
Abstract
The impact of the COVID-19 pandemic on pediatric obesity and comorbidities was investigated via a retrospective analysis of new patient visits at a pediatric weight management clinic. Prepandemic (N = 1590, January 1, 2017, to March 20, 2020) and postpandemic (N = 1040, April 1, 2020, to June 8, 2023), patients ages 2–21 years with overweight or obesity were studied. Results revealed significant increase in obesity severity during the postpandemic period (OR = 1.70 [1.45, 1.99]), with more comorbidities (OR = 1.28 [1.22, 1.34]). Prediabetes (OR = 1.62 [1.07, 2.47]), eating disorder/hyperphagia (OR = 1.77 [1.26, 2.50]), and attention deficit hyperactivity disorder (OR = 1.36 [1.09, 1.69]) diagnoses were more prevalent postpandemic. Patients aged 10 to <14 years (OR = 2.39 [1.51, 3.79]) and non-Hispanic patients (OR = 1.44 [1.07, 1.94]) had higher odds of mood/mental health disorder diagnoses postpandemic. In conclusion, the COVID-19 pandemic is associated with worsening pediatric obesity severity and higher prevalence of obesity-related comorbidities in new patients presenting for treatment.
Introduction
The COVID-19 pandemic has been associated with an increase in obesity prevalence and rate of body mass index (BMI) change in pediatric populations across the globe,1-3 with proposed risk factors including increased screen time, fewer opportunities for exercise, less access to nutritious foods, and increased stress during the pandemic.2,4,5 In a longitudinal cohort study conducted by the Centers for Disease Control and Prevention (CDC) of over 400 000 children and adolescents ages 2–19 years in outpatient visits across the United States, the estimated prevalence of obesity increased from 19.3% to 22.4% between August 2019 and August 2020. 6 These findings of increased obesity severity postpandemic are consistent with results from other cohort studies assessing BMI of children and adolescents through electronic health records (EHRs) of primary care visits in the United States.7-12
In addition, disparities in the severity of obesity have been observed in relation to demographic variables and specific patient characteristics. Pediatric patients with moderate or severe obesity experienced significantly higher rates of BMI increase during the pandemic when compared with their counterparts with healthy weight.6,8,12 Furthermore, children and adolescents who lacked commercial insurance and who were either Black or Hispanic experienced the highest rates of BMI increase during the pandemic, highlighting important public health disparities exacerbated by COVID-19.8,13 As childhood obesity often persists into adulthood and increases the risk of other chronic diseases and premature mortality,14,15 these findings pose serious short and long-term problems for both individual and population health.
Most existing literature regarding the impact of COVID-19 on pediatric obesity analyzes changes in pediatric BMIs recorded at primary care visits or in school settings, and there is conflicting data regarding rate of attenuation of BMI increase during the post pandemic years.7,11,12,16,17 To our knowledge, there have been no studies assessing BMI status of patients at pediatric weight management clinics and very few long-term studies assessing BMI status in children and adolescents past 2021. Furthermore, although some studies report an increase in certain pediatric obesity comorbidities,18,19,20 the extent to which COVID-19 has influenced comorbidity prevalence remains unknown. Examining data over an extended period of time before and after the onset of COVID-19 from clinics specifically designed to treat pediatric obesity could provide insight into the severity and acceleration of the pediatric obesity epidemic in the United States and elucidate the effects if any of COVID-19 on the prevalence of pediatric obesity comorbidities.
The overall objective of this study is to describe the impact of COVID-19 on pediatric obesity by examining the change in BMI and comorbidities in new patients presenting for an initial visit to a pediatric weight management clinic in the United States during the pre- and postpandemic period. We hypothesize that new patients presenting during the postpandemic period will have higher BMI and more accompanying comorbidities compared with new patients presenting during the prepandemic period.
Methods
Study Design and Population
This is a retrospective chart review examining the EHR data of new patient visits at a pediatric weight management clinic prior to and following the onset of the COVID-19 pandemic. The COVID-19 prepandemic period was defined as January 1, 2017, to March 20, 2020, and the postpandemic period was defined as April 1, 2020, to June 8, 2023. This study was granted a waiver of consent due to study design and approved by the associated Hospital’s Institutional Review Board, ethical approval number CR00000625.
