
Abstract

Educational Objectives
Unintentional THC ingestions range in symptoms and can present in groups, such as a family, and should be included in the differential diagnosis for the acutely altered patient.
Unintentional THC ingestions in children are preventable and it is the responsibility of medical providers to treat such incidents as sentinel events, and educate our communities to create safe environments for the children that we care for.
Case Report
A 6-year-old boy was brought to the Emergency Department (ED) by Emergency Medical Services (EMS) with concern for acute anaphylaxis.
Emergency Medical Services was notified of a 6-year-old boy and 34-year-old mother complaining of shortness of breath. Upon their arrival to the scene, EMS clinicians found additional EMS units already there responding to a different call. It was reported that the boy was at home with his parents sharing “box-mixed” pancakes for breakfast when the family began experiencing a range of symptoms. The boy’s father developed chest pain and dizziness while eating. He reportedly also developed mental status changes and was taken earlier by EMS responders to a nearby hospital and evaluated for suspected stroke. The boy and his mother developed symptoms shortly thereafter. On EMS arrival, they found both to have “labored breathing” and “altered mental status.” EMS providers report a normal point of care glucose for both mother and son, and administered naloxone to both with no significant response. The 6 year old then began to have non-bloody emesis and alterations in consciousness. Given the constellation of symptoms and multisystem involvement, he was treated with epinephrine, dexamethasone, Benadryl, and albuterol for presumed anaphylaxis. The 6-year-old patient and his mother were both taken to the same children’s hospital ED.
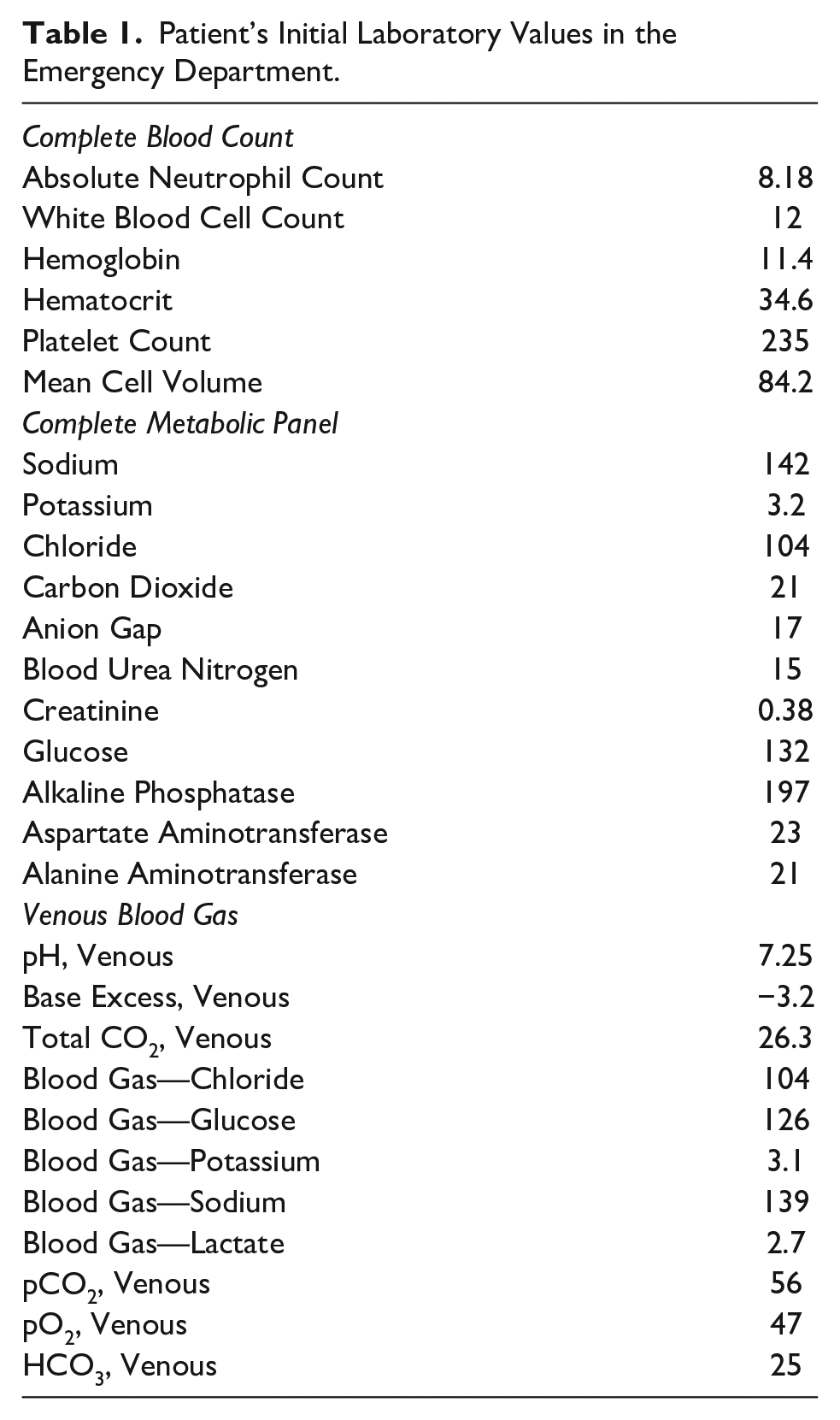
On arrival to the ED, the patient and his mother were both found to be obtunded. The mother was assessed, stabilized, and transferred to the Adult ED. Our patient, the 6-year-old boy, presented with the following vital signs; heart rate 128 beats/min; blood pressure 100/69 mm Hg; respiratory rate 18 breaths/min; oxygen saturation 98%; and an end-tidal carbon dioxide 47 mm Hg. On exam, he was in no acute distress, his pupils were 4 mm and reactive bilaterally, he had a normal cardiopulmonary exam and exhibited no hyperreflexia, clonus, nor rigidity. He was calculated to have a Glasgow Coma Scale of 