
Abstract
We conducted a cross-sectional survey of complex care programs on behavioral health services provided to children with medical complexity (CMC). Quantitative and qualitative data were analyzed by using convergent mixed methods. Rates of CMC receiving behavioral health services were at or above national averages for the general pediatric population and the most reported concerns were externalizing behaviors. Of 25 programs, 7 (28%) reported integrated care and programs with integrated care found the service improved access and were more likely to screen for caregivers’ mental health. Themes included: 1. Current models of care for pediatric mental and behavioral health limits access for CMC; 2. Collaboration is highly desired by medical teams; 3. Providing mental health for family members of CMC is important. Despite high service use and frequent availability of integrated care, complex care programs still report insufficient access to behavioral health services required to meet the needs of CMC.
Keywords
Introduction
Integrated mental and behavioral health is a collaborative model of multidisciplinary care provided by both medical and behavioral health providers in conjunction with patients for whole person care. 1 It has been shown to improve behavioral health service access and outcomes for the child population.2-4 It has been promoted by national and international pediatric organizations as a solution for unmet mental health needs and incorporated into recommendations for pediatric medical homes.5,6 However it is not universally available. Prior reports show 35% of primary care pediatric offices in the United States have co-located behavioral health providers, behavioral health providers in same space as medical providers, while only 13% reported fully integrated behavioral health services with only a slight increase in prevalence over the past decade.7-9 Barriers to implementation vary, and include increased costs, service reimbursement, provider and organizational capacity, and competing clinical needs of persons with chronic medical conditions or who are part of vulnerable populations.10,11
Children with medical complexity (CMC), who are children with complex chronic medical conditions causing functional impairment and high health care utilization, have more unmet mental health care needs than non-complex peers.12-14 They are a heterogeneous population, comprising of 1% children, with medical conditions impacting multiple organ systems resulting in developmental delays or disabilities and dependent on medical technology.15,16 Their unmet mental and behavioral health needs are likely multifactorial due to the interaction of their medical conditions, developmental differences, and medical treatments, although this is not well understood. 15
Recent literature shows CMC have higher rates and different mental and behavioral health (MBH) diagnoses than children without complex conditions. 15 Children with complex chronic conditions also report high rates of specialized MBH care which is harder to access. 17 These factors likely contribute to the high unmet MBH care need for CMC. Integrated behavioral health services for CMC could be an efficient way to meet this unmet need especially as mental health concerns are the most common reason for an outpatient visit in CMC. 18
While integration of MBH in primary care and care of CMC both have had increasing attention, this intersection of integrated MBH care for CMC has not been as well described. One area where this intersection occurs is in outpatient complex care programs. Complex care programs (CCPs) are specialized care settings, typically affiliated with academic medical centers, developed in response to the unique and unmet needs of CMC; they have been shown to improve care for their patients.19-22 Complex care programs vary in structure and services offered, but have a common goal of improving health outcomes and access to care through care coordination. Complex care programs often serve as the medical home for a child with medical complexity but because of the small size and limited number of CCPs, a small proportion of CMC attend such programs.20,23,24 Complex care programs can reduce unmet mental health needs of CMC enrolled, though 1 study reported considerable remaining unmet needs for MBH services (42.5%) after enrolling in a CCP. 14
This study was designed to assess the need for mental and behavioral health (MBH) care for CMC as perceived by complex care program (CCP) leaders, to document MBH screening and services in CCPs, and to understand how medical care and MBH currently are integrated among a national sample of pediatric outpatient CCPs.
Methods
Survey Design
This study was a convergent mixed-methods, cross-sectional survey of outpatient complex care programs in the United States. The survey was developed jointly by all authors who are members of the Mental and Behavioral Health Workgroup of the Children and Youth with Special Health Care Network (CYSHCNet), a national research network based primarily at large children’s hospitals. 25 The workgroup was a multidisciplinary team representing multiple academic centers and parent partners with lived experience caring for a CMC. The parent partners provided insight into how families perceive MBH integration and input to develop survey questions that are relevant to families on how MBH services are provided.
