk for NOWS” as those infants with in utero opioid exposure as verified by pharmacy records, urine drug screen (UDS) results, and/or chart review. Our network pharmacies provide members with nearly all their prescriptions. 22 Maternal opioid prescriptions dispensed from pregnancy onset until infant delivery were extracted from pharmacy records. As many opioid use disorder medication programs occur outside our health care system, methadone or buprenorphine treatment was confirmed by chart review. All maternal and infant UDS results were obtained from our regional health system databases. We perform universal UDS during the first trimester with additional maternal UDS performed if the initial screen is positive or if there is suspected substance abuse. Our regional guidelines recommend infant testing if maternal testing is unavailable or if the infant displays drug exposure or withdrawal symptoms. Infant testing reduced nonresponse bias resulting from mothers who refused UDS or had no prenatal care. We performed chart review for hospital administered opioids to avoid misclassification of positive maternal or infant UDS from opioids received during labor. Ninety-two percent of women in our study had at least one UDS. The FNASS or ESC evaluation was identified from inpatient nursing flowsheets. We excluded infants <35 weeks gestation as they are all admitted to the NICU after birth in our centers and withdrawal presentation is more variable at younger gestations. Infants transferred from/to a nonstudy site were also excluded.
We ascertained factors affecting NOWS incidence and severity.23-25 From outpatient pharmacy records and/or maternal and infant UDS, we determined the type of maternal opioid and additional maternal exposures, including alcohol, selective serotonin reuptake inhibitors, benzodiazepines, marijuana, cocaine, and methamphetamines/amphetamines. We conducted chart review to verify nicotine exposure and to confirm the additional substance exposures above. As breastfeeding reduces NOWS incidence and length of treatment (LOT), any breastfeeding during the birth hospitalization was identified from feeding documentation in the electronic medical record.26-28 We used the neighborhood deprivation index (NDI) as a measure of socioeconomic status. The NDI measures aspects of poverty proven to be markers for health outcomes. Higher NDI indicates higher deprivation/lower neighborhood socioeconomic status. 29 Additional factors that could affect LOS such as delivery mode, gestational age (GA), small for gestational age (SGA<10%), sex, and facility were obtained from our regional health system databases.
Study Outcomes
The primary outcomes assessed were pharmacotherapy initiation and LOS among in utero opioid-exposed infants. Initiation of pharmacotherapy included any infant administered methadone for NOWS. The total LOS of the birth hospitalization in all locations (mother baby unit, NICU, and Pediatrics) was determined. For mothers with nonprescribed opioid or polysubstance abuse, a full psychosocial evaluation is performed to establish if a Child Protective Services referral is required. Child Protective Services determination of custody/disposition can prolong hospital stay beyond the medically necessary observation or treatment period. The LOS was calculated from when the infant was medically ready for discharge as determined by chart review.
We included LOT as a secondary outcome. The LOT was calculated as the total days that the infant received methadone, adjunct clonidine, breakthrough morphine, or phenobarbital treatment. Due to concern that using a function-based assessment could lead to premature discharge, we examined the balancing measure of emergency department (ED) visits/readmissions. We identified all ED visits/readmissions within 30 days of hospital discharge and performed chart review to determine whether NOWS was the encounter indication.
Data Analysis
Sample size was determined by including all infants meeting study eligibility during the study period.
Baseline characteristics of infants managed using ESC or FNASS assessment were compared using t tests for continuous variables and chi-square tests for categorical variables. We compared pharmacotherapy initiation by chi-square test. For skewed LOS and LOT data, we performed the Wilcoxon rank sum test. We evaluated ED visits/readmissions by Fisher exact test.