9. Intravenous access was obtained, labs including toxicology studies of blood and urine were sent, and supplemental oxygen was administered via non-rebreather without clinical change. An additional trial of naloxone was administered with no significant response. While he continued to breathe spontaneously, given his alteration in consciousness, the team prepared for possible intubation. Laboratory studies obtained on arrival are found in Table 1. Venous blood gas was notable for a mild respiratory acidosis with pH 7.29 and PCO2 52 mm Hg and his co-oximetry panel was normal. Computed tomography of the head and chest radiography were both normal. Decision was made to forgo intubation. Decision was then made to transfer the patient to the Pediatric Intensive Care Unit (ICU) for further care and cardiopulmonary monitoring.
Patient’s Initial Laboratory Values in the Emergency Department.
Discussion
Hospital Course
The patient arrived to the ICU where he continued to exhibit somnolence. The toxicology service was consulted due to persistent lethargy and concern for a potential ingestion. Notably, the patient’s presentation did not seem to align with other toxidromes featuring lethargy. Serum toxicology screens for acetaminophen, salicylate, and ethanol were negative, and qualitative urine drug screen was positive for tetrahydrocannabinol (THC) (Table 2). The Child Advocacy team was consulted, and Child Protection Services along with social work were promptly alerted and involved for further inquiry and investigation.
Qualitative Urine Drug Screen and Serum Drug Screen.

Further evaluation to rule-out infection with a lumbar puncture, magnetic resonance imaging and electroencephalogram were all deferred after early detection of THC by urine drug screen. Serial neurological exams showed progressive improvement in mentation. He remained hemodynamically stable throughout monitoring in the ICU, and ultimately returned to baseline independent of any further medical intervention. After a 24-hour intensive care admission, the child was transferred to the medical floor for ongoing evaluation and consultation with the child protection team. The child was ultimately discharged with a family member pending safe placement determination from child protective services.
The patient’s mother was observed in the adult ED where her work-up was significant for a positive qualitative urine drug screen for THC. She reported giving “a gummy treat” to her husband and her child.
