
Abstract
Background:
It is necessary to evaluate the risk factors of secondary bleeding after tonsillectomy in children, to provide reference for clinical children management and care.
Methods:
Children who underwent tonsillectomy from January 1, 2018, to December 31, 2022, in our hospital were retrospectively included. The characteristics of children with and without secondary bleeding were analyzed.
Results:
A total of 1068 children undergoing tonsillectomy were included, and the incidence of secondary bleeding children undergoing tonsillectomy was 4.87%. Age ≥ 9 years old (odds ratio [OR] = 2.609, 95% confidence interval [CI] = 2.112-3.437), type of surgery (OR = 1.764, 95% CI = 1.148-2.291), and degree of tonsil embedding (OR = 2.116, 95% CI = 1.805-2.644) were the risk factors of secondary bleeding after tonsillectomy in children (all P < .05).
Conclusion:
Medical staff should proactively monitor and address the identified risk factors by implementing timely warning systems and preventive strategies to reduce the postoperative bleeding following tonsillectomy.
Introduction
Tonsillectomy is a prevalent procedure within the field of otorhinolaryngology. In recent years, advancements in medical technology have led to the introduction of numerous innovative techniques for performing tonsillectomies. These include unipolar electrocoagulation, bipolar electrocoagulation, laser surgery, ultrasonic scalpel, and plasma radiofrequency ablation, among others. Each of these methods offers unique advantages and considerations, contributing to the ongoing evolution of this surgical practice.1,2 But postoperative bleeding is still one of the most important and even fatal complications. Post-tonsillectomy bleeding represents a grave complication that demands vigilant preventive measures. Inadequate prevention can result in challenging bleeding episodes, with severe cases posing a significant risk to the patient’s life. 3 Therefore, the prevention and management of bleeding after tonsillectomy are of great significance to the prognosis of patients. 4
Postoperative bleeding is the main complication following tonsillectomy, occurring at a rate that ranges from 2.41% to 16.22%.5-7 Bleeding after tonsillectomy can be divided into primary bleeding and secondary bleeding. Primary bleeding occurs within 24 hours after operation, and secondary bleeding occurs 24 hours after operation. Primary bleeding is considered to be related to surgical technique, while secondary bleeding is considered to have no correlation with surgical technique, which is mainly observed within 10 days after operation. 8 Currently, the majority of research has predominantly concentrated on comparing the operative duration and intraoperative blood loss associated with various surgical techniques. However, there is a notable scarcity of studies that delve into the risk factors contributing to postoperative bleeding.9,10 Recognizing the patterns and influencing factors of bleeding after surgery is crucial for implementing proactive strategies that can mitigate the risk of such complications. By identifying the specific factors that contribute to postoperative bleeding, medical professionals can tailor their approach to patient care. This includes the development of targeted interventions and the provision of personalized post-operative care plans. Effective early interventions can lead to better management of postoperative complications, thereby potentially reducing the need for additional medical interventions and improving the quality of life for patients who have undergone tonsillectomy. Therefore, this research has undertaken a retrospective review of cases involving postoperative bleeding in pediatric patients after tonsillectomy, assessing the factors that related to this complication. The objective of this analysis is to provide useful implications for clinical treatment strategies and postoperative management for children who have had tonsillectomy surgery.
Methods
Population
This study included children who underwent tonsillectomy from January 1, 2018, to December 31, 2022, in the Department of Otolaryngology in our hospital as the study population. The inclusion conditions of the children were as follows: The age of the child was less than or equal to 16 years old; the disease was caused by sleep apnea due to tonsillar adenoid hypertrophy and chronic tonsillitis caused by acute suppurative tonsillitis more than 3 times a year for more than 2 years; the children underwent tonsillectomy in our hospital; and the children and their parents agreed to participate in this study. The exclusion criteria were as follows: children with history of acute inflammation of tonsil in recent 2 weeks, children with history of autoimmune diseases and other consumptive diseases, and children with hematological diseases.
All operations were performed under oral intubation and intravenous anesthesia. The children were positioned with their shoulders elevated and heads slightly lowered, facilitating the use of a mouth prop to keep the mouth open. Using the low-temperature plasma surgery system, a therapeutic device manufactured by Jesse Company, USA, the surgical team conducted repeated assessments of the wound throughout the procedure.11,12 We meticulously controlled bleeding throughout the surgery, making repeated interventions until no active bleeding was visibly evident to the naked eye by the conclusion of the procedure.
