
Abstract
Educational Objectives
Supracondylar humeral fractures are among the most common fractures in the pediatric population.
Point-of-care ultrasound can be performed at the bedside to aid in screening for elbow fractures in the pediatric population.
Case Report
A 6-year-old female with no pertinent past medical history presented to the pediatric emergency department (PED) with left elbow pain after sustaining a fall the day prior. As per the patient’s mother, the patient was playing when she tripped and landed on her left elbow. The mother denied any head injury, trauma, or loss of consciousness. Upon standing from her injury, the child could not move the elbow from the flexed position; however, her parents noted minimal swelling. On presentation to the PED, the family stated the pain had worsened, and the child could not move the elbow in any direction. Vital signs were appropriate for the patient’s age. The child had her left elbow held approximately at a 40° angle, supporting her wrist with the contralateral hand. The musculoskeletal exam was notable for tenderness to palpation and edema along the olecranon and the posterior aspect of the distal humerus, as well as tenderness to palpation at the proximal radial head. There was a decreased range of motion in both flexion and extension of the elbow due to pain. No apparent signs of deformity, ecchymosis, or laceration were appreciated. The patient could flex and extend her fingers, capillary refill was less than 2 seconds, and the radial pulse was intact.
Discussion
Hospital Course
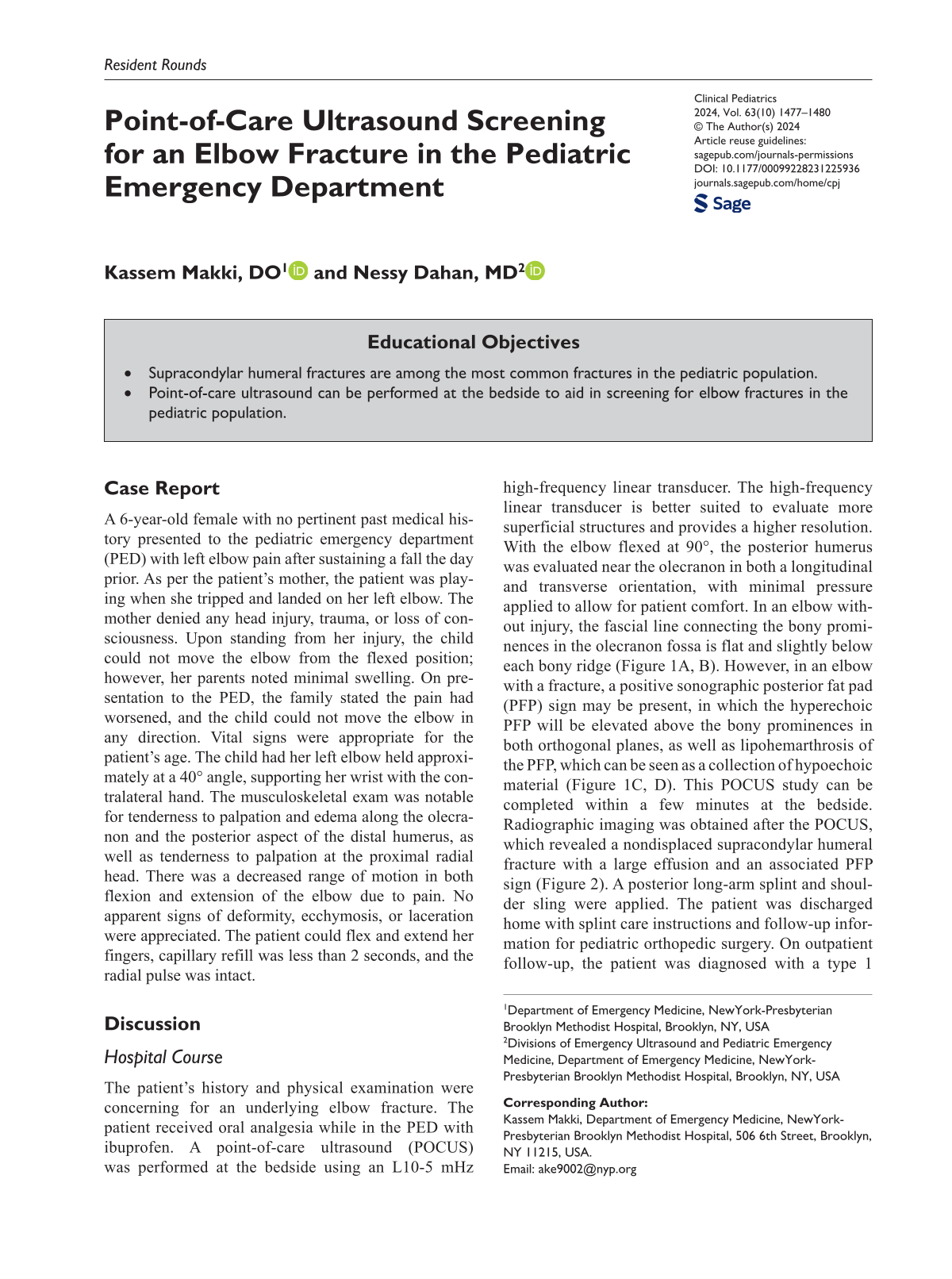