Comparing ESC with FNASS assessment, we used logistic regression to estimate the adjusted odds ratio of pharmacotherapy initiation and ED visits/readmissions and log-gamma regression for LOS and LOT. 30 Given the skewed LOS distribution, we used a generalized linear model that assumes a skewed gamma outcome distribution with a log link function that has been applied to hospital LOS analysis. 30 This model is appealing as the estimated effect from this log-gamma model is easily interpretable as the ratio of mean outcomes (ROM); for example, we interpret the estimated effect for ESC of 1.15 as a 15% longer mean LOS among infants managed using ESC versus FNASS. Models were adjusted for GA, SGA, payor type, cesarean delivery, facility, maternal opioid type, and maternal selective serotonin reuptake inhibitor, nicotine, alcohol or benzodiazepine use. We conducted analyses using SAS version 9.4.
Ethical Considerations
Our regional institutional review board approved this study. This study was performed in accordance with the Declaration of Helsinki.
Results
From April 2018 to August 2021, 50 324 infants were born at ≥35 weeks at the study hospitals (Figure 2). We excluded one infant due to non-NOWS-related medical acuity requiring a morphine infusion and another infant due to mixed use of FNASS and ESC assessments. Among those evaluated for withdrawal, we identified in utero opioid exposure in 251 infants (5 per 1000); 151 were evaluated by FNASS and 100 by ESC assessment.
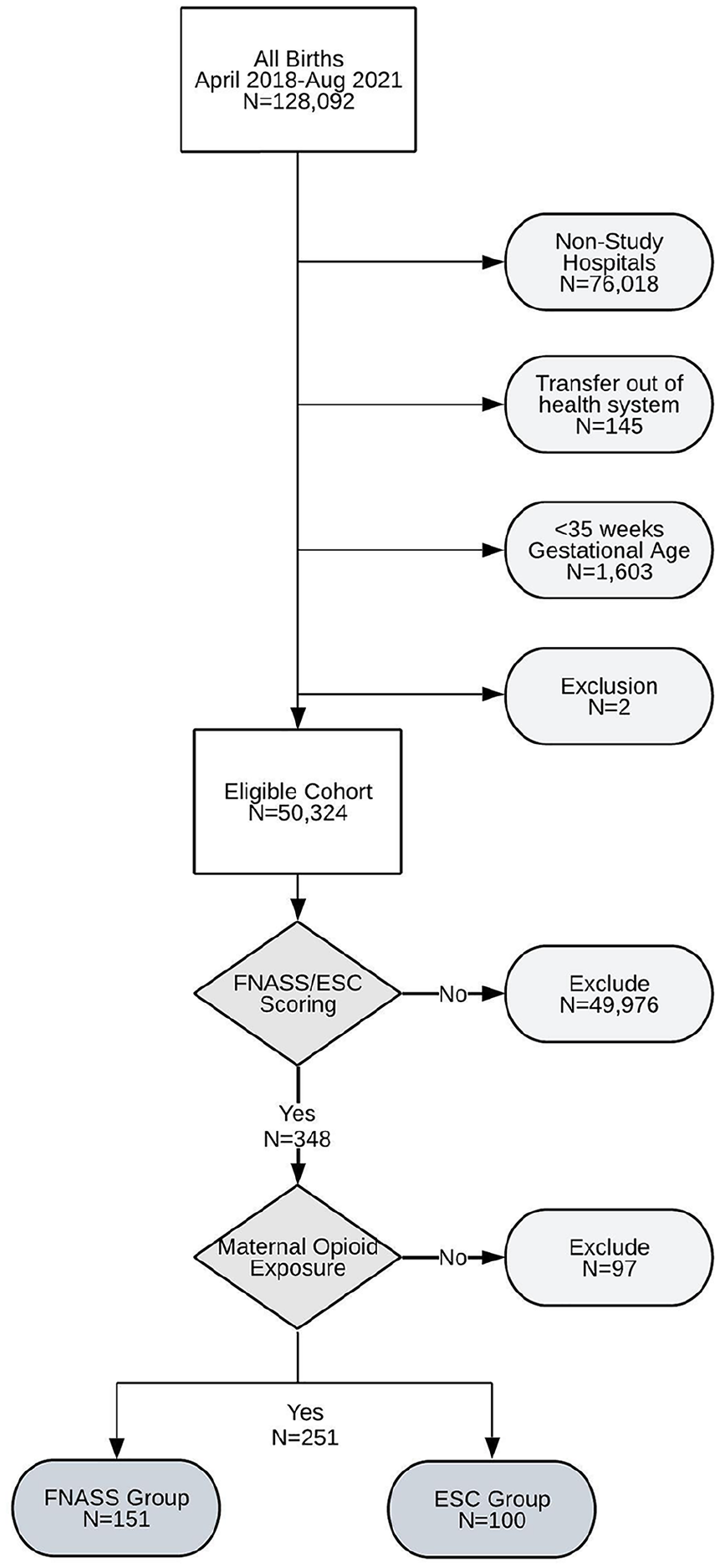
Flowchart for FNASS and ESC cohort selection.
