
Abstract

Educational Objectives
Discuss the importance of early recognition and intervention in preventing irreversible neurological and cardiac damage in pediatric patients with severe malnutrition.
Identify challenges to diagnosis and management of nutritional deficiencies in pediatric patients with developmental delays.
Case Report
A 5-year-old nonverbal, ambulatory boy with autism presented to the emergency department with progressive weakness, lethargy, and acute inability to ambulate. On presentation his neurological examination revealed diffuse peripheral hypotonia and profound weakness resulting in challenges with self-care, mobility, and ambulation. He was noted to have profound gross motor regression.
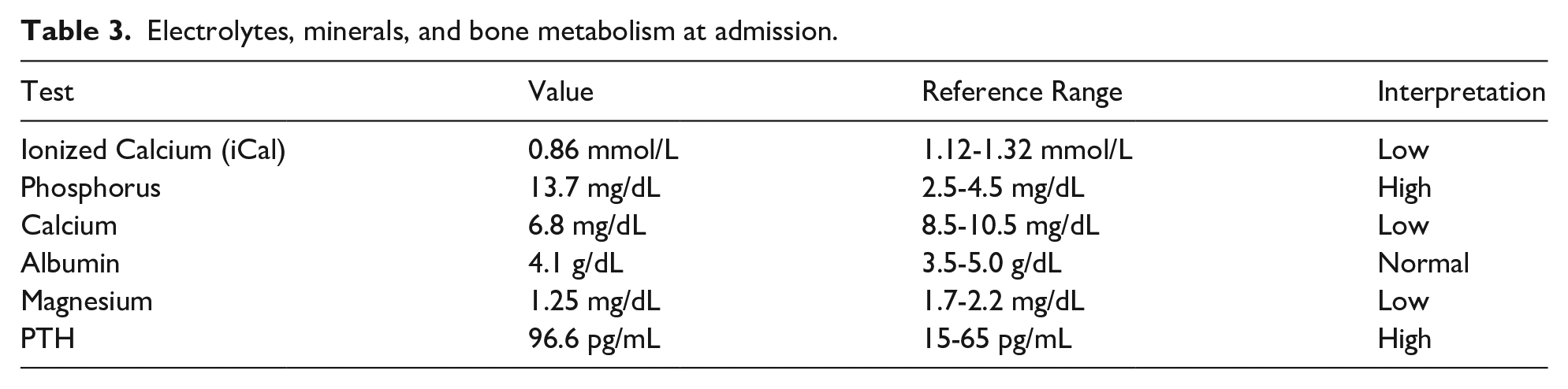
Upon admission to the regular nursing unit, he was noted to be severely malnourished (weight 11 kg, percentile <0.01%, Z = –5.20). He was tachycardic and tachypneic, with a heart rate of 145 beats per minute and a respiratory rate of 57 breaths per minute. He was febrile with a temperature of 38.0°C. His blood pressure was elevated at 106/74 and his oxygen saturation was 100% on room air. His neurological examination revealed an awake and alert school aged boy, at his baseline mentation given his known speech delay and autism. All his cranial nerves were intact, and he was able to move both of his upper extremities equally and spontaneously without focal deficits. He had decreased tone in both of his lower extremities and profound lower extremity weakness bilaterally, with minimal movements of his lower extremities. His plantar reflexes were down-going and he was unable to ambulate. On admission, his cardiovascular examination revealed sinus tachycardia, no murmur, strong pulses with brisk capillary refill. His abdominal examination revealed ascites. He was noted to have several electrolyte deficiencies. He was hypocalcemic (total serum calcium level of 6.8 mg/dL and a low ionized calcium of 0.86 mmol/L [reference range: 1.12-1.32 mmol/L]), hyperphosphatemic (13.7 mg/dL [normal: 2.5-4.5 mg/dL]) and hypomagnesemic (1.25 mg/dL [normal: 1.7-2.2 mg/dL]) (Table 1).
Vitamin levels on initial admission.

Hospital Course
A nutritional history revealed a 23% weight loss in the preceding 20 months and an exclusive almond milk diet. The patient was started on Kate Farms formula via nasogastric (NG) tube and vitamin supplementation. He was carefully monitored for refeeding syndrome on the regular nursing unit.
The patient’s course was complicated by cardiogenic shock, and he was transferred to the intensive care unit for hypothermia, hypotension, and hypoxia (oxygen saturations 70%-80% on room air). He was intubated, placed on mechanical ventilation, and started on vasopressors (epinephrine, norepinephrine). Echocardiogram revealed moderate bi-ventricular dysfunction; requiring milrinone infusion. Ascites was confirmed via ultrasound, and empiric antibiotics (cefepime, metronidazole, vancomycin) were given for presumed sepsis. The patient was extubated after 2 days. A follow-up echocardiogram showed mild left ventricular dysfunction (ejection fraction of 45%) and hypokinetic posterior wall motion. Milrinone and vasopressors were weaned off, and the patient was transferred to a regular nursing unit, without oxygen supplementation, for continued monitoring and discharge planning.
