
Abstract
Introduction:
Methicillin-resistant Staphylococcus aureus (MRSA) in cystic fibrosis (CF) impairs lung function and contributes to the progression of the disease. Optimal eradication regimens for new-onset MRSA infections in people with CF (pwCF) remain undefined.
Materials and Methods:
This prospective, multicenter study evaluated a standardized, step-up MRSA eradication regimen in pwCF with new-onset MRSA infections between 2020 and 2022.
Results:
Ninety-one pwCF (52.7% male, median age: 9 years) were included. Our treatment regimen included oral rifampicin and co-trimoxazole or oral rifampicin and fusidic acid. Intravenous teicoplanin treatment was initiated in patients whose clinical condition was unstable. The eradication success rates after 1 year were 82.4%, 92.9%, and 55.6%, respectively. No significant changes in median FEV1% predicted or BMI z-scores were observed between MRSA-eradicated and non-eradicated groups at baseline or 12 months.
Conclusion:
A standardized step-up MRSA eradication protocol is effective for new-onset MRSA infections in pwCF. Randomized controlled trials are needed to confirm these findings.
Introduction
Respiratory failure due to progressive lung damage and severe bronchiectasis is the major cause of mortality in cystic fibrosis (CF). 1 With progressive lung disease, Pseudomonas aeruginosa, Burkholderia cepacia, Achromobacter xyloxidans, and methicillin-resistant Staphylococcus aureus (MRSA) colonize the airway.2,3 With longer survival of people with CF (pwCF), the prevalence of MRSA has risen to 25% in recent years. However, Cystic Fibrosis Foundation (CFF) registry indicate a decline to 19%, likely due to increased access to modulator therapies. 3 - 5 However, modulators are not effective for all mutations and are also not universally accessible.6,7
Staphylococcus aureus is a gram-positive pathogen that spreads between people with and without CF. While methicillin-sensitive Staphylococcus aureus (MSSA) is one of the earliest infections and the most common microorganism in CF, MRSA infections occurs more commonly in young adults rather than children.8,9 Pancreatic insufficiency, CF-related diabetes (CFRD), increased hospitalizations, and co-infection with Pseudomonas aeruginosa are some of the patient- related risk factors for MRSA in CF.8,9 Methicillin-resistant Staphylococcus aureus and Pseudomonas infections are associated with significant negative clinical outcomes for CF. Pseudomonas aeruginosa eradication is accepted as a standard care of CF universally, however, eradication of MRSA still remains controversial among different guidelines.2,8,10,11 Several studies have reported worse clinical outcomes with MRSA infection in CF. 4 ,12-15 Individuals with CF who had persistent MRSA infection had a 43% more rapid decline in lung function. 4 Increased hospitalization rates and increased outpatient treatment requirements in MRSA infected patients are reported. 16 In addition, chronic MRSA infection is also a risk factor for worse lung function recovery after pulmonary exacerbations and is associated with higher mortality rates.15,17 Therefore, Royal Brompton Hospital guidelines recommend eradication of MRSA when first isolated in respiratory samples of CF patients. 18
The optimal eradication regimen for MRSA remains uncertain, with protocols varying in durations and antibiotic combinations.19-22 Differences in patient characteristics and definition of eradication success further complicate outcomes. A recent Cochrane review found insufficient evidence to support a specific eradication regimen. 23 A retrospective study from one of our centers reported a 35.4% eradication rate at 1 year with no significant difference between intravenous and nonintravenous regimens. 24 Given the need for prospective studies, we aimed to evaluate the effectiveness of a standardized MRSA eradication protocol and assess clinical factors influencing success over 1 year.
The primary aim of the present study was to determine the success rate of a standardized eradication protocol for MRSA. Secondary aim was to assess the clinical outcomes of eradication success and failure by comparing factors associated with disease severity (FEV1 pp, BMI z score) at baseline and at the end of 1 year. We also aimed to investigate the factors affecting the eradication success.
Materials and Methods
The study was conducted as a multicenter prospective and from 4 different CF centers in Istanbul which was performed between March 2020 and November 2022. The sample size calculation was based on a previously reported MRSA eradication rate of 84% in cystic fibrosis patients. Assuming a 5% significance level and 80% statistical power, a clinically significant difference of 15% was considered. Using these parameters, the estimated sample size required for each group was determined to be approximately 40 patients. 25 The study received ethical approval from the Marmara University Ethics Committee with number 09.2021.338. Written informed consent was obtained from all participants in the study. Parents gave their consent for their children.
Participants
Patients with CF whose respiratory samples were positive for new-onset MRSA infection were included in the study. Inclusion criteria were; CF diagnosis according to the consensus guideline of Cystic Fibrosis Foundation (CFF), 26 to continue regular follow-ups in the CF center, and the presence of new-onset MRSA infection in sputum or deep pharyngeal aspirate cultures. New-onset MRSA infection was defined as either a first ever isolation of MRSA or a new MRSA isolation after a clearance period of 12 months (after performance of 4 negative cultures).