The survey consisted of 15 primary questions and 54 additional questions within branching logic that were categorical or open-ended responses developed by the workgroup in response to gaps in knowledge identified as part of the CYSHCNet research agenda. 26 The survey elicited descriptions of program characteristics including estimated MBH needs of the patients served, information about the extent of MBH integration based on location of services, and services provided by the complex care programs’ staff themselves such as MBH screening and referrals. Descriptions of integration used the SAMHSA-HRSA CIHS’s Standard Framework for Levels of Integrated Healthcare. 1 The levels emphasized service locations and included having an MBH provider located in either shared clinic space, same building (but not in shared clinic space), same healthcare system, and external settings to which referrals are made (eg, community, schools, other healthcare institutions). The series of questions asked about access, communication, diagnostic services, treatment, referral, and coordination at each location. These survey items were descriptive in nature, with sites denoting whether they had access to these professionals.
A pilot survey was completed by 10 complex care providers of different disciplines who, while practicing in complex care programs, would not be the respondent in the final survey. Cognitive interviewing methods were used with select members of the pilot group after they completed the survey to enhance construct validity of survey items. 27 The study was approved by the institutional review board at the University of Colorado. The Checklist for Reporting of Survey Studies was followed during data analysis and writing of the manuscript; the checklist was not published during the periods of the survey design and administration. 28
Sampling Methods
The target population was pediatric outpatient complex care programs in the United States. In the absence of national standards or certification for pediatric complex care programs, CCPs are self-identified and vary in their structure and services. An accurate count of their number is not available, so the survey sampling frame included all members of CYSHCNet and other known outpatient programs identified from conversations on the Complex Care listserv. 29 The listserv is one of the oldest and largest pediatric complex care interest groups; it has been in existence since 2010 and has more than 1000 members. Invitations to participate in the study were made to complex care program leaders in the sample for which an email address was available; there were 50 programs identified by this method. The survey asked potential respondents to self-exclude if they did not have an outpatient service (ie, only provided inpatient consultation) or if the program focused on specific medical problems or organ systems (ie, programs for children with cerebral palsy or a rehabilitation program); the programs could have a range of outpatient service delivery models such as primary care, consultative care, or a mix.
Survey Administration
A web-based survey was sent via email to 50 programs, each email containing a unique link. The survey was carried out in July to August 2021; 2 email reminders were sent to the non-responding programs. The survey was sent to the designated contact for CYSHCNet sites and to the active member on the listserv for other sites, usually the medical director. The survey was completed by the program leader or another knowledgeable staff member at that site. Only 1 response from each program was accepted; if more than 1 response per program was submitted, the program respondents were contacted by email to verify which response was to be used. The survey was brief, taking 15 minutes to answer during pilot testing. Respondents were offered early access to survey results as an incentive for completion of the survey. Responses were confidential but not anonymous for tracking purposes. Surveys were sent and data stored in Qualtrics. 30
Statistical Analysis
Descriptive statistics were performed for responses to quantitative questions describing programs, screening patterns, and levels of MBH integration. For questions using ranking, weighted scores were used to determine the top 3 results. Fisher’s exact tests were used to identify significant associations between having a co-located behavioral health provider and specific outcomes such as MBH screening rates; this metric was of particular interest, as typical screening tools have not been developed for CMC, and having a co-located behavioral health provider has shown to improve screening in general pediatric populations. 31 All analysis was conducted using Stata. 32 A statistical significance level of P < .05 was used for all analysis.
Qualitative, open-response survey items were de-identified (ie, hospital, city/state, and program names were redacted), coded, themes analyzed, and quotations extracted using qualitative thematic analysis methods. Dedoose was used for data coding and analysis. 33 After quantitative and qualitative data were analyzed independently, data were integrated and analyzed as per established convergent mixed-methods techniques. 34 The parent partners provided interpretation of data from the lens of families and caregivers during the analysis.
Results
All CYSHCNet sites (n = 13, 1 member site has 2 CCPs) and 14 additional programs responded (Figure 1) for a 54% response rate. All respondents were at academic medical centers. Data from 2 programs were removed from analysis due to respondents completing less than 50% of the survey. A total of 25 programs’ data were used in the analysis. The respondents were program medical directors (68%, n = 17), other medical providers (24%, n = 6), and behavioral health providers (8%, n = 2). Programs varied in size from serving <250 patients to >1000 patients (Figure 2).