The FNASS and ESC groups were similar in terms of sex, GA, birthweight, infant race/ethnicity, and delivery mode (Table 1). The FNASS infants were more likely to be SGA (11.9% vs 4%, P = .03). The type of in utero opioid exposure was comparable between groups apart from higher fentanyl use during the ESC period (7% vs 0%, P = .001). Individual substance co-exposure to tetrahydrocannabinol, cocaine, methamphetamines, benzodiazepines, alcohol, or nicotine was the same among FNASS and ESC infants. Maternal selective serotonin reuptake inhibitor use was more common in the ESC group (28% vs 14.6%, P = .01). The overall substance co-exposure rate was greater in the ESC period (75% vs 62%, P = .03). The 2 groups had equally high breastfeeding rates. They were also similar regarding socioeconomic indicators such as insurance payor and NDI. Child Protective Services assigned custody to other family members or foster care in 11.9% and 14% of FNASS and ESC infants, respectively (P = .63).
Characteristics of FNASS and ESC Cohorts.
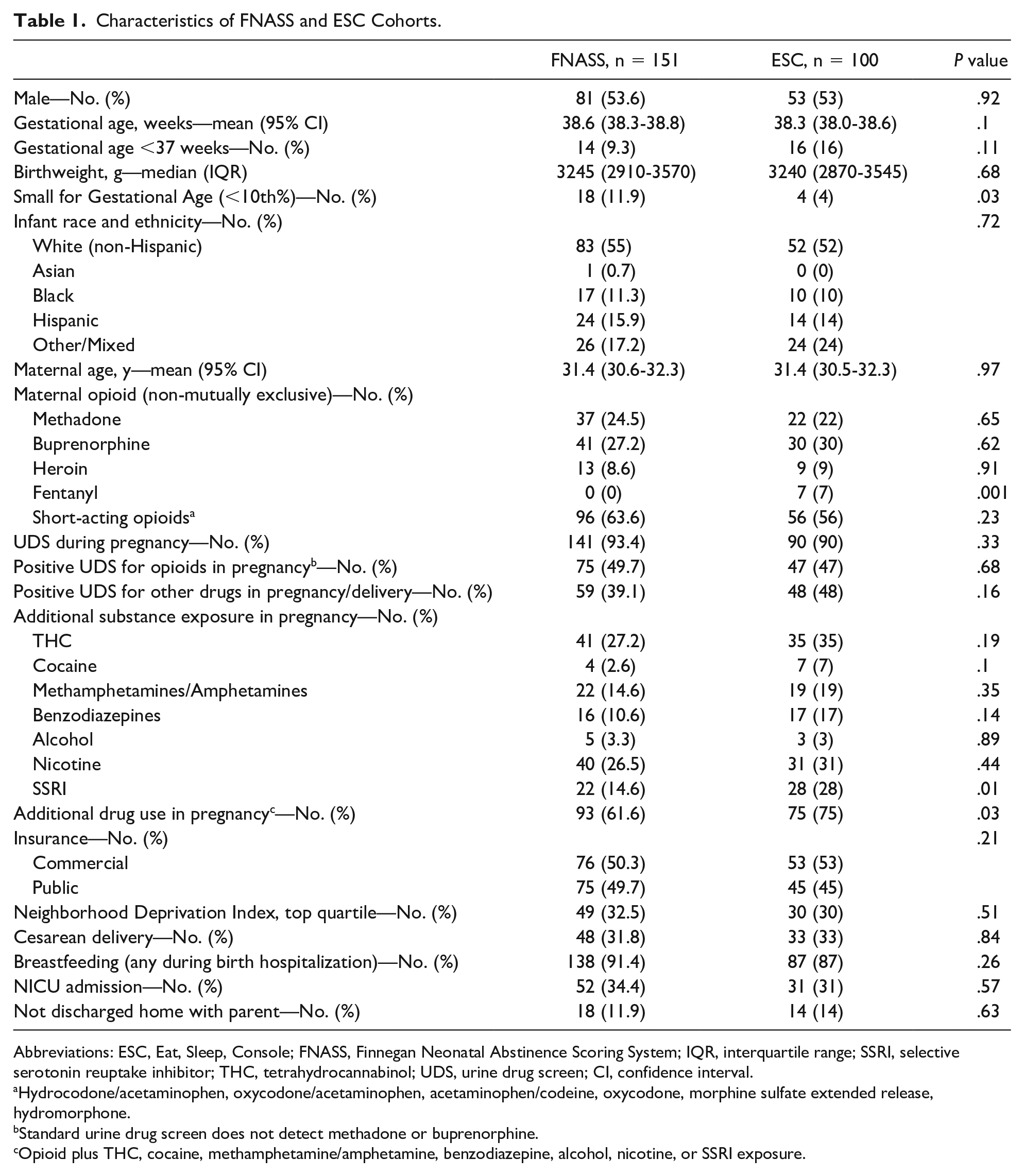
Abbreviations: ESC, Eat, Sleep, Console; FNASS, Finnegan Neonatal Abstinence Scoring System; IQR, interquartile range; SSRI, selective serotonin reuptake inhibitor; THC, tetrahydrocannabinol; UDS, urine drug screen; CI, confidence interval.