Patients with a history of hypersensitivity or adverse reaction to antibiotics, patients with liver disease or abnormal liver function tests at the beginning of the study (alanine transaminase [ALT] and/or aspartate aminotransferase [AST] levels more than twice the upper limit of the normal range) patients with chronic MRSA infection, and MRSA resistant to both antibiotics; co-trimoxazole and rifampicin were excluded from the study.
Patients’ demographic, anthropometric, and clinical data were recorded from the medical records. Respiratory colonization profile of the patients was also recorded. Chronic infection was defined as the persistence of the same microorganism in more than 50% of the cultures in the preceding year and intermittent infection as having positive cultures in less than 50% according to Leeds criteria. 27 Pulmonary exacerbation was defined according to Fuchs criteria. 28
Eradication Protocol
Patients with new-onset MRSA isolation were treated with a standardized protocol of oral or IV antibiotherapy based on the protocol in the Royal Brompton Hospital CF Care Guidelines, 18 according to their clinical status. Clinically stable patients were treated with oral rifampicin (10 mg/kg twice daily-bd, max 600 mg) plus oral co-trimoxazole (6 weeks-5 months: 120 mg bd, 6 months-5 years: 240 mg bd, 6-11 years: 480 mg bd, 12-18 years: 960 mg bd) for 21 days. In case of co-trimoxazole resistance, oral rifampicin and fusidic acid (<1 year: 15 mg/kg 3 times daily-tds, 1-4 years: 250 mg tds, 5-12 years: 500 mg tds, >12 years: 750 mg tds or 500 mg sodium fusidate tablets tds) were used for 21 days. Intravenous (IV) antibiotics for 14 days were administered to patients who were clinically unstable or oral eradication failed. Patients with respiratory distress, hypoxia, hypercarbia, fever, and decreased oral intake were accepted as clinically unstable. First-line IV antibiotic choice was teicoplanin (>2 months-11 years: 10 mg/kg 12 hourly for 3 doses, followed 24 hours later by 10 mg/kg od. > 12 years: 6 mg/kg 12 hourly for 3 doses [loading dose] followed 24 hours later by 6 mg/kg od) and vancomycin (3 months to < 12 years: 60-80 mg/kg/day Q 6 hours, >12 years to 18 years: 60-70 mg/kg/day Q 6-8 hours). Teicoplanin was preferred primarily as it does not require blood level analysis. If first-line IV treatment fails, IV linezolid treatment (<12 years: 10 mg/kg tds, max 600 mg tds, >12 years: 600 mg bd) was used. In patients receiving parenteral therapy, complete blood count, renal function tests (urea, creatinine), and liver function tests (ALT, AST) were monitored twice weekly. If this treatment also fails, nebulized vancomycin was the third line eradication treatment. 18