The study sample included all patients ages 2–21 years who were seen for new patient visits at the pediatric weight management clinic in-person or online between January 1, 2017, and June 8, 2023, for whom medical records could be retrieved. Exclusion criteria included patients with Down syndrome and patients with incomplete anthropometric data. A total of 1590 eligible visits were identified for the prepandemic period, and a total of 1040 eligible visits were identified for the postpandemic period.
Study Measures
Data extracted from each visit included date of birth, date of visit, height, weight, sex (male and female), BMI, systolic blood pressure (SBP), diastolic blood pressure (DBP), hemoglobin A1c (HbA1c), lipid profile, aspartate aminotransferase (AST), alanine transaminase (ALT), and list of diagnoses from the EHR. Laboratory data was extracted if the lab results were completed between 3 months prior and 2 weeks after the date of the first patient visit. Body mass index measurements were classified as normal weight (BMI < 85th percentile), overweight (BMI ≥ 85th percentile to <95th percentile), class 1 obesity (BMI ≥ 95th percentile to <120% of the 95th percentile), class 2 obesity (≥ 120% to <140% of the 95th percentile or BMI ≥ 35 to <39 kg/m2, whichever is lower based on age and sex), and class 3 obesity (≥ 140% of the 95th percentile or BMI ≥ 40 kg/m2, whichever is lower based on age and sex) according to the American Academy of Pediatrics Clinical Practice Guidelines for Pediatric Obesity 21 and US CDC growth curves. 22 BMI-percentiles and z-scores were also calculated according to the same parameters.
Diagnosis of prediabetes, type 2 diabetes mellitus (T2DM), dyslipidemia, and elevated liver function tests (LFTs)/nonalcoholic fatty liver disease (NAFLD) was based on the medical provider diagnosis if no lab results were available in the patient’s EHR, as the medical provider may have received documentation regarding the patient’s medical comorbidities from a referring medical provider or may have had access to lab results that were not saved in the patient’s EHR. For visits with available lab results, prediabetes was classified according to the American Diabetes Association Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes-2020, 23 unless medical records indicated that the patient had type 1 diabetes mellitus or was taking anti-diabetic medication.
Dyslipidemia was classified as any combination of abnormal cholesterol (total cholesterol, triglyceride, high-density lipoprotein [HDL], low-density lipoprotein (LDL), and non-HDL) according to values referenced in the Expert Panel on Integrated Guidelines for Cardiovascular Health and Risk Reduction in Children and Adolescents: Summary Report. 24 However, classification of abnormal triglyceride level was left to the discretion of the diagnosing medical provider due to uncertainty of the patient’s fasting status during the lab draw. Available lab work that was not assessed by a medical provider was otherwise assumed to be non-fasting. Elevated LFTs/NAFLD was classified according to the North American Society for Pediatric Gastroenterology, Hepatology & Nutrition (NASPGHAN) Clinical Practice Guideline for the Diagnosis and Treatment of Nonalcoholic Fatty Liver Disease in Children. 25
Diagnosis of elevated blood pressure (BP) and hypertension (HTN) was dependent on medical provider diagnosis if the BP was not recorded on the date of visit, as the medical provider may have received documentation regarding the patient’s medical comorbidities from a referring medical provider. For visits with a recorded SBP/DBP, elevated BP and HTN were classified according to the Clinical Practice Guideline for Screening and Management of High Blood Pressure in Children and Adolescents, 26 unless medical records indicated that the patient was taking anti-hypertensive medication. If SBP and DBP were recorded multiple times during a visit, only the last record was included in the analyses.