Hydrocodone/acetaminophen, oxycodone/acetaminophen, acetaminophen/codeine, oxycodone, morphine sulfate extended release, hydromorphone.
Standard urine drug screen does not detect methadone or buprenorphine.
Opioid plus THC, cocaine, methamphetamine/amphetamine, benzodiazepine, alcohol, nicotine, or SSRI exposure.
There was no difference in pharmacotherapy initiation between the FNASS and ESC groups (14.6% vs 18%, P = .47) (Table 2). For the methadone- or buprenorphine-exposed subgroup, pharmacotherapy initiation was also the same (FNASS 17.6% vs ESC 22.5%, P = .5). For infants exposed to short-acting opioids, 10.7% of FNASS and 13% of ESC (P = .69) received pharmacotherapy. Median LOS for all in utero opioid-exposed infants was 3.4 (interquartile range [IQR] 3-5.3) and 3.7 (IQR 3-5.5) days (P = .49) for FNASS and ESC groups, respectively. Among infants receiving methadone treatment, median LOS was comparable between FNASS 14.4 days (IQR 12-20.2) and ESC 14.1 days (IQR 12.6-14.7) (P = .68). Median LOT was similar between FNASS 9 days (IQR 8-15) and ESC groups 9.5 days (IQR 9-10) (P = .84). The ED visits/hospital readmissions for NOWS indications demonstrated no significant difference: FNASS 1.3% and ESC 2% (P = .65).
Outcomes of FNASS and ESC Cohorts.
