
Abstract
Educational Objectives
To summarize the qualitative impact of the 2022 infant formula shortage on providers, WIC staff and families in Oregon and evaluate the response by providers and WIC with attention to interprofessional collaboration.
To highlight the need for improved communication between WIC and medical providers, to be addressed in both pediatric resident training and in clinical practice.
Introduction
A national infant formula shortage began in the United States in February 2022. This shortage was the culmination of several factors, including a recall and halt of supply production by Abbott Nutrition that exacerbated pandemic-related supply chain issues, and resulted in access challenges for families across the country. 1 Millions of U.S. families rely on formula to feed their infants, toddlers, and children with complex medical needs. 2 In 2018, Women, Infants, and Children (WIC) infants consumed approximately 56% of formula in the United States. 3 Recent data show that an estimated 39% of infants in the country were served by the Special Supplemental Nutrition Program for WIC in 2022. 4 Both medical providers and WIC served as resource points for families experiencing the effects of the shortage. The roles of WIC and pediatricians and their interaction during this stressful time have not been examined; therefore, this study sought to address that gap in knowledge.
Methods
This study was completed with providers working in Oregon. The Institutional Review Board (IRB) approval for survey distribution and data analysis was granted from both affiliated institutions. Surveys were developed for physicians caring for infants (pediatricians and family practitioners) and WIC staff to examine shortage-related perceptions, impacts on families, and interprofessional communications. Cognitive interviews were conducted with a group of physicians to refine the survey questions. Survey participants were recruited via email listservs and newsletters to complete the survey online. Responses were anonymous and stored on the Qualtrics XM platform.
Qualitative analysis of the responses was performed using inductive methods. Three independent investigators analyzed de-identified survey responses. Women, Infants, and Children staff and physician responses were reviewed independently initially to identify repeating concepts. These concepts were shared between investigators and grouped into themes and subthemes. Demonstrative quotes were identified for each subtheme.