Patients received eradication treatments according to antibiotic susceptibility of the cultures. Topical treatment including nasal, skin, oral, and a 3-week environmental decontamination were recommended in addition to all oral/parenteral eradication treatments. Inhaled, oral and IV antibiotic dosages were administered according to the Royal Brompton Hospital CF Care Guidelines. 18 Figure 1 summarizes the standardized eradication protocol for MRSA.
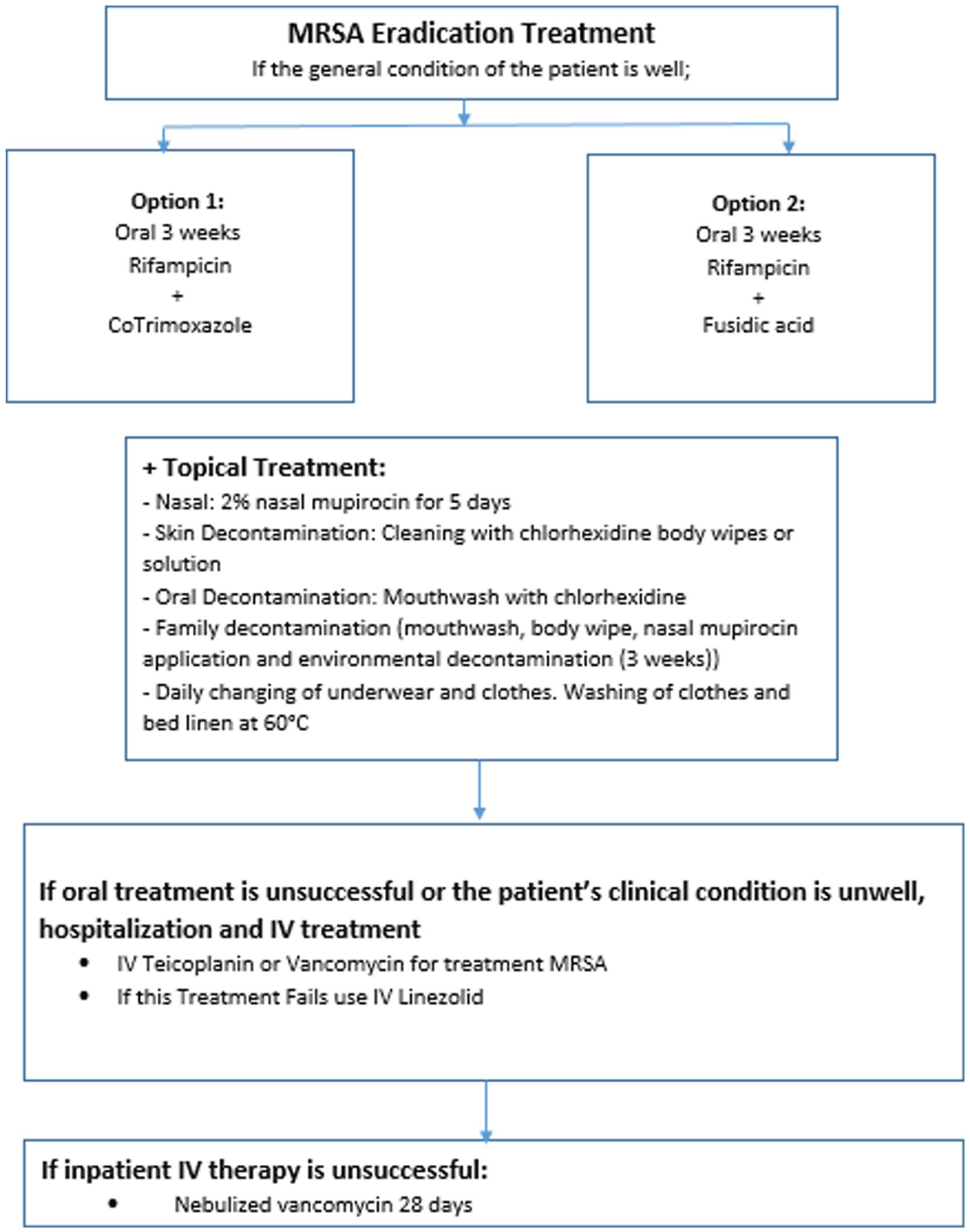
Eradication protocol for MRSA.
The eradication rate of the patients was evaluated according to the results of control sputum culture or deep pharyngeal culture. Successful eradication was described as not having any MRSA growth for 12 months after completing all steps of the protocol. At least 3 respiratory samples were obtained during 1 year. First respiratory sample was obtained 2 weeks after finishing the eradication protocol. Respiratory samples including sputum samples or deep pharyngeal swabs were obtained every 3 months. The delta changes in FEV1 pp and BMI z-score were calculated as the absolute differences between the 12-month and baseline measurements.
Statistical Analysis
Statistical analyses were performed using the IBM Statistical Package for the Social Sciences (SPSS) Version 20 for Windows (SPSS Inc., Chicago, IL). Continuous variables that were normally distributed were presented as means and standard deviations whereas the data with asymmetrical distribution were presented as medians and percentiles. Categorical variables were presented as proportions. Mann-Whitney U test was performed to compare 2 independent nonparametric variables data. Wilcoxon test was performed to compare paired groups with nonparametric variables. Categorical data were analyzed via chi-square or Fisher exact tests. P ≤ .05 was considered to be significant.
Results
The study included 91 people with CF from 4 different CF Centers in Istanbul, Turkey. Forty-eight (52.7%) of the patients were male while median (25-75th percentile) age of the patients was 9 (4-13.5) years. Thirty-two of the patients (35.2%) had been diagnosed with CF by newborn screening test which is performed by immune reactive trypsinogen analysis in blood spot. Thirty-seven (40.7%) of the patients were not eligible for modulator treatment while 12 of the patients (25.2%) were using modulator treatment during the study. Even though the remaining 31 patients (34.1%) were eligible for modulator therapy, they could not receive the drugs during the study period. Patients’ demographic data and baseline characteristics are presented in Table 1.
Demographic and Clinical Characteristics of the Patients (n = 91).