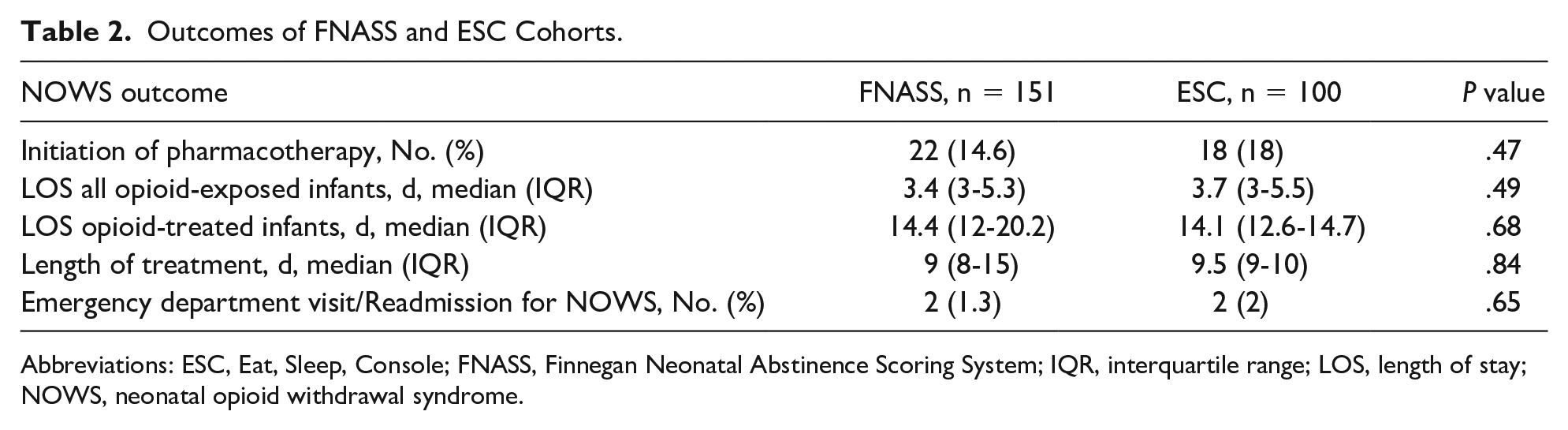
Abbreviations: ESC, Eat, Sleep, Console; FNASS, Finnegan Neonatal Abstinence Scoring System; IQR, interquartile range; LOS, length of stay; NOWS, neonatal opioid withdrawal syndrome.
Comparing infants managed with ESC versus FNASS assessment, the unadjusted odds of receiving pharmacotherapy were odds ratio (OR) = 1.29, 95% confidence interval (CI) = 0.65-2.55, P = .47 (Table 3). Following adjustment, the odds of receiving pharmacotherapy were no different between groups (adjusted odds ratio [aOR] = 0.85, 95% CI = 0.34-2.1, P = .72). Among all opioid-exposed infants, the mean LOS was the same for FNASS and ESC groups by log-gamma regression (ROM = 1.00, 95% CI = 0.83-1.20, P = .97). In multivariable models, the mean LOS was also similar between groups (aROM = 0.92, 95% CI = 0.78-1.08, P = .3). The unadjusted LOS (ROM = 0.86, 95% CI = 0.65-1.14, P = .28) and adjusted LOS (aROM = 0.87, 95% CI = 0.74-1.01, P = .07) with ESC trended toward shorter stays for infants receiving methadone. Both LOT (ROM = 0.84, 95% CI = 0.60-1.18, P = .31) and adjusted LOT (aROM = 0.91, 95% CI = 0.71-1.16, P = .42) were comparable among ESC and FNASS groups. The probability of ED visit/readmission for NOWS (aOR = 0.9, 95% CI = 0.35-2.34, P = .83) did not increase with ESC.
Regression Models for ESC Effect on NOWS Outcomes.