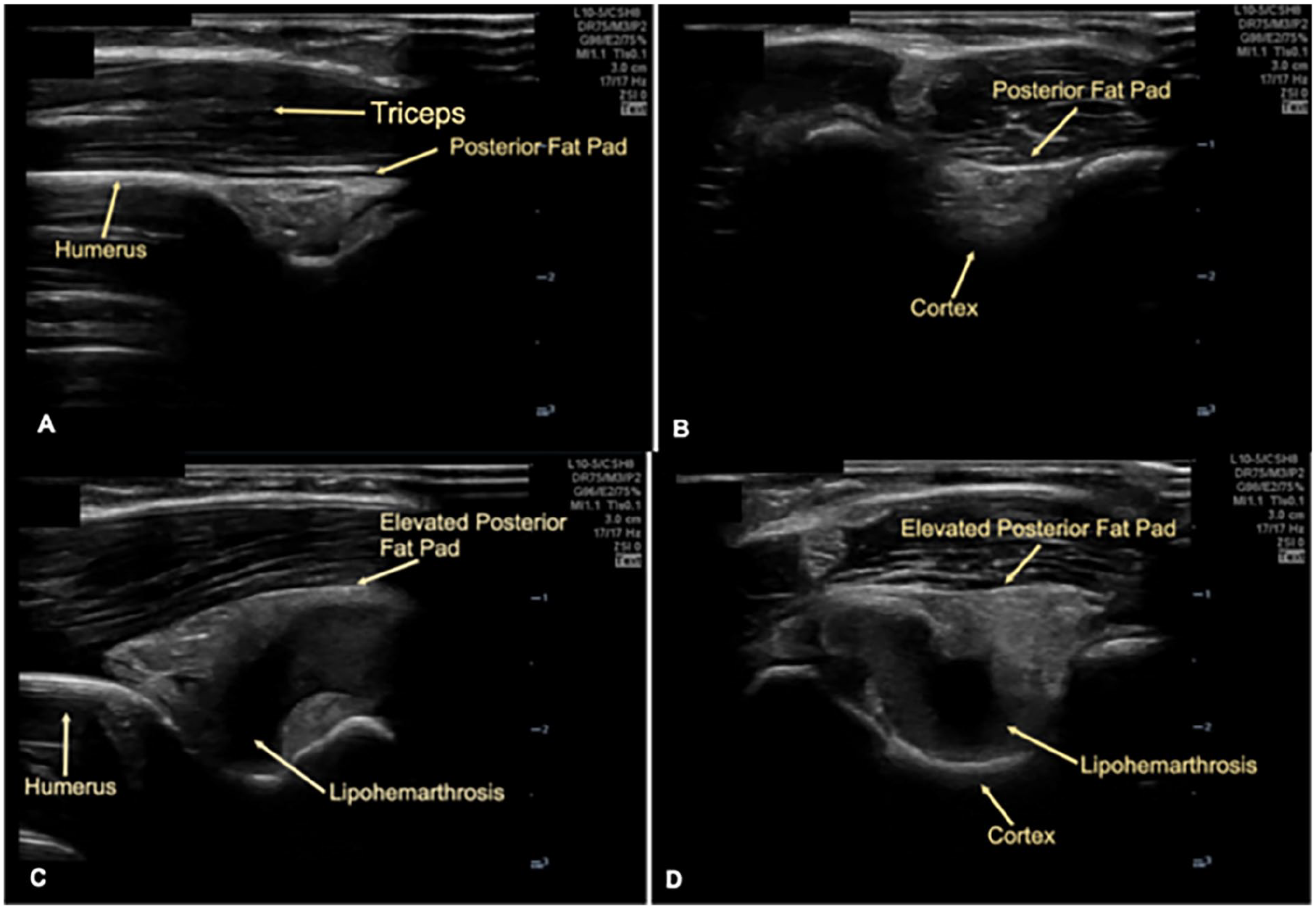
The patient’s history and physical examination were concerning for an underlying elbow fracture. The patient received oral analgesia while in the PED with ibuprofen. A point-of-care ultrasound (POCUS) was performed at the bedside using an L10-5 mHz high-frequency linear transducer. The high-frequency linear transducer is better suited to evaluate more superficial structures and provides a higher resolution. With the elbow flexed at 90°, the posterior humerus was evaluated near the olecranon in both a longitudinal and transverse orientation, with minimal pressure applied to allow for patient comfort. In an elbow without injury, the fascial line connecting the bony prominences in the olecranon fossa is flat and slightly below each bony ridge (Figure 1A, B). However, in an elbow with a fracture, a positive sonographic posterior fat pad (PFP) sign may be present, in which the hyperechoic PFP will be elevated above the bony prominences in both orthogonal planes, as well as lipohemarthrosis of the PFP, which can be seen as a collection of hypoechoic material (Figure 1C, D). This POCUS study can be completed within a few minutes at the bedside. Radiographic imaging was obtained after the POCUS, which revealed a nondisplaced supracondylar humeral fracture with a large effusion and an associated PFP sign (Figure 2). A posterior long-arm splint and shoulder sling were applied. The patient was discharged home with splint care instructions and follow-up information for pediatric orthopedic surgery. On outpatient follow-up, the patient was diagnosed with a type 1 supracondylar humeral fracture, placed in a fiberglass cast, and instructed to follow-up in 3 to 4 weeks for repeat clinical and x-ray evaluation.