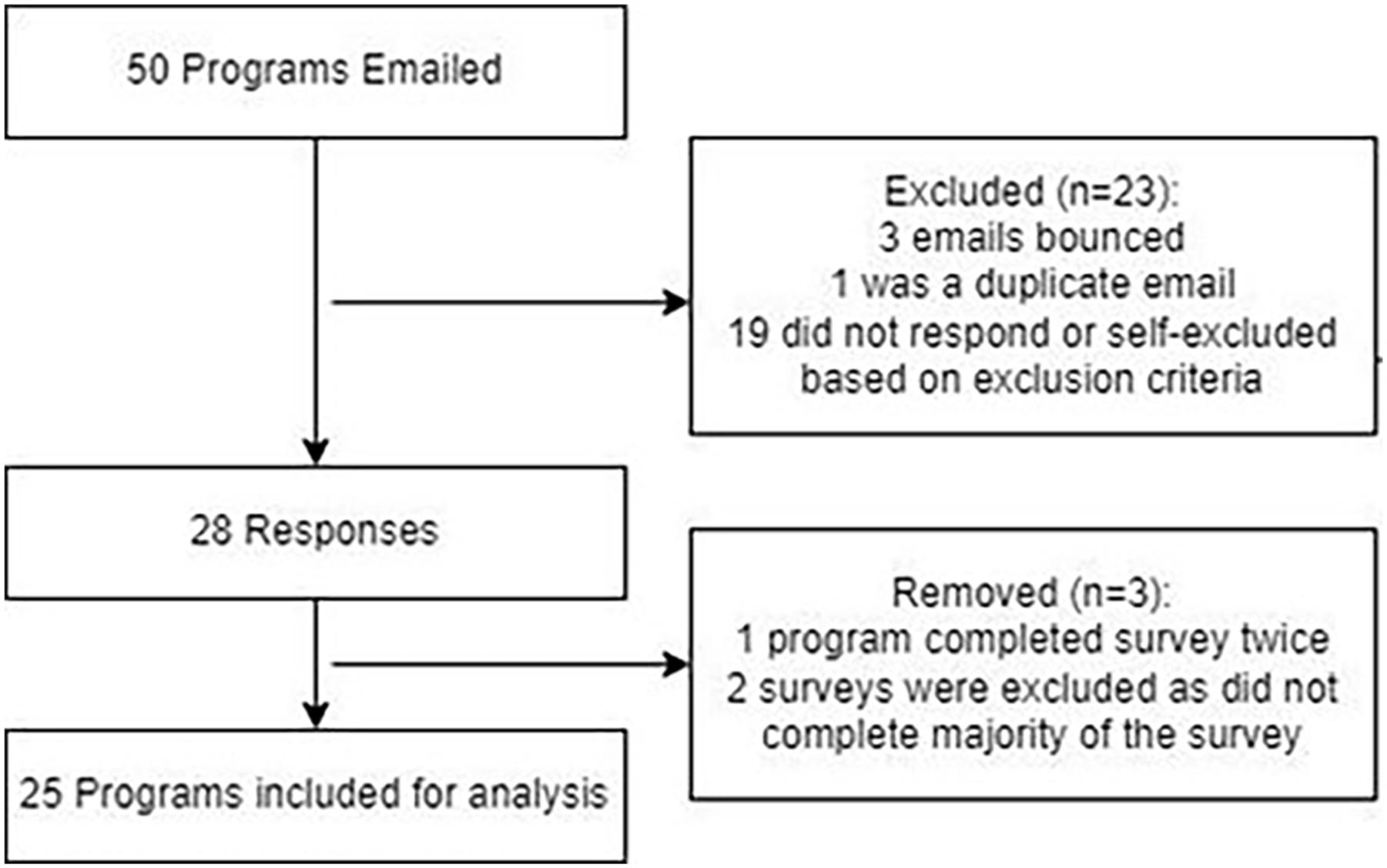
Flow diagram of survey respondents.