Data Collection
We collected the age, sex, body mass index (BMI), diagnosis, experience of surgery operator, type of surgery (total excision, partial excision, and total retention), degree of tonsil embedding, and duration of surgery from the medical record. In this study, secondary bleeding was defined as bleeding at the surgical site in children 24 hours after tonsillectomy. 8 The classification criteria of tonsil embedding degree were as follows: According to the size of tonsil pulled out of tonsillar fossa before operation, tonsil is divided into mild, moderate, and severe; >75% of tonsillar tissue protruding from tonsillar fossa was mild, <25% of tonsillar tissue protruding from tonsillar fossa was severe, and between the 2 was moderate. 13 The classification standard of surgical methods: cutting the mucosa along the mucosal junction of palatolingual arch and tonsil, exposing the tonsillar capsule, and then complete tonsillectomy along the tonsillectomy was total tonsillectomy. A certain amount of tonsillar tissue, tonsillar capsule, and tonsillar space are preserved during the operation, which was partial tonsillectomy. Postoperative tonsillar bleeding was graded according to different hemostatic methods and with or without blood transfusion, 14 including a total of 4 grades. I grade: after using hemostatic and anti-inflammatory drugs or without any treatment to stop bleeding or suck out clots, II grade: stop bleeding under general anesthesia by endotracheal intubation, III grade: ligation of external carotid artery to stop bleeding, and IV grade: bleeding has endangered the life of children. Throughout the research process, strict data quality control should be conducted, including data verification and data auditing, to ensure the quality of the data.
Statistical Analysis
SPSS 23.0 software was used for data processing. Categorical data were expressed as counts (n) and percentages (%) for the respective categories. Continuous variables were depicted as mean ± standard deviation (SD) for normally distributed data and median with interquartile range (IQR) for skewed data. T-test or nonparametric test was used to compare measurement data between groups, and χ2 test was used to compare counting data between groups. Spearman correlation analysis was conducted to analyze the correlation of secondary bleeding and characteristics of included children. Logistic regression analysis was performed to evaluate the risk factors of secondary bleeding after tonsillectomy in children. P < .05 showed that the difference between groups was statistically significant.