Discussion of Case
Pediatric exposure to THC is on the rise.1,2 National Poison Data System revealed a 1375.0% increase in the number of reported pediatric THC ingestions between 2017 and 2021. 2 This is largely due to increasing availability of THC-infused products following their legalization for recreational use, their resemblance to other snacks or treats in copycat packaging, and unsafe storage in the home.3-6 Currently, recreational use of marijuana and cannabinoid products has been legalized in 23 states with emerging evidence showing an association between legalization and this rising trend of pediatric exposures. 7 The ingestion of THC-infused products leads to higher concentrations of the potent psychoactive metabolite, 11-OH-THC. This is likely due to a greater rate of hepatic hydroxylation of Δ9-THC into 11-OH-THC, producing longer lasting and more potent effects on the central nervous system. 8 Bolstering the societal impact of these products is the dearth of regulatory restrictions governing the production and packaging of THC edibles. A major implication is that the concentration of THC in edible products varies greatly between products and vendors. As a result, significant toxicities have been observed from a seemingly small volume ingestion.8,9 Furthermore, THC edibles are often sold to resemble gummies, candies, cookies, beverages, or other common consumables which appear visually appealing to children. When poorly stored or labeled, edibles may be found by children or unintentionally given to children resulting in toxicity.
The presentation of THC ingestions range significantly from asymptomatic to critically ill. The most common presenting symptom of pediatric THC toxicity is lethargy.2,10 Other symptoms may also include ataxia, tachycardia, emesis, mydriasis, hypotonia, seizures, and altered mental status. 11 Bradycardia and atrioventricular heart block have also been reported in young infants. 12 In adolescents, somnolence may be interspersed with periods of agitation often requiring pharmacologic measures to control. 13 In cases of severe toxicity, respiratory depression and coma may occur. Some data suggest that ingestions of products containing THC concentrations of 1.7 mg/kg or higher, may predict severe toxicity. 14
Due to variable and impressive presentations, pediatric patients with unintentional THC ingestion often undergo extensive, invasive, and costly evaluations, as the differential for the acutely altered patient is vast and could be life-threatening. 15 Notably, when acute neurological symptoms are present without respiratory compromise, THC intoxication should be strongly considered. Collateral information, if available, is crucial to understand the events leading to presentation and assess for possible exposures in or around the home. A thorough history, along with early and rapid urine drug screening, is pivotal to confirm suspicion early on and may prevent unnecessary imaging or medical interventions. While urine drug screens are fairly specific for detecting THC, serum THC testing should be considered for confirmation; however, this can take several days to result and would not help in the immediate period.
Given the potential severity of THC exposure, the authors suggest considering unintentional ingestions akin to sentinel events. Medical providers encountering pediatric THC exposure should treat the incident as a serious, harmful, yet an avoidable event within the patient’s environment. 16 Upon confirmation of exposure, thorough interviewing should be conducted to determine the original storage circumstances of the offending agent and how the exposure transpired. Mandatory reporting to Child Protection Services teams also facilitates systematic review of the child’s environment to identify root causes. In addition, coordination with social work and Child Advocacy teams is vital toward providing support to family, obtaining information, and preventing recurrence. If available, medical lock boxes may be provided to parents to safeguard their medication from household children. 17 Ultimately, education and engagement with the patient’s family on proper storage and safe use of THC edibles is essential to preventing future unintentional exposures.
Unintentional THC ingestions in the pediatric population typically present in isolation, as individual cases. To our knowledge, this is the first case series of a familial exposure and presentation to the ED with altered mental status due to THC toxicity.
Final Diagnosis
Acute THC toxicity in a 6-year-old boy and his parents.
Conclusion
Tetrahydrocannabinol ingestions in pediatric patients may be challenging to ED providers. Highly variable clinical presentations, the loss of reliable history, and the broad differential diagnosis of the acutely altered child pose several diagnostic and therapeutic dilemmas. With increasing availability of cannabinoid products without stringent production and packaging regulations and the subsequent rising prevalence of pediatric ingestions, ED providers should begin to strongly consider THC intoxication high on the differential of the acutely altered patient and use urine drug screening for early detection. Furthermore, patient family education and ingestion prevention is necessary and must be addressed earlier as routine preventive care. ED and primary care providers should routinely provide parents with anticipatory guidance regarding the safe storage and use of edible THC products as they become more ubiquitous in society.
Author Contributions
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Our case report did not require an ethical board approval because per Northwell Health institutional guidelines: the review of medical records for publication of case reports of up to 3 patients is not considered human-subject research and does not require IRB review and approval.