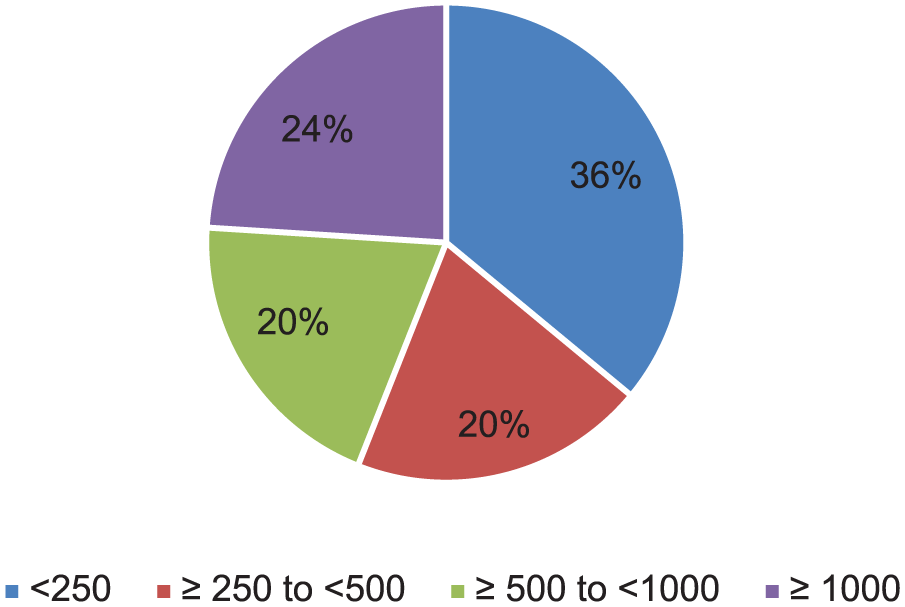
Program size of responding CCPs described by number of patients served.
Most programs (88%, n = 22) reported that 10% or more of their patients receive MBH services. Complex care providers reported that the top 3 MBH concerns seen were disruptive behavior (ie, tantrums), anxiety, and self-injurious behavior (ie, head banging) making externalizing behaviors the most common concern.
Mental and Behavioral Health Provider Availability
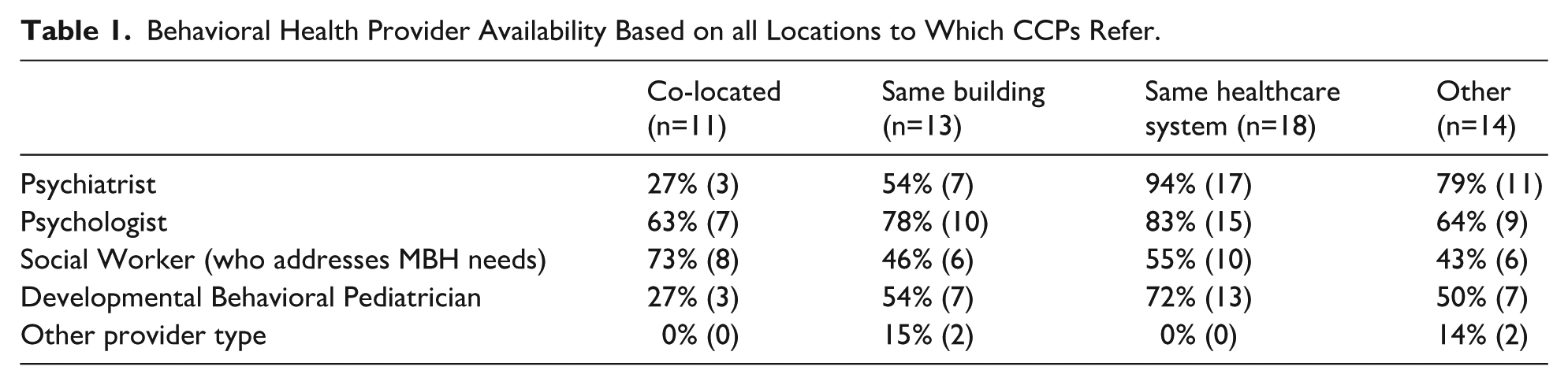
Forty-four percent (n = 11) of programs reported having a behavioral health provider located in the same clinic space. Social workers were the most frequently identified co-located behavioral health provider (73%, n = 8). Further details of provider availability are in Table 1.
Behavioral Health Provider Availability Based on all Locations to Which CCPs Refer.