Ethics Statement
This study, which used a retrospective cohort design, was conducted with the approval of the Ethics Committee at the Children’s Hospital of Nanjing Medical University (Approval Number: 202208162-1). This investigation did not obtain written informed consent from the included patients. However, this study protocol was reviewed and approved by the Ethics Committee and all data were processed and reported in an anonymized manner to ensure confidentiality.
Results
A total of 1068 children undergoing tonsillectomy were included. The average age of included children was 6.18 years old, and most children were diagnosed as adenoid hypertrophy. The characteristic details of included children were presented in Table 1.
The Characteristics of Included Children (N = 1068).
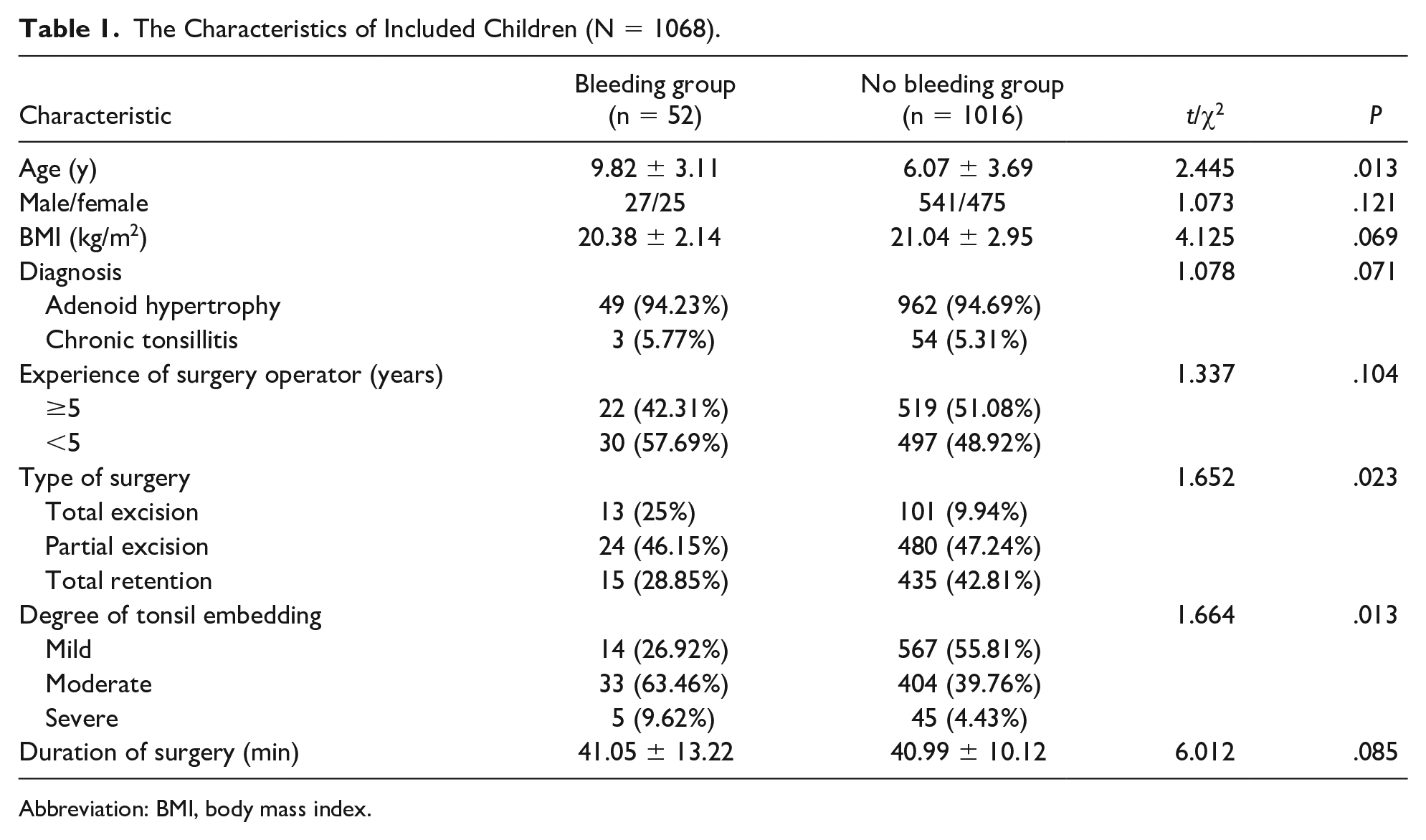
Abbreviation: BMI, body mass index.
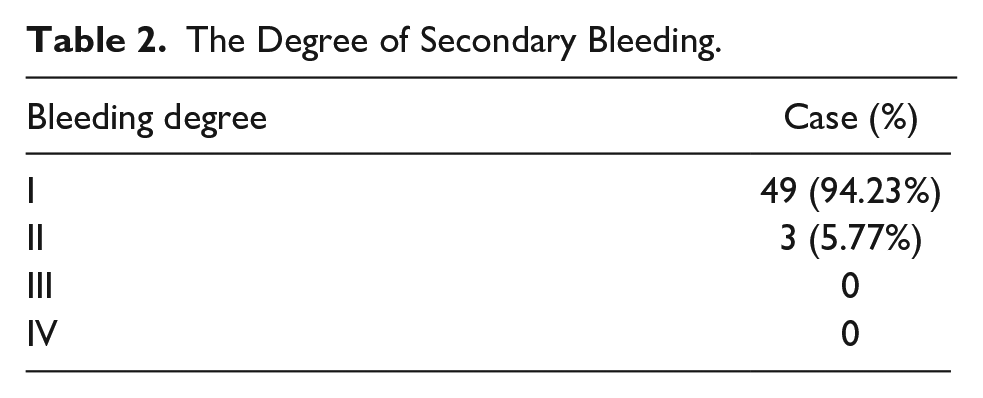
Fifty-two children had the secondary bleeding, and the incidence of secondary bleeding children undergoing tonsillectomy was 4.87%. Among the 52 patients with secondary bleeding, 49 cases were grade Ⅰ, 3 cases were grade Ⅱ (0.9%), and 0 cases were grade Ⅲ and Ⅳ (Table 2). All patients with secondary bleeding occurred within 14 days after operation, mostly concentrated on the fourth to seventh day after operation. All children were treated with epinephrine gargle, intravenous drip hemostatic or without any treatment to stop bleeding, and none of them endangered their lives in this study. There were significant differences in the age, type of surgery, and degree of tonsil embedding between children with and without secondary bleeding (all P < .05). There were no significant statistical differences observed in terms of sex, BMI, diagnosis, the experience of the surgical operator, and the duration of surgery between the groups of children who experienced secondary bleeding and those who did not (all P > .05), indicating that those factors might not be associated with the occurrence of secondary bleeding.