Results
Our survey received 17 physician responses and 35 WIC staff responses. Physician responses were captured from 10 Oregon counties, of which 50% are designated as rural, and various practice sizes including small clinics (4-5 physicians), an academic center, and large medical groups (100+ physicians). Women, Infants, and Children staff responses represented 18 Oregon counties, of which 70% are designated as rural (Figure 1). Among WIC staff respondents, most were certifiers, coordinators, or dietitians.
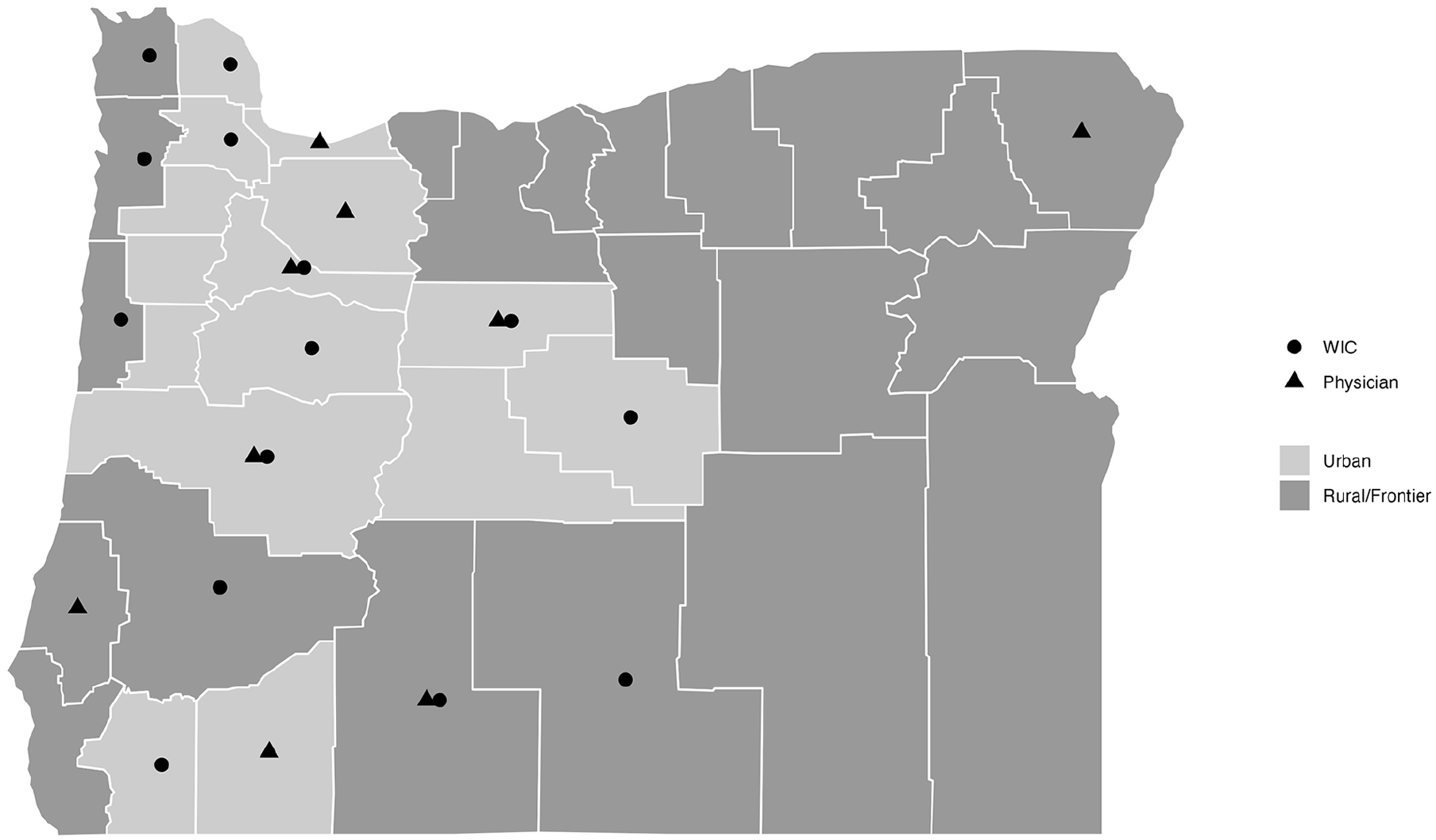
Practice locations of physician and WIC respondents demonstrating representation of both urban and rural practitioners.
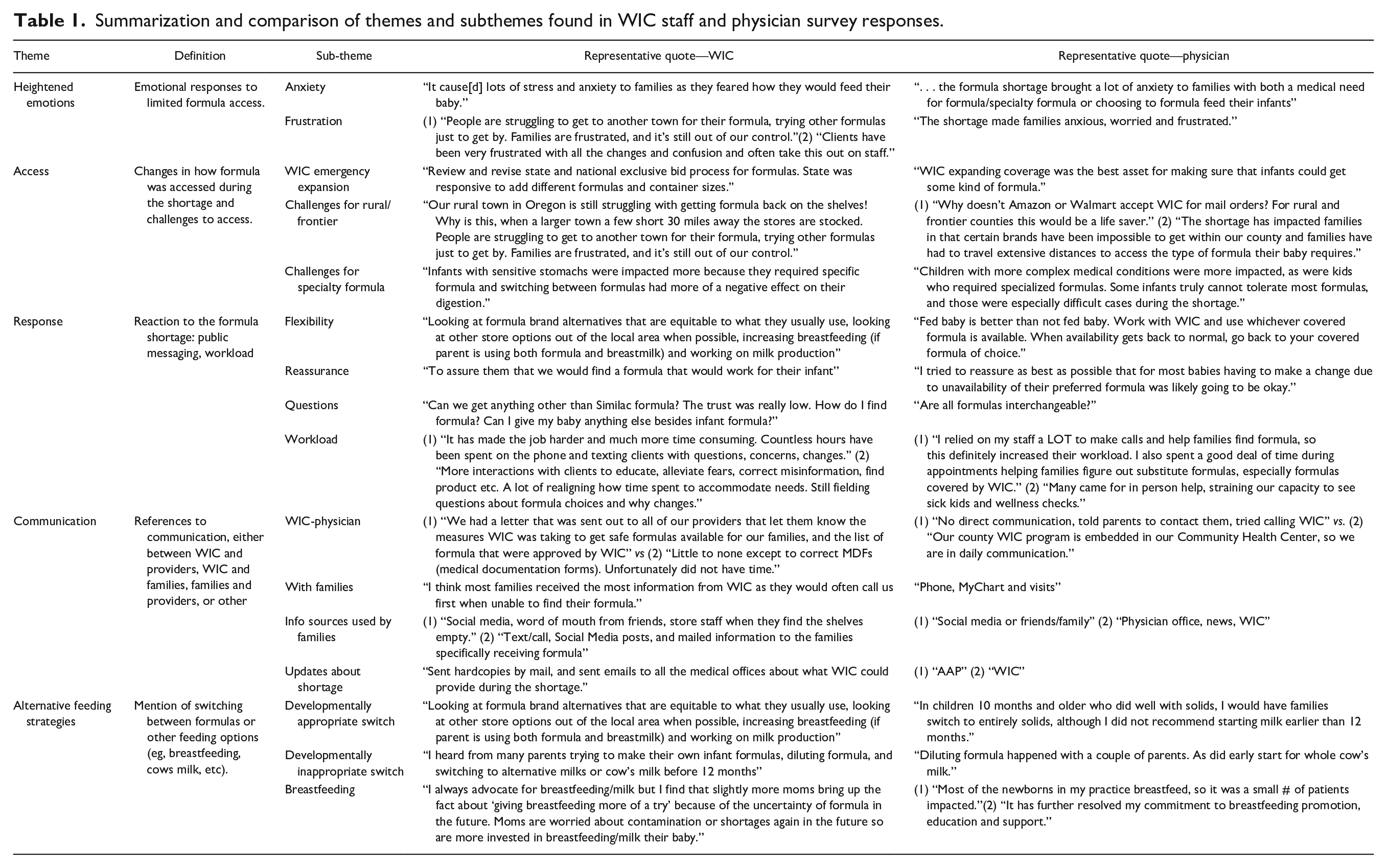
On review of responses, 5 themes were identified, with corresponding sub-themes to capture further nuance: heightened emotions (anxiety, frustration), access (WIC emergency expansion, challenges for rural/frontier populations, challenges for specialty formula), response/actions (flexibility, reassurance, questions, workload), communication (WIC-physician, with families, information sources used by families, updates about shortage), and alternative feeding strategies (developmentally appropriate, developmentally inappropriate, breastfeeding) (Table 1). There were similar themes and subthemes between the physicians and WIC staff, demonstrated by representative quotes for each. However, there were notable differences in the impact of the shortage on workload and communication between the 2 groups. Women, Infants, and Children staff experienced a greatly increased workload given that most of their families were impacted by the formula shortage, while physicians shared the increased workload across multidisciplinary staff. In most Oregon counties, there was unidirectional communication about the shortage from WIC to patients and medical groups. While most WIC staff reported that their office had put out formal communications to their families about the formula shortage, less than a quarter of physicians reported that their office had put out such communications.