Longitudinal (A) and transverse (B) sonographic views of the unaffected right elbow, with a normal-appearing posterior fat pad congruent with the humeral line and without evidence of lipohemarthrosis. Longitudinal (C) and transverse (D) sonographic views of the affected left elbow showed abnormal PFP elevation above the humeral line and lipohemarthrosis of the posterior fat pad.

Plain radiograph of the left elbow demonstrating a nondisplaced supracondylar humeral fracture with a large effusion and an associated posterior fat pad sign (arrow).
Discussion of Case and Literature
A common chief complaint among the pediatric patient population in the PED is a painful upper extremity, especially after a traumatic event such as a fall. Underlying fractures are an important consideration in the differential diagnosis, especially in the case of trauma. Pediatric fractures commonly involve the radius (54.5%), supracondylar region (18.3%), and proximal humerus (8.6%). 1 With regards to the elbow, fracture types may involve the supracondylar humerus, radial neck, lateral condyle, and medial epicondyle. 2 Other causes of posterior elbow pain in young patients include olecranon apophysitis or avulsion, olecranon bursitis, posterior olecranon impingement, or olecranon osteochondrosis. 3 Occult fractures constitute 2% to 18% of all fractures seen in children. 4 Along with a good history and physical exam, proper imaging modalities are needed to define the fracture’s type, location, and severity.