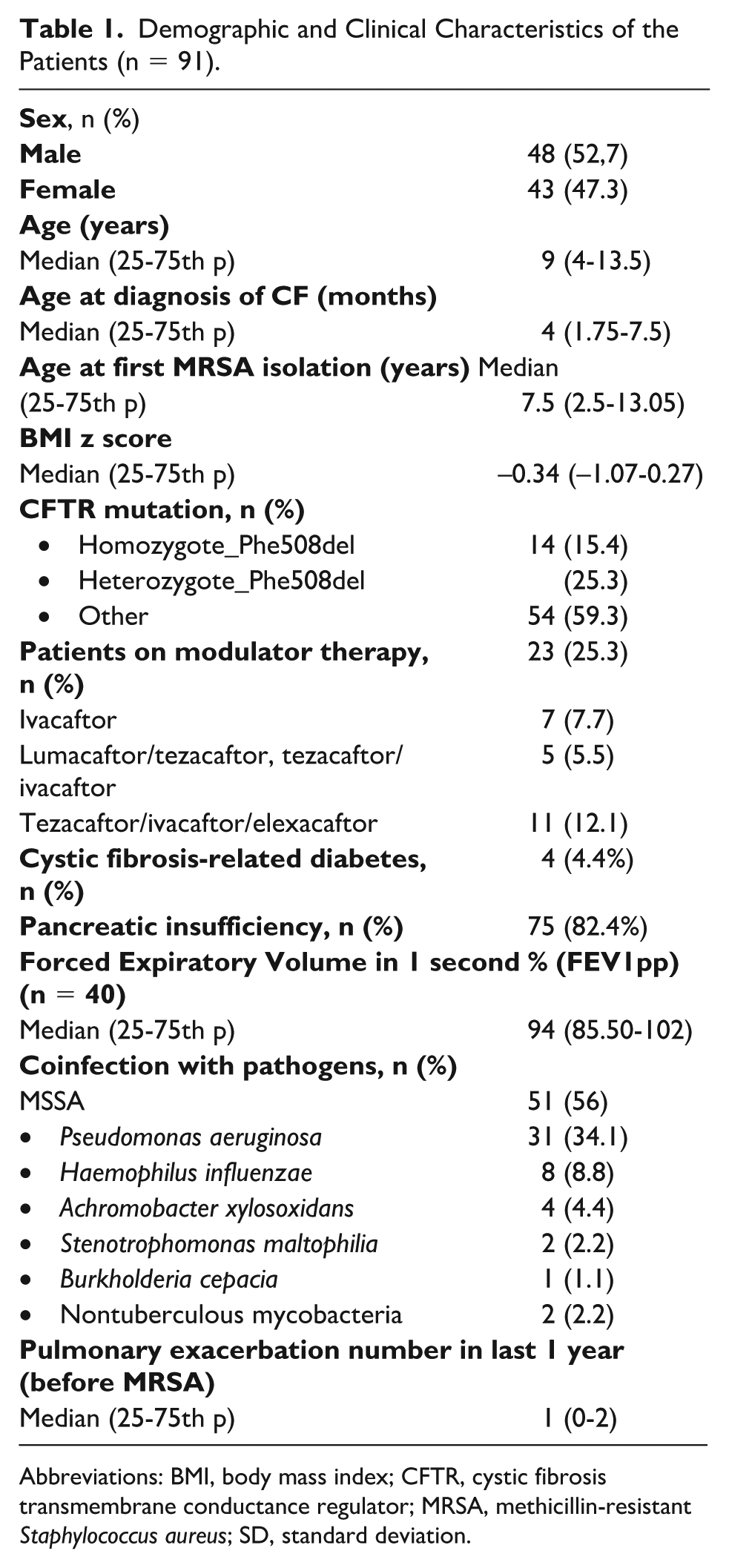
Abbreviations: BMI, body mass index; CFTR, cystic fibrosis transmembrane conductance regulator; MRSA, methicillin-resistant Staphylococcus aureus; SD, standard deviation.
The median age of the patients at first isolation of MRSA was 7.5 (2.5-13.05) years. A new-onset respiratory symptom was present in 52 (57.1%) of the patients at the time of first isolation of MRSA. The most common new-onset symptom was cough with a frequency of 51.6% (n = 47) while increased sputum production follows (n = 25, 27.5%). On physical examination, new-onset tachypnea was present in 5 patients (5.5%) while 2 patients (2.2%) had new-onset dyspnea. None of the patients were hypoxic at the time of first isolation of MRSA.
34.1% (n = 31) of patients had a Pseudomonas aeruginosa infection. In addition, 4 patients (4.4%) had an accompanying allergic bronchopulmonary aspergillosis (ABPA) infection. Burkholderia cepacia infection was detected in 1 patient (1.1%), while 2 patients (2.2%) had non-tuberculous mycobacteria (NTM) infections.
Patients received eradication treatments based on the antibiotic susceptibility of the cultures. Among the patients, 35 (38.5%) had methicillin-resistant Staphylococcus aureus (MRSA) with susceptibility to non-beta-lactam antibiotics, while 50 (54.9%) had multidrug-resistant MRSA. Antimicrobial susceptibility results were unavailable for 6 patients (6.6%). In 68 of the patients (74.7%), oral rifampicin and oral co-trimaxazole treatment was initiated while oral rifampicin and fusidic acid treatment was initiated in 14 (15.4%) of the patients. Nine patients (9.9%) received parenteral teicoplanin treatment. Figure 2 shows the number of patients with different eradication regimens.