The Degree of Secondary Bleeding.
As shown in Table 3, age (r = 0.614), type of surgery (r = 0.538), and degree of tonsil embedding (r = 0.524) were all associated with the occurrence of secondary bleeding in children with tonsillectomy (all P < .05).
The Correlation of Secondary Bleeding and Characteristics of Included Children.
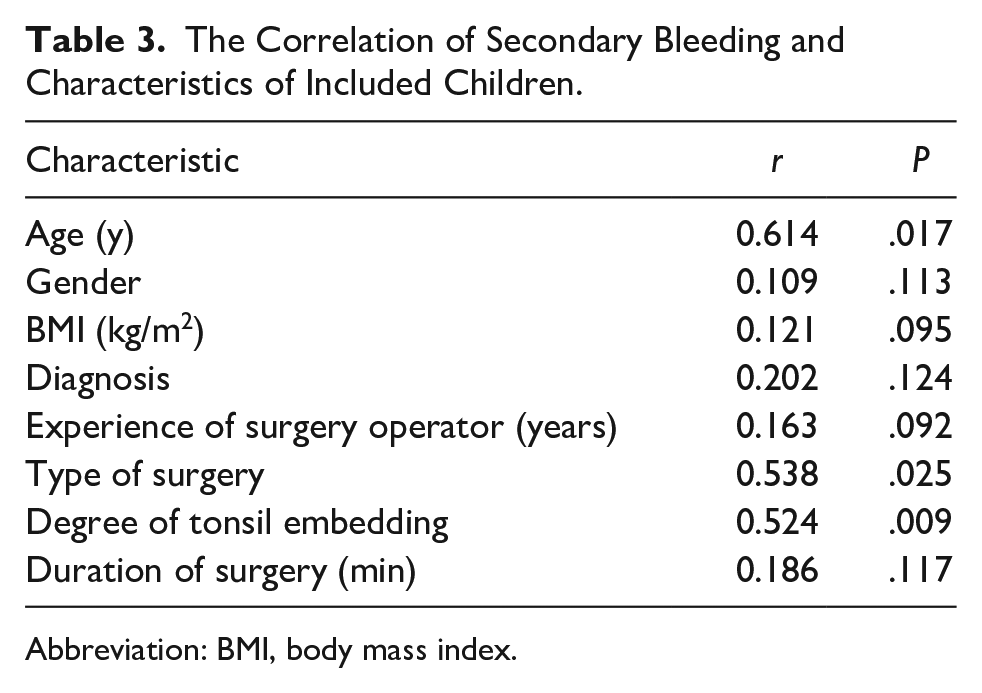
Abbreviation: BMI, body mass index.
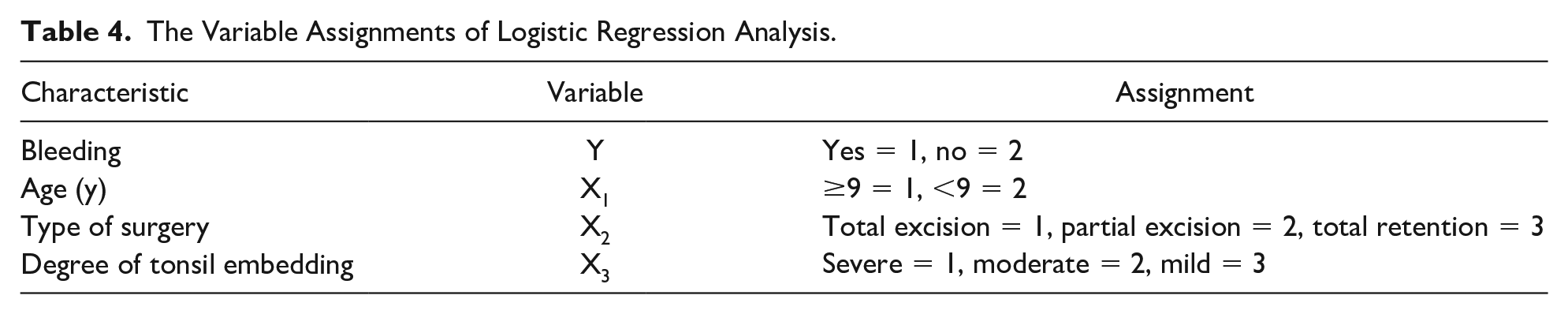
The variable assignments of logistic regression analysis are shown in Table 4. As shown in Table 5, the results of logistic regression analysis indicated that age ≥9 years old (odds ratio [OR] = 2.609, 95% confidence interval [CI] = 2.112-3.437), type of surgery (OR = 1.764, 95% CI = 1.148-2.291), and degree of tonsil embedding (OR = 2.116, 95% CI = 1.805-2.644) were the risk factors of secondary bleeding after tonsillectomy in children (all P < .05).