Diagnoses of attention deficit hyperactivity disorder (ADHD), eating disorders/hyperphagia, and mood/mental health disorders were based solely on diagnoses listed in the patients’ EHR by the pediatric weight management clinic medical provider. Eating disorders/hyperphagia included diagnoses of binge eating disorder (BED), bulimia nervosa, unspecified eating disorder, and hyperphagia. Mood/mental health disorders included diagnoses of major depressive disorder (MDD), dysthymia, unspecified depression, depressed mood, depressed effect, mood disorder, reactive depression, adjustment disorder with depressed mood, affective disorder, disruptive mood dysregulation disorder (DMDD), premenstrual dysphoric disorder (PMDD), generalized anxiety disorder, unspecified anxiety, emotional disturbance of adolescence, bipolar disorder, schizophrenia, and posttraumatic stress disorder (PTSD).
Sociodemographic and Other Covariates
Sociodemographic variables used in analyses included sex at birth (male or female), race (black, white, Asian, other), and ethnicity (Hispanic/Latino or Non-Hispanic/Latino). All sociodemographic variables were collected from medical records.
Data Analyses
Because this study is a descriptive retrospective chart review during 2 specific time periods, sample size determination was not conducted. Patient characteristics in both the prepandemic and postpandemic period were reported using median, 25th, and 75th percentile for BMI and BMI z-score, while number of participants and percentages were reported for categorical variables (age group, obesity class, comorbidities, sex, race, ethnicity). The distribution of patient BMI and BMI z-score during the prepandemic and postpandemic periods was not normal. Wilcoxon rank sum test was used to compare BMI and BMI z-score between the 2 study periods, and Chi-square test/Fisher’s exact test was used to compare categorical variables between the 2 study periods. P-values less than or equal to .05 were considered statistically significant.
We compared the proportion of patients with overweight and obesity classes 1–3 across racial groups, sex, ethnic groups, and age groups during the pre- and postpandemic periods, as well as the BMI z-score across racial groups during the 2 study periods, with P-value assessed by Chi-square test/Fisher’s exact test and Kruskal–Wallis test, respectively.