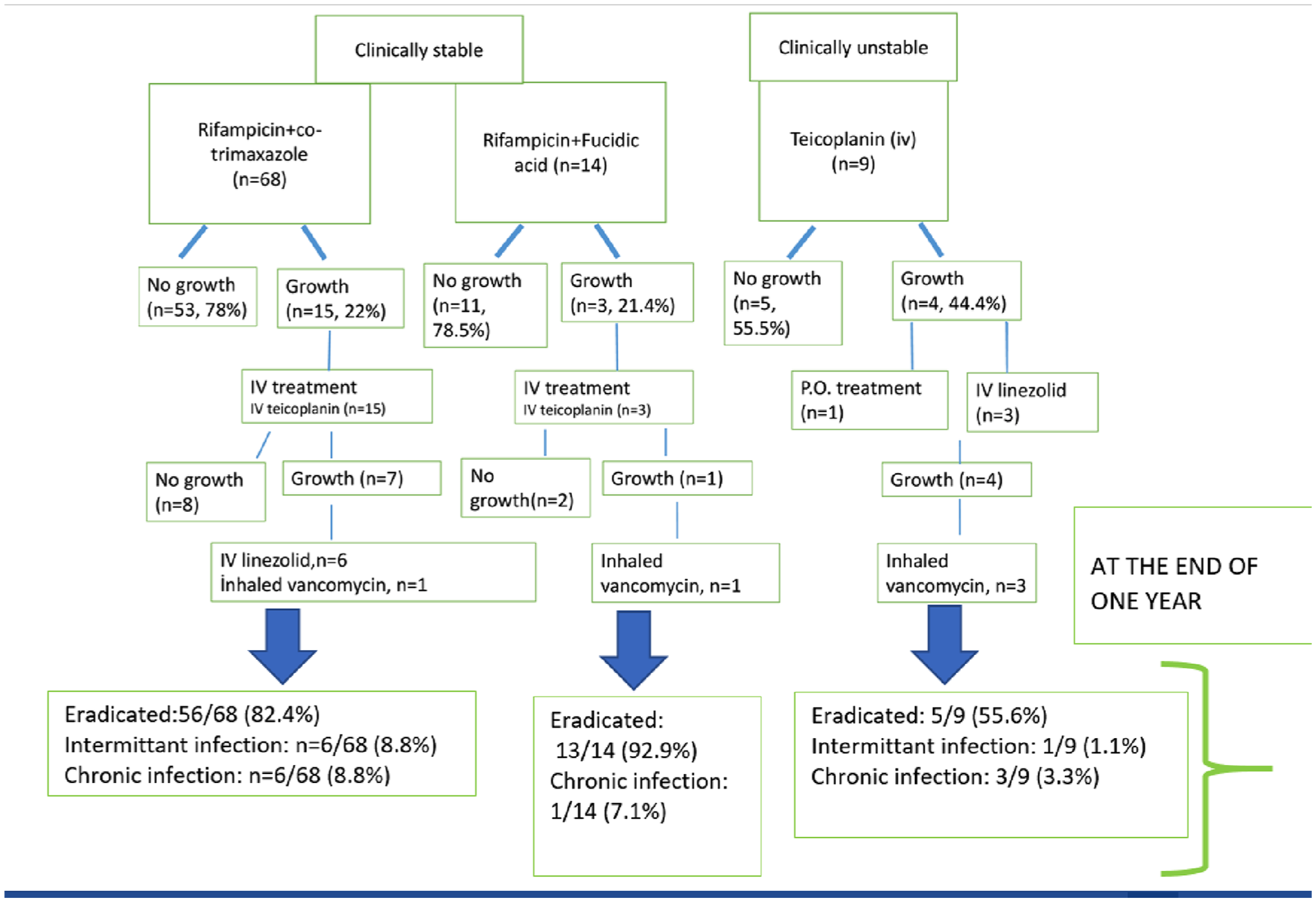
Eradication status of the patients according to treatments.
After the first-step eradication treatment, 24.2% of the patients (n = 22) required an additional eradication (second) treatment, while 11 patients (12.1%) needed a third subsequent treatment (iv linezolid, n = 6; inhaled vancomycin, n = 5). (One patient’s parents did not accept to have a third step eradication treatment in the parenteral teicoplanin group.) In 75.8% of the patients (n = 69), there was no growth of MRSA after first-step eradication treatment. At the end of 1 year, MRSA was eradicated in 74 (81.3%) of the patients.
Intermittent MRSA infection was detected in 7 (7.7%) of the patients while 10 patients (11%) were accepted to be colonized with MRSA at the end of 1 year.
Eradication rate of the patients whose first step eradication treatment was rifampicin plus co-trimaxazole was 82.4% (n = 56) at the end of 1 year while this ratio was 92.9% (n = 13) in rifampicin plus fusidic acid group and 55.6% (n = 5) in parenteral teicoplanin group.
All of the patients who required nebulized vancomycin (n = 5) failed to eradicate MRSA at the end of 1 year while 1 of 6 patients’ eradication was successful with linezolid.
Table 2 shows the comparison of clinical and demographical characteristics of the patients according to their MRSA eradication status at the end of 1 year. There was no significant difference in terms of sex, age, comorbidities, treatments, baseline pulmonary function, and BMI z score between the patients according to their MRSA eradication status at the end of 1 year. Coinfection with another microorganism (Pseudomonas aeruginosa, Hemophilus influenza, Achromobacter xyloxidans, Stenotrophomonas maltophilia) did not differ between eradicated and non-eradicated groups (P > .05 for all).