The Variable Assignments of Logistic Regression Analysis.
Logistic Regression Analysis on the Risk Factors of Secondary Bleeding After Tonsillectomy in Children.
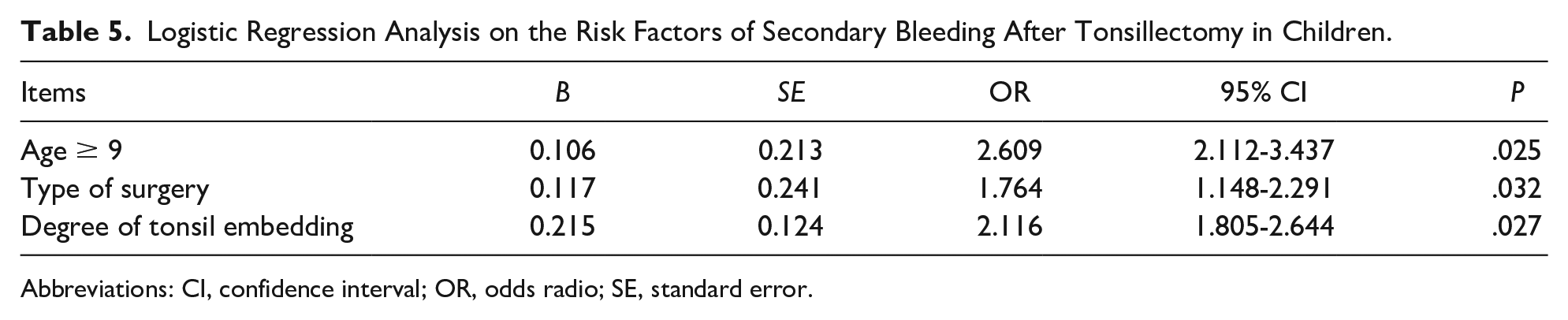
Abbreviations: CI, confidence interval; OR, odds radio; SE, standard error.
Discussions
This study has uncovered that the rate of secondary bleeding post-tonsillectomy is 4.87%. Moreover, it has delineated age, the nature of the surgical intervention, and the depth of tonsil embedding as variables significantly linked to the likelihood of secondary bleeding in children who have undergone the procedure. It is crucial to recognize that children, having a lower blood volume than adults, are at a greater risk of experiencing respiratory and circulatory system failure in the event of significant bleeding. This increased vulnerability underscores the importance of careful monitoring and prompt medical intervention for pediatric patients. 15 Consequently, for pediatric patients, postoperative hemorrhage can quickly escalate into a severe and potentially life-threatening complication of tonsillar surgery. Due to the lack of a unified and explicit criterion for defining the severity of tonsillar bleeding, combined with variations in postoperative hospital stay and follow-up practices, there is a significant variation in the reported rates of postoperative bleeding following tonsillectomy.16-18 Clinically, health care professionals should implement early and effective intervention strategies targeting these influential factors to reduce the incidence of postoperative bleeding in pediatric patients after tonsillectomy.
This study’s findings reveal that age emerges as a significant independent risk factor for the incidence of bleeding as a complication following tonsillectomy. Specifically, children over the age of 9 are found to be at a 2.6 times greater risk for postoperative bleeding compared with those below the age of 9. This observation aligns with the outcomes of other related studies, reinforcing the significance of age as a critical determinant in the risk assessment for hemorrhagic complications in pediatric tonsillectomy patients.19,20 The possible causes are as follows: the tonsils of older patients develop fibrosis after repeated episodes of inflammation, lack of clear boundary of adhesion with surrounding tissues, larger wound in the process of surgical separation, unwillingness to swallow and gargle and eat less after operation.21,22 Poor oral hygiene increases the susceptibility to infections, which can result in delayed wound healing and, in some cases, lead to bleeding. Some older children have anatomical changes such as obesity, narrow pharyngeal cavity, hypertrophy of tongue root, shortening of mandible, protruding upper incisors, and short neck, and the inferior pole of tonsil is often poorly exposed. It is more challenging to avoid damage to the root of the tongue and the pharyngeal constrictor muscles in children, as indicated by studies.23-25 In addition, older patients typically require larger tracheal intubation tubes, which can limit the operational space. 26 Consequently, for older children, a heightened level of vigilance is necessary to prevent the occurrence of postoperative bleeding.