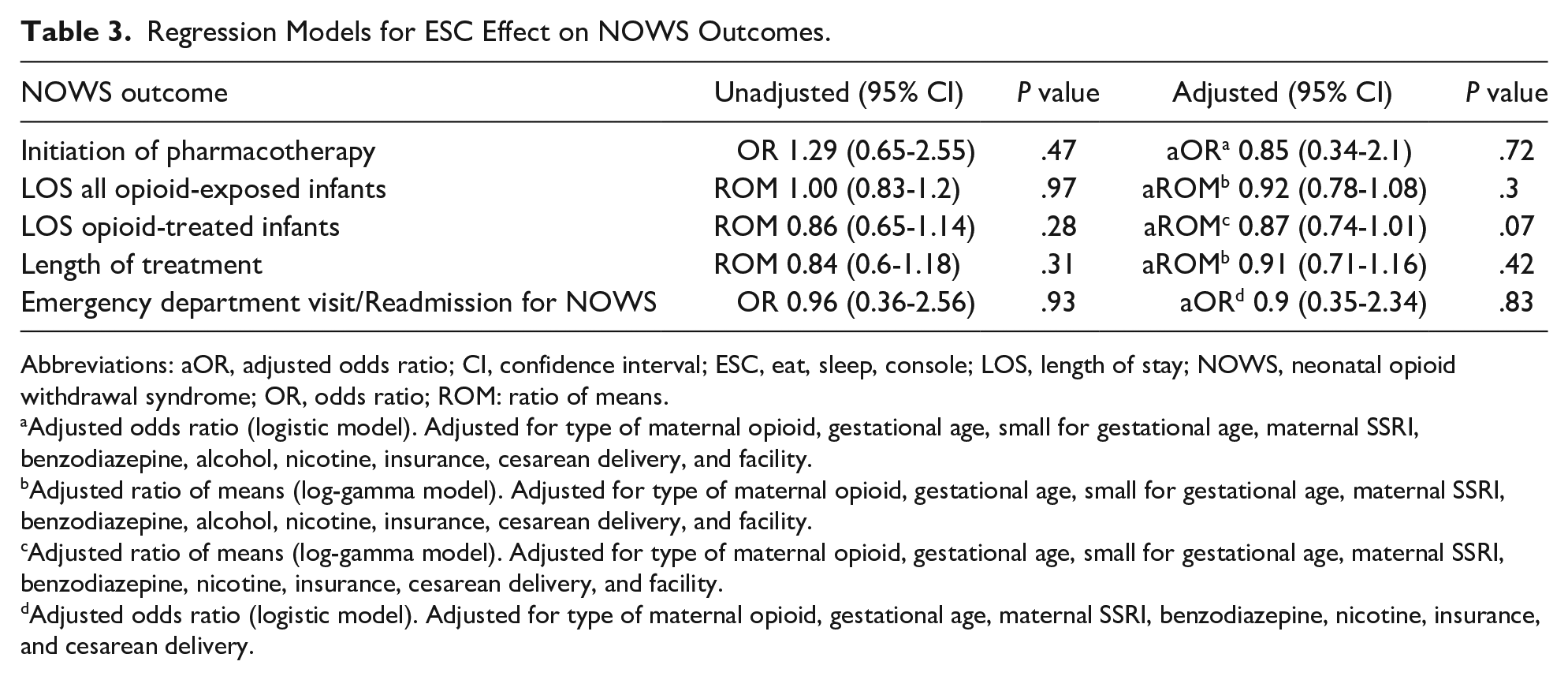
Abbreviations: aOR, adjusted odds ratio; CI, confidence interval; ESC, eat, sleep, console; LOS, length of stay; NOWS, neonatal opioid withdrawal syndrome; OR, odds ratio; ROM: ratio of means.
Adjusted odds ratio (logistic model). Adjusted for type of maternal opioid, gestational age, small for gestational age, maternal SSRI, benzodiazepine, alcohol, nicotine, insurance, cesarean delivery, and facility.
Adjusted ratio of means (log-gamma model). Adjusted for type of maternal opioid, gestational age, small for gestational age, maternal SSRI, benzodiazepine, alcohol, nicotine, insurance, cesarean delivery, and facility.
Adjusted ratio of means (log-gamma model). Adjusted for type of maternal opioid, gestational age, small for gestational age, maternal SSRI, benzodiazepine, nicotine, insurance, cesarean delivery, and facility.