The PED provider often encounters difficulties in evaluating for fractures due to the complexity of pediatric anatomy, necessitating a careful balance between diagnostic accuracy and minimizing radiation exposure. Plain radiography is often used as a first-line imaging modality for suspected upper extremity fractures; however, a fracture can be difficult to discern due to overlapping bones, growth plates, and maturing bones in the pediatric population. 5 The PFP sign on plain radiographs serves as a diagnostic finding for occult elbow fractures. 6 However, the radiographic PFP sign can be subtle and falsely negative if missed, or may be falsely positive if radiographic images are obtained with the elbow not flexed adequately at 90°. 5
Point-of-care ultrasound is a valuable adjunct, offering a fast and safe alternative to screen for upper extremity fractures at the bedside without radiation exposure, especially when radiographs are not immediately available. While proper positioning is important for both POCUS and radiographic evaluation, administration of an oral analgesic may allow for patient comfort for both imaging modalities. The sonographic PFP sign, along with evidence of lipohemarthrosis, are sonographic findings highly suggestive of a fracture within the elbow joint. In a study standardizing the sonographic examination of pediatric elbow injuries, the researchers found that the abnormal PFP sign, as a sole parameter for fracture detection, had a sensitivity of 0.97, specificity of 0.97, a positive predictive value of 0.97, and a negative predictive value of 0.97. 6 A second study showed that the presence of an elevated PFP or lipohemarthrosis on POCUS evaluation of the elbow in pediatric patients with an elbow injury had a sensitivity of 98%, specificity of 70%, positive likelihood ratio of 3.3, and negative likelihood ratio of 0.03 for a fracture. 7
It is important to note that while ultrasound can significantly aid in diagnosis and management of pediatric elbow fractures, it may not entirely replace plain radiographs, which remain crucial for definitive classification of fracture type and further management, whether conservative or surgical. An experienced sonographer may be able to deduce fracture type if there is evidence of bony cortex disruption, though this may often be difficult to discern sonographically, especially in a child with varying ossification centers within the elbow joint. 7 In addition, despite the benefits of POCUS, challenges persist. High-quality equipment, albeit essential for optimal imaging, may not be available due to high costs limiting widespread use in all PEDs. In addition, the interpretation of radiographs by pediatric radiologists, even if not physically present at the site, offers specialization and enhanced accuracy through centralization. In contrast, POCUS, though accessible in many PEDs, introduces a variable skill set among its users and is operator-dependent, raising concerns about consistency in image acquisition and proficiency of image interpretation. 8
Point-of-care ultrasound may prove most beneficial in resource-poor regions without access to timely radiography or interpretation or in cases where the obtained radiograph is equivocal for a fracture. In the case of the latter, evidence of a sonographic PFP sign or lipohemarthrosis may provide the PED team additional diagnostic information to aid in management, and ultimately lead to splinting the upper extremity to stabilize the joint and referral to the pediatric orthopedic team for a possible occult fracture. In addition, in cases of an elbow injury with a low pretest probability for a fracture based on a reassuring musculoskeletal examination, POCUS may allow for rapid screening for sonographic features suggestive of a fracture at the bedside, or lack thereof, and possible avoidance of radiography and radiation exposure as determined by the medical provider, given its high sensitivity, high negative predictive value, and low negative likelihood ratio for elbow fractures.6,7
Final Diagnosis
With the aid of both POCUS and radiography, the patient was ultimately diagnosed with a type 1 supracondylar humeral fracture at the pediatric orthopedic surgery outpatient follow-up visit.
Conclusion
Supracondylar humeral fractures are among the most common fractures seen in the pediatric population. Diagnostic imaging with plain radiographs has been shown to have confounding variables, such as overlapping bones, growth plates, and maturing bones in the pediatric population. Point-of-care ultrasound offers a quick and effective imaging modality that can be performed at the bedside to screen for and aid in diagnosing and managing patients with suspected elbow fractures, especially those that are occult. The case presented illustrates the utility of POCUS as a screening tool for identifying features suggestive of an elbow fracture in pediatric patients coming to the PED after a traumatic event. However, a limitation of POCUS is its inability to further classify the fracture type, crucial for determining the appropriate treatment approach. Future studies should explore protocols where POCUS serves as the primary screening tool, potentially reducing the reliance on radiography and associated radiation exposure in the PED. Furthermore, a comprehensive assessment of cost-effectiveness and overall morbidity could shed light on the advantages and disadvantages of POCUS compared to plain radiographs in diagnosing and managing upper extremity fractures in the pediatric population.
Author Contributions
KM: Contributed to conception and design; contributed to analysis; drafted the manuscript; revised the manuscript; gave final approval; agrees to be accountable for all aspect of work ensuring integrity and accuracy.
ND: Contributed to conception and design; contributed to analysis; drafted the manuscript; revised the manuscript; gave final approval; agrees to be accountable for all aspect of work ensuring integrity and accuracy.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.