On the regular nursing unit, he was monitored for refeeding syndrome and completed a 5-day course of prophylactic sodium-phosphorus supplementation. A repeat echocardiogram revealed an improved ejection fraction of 56%.
While admitted on the regular nursing floor, the patient experienced worsening bilateral lower extremity weakness resulting in flaccid paralysis of bilateral lower extremities. The pediatric neurology team was consulted and a magnetic resonance imaging (MRI) scan of his brain showed medial thalamic hyperintensities indicative of thiamine (vitamin B1) and pyridoxine (vitamin B6) deficiency given low serum level of 10.4 mmol/L (normal range 20-125 nmol/L). Nutritional assessment demonstrated deficiencies in several vitamins, including vitamin A (0.6 µmol/L), vitamin B6 (10.4 µg/L), and vitamin C (6 µmol/L). In contrast, vitamin D (25-OH) was within the normal range at 53 ng/mL (Table 3).
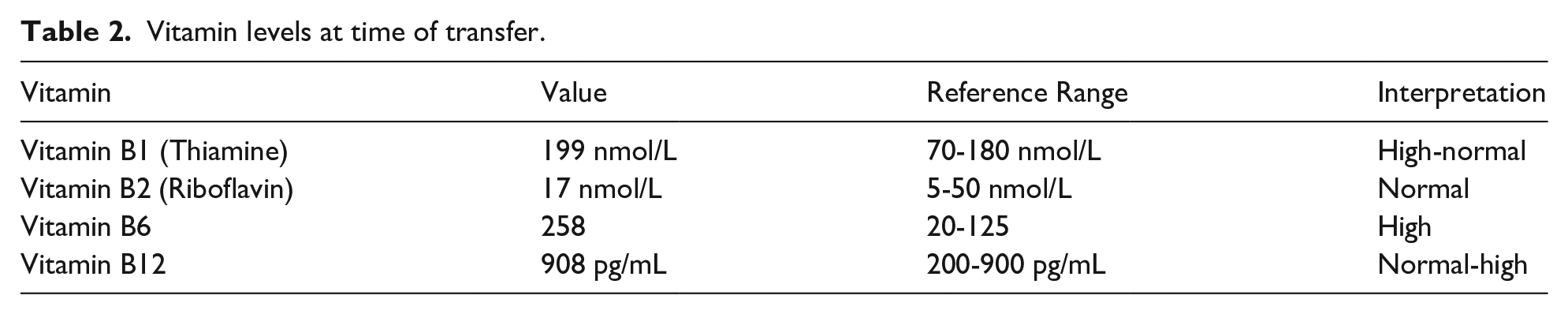
At that time, the patient was transferred to our hospital from another institution for a second opinion. He had been receiving daily supplementation with 50 mg of thiamine and 25 mg of pyridoxine, along with Kate Farms NG tube feeds. Upon arrival, laboratory studies demonstrated normal levels of thiamine (vitamin B1), pyridoxine (vitamin B6), riboflavin (vitamin B2), and vitamin B12 (Table 2). A multivitamin was initiated to treat his vitamin A and C deficiencies. The patient was evaluated by speech, occupational and physical therapy to address his sensory food aversion, hypotonia, and deconditioning. The patient’s treatment plan was complicated by aversion to broadening oral intake, the cost of formula supplementation, family’s initial discomfort with NG tube supplementation, and poor access to outpatient therapies near his home. His weakness and sensory food aversion steadily improved throughout his hospital stay. Ultimately, he transitioned to a standard pediatric formula with vitamin supplementation without a NG tube. By discharge, he was ambulating again.
Vitamin levels at time of transfer.
Electrolytes, minerals, and bone metabolism at admission.
Parental Consent Was Obtained to Publish This Case
Discussion of Case and Literature
Children with limited oral intake due to sensory food aversion are at risk for nutritional deficiencies, including vitamin deficiencies. Sensory food aversion refers to a child’s refusal to eat certain foods due to negative reactions to their taste, texture, smell, or appearance. This aversion often appears when new foods are introduced and can be associated with specific nutritional deficiencies or oral motor issues. Children with sensory food aversion generally show better eating behavior when offered preferred foods and may have other sensory sensitivities, such as discomfort with textures or environmental stimuli like lights and noises. 1
Autism spectrum disorder (ASD), as defined by the Diagnostic and Statistical Manual of Mental Illnesses 5 (DSM-5), is a neurodevelopmental disorder characterized by persistent deficits in social communication and interaction across multiple settings, along with restricted, repetitive patterns of behavior, interests, or activities such as sensory sensitivities or food aversions with symptoms present from early development and causing significant impairment in daily functioning. 2 This patient met the criteria for an autism diagnosis and had been diagnosed with it prior to this presentation. Sensory food aversion is commonly seen in children with autism, as in our patient whose diet was limited to almond milk.