Summarization and comparison of themes and subthemes found in WIC staff and physician survey responses.
Discussion
Our study demonstrates the effects of the national infant formula shortage on families and reveals some of the differential impacts felt by WIC and medical providers in supporting families. The disproportional burden of information sharing from WIC highlights the lack of robust communication pathways between WIC and clinicians. The American Academy of Pediatrics asserts that pediatricians should work collaboratively with state and local WIC agencies. 5 The Accreditation Council for Graduate Medical Education states that pediatrics residents must demonstrate an understanding of the complexity of health systems and be able to coordinate care “across the healthcare continuum.” 6 To improve collaboration with WIC and facilitate coordinated care, the ACGME could incorporate a required competency regarding WIC services by the conclusion of a pediatrics residency. Recent studies have highlighted how WIC-enrolled families may have used more effective strategies in navigating the shortage and that these individuals benefited from the flexible strategies employed by WIC, strategies which could have been shared with non-WIC families with improved physician-WIC communication.7,8 Strategies such as increasing physician competency around WIC, co-locating WIC and medical offices, and aligning messaging between the 2 spheres may help to reduce the anxiety and frustration felt by families, WIC staff, and medical providers should similar crises emerge in the future. Furthermore, improved communication and cooperation between WIC and medical providers would likely facilitate streamlined coordination of care even outside times of crisis and be beneficial to daily clinical care.
Author Contributions
All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Footnotes
Acknowledgements
The authors would like to acknowledge the support of the Oregon Rural Practice-based Research Network and the Oregon Pediatric Society in disseminating our survey to medical providers in Oregon. Thank you to the anonymous physicians and WIC staff who completed our survey and shared their experiences.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding support was provided by Doernbecher Philanthropy Board.