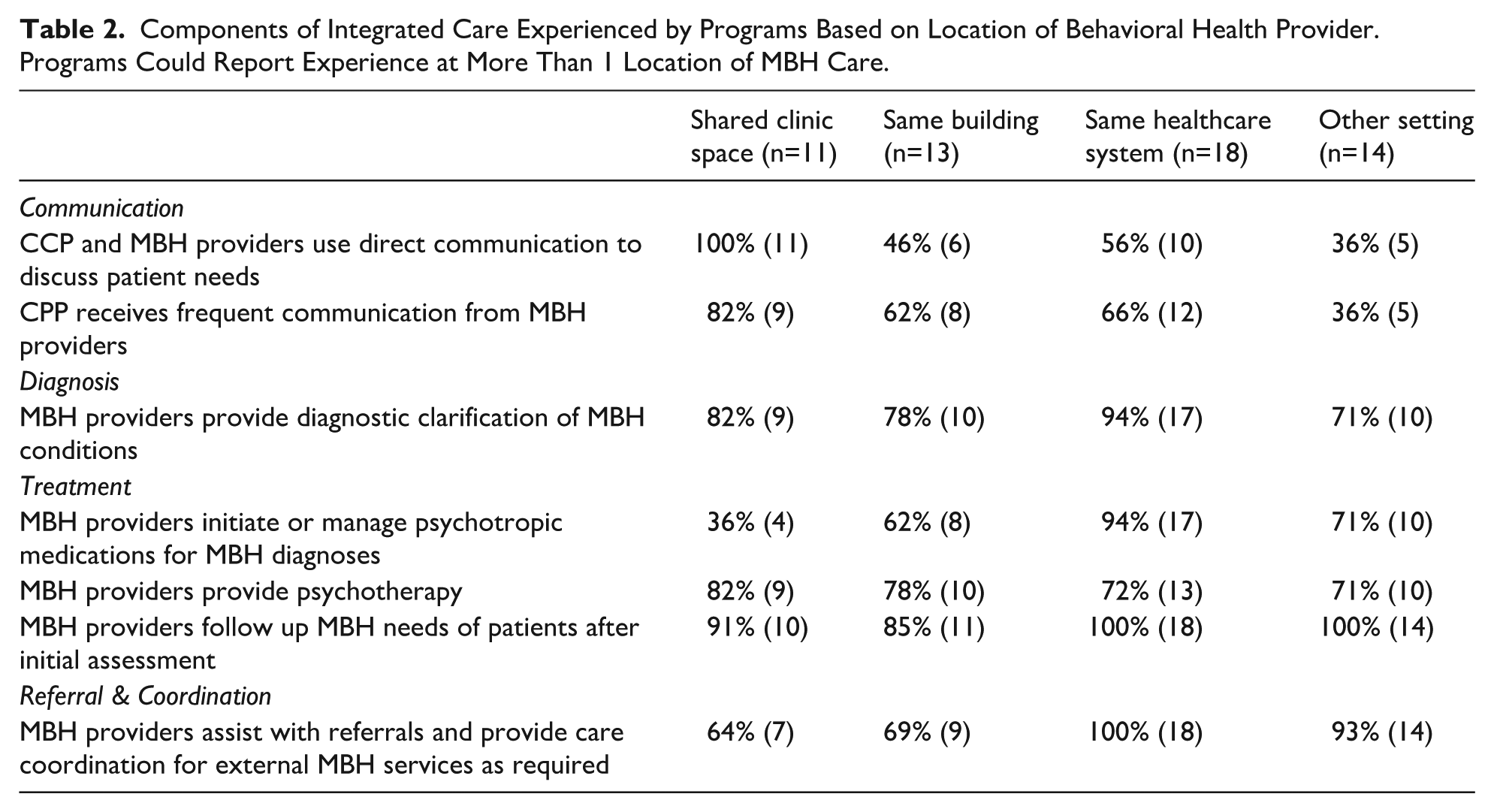
Of the programs with MBH in shared clinical space, 64% (n = 7) had a behavioral health provider accessible at the time of the medical appointment. More than half (n = 6) of programs with a behavioral health provider in a shared clinic space had a provider available every day. Other components of integration are reported in Table 2.