Almond milk has minimal thiamine (0.005 mg/100 g) and pyridoxine (<0.001 mg/100 g). The World Health Organization (WHO) recommends 0.07 mg/d of thiamine for school age children, and the National Institute of Health (NIH) recommends 0.5 mg/d of pyridoxine. 3 The neurological and cardiac sequela of these deficiencies can be life-threatening and are reversible with early treatment. 3 Daily thiamine requirements can be met with intake of thiamine rich foods, including salmon, beans, nuts, oatmeal, and whole grain bread. Similarly daily pyridoxine requirements can be met by eating pyridoxine rich foods, including meats, potatoes, chickpeas, bananas, and avocados.3,4
Thiamine deficiency, or beriberi, may present with neurological symptoms, including peripheral neuropathy, muscle wasting, and confusion. In pediatric patients, beriberi may also present as irritability, vomiting, muscle weakness, tremors, and acute encephalopathy.3,5 Cardiovascular symptoms for thiamine deficiency may include cardiomegaly, dilated cardiomyopathy, and high- output cardiac failure.4,5
Pyridoxine deficiency may lead to peripheral neuropathy, seizures, and cognitive impairments. Pyridoxine is an essential nutrient used in the synthesis of neurotransmitters, including serotonin and dopamine, which are critical for cognitive function and mood regulation.4,6 Magnetic resonance imaging findings in pyridoxine deficiency-related encephalopathy have revealed characteristic findings such as symmetric thalamic hyperintensities.7,8 These findings underscore the importance of early diagnosis and intervention.
Thiamine deficiency has been reported in parts of West Africa, the Caribbean, the Middle East, South America and Central and Southeast Asia. Thiamine deficiency accounts for up to 45% of deaths in children below 5 years old in Cambodia and 34% of infant deaths in Laos for instance. In South American countries, thiamine deficiency has been reported among low-income populations, especially communities with limited access to diverse diets. In the Middle East, regions experiencing conflict or economic hardship report thiamine deficiency, particularly in refugee populations.9,10
Pyridoxine deficiency has been reported in Sub-Saharan Africa and Central and Southeast Asia. Sub-Saharan Africa has a high prevalence of pyridoxine deficiency, primarily due to reliance on starchy roots and tubers, and is exacerbated by food insecurity and malnutrition. Prevalence rates include 58% in Cambodian children, 2.5 per 1000 infants in Laos, and over 20% in Thailand. 10
The risk for thiamine and pyridoxine deficiencies is considered public health concerns in West African, Southeast and South Asian communities. Southeast Asian public health efforts are aimed at improving nutrition through education, fortification, and supplementation. 11 Of note, these vitamin deficiencies are often underdiagnosed due to limited diagnostic guidelines and biomarkers. Global prevalence estimates are often underrepresented due to data discrepancies related to assay methodology differences across laboratories and limited population-level biomarkers. 11
Final Diagnosis
Our patient’s brain MRI revealed symmetric medial thalamic hyperintensities, consistent with thiamine and pyridoxine deficiency-related encephalopathy. Multidisciplinary consultations and collaboration with the family were integral to tailoring a comprehensive treatment plan. The patient’s sensory food aversion underscored the importance of addressing his nutrition to prevent further neurological deterioration. Following several iterations of his diet, the patient was discharged home on a standard pediatric formula, without a NG tube, and 25 mg/d of both thiamine and pyridoxine, in addition to a multivitamin with follow-up with physical and occupational therapies, neurology, and cardiology for repeat electrocardiogram and echocardiogram.
Conclusion
This case highlights the neurological and cardiac sequelae of vitamin deficiencies due to sensory food aversions in pediatric patients. Early recognition is vital to prevent irreversible damage. In pediatric patients with food aversions, weakness, lethargy, and other neurological symptoms may be indicators of severe malnutrition and vitamin deficiencies, including thiamine and pyridoxine. 3 These reversible conditions carry significant morbidity and mortality in children if they go unrecognized, especially in the western world. In parts of the world with greater food insecurity, these conditions are much more common and account for high mortality rates in children. Thus, age-appropriate diet counseling is imperative for health workers caring for pediatric patients. Prompt comprehensive inpatient care encompassing cardiac and neurological evaluations, nutritional interventions, and tailored rehabilitation therapies are essential to optimize treatment outcomes, enhance quality of life, and assure safe disposition for patients.9,10 In 1 month follow-up, our patient had gained 5.1 kg from his initial presentation and was back at his neurological and cardiovascular baselines. This case highlights the unique multidisciplinary care coordination challenges pediatricians face for children with significant food aversions. Early recognition is vital to prevent irreversible damage.
Author Contributions
Dr. Coelho and Dr. Kumar were responsible for the conception and design of the case report, acquisition and interpretation of data, drafting of the manuscript, reviewing and editing of the manuscript and approval of the final version for publication.
Footnotes
Acknowledgements
We would like to acknowledge Drs. Catherine Brown and Jonathan Lim for their contribution to this work.
Authors’ Note
Any other identifying information related to the authors and/or their institutions, funders, approval committees, etc., that might compromise anonymity: not applicable.
Ethical Considerations and Informed Consent Statements
Verbal and written informed consent were obtained from the patient’s mother. This case report meets ethical guidelines.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: M.M.C. has no conflict of interest. A.K. receives royalties from Wolters Kluwer for a Book she published.
Data Availability Statement
Not Applicable. Manuscript is a Case Report.
IRB approval Statement
IRB approval was waived for this paper given it is a Case Report. Appropriate informed consent was obtained from a parent.