Comparison of the Patients According to Their Eradication Status (n = 91).
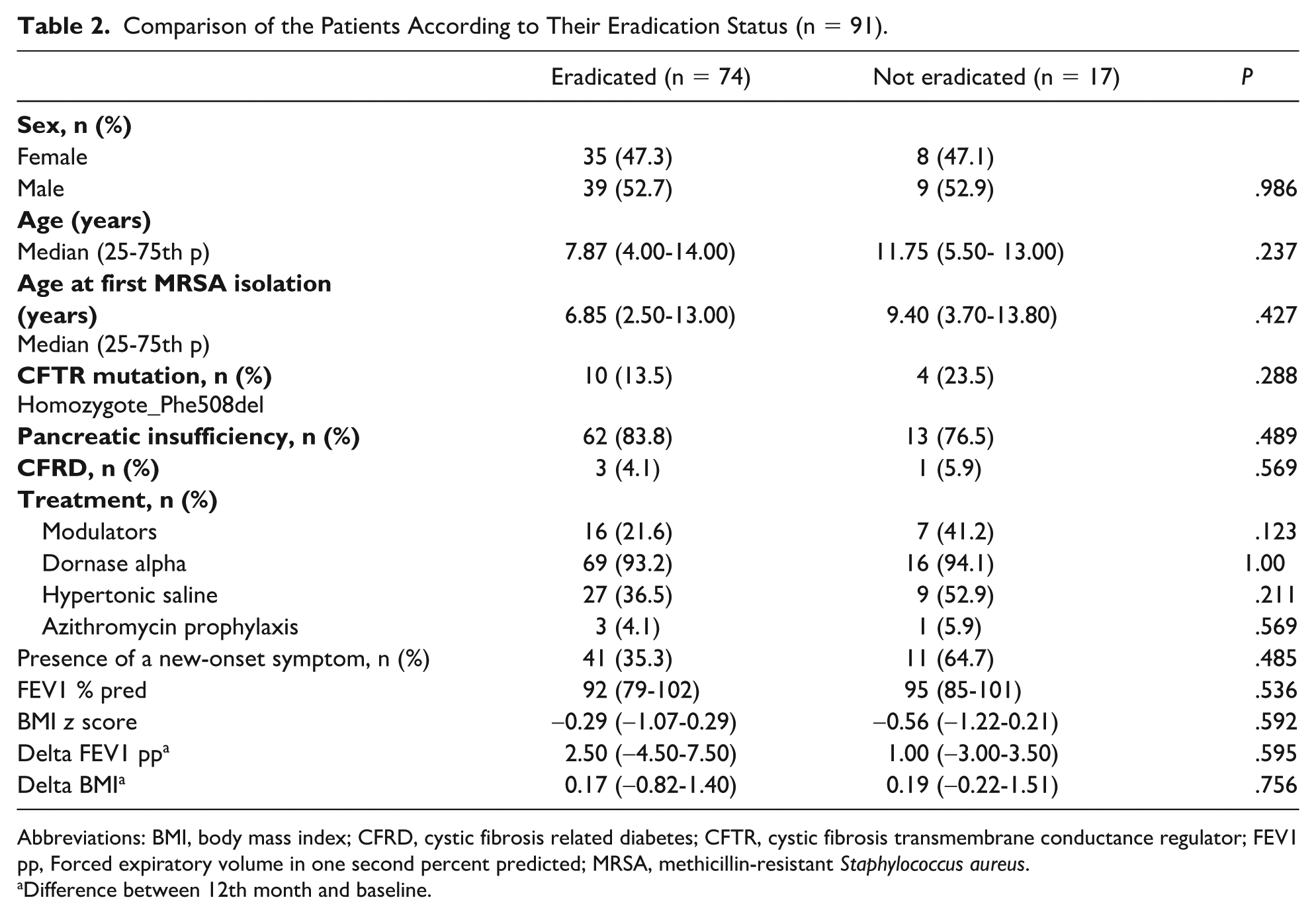
Abbreviations: BMI, body mass index; CFRD, cystic fibrosis related diabetes; CFTR, cystic fibrosis transmembrane conductance regulator; FEV1 pp, Forced expiratory volume in one second percent predicted; MRSA, methicillin-resistant Staphylococcus aureus.
Difference between 12th month and baseline.
There were no significant difference in terms of baseline and 12th month results of median FEV1 pp and BMI z scores in both MRSA-eradicated and non-eradicated groups (Table 3).
Baseline and 12th Month Comparison of Eradicated and Non-Eradicated Groups.
