
Abstract

Introduction
Intussusception mostly occurs in children between 3 months and 3 years of age and presents with abdominal pain and irritable crying. 1 Appendicitis also causes abdominal pain in children, with peak incidence in teenage; 2% to 9% of patients with appendicitis are aged under 5 years. 2 Both intussusception and appendicitis are important emergent abdominal diseases in children. Due to their non-specific symptoms and the difficulty young children may have in describing their symptoms, timely diagnosis can be challenging, particularly in infants. When both diseases occur simultaneously, clinical practice and management become even more challenging. The concurrent occurrence of intussusception and appendicitis is extremely rare, and no cases had been previously reported in infants prior to this one. We describe a special case of a 10-month-old boy with simultaneous intussusception and ruptured appendicitis.
Case Description
The patient was a 10-month-old male infant with no history of systemic disease. At 6 months of age, the patient experienced intussusception and received treatment via hydrostatic reduction. Abdominal computed tomography (CT) scan and Meckel’s scan were performed after the initial episode of intussusception to exclude the possibility of a lesion of lead point, but no Meckel’s diverticulum or other abdominal lesions were found. At 10 months of age, the patient experienced intermittent irritable crying for 2 days before visiting the emergency department (ED). He tended to bend his body while crying, and his appetite and activity were significantly reduced. The patient did not show symptoms of fever, vomiting, diarrhea, or passage of bloody stools. In the ED, abdominal examination revealed soft, tympanic percussion and irritable crying during palpation without muscle guarding. Blood tests revealed leukocytosis (24 100/µL) and elevated C-reactive protein (8.01 mg/dL). Abdominal radiography revealed dilated bowel loops in the upper abdomen and a paucity of bowel gas over the lower abdomen. Abdominal sonography revealed one 3.19 cm × 3.46 cm concentric hypo- and hyper-echoic target lesion over the right abdomen without ascites (Figure 1). Under the impression of intussusception, the patient underwent immediate hydrostatic reduction. After which, his symptoms subsided, and he was asleep all night.
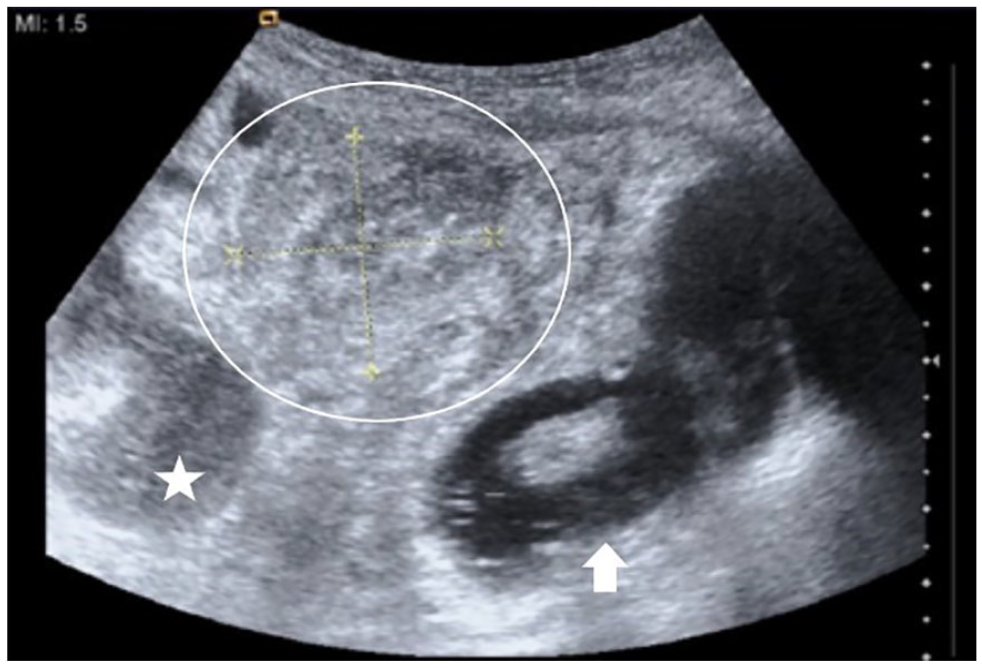
Sonography of intussusception before operation: a target lesion (circle), beside the right kidney (star), under hydrostatic reduction (arrow).
However, irritable crying resumed on the following day. Muscle-guarding was also observed. Based on the patient’s clinical symptoms and physical examination findings, the possibility of intestinal rupture with complications of peritonitis was suspected. After consulting with a pediatric surgeon, the patient underwent immediate laparoscopic laparotomy. During the surgery, the pediatric surgeon discovered that the appendiceal tip had a necrotic appearance with adhesions between the appendix and cecum (Figure 2) with erythematous changes around the ileocecal region. No recurrent intussusceptions were observed. Consequently, the patient underwent laparoscopic appendectomy and was administered antibiotic injections for a duration of 1 week. His-topathological examination confirmed hyperemia, edema, and infiltration of polymorphonuclear leukocytes throughout the whole thickness of the excised appendix. There was no recurrent abdominal pain or fever after treatment. The patient started oral intake smoothly 2 days after surgery and was discharged after antibiotic treatment without complications.