Ordinal logistic regression was used to examine the effect of study period and other patient characteristics on obesity classification. Separate logistic regression models were used to examine the effect of patient characteristics and study period on the occurrence of each comorbidity. We assessed statistical interaction between all the predictor variables in the logistic regression models. Hosmer and Lemeshow test was used to assess whether each logistic regression model was able to fit the data.
Results
Section I. Patient Characteristics
Comparison of patient characteristics during the pre- and postpandemic periods showed an increase in the percentage of Black patients (40.2% vs 48.2%), non-Hispanic patients (60.1% vs 69.9%), and patients ≥14 years (35.7% vs 46.1%) presenting as new patients to the pediatric weight management clinic during the postpandemic period (Table 1). There was no significant difference in the sex of patients between the 2 study periods.
Descriptive Characteristics.
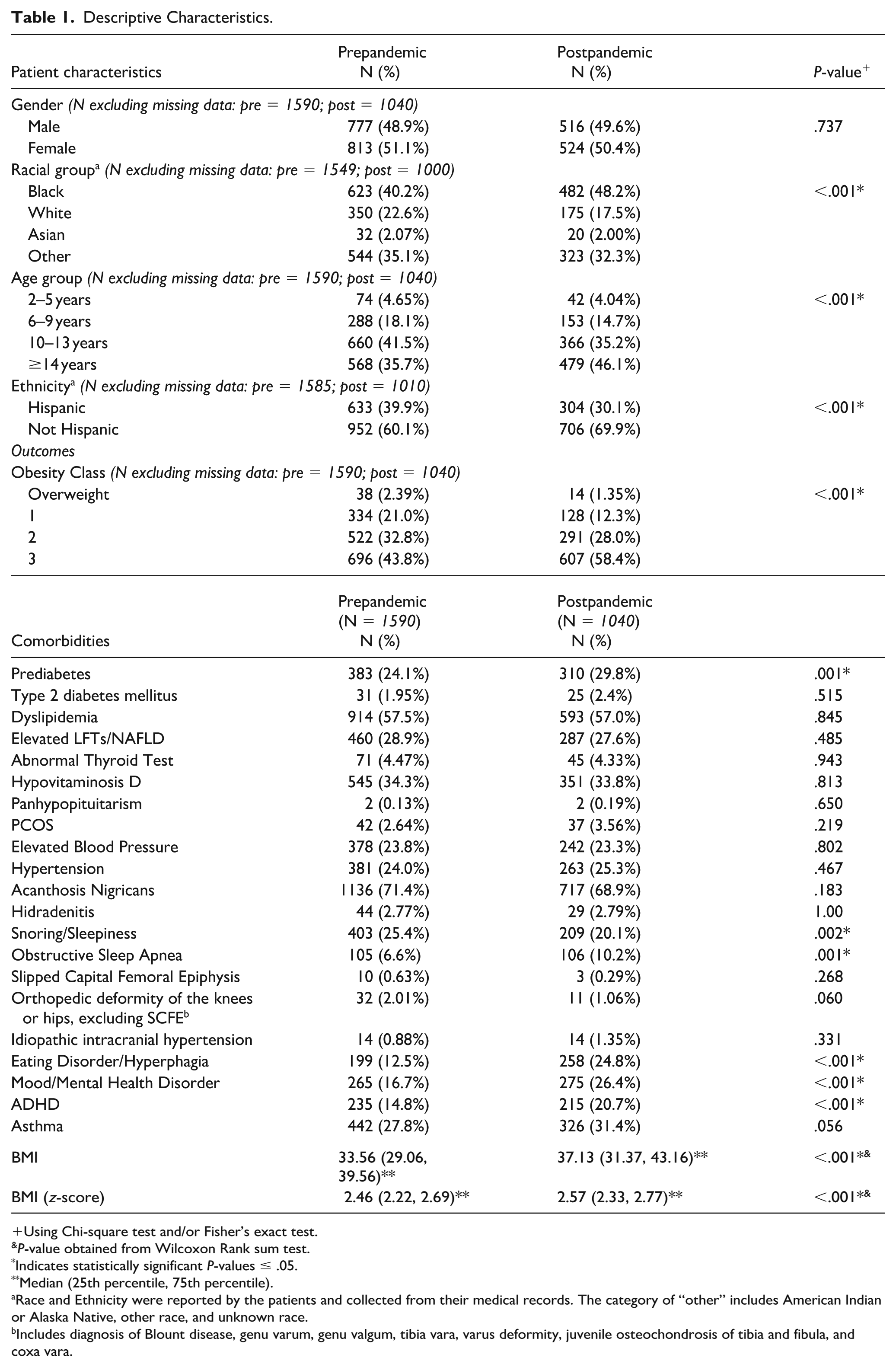
Using Chi-square test and/or Fisher’s exact test.
P-value obtained from Wilcoxon Rank sum test.
Indicates statistically significant P-values ≤ .05.
Median (25th percentile, 75th percentile).
Race and Ethnicity were reported by the patients and collected from their medical records. The category of “other” includes American Indian or Alaska Native, other race, and unknown race.
Includes diagnosis of Blount disease, genu varum, genu valgum, tibia vara, varus deformity, juvenile osteochondrosis of tibia and fibula, and coxa vara.
Section II. Obesity Class and BMI
There was an increase in patients with class 3 obesity (43.8% vs 58.4%) presenting as new patients to the pediatric weight management clinic during the postpandemic period (Table 1), and patients seen during the postpandemic period were significantly more likely to be diagnosed with a higher obesity classification compared with patients during the prepandemic period (OR = 1.70, 95% [1.45, 1.99]) (Table 2). There was also a significant increase in BMI z-score from prepandemic to postpandemic (P < .001). BMI z-score median (25th percentile, 75th percentile) in the prepandemic and postpandemic was 2.46 (2.22, 2.69) and 2.57 (2.33, 2.77), respectively (Table 1).
Associations Between Observation Period and Weight Status/Comorbidity Presence.