Components of Integrated Care Experienced by Programs Based on Location of Behavioral Health Provider. Programs Could Report Experience at More Than 1 Location of MBH Care.
Mental and Behavioral Health Services Offered
Sixty-eight percent (n = 17) of programs did not report screening for MBH in patients and 64% (n = 16) did not report screening families for mental health concerns such as depression or anxiety. Compared with programs without a co-located behavioral health provider, programs with a co-located behavioral health provider were more likely to screen families for mental health concerns (64% vs 14%, P = .02). Having a co-located behavioral health provider made it more likely that CMC were screened for MBH concerns though this did not reach significance (55% vs 14%, P = .08).
Eighty percent (n = 20) of programs reported that they could address caregiver mental health concerns, primarily through referrals for mental health services. There was no evidence that addressing caregiver mental health concerns differed by having a co-located behavioral health provider (91% vs 71%, P = .34).
Barriers to Mental and Behavioral Health Care
Programs reported the top 3 barriers to accessing MBH care were: 1. limited experience and expertise addressing patients’ specific MBH needs in the context of their medical complexity; 2. lack of insurance coverage for MBH services; and 3. insufficient time on the part of either the patient/family or the provider.
Qualitative Responses
Of the 25 respondents, 21 provided free text responses describing MBH services provided at each location referred to by CCPs as well as what they would like to improve about MBH services. The responses clustered into the following 3 themes: (1) Current models of care for pediatric MBH limit access for CMC; (2) Collaboration is highly desired by medical teams; and (3) Providing mental health services for family members of CMC is important to CCPs. These themes and associated quotes are illustrated further by representative quotes in Table 3.
Qualitative Themes Developed From Free-Text Responses (With Respondent ID Next to Quote).
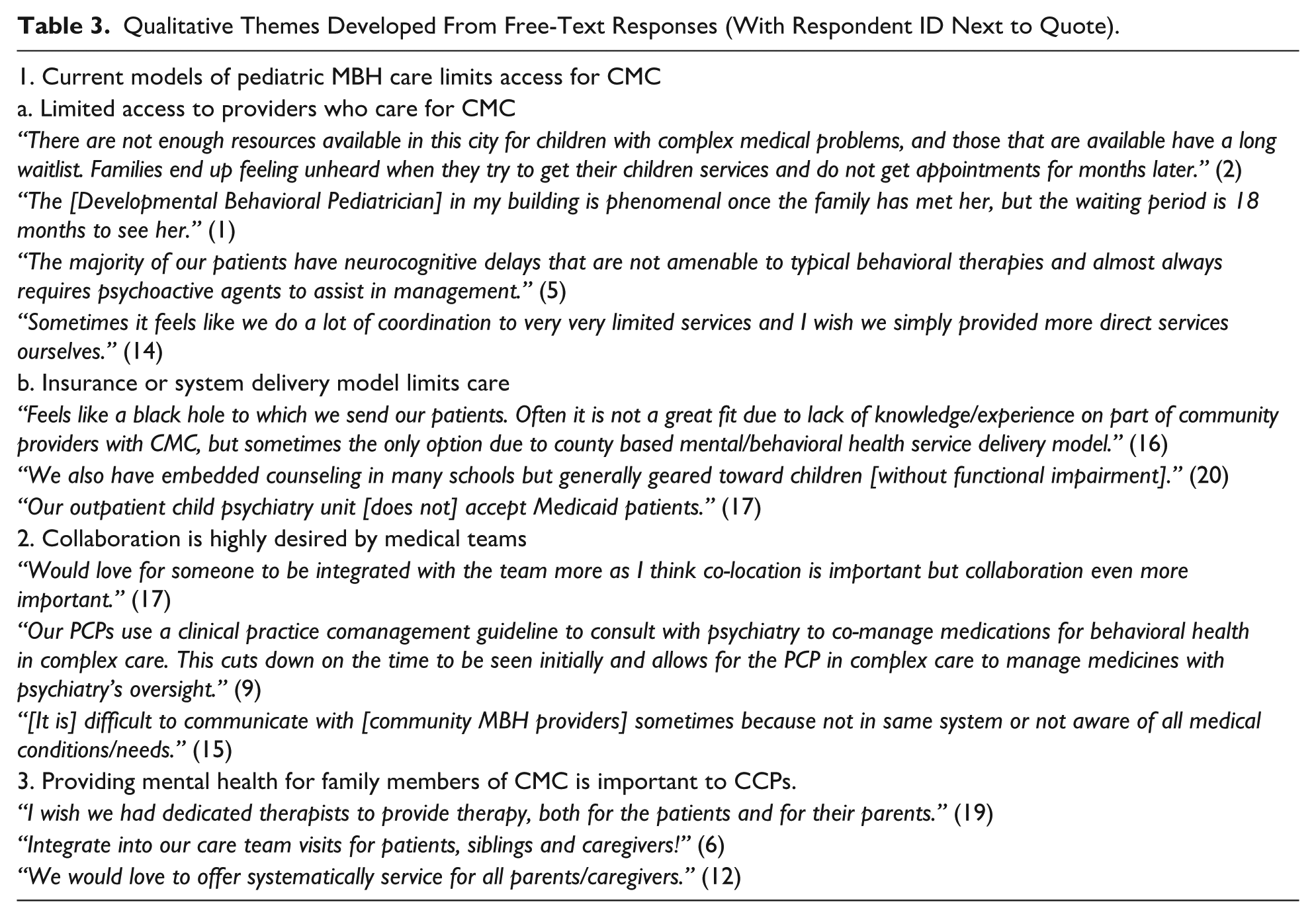