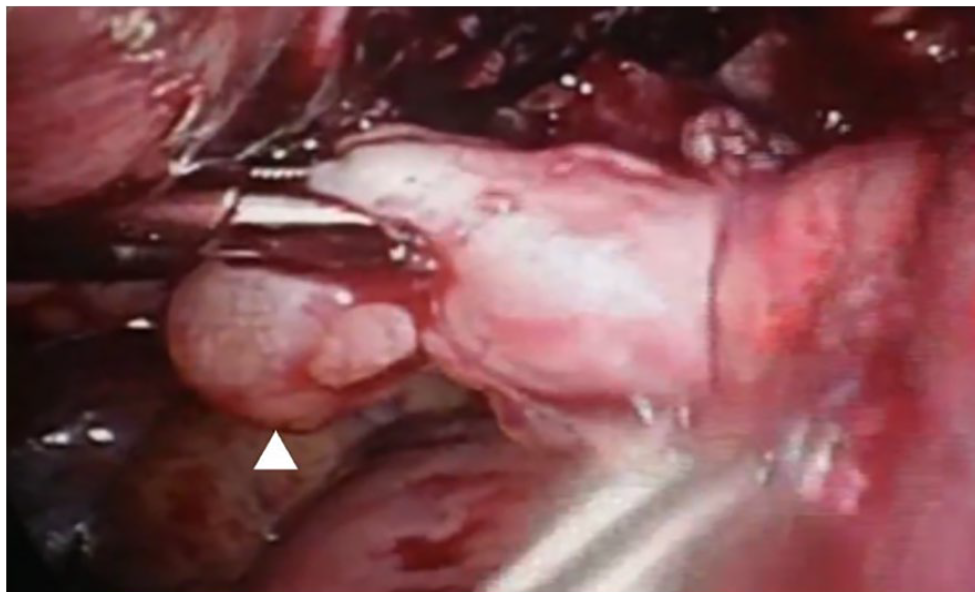
Surgical finding: swollen appendix with necrotic appearance of the appendiceal tip (arrowhead).
Discussion
We report a rare case of simultaneous intussusception and appendicitis in a 10-month-old infant. Intussusception was confirmed using sonography, and the symptoms subsided after hydrostatic reduction. A surgical diagnosis of ruptured appendicitis with ileitis was made. In-tussusception and appendicitis are both emergent gastrointestinal diseases in children, which may result in severe complications without prompt diagnosis and intervention. However, these diseases have similar clinical symptoms, including severe abdominal pain and irritable crying. This makes it difficult to distinguish them in infants. Sonography is an important tool for imaging examination, with high sensitivity and specificity for both diseases.1,2 However, our patient had a typical target lesion but no evidence of appendicitis, such as tubular lesions or ascites.
These diseases typically occur in different age groups.1,2 Intussusception frequently occurs in children younger than 3 years of age, while appendicitis is more common in adolescents. Acute appendicitis is rare in infants. Due to the poor communication skills of this age group and the lack of specific symptoms, acute appendicitis is usually diagnosed under operation. 3 Furthermore, in infants, appendicitis can progress rapidly and lead to rupture. Seventy percent of patients younger than 3 years old develop a perforation within 48 hours of symptom onset. 4 More than this rarity, it coexisted with intussusception in our presented case.
The simultaneous presence of intussusception and appendicitis is exceedingly rare in children, with previous reports only involving cases in 3- and 5-year-old children.5,6 We further confirmed that these 2 diseases could occur simultaneously in infants. In our case, we initially diagnosed intussusception and identified appendicitis; however, we could not confirm the onset of appendiceal inflammation before or after intussusception.
No previous reports have confirmed that appendicitis is induced by intussusception. In contrast, the appendix can be a leading cause of intussusception, both in normal and pathological appendices. 7 Neither the previous CT nor the operation revealed the presence of any other intra-abdominal lesion acting as a leading point for the intussusception. However, if a CT scan had been performed at that time, it might have provided more detailed information to precisely diagnose these 2 conditions. However, imaging studies should not impede emergency surgeries if patients have signs of intestinal perforation. Delay in initiating emergency surgery is associated with a significant increase in morbidity and mortality. 8 In our case, we did not perform CT examination as the patient presented with obvious peritoneal signs and there was a possibility of intestinal perforation after previous hydrostatic reduction. Therefore, immediate surgical intervention was performed.
In conclusion, intussusception and appendicitis can occur simultaneously in infants. Although the diagnosis of appendicitis in infants can be particularly challenging due to non-specific symptoms and their young age, it is important to remain vigilant and recognize that this is an important medical condition that should not be disregarded. When dealing with intussusception, it is important to consider other emergent gastrointestinal diseases, such as appendicitis, as potential differential diagnoses if the patient experiences recurrent irritable crying after hydrostatic reduction, instead of solely suspecting recurrent intussusception.
Author Contributions
T-CW and C-FH contributed to the study conception and design; C-SL and S-HS contributed to the data collection; C-FH contributed to the analysis and interpretation of results; C-KH contributed to the draft manuscript preparation. All authors reviewed the results and approved the final version of the manuscript.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This article was supported by Taipei Veterans Hospital (Grant number: V111C-208).
Ethical Clearance
Written informed consent for the publication of patient information and images was provided by a legally authorized representative.
Informed Consent
Written informed consent for patient information and images to be published was provided by a legally authorized representative.