Adjusted odds ratio (logistic model). Adjusted for type of maternal opioid, gestational age, maternal SSRI, benzodiazepine, nicotine, insurance, and cesarean delivery.
Discussion
For infants at risk for NOWS, our study showed similar initiation of pharmacotherapy, LOS, and LOT using FNASS versus ESC assessment. These results contrast with prior publications where ESC assessment as one component of a new ESC approach resulted in decreased pharmacotherapy initiation and LOS.9,11-19 A potential reason for the differing results is that ESC assessment in these studies was always accompanied by other substantial NOWS management changes. Pharmacotherapy initiation may have been impacted by nonpharmacologic care optimization9,11,14-17 or admission to the pediatric ward instead of NICU.9,13 A decrease in time to medical readiness for discharge, as seen in the recent randomized controlled trial, may have resulted from significant increases in nonpharmacologic interventions such as breastfeeding, potential location of care changes, or implementation of a strict ESC study protocol compared with usual care which may have lacked NOWS management standardization. 19 In addition, LOT in prior studies was likely affected by switching from a prolonged opioid taper to as-needed morphine9,12,14-17 or shifting from scheduled morphine to methadone. 11 This implementation of multiple practice changes makes it difficult to identify whether previously reported improvements resulted from ESC assessment itself or other care model changes.
Baseline opioid treatment rates for NOWS in these publications ranged from 31% to 98%. Our baseline treatment rate was substantially lower at 14.6%. During our study period, the only new intervention was the change in withdrawal assessment tool. Adherence to the same model of care with emphasis on nonpharmacologic interventions allowed us to evaluate the independent impact of ESC assessment. The approximately 15% requiring opioid treatment may represent infants with severe NOWS that cannot be managed with nonpharmacologic measures alone, regardless of the assessment tool used. This theory is supported by all prior ESC implementation studies where pharmacotherapy rates following introduction of the ESC approach did not go below a level of 14%.9,11-19 Our data highlight that ESC assessment may not be as vital to the ESC approach as standardized practice or nonpharmacologic care. In our population where both these elements were already maximized, we reached a low baseline treatment rate with FNASS and saw no additional improvement with ESC assessment. The heterogeneity of treatment effect reported in the recent New England Journal of Medicine study, 19 where some centers also saw no improvement in outcomes, suggests factors other than ESC assessment itself play an important role in predicting success of the ESC approach. In centers with higher medication treatment rates, the ESC approach may reduce pharmacotherapy primarily from standardization of NOWS management protocols, including better nonpharmacologic care adherence.
Our lower baseline pharmacotherapy rate may be partially attributable to our patient population. While previous publications report 87% to 100% public insurance,9,12,15-17,20 our study population primarily had commercial insurance (51%). Most of our mothers had prenatal care and were in a treatment program or receiving chronic pain medications. In addition, our Early Start Program provides one-on-one substance use disorder support during pregnancy which destigmatizes opioid usage, engages maternal involvement early in pregnancy, and sets delivery expectations. 31 The seamless integration between early start, prenatal care, and delivery helps us to maximize nonpharmacologic care.