Respondents described multiple factors that limit access to pediatric MBH for CMCs. These factors included limited access to behavioral health providers who cared for CMC (long wait lists, not enough providers), typical care options did not fit the needs of CMC, and behavioral health providers being unwilling to provide care for CMC (including integrated/co-located providers). This latter statement is best represented by 1 respondent: “We have an MBH provider within our primary care clinic space but she really doesn’t see patients with medical complexity so it is not helpful to my patients.” Respondents reported sometimes using atypical behavioral health providers, such as neurologists, to address patients’ MBH needs. In addition, inadequate MBH delivery models (such as county-based MBH services, school-based MBH services, and limited availability of specialized MBH required for this population) and limited insurance benefits were reported barriers.
Three CCPs reported that having integrated MBH care was a facilitator to access. These 3 programs were independent CCPs not housed within a larger general pediatric primary care practice. “[Primary Care Providers] in our clinic can identify MBH service needed within the consult and will inform the MBH provider to determine whether they can see the patient within the same appointment, rather than rescheduling for another day” represents the success of integrated MBH specific for CMCs into CCPs.
Discussion
Our study found that the proportion of patients seen within our sample of complex care programs who receive mental and behavioral health care is equal to or higher than reported national pediatric rates, yet substantial unmet needs for MBH services persist even within these specialized programs due to unique considerations in MBH care of CMC. This is the first study to describe the factors contributing to persistent unmet MBH needs of CMC despite high access to services.
Most CCPs in our sample reported that 10% or more of their patients use any behavioral health services. This is higher than the 9.6-10.1% of the general pediatric population which receives behavioral health services and is in agreement with prior literature reporting higher use of behavioral health services by CMC.35-37 Despite this level of service use, respondents still expressed unmet MBH needs and identified barriers to care specific to their patients having medical complexity. Respondents identified integrated, collaborative behavioral health providers as a potential solution to this unmet need. Three programs reported success in meeting the needs of CMC with this model.