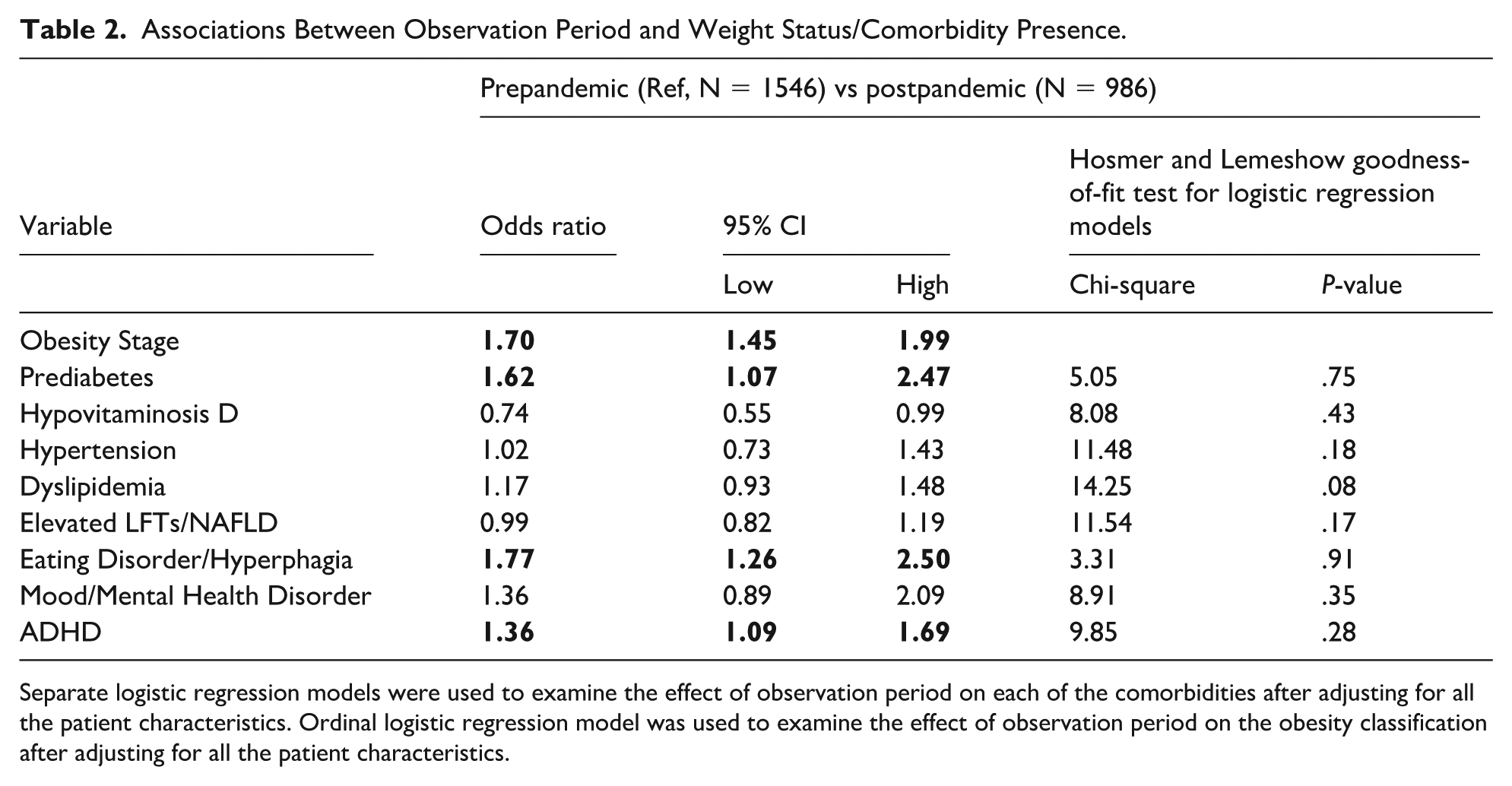
Separate logistic regression models were used to examine the effect of observation period on each of the comorbidities after adjusting for all the patient characteristics. Ordinal logistic regression model was used to examine the effect of observation period on the obesity classification after adjusting for all the patient characteristics.