Our FNASS protocol may have likewise impacted medication initiation. The conventional treatment threshold in many centers is 3 scores ≥8 or 2 scores ≥12 despite lack of research validating these treatment thresholds. 32 Our treatment threshold of 2 scores >10 may have led to less treatment than centers using a cutoff of 8 but more than centers using a cutoff of 12. The difference in treatment is likely small as the maximum FNASS score (median) was 7 and 6 in the untreated FNASS and ESC groups, respectively (P = .46), and 15 versus 16 in the treated FNASS and ESC groups (P = .97). In addition, nursing completion of the Finnegan interobserver reliability program may have reduced inconsistent high scores and contributed to our low baseline opioid treatment rate. The improvement in pharmacotherapy initiation seen in the recent randomized controlled trial may be partly attributable to a change from usual care with unknown Finnegan score reliability and higher baseline treatment rates (45%-61%) to the ESC approach with required inter-rater reliability training. 19
The similar LOS among infants managed with FNASS versus ESC assessment was likely multifactorial. The main driver of LOS is pharmacotherapy initiation. Since ESC did not decrease initiation of pharmacotherapy, we did not see a consequent decline in LOS attributable to infants who avoided opioid treatment. In addition, ESC implementation did not reduce LOT which would have resulted in a shorter LOS. Most pharmacologically treated infants received the minimum 8-day methadone taper in both the FNASS and ESC groups which left little opportunity for ESC to significantly reduce LOT. Previous studies changed from a standardized taper to as-needed morphine which may have shortened LOT and/or LOS in conjunction with ESC.9,12,14-17
Prior ESC publications were before and after quality improvement evaluations which usually did not adjust for differences in maternal and infant characteristics between the 2 time periods. One strength of our study is that we adjusted for differences in case mix as well as potential confounders in our analyses evaluating the effect of ESC assessment on NOWS outcomes. Our closed hospital and clinic system and integrated electronic medical records allowed for more complete ascertainment of maternal pregnancy data, including prescription history, type of opioid exposure, and substance co-exposures. Our integrated health care system combined with higher patient commercial insurance coverage also allowed for better determination of ED visits/readmissions.
Another study strength is that we examined NOWS outcomes following a single change from FNASS to ESC assessment. In previous studies, ESC assessment was always bundled with other major NOWS management changes making it difficult to discern which element of the quality improvement bundle was driving change.
Our study was limited in its ability to detect small differences in outcomes between FNASS and ESC groups. To see a significant difference in medication treatment, however, all of the next 133 ESC patients would need to completely avoid pharmacotherapy. Another study limitation is that ESC implementation occurred during the COVID era which prohibited postmaternal discharge boarding and restricted additional family/friend visitation. This visitor restriction prevented caregiver ability to optimize nonpharmacologic care which may have impacted NOWS outcomes. A final limitation was that we could not measure the nonpharmacologic interventions to assure equivalence between the 2 periods.
Conclusion
Our results suggest the impact of ESC or FNASS on NOWS outcomes lies in a standardized model of care and not in the assessment tool itself. The ESC assessment alone did not reduce pharmacotherapy or shorten LOS compared with FNASS. Eat, sleep, console also did not lead to increased ED visits/readmissions in the immediate newborn period. With ESC assessment, withdrawal symptoms themselves are not an indication for pharmacologic treatment unless they interfere with a baby’s function. It is unknown whether less aggressive treatment of withdrawal symptoms leads to short-term sequelae such as poor weight gain following hospital discharge. Long-term studies are also needed to determine neurodevelopmental outcomes of different NOWS management approaches. Since the assessment tool does not reduce LOS, studies are needed to further elucidate risk factors for in utero opioid-exposed infants who need opioid treatment to eliminate prolonged observation for lower risk infants.
Author Contributions
No AI was used in the drafting or revision of the manuscript.
LJC: conceptualized and designed the study, collected data, drafted the initial manuscript, and critically reviewed and revised the manuscript.
MWK: conceptualized and designed the study, supervised data collection and analysis, and critically reviewed and revised the manuscript.
CL: contributed to the study design, performed data analysis, and critically reviewed and revised the manuscript.
EMW and SL: designed the data collection instruments, collected and analyzed the data, and critically reviewed and revised the manuscript.
All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Footnotes
Acknowledgements
Thank you to Nancy Goler and Allen Fischer for their continual support of this project and review of the manuscript, to Adrienne McIntyre for her regional nursing coordination and support, to Christine Broome for helping develop the nursing education tools, and to Susan Hintz for her expert review of the manuscript. We would also like to acknowledge Boston Medical Center, Yale, and Children’s Hospital at Dartmouth-Hitchcock for permission to use the ESC Care Tool in the electronic medical record.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by The Permanente Medical Group Delivery Science Research Grant. The funder/sponsor did not participate in the work.