Externalizing behavioral problems and anxiety were the most common MBH needs seen by CCPs contrasting with attention deficit hyperactivity disorder and anxiety which are the most frequent MBH diagnoses in the general pediatric population. 29 One study looking at mental health diagnoses in CMC reported stress and trauma were the most common diagnoses, with anxiety and disruptive disorders high in prevalence as well. 15 While our survey asked about trauma, it was not ranked as a common diagnosis. This may be in part due to differences between concerns voiced by CMC and families who attend a CCP as compared with diagnoses from claims data, or differences between concerns of CMC who attend a CCP compared with those who do not. More importantly, our study agrees with prior literature that MBH needs in CMC are different than the general pediatric population which could lead to unmet need. In addition, children in the general population with behavioral disorders are less likely to receive treatment than other mental health disorders, which could be another reason for unmet needs among CMC which report high rates of behavior disorders.35,38
Our respondents reported the largest barrier to appropriate MBH care was finding a provider able to address MBH needs that occur together with complex medical conditions. Programs report access was often limited by insurance, but this was not the only factor. Some respondents reported barriers to care due to MBH providers unwilling to see CMC, even when behavioral health providers were co-located or integrated. Forty-four percent of the CCPs in our study reported having a co-located behavioral health provider and 28% reported having an integrated behavioral health provider. 7 The most common co-located provider was a social worker. Mental and behavioral health services provided by a psychologist or psychiatrist within a CCP were less common than in other settings. Importantly, integrated providers without experience or education on the needs of CMC were not supportive in meeting the MBH needs of CMC. Our findings shed light on the substantial unmet MBH need of CMC, even within specialized complex care programs, and agree with reports that unmet needs of CMC are often due to the complexity of their care.13,14 Further understanding on behavioral health provider education and other supports including to address MBH needs of CMC is critical to filling this unmet need.
Complex care programs with integrated MBH care specifically for CMC reported easier access to MBH services. This was likely facilitated by bi-directional communication between behavioral health and medical clinicians that consider the interaction between the child’s complex medical needs and their unique MBH concerns. Direct and frequent provider-to-provider communication was reported more often with a co-located behavioral health provider. Respondents desired integrated and collaborative care even more than just co-located care. Understanding factors that facilitate collaboration, in addition to having integrated behavioral health providers who are specifically able to address the MBH needs of CMC, is critical to develop this high-quality model of care.
There is growing evidence that parents and other caregivers of CMC have poor mental health compared with peers.39-41 Having a co-located MBH provider made it more likely that caregivers were screened for mental health concerns in our study. More importantly, 80% of programs reported being able to help caregivers with mental health concerns; being able to assist family and caregivers regardless of co-located mental health provider status implies that CCPs are recognizing the importance of caregiver mental health to their patient’s wellbeing. Though family and caregiver MBH support was largely addressed through referrals and not through direct MBH care in the CCPs, respondents recognized that direct care would be preferable and that it was a service they would like to include in their clinics. Prior studies support that CCPs reduce unmet family mental health needs. 14 Models able to adequately support mental and behavioral health of the whole family of a child with medical complexity could impact whole family wellbeing.
Limitations
Our sample, made necessary by the lack of a complete available list of CCPs, and resulting small sample size made statistical inferences difficult and limited the power to show important differences during our analysis. The sample size was sufficient to reach thematic saturation in our qualitative analysis. Our response rate was in no doubt affected by us asking programs to self-exclude. Based on a review of programs who did not respond to the survey, at least 7 were specialty or inpatient CCPs.
In addition, our results are reflective of the MBH needs of CMC receiving care through CCPs at academic medical centers. Integrating MBH has been reported as more successful in larger practices with more resources, such as academic medical centers.9,42 Therefore, our data should only represent the access to integrated MBH for CMC receiving care through CCPs and not CMC generally. We did not take into consideration the perceptions of patients or their families on MBH care through CCPs; the experience of patients and their families is being investigated by this workgroup in another study.
Conclusion
Children with medical complexity cared for by complex care programs continue to experience multiple barriers to mental and behavioral health care despite greater rates of MBH service use and access to integrated behavioral health providers than the general pediatric population. The unmet MBH needs of CMC are impacted by multiple factors including the unique MBH problems created by their medical conditions, the difficulty identifying mental health professionals willing or able to care for this population of children and their families, insurance limitations, and the caregiving challenges caring for CMC create. Integrating behavioral health providers with experience caring for CMC into CCPs represents 1 way to address MBH access and increase mental health screening rates for caregivers of CMC.
Author Contributions
All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Footnotes
Ethical Considerations
Our study received an exempt status by the Colorado Multiple Institutional Review Board June 2021 with continuous renewal.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project is supported by the Health Resources and Services Administration (HRSA) of the U.S. Department of Health and Human Services (HHS) under UA6MC31101 Children with Special Health Care Needs Research Network. This information or content and conclusions are those of the author and should not be construed as the official position or policy of, nor should any endorsements be inferred by HRSA, HHS, or the U.S. Government.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Survey response data are available on request to the corresponding author.