The primary indication for tonsillectomy in children is tonsillar hypertrophy, which can impair respiration and lead to the development of obstructive sleep apnea syndrome. In addition, it can result in recurrent and acute episodes of chronic tonsillitis.27,28 In theory, physiologically hypertrophic tonsil adheres slightly to the surrounding tissue and is easy to peel off, bleed less, and stop bleeding quickly. 29 Inflammatory tonsil adheres closely to the surrounding tissue due to repeated inflammatory stimulation, and it is difficult to separate and bleed easily. 30 Some studies31-33 have clearly pointed out that chronic inflammation is a risk factor for postoperative bleeding. In this study, the sample size of the chronic tonsillitis group is small and cannot be analyzed, which needs further investigations in the future.
Since the introduction of low-temperature plasma technology in tonsillectomy, the procedure of partial tonsillectomy has become feasible.34,35 In the case of children with simple tonsillar hypertrophy, partial tonsillectomy is an option that retains the tonsillar capsule and a portion of the tonsillar tissue. This approach aims to preserve as much of the children’s tonsillar immune function as possible.20,36 Different surgical methods have an effect on postoperative bleeding, and the incidence of postoperative bleeding in children with total tonsillectomy is higher, which may be related to the scope of operation and the content of resection. Tonsil capsule is like a cover membrane to protect deep blood vessels and nerves. 37 Tonsillar capsule is retained during the operation, which does not damage the peritonsillar space and reduces the incidence of bleeding. In this study, it has been found that the type of surgery and degree of tonsil embedding are related to secondary bleeding after tonsillectomy. Therefore, for children with simple tonsillar hypertrophy, partial tonsillectomy may be preferentially performed, which can not only reduce the probability of postoperative bleeding but also preserve the immune function of tonsil as much as possible. For children who undergo total tonsillectomy and those with deep tonsillar entrapment identified intraoperatively, it is recommended to extend their hospital stay to allow for thorough observation. Parents should be educated on the postdischarge care and the importance of adhering to specific guidelines to minimize the risk of postoperative bleeding. This includes providing clear instructions regarding the child’s diet and activities, emphasizing the critical aspects that require attention after discharge. By doing so, the likelihood of secondary hemorrhagic events can be significantly reduced, ensuring the safety and well-being of the child during their recovery period.38,39
There are some shortcomings in this study that are worth considering. First of all, the sample size of the children with hemorrhage in this study is small, which may be difficult to produce effective statistical significance for some related factors. Second, this study uses a retrospective design, which inherently limits the scope of factors that can be analyzed and included. Consequently, there may be additional variables influencing postoperative bleeding in children that were not accounted for. It is important to note that retrospective studies are positioned at a lower tier in the hierarchy of scientific evidence. Moving forward, it will be essential to enlarge the sample size and incorporate a broader spectrum of relevant factors that could potentially impact bleeding in pediatric patients. This expanded approach will enhance the reliability of this study’s findings and offer more robust guidance for the management and nursing care of children post-tonsillectomy.
Conclusions
In summary, this study has found that the incidence of secondary bleeding after tonsillectomy is 4.87%, and age, type of surgery, and degree of tonsil embedding are associated with the occurrence of secondary bleeding in children with tonsillectomy. Clinicians and nursing staff should pay close attention to children with identified risk factors. It is crucial to maintain a high index of suspicion, promptly recognizing and evaluating any signs of bleeding in a timely manner. This proactive approach can significantly reduce the incidence of postoperative hemorrhage and enhance the overall prognosis for these children. By implementing vigilant monitoring and early intervention strategies, health care professionals can optimize children’s outcomes and contribute to a safer recovery process following tonsillectomy.
Author Contributions
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval and Consent to Participate
In this study, all methods were performed in accordance with the relevant guidelines and regulations. The study has been reviewed and approved by Ethics Committee of the Children’s Hospital of Nanjing Medical University (Approval Number: 202208162-1). And written informed consents had been obtained from all the included children and their patents.
Data Availability Statement
All data generated or analyzed during this study are included in this published article.