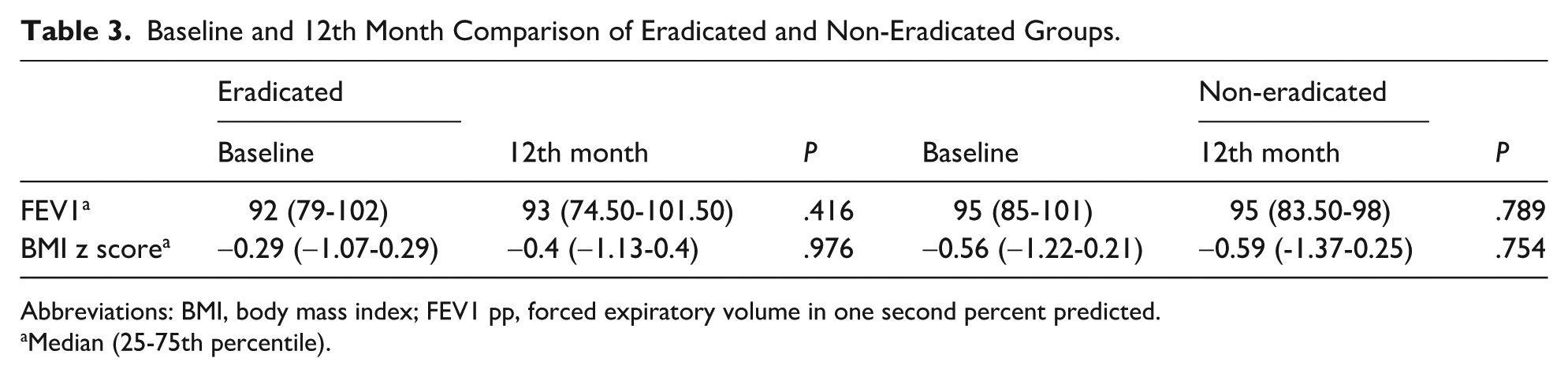
Abbreviations: BMI, body mass index; FEV1 pp, forced expiratory volume in one second percent predicted.
Median (25-75th percentile).
Discussion
The current multicenter study represents the results of a standardized MRSA eradication protocol and includes prospective data regarding the success of a standardized eradication regimen and clinical outcomes of MRSA-infected people with CF. At 1 year, MRSA was eradicated in 74 (81.3%) of the patients, a relatively high eradication ratio. The optimal regimen for MRSA eradication in CF remains a challenge, with existing literature showing varying success rates for first MRSA infection. 23 In this study, we achieved an 81.3% eradication rate, which is higher than the 18% to 20% success reported for chronic MRSA infections, supporting the importance of early MRSA eradication.21,29
Definition of eradication varies between studies. Dolce et al 30 conducted a randomized controlled study and defined eradication as 3 negative cultures over a 6-month period, reported the eradication rate as 63.2% at the end of 6 months by using a 21-day oral eradication treatment while eradication rate was 38% (5 of 13) in the observation-only group. Muhlebach et al 31 included people with CF aged between 4 and 45 years and reported that 82% were MRSA negative at day 28 in the treatment arm while 26% of the participants were negative in observation arm. In our study, we found the eradication rate as 81.3% at the end of 1 year. A previous retrospective study from one of the centers in the current study showed that MRSA eradication rate was 35.4% at the end of 1 year while 36 of 48 patients received parenteral teicoplanin. With the results of our previous study, we recognized the low ratio of MRSA eradication and nonsuperiority of parenteral eradication to oral eradication. 24 Thereby, we implemented a standardized, step up eradication protocol according to previous guidelines. The increased eradication rates show the efficacy of our new protocol.
There are many different eradication regimens for MRSA infection in CF including single or dual oral antibiotics, inhaled antibiotics, parenteral single/ dual antibiotics, or more aggressively; a combination of parenteral, oral and inhaled antibiotics for a longer time period. All of these studies include environmental hygiene procedures and topical treatments.25,30,32 Oral therapy is as effective as parenteral therapy for eradication of first MRSA in CF. 24 In our study, MRSA eradication rate with parenteral treatment was not superior to oral eradication regimen. Even though we selected a parenteral eradication protocol for patients with unstable clinical conditions, these results are important to demonstrate the success of an oral eradication protocol for a clinically stable pwCF. Thereby, we expect decreased hospitalization rates, decreased treatment burden and decreased health care costs after implementing our new eradication protocol. 33 Even though oral eradication regimens for MRSA infection are accepted by most of the CF centers, there is only a few randomized controlled studies for the optimal oral eradication regimen. 31 Dolce et al 30 conducted a randomized multicenter study and active treatment group received oral rifampicin plus oral TMP-SMX for 21 days together with nasal mupirocin for 5 days similar to our study. Methicillin-resistant Staphylococcus aureus eradication was accepted as 3 consecutive negative cultures over a 6 months and reported as 63.2% in the treatment arm. Another randomized controlled study included dual oral antibiotherapy (TMP-SMX or minocycline and rifampin) for 2 weeks in addition to nasal, oral, and skin decontamination and environmental decontamination for 3 weeks and reported a success rate of 82% at day 28. However, in this study, fusidic acid was not been used as it was not licensed in the United States. 31 Hall et al performed a retrospective cohort study including 37 CF patients and 67.6% (n = 25) had new-onset MRSA. Even though statistically insignificant, they reported that dual oral eradication regimens are superior to single oral regimens to eradicate new MRSA infection (84.6% vs 50%, P = .1); rifampicin/fusidic acid combination had the highest success rate when compared with other dual regimens (100% vs 60%, P = .13) and achieved higher rates of sustained MRSA clearance at 6 months (57.1% vs 30.8%) and 12 months (46.7% vs 21.4%). They also reported that eradication rate for shorter courses (≤14 days) was 75% while it was 100% for longer courses (>14 days). Even though small number of patients are one of the limitations of the study, it is important to demonstrate the importance of a dual oral antibiotic course with a relatively shorter period similar to our study. In addition, rifampicin and fusidic acid combination had the highest eradication ratio at the end of 1 year, similar to our study. 21 Multiple studies including new onset and persistent MRSA-infected patients with CF have reported that rifampicin and fusidic acid combination are well tolerated and have a relatively high eradication success rate with a ratio between 71% and 100%.20,22,34,35 However, sample sizes of these studies are small and include a prolonged eradication regimen up to 6 months. In our study, we showed that a relatively shorter period of dual oral antibiotherapy is successful at eradication of first MRSA which shows that longer periods of treatment may not be necessary, similar to Hall et al’s 21 study. All of the patients who required nebulized vancomycin (n = 5) failed to eradicate MRSA at the end of 1 year in our study. Even though number of pwCF is small, a similar finding has been previously reported by Dezube et al. They concluded that the addition of a single course of inhaled vancomycin did not have an additional benefit for persistent MRSA infection with a risk of bronchospasm up to 28% of the patients. 29
Clinical outcomes of MRSA eradication were also evaluated as the 1-year absolute difference from baseline and compared between eradicated and non-eradicated groups. We did not find a significant difference in terms of change in baseline and 12th month FEV1 pp and BMI Z scores of the patients according to their MRSA eradication status.
Dolce et al 30 reported that even though statistically insignificant, patients in the active treatment arm had a mean (±SD) FEV1 change from baseline +7.13% (±14.92) while observation group had a mean change -1.16% (±5.25) (P = .08) at 6th month. Muhlebach et al 31 reported that at day 28, mean relative change in FEV1 was +2.5% in the treatment arm while it was -2.4% in the observation arm (P = .08). Different from other studies, we did not include an observation group and treated all of the patients. In our study, median FEV1 change between the baseline and 12th month of the eradicated group was 2.5% while it was 1% in non-eradicated group; however, this difference did not reach statistical significance. Even though MRSA could not be eradicated in some patients, these patients may optimize their daily respiratory therapies with close follow up which may affect the results. In addition, there were only small number of patients in the non-eradicated group. There is a need for longer, randomized control in this area.
Demographic and clinical characteristics of the patients are potential factors which may affect the risk of eradication failure of MRSA. Pancreatic insufficiency, CFRD, coinfection with Pseudomonas aeruginosa and frequent hospitalization in the last year were defined as risk factors to develop persistent MRSA infection. 36 We did not find a significant difference between baseline clinical and demographic characteristics of eradicated and non- eradicated groups including age, sex, pulmonary function, BMI z-scores, pancreatic insufficiency, CFRD and the frequency of pulmonary exacerbations and hospitalizations in the last year. Hall et al 21 reported that the prevalence of DF508 homozygosity, CFRD, and pancreatic insufficiency was higher while pretreatment FEV1 was lower in patients who failed to eradicate MRSA, however, these differences did not reach statistical significance. In our study, even though statistically insignificant, the median age of the eradicated group was younger than non-eradicated group (6.85 vs 9.40 years, P = .427) and the prevalence of DF508 homozygosity, CFRD were higher in the eradication failure group.
There are some limitations of the study. First, as we treated all of the patients due to concerns about lung function deterioration, we did not include a control group. Second, we did not screen household members and CF center staff regarding MRSA colonization which may be a potential source for reinfection, however, infection control measures were strictly followed.
In conclusion, our study shows the success of a standardized, step-up MRSA eradication protocol. Dual oral antimicrobial therapy is an efficient, cost-effective, and well- tolerated therapy for MRSA eradication with a high success rate. Even though we did not find a significant difference in terms of FEV1 and BMI z scores between pwCF who were eradicated or failed to eradicate MRSA at the end of 1 year, long-term results are needed in this area. There is an urgent need for further, randomized controlled studies for better understanding long-term effects of MRSA infection and finding the optimal eradication regimen.
Author Contributions
BK, FK, EEE, YG, EÇ and SG: designed the study. AG, CYY, MY, MK, MSB, ŞK, GT, BU, HA, HY and GBB: collected data. AG, CYY, AAKS and APE: wrote the manuscript. BK, FK, EEE, YG, EÇ and SG critically reviewed and supervised the whole study process. All authors read and approved the final manuscript.
Footnotes
Ethical Considerations
The study received ethical approval from the Marmara University Ethics Committee with number 09.2021.338. Written informed consent was obtained from all participants in the study. Parents gave their consent for their children.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.