Section III. Race and Obesity Class/BMI
Each ethnicity group, sex, age, and racial group except for Asian showed an increase in percentage of patients with class 3 obesity during the postpandemic period, and each racial group except for Asian showed an increase in both the mean and median BMI z-score during the postpandemic period.
Section IV. Comorbidities and Obesity Class
Univariate analyses of presence of comorbidities between the pre- and postpandemic periods showed a significant increase in percentage of patients with prediabetes (24.1% vs 29.8%, P = .001), eating disorder/hyperphagia (12.5% vs 24.8%, P < .001), mood/mental health disorder (16.7% vs 26.4%, P < .001), ADHD (14.8% vs 20.7%, P < .001), and obstructive sleep apnea (6.6% vs 10.2%, P = .001), as well as a decrease in the percentage of patients with snoring/sleepiness (25.4% vs 20.1%, P = .002) (Table 1).
Univariate analyses between the pre- and postpandemic periods yielded similar results after exclusion of individuals with overweight when examining presence of psychiatric disorders. There were a total of 1552 eligible visits during the prepandemic period and 1026 eligible visits during the postpandemic period after exclusion of patients with overweight. There was a significant increase in percentage of patients with eating disorder/hyperphagia (N = 196 vs 256, 12.6% vs 25.0%, P < .001), ADHD (N = 235 vs 211, 15.1% vs 20.6%, P < .001) and mood/mental health disorder (N = 259 vs 265, 16.7% vs 25.8%, P < .001).
Increase in the total number of comorbidities was associated with a higher obesity classification (OR = 1.28, 95% [1.22, 1.34]).
Section V. Prediabetes and Patient Characteristics
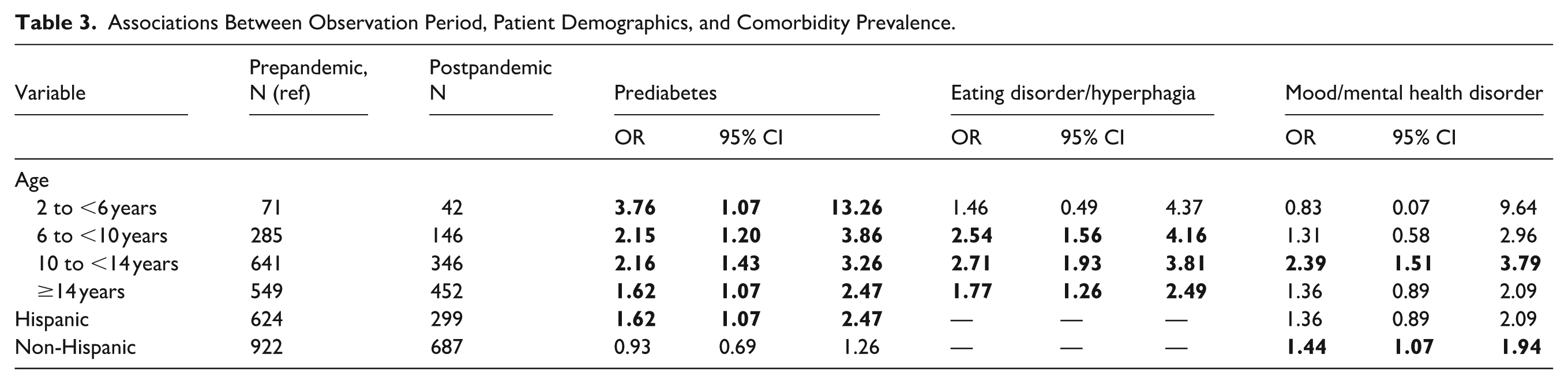
Patients seen during the postpandemic period had significantly higher odds of having prediabetes compared with patients during the prepandemic period (OR = 1.62, 95% [1.07, 2.47]) after adjusting for age, sex, race, and ethnicity (Table 2). We did not observe any statistically significant interaction between study period and age group; all age groups had significantly higher odds of prediabetes during the postpandemic period as compared with the prepandemic period (Table 3). We found that ethnic group moderated the association between study period and occurrence of prediabetes. Hispanic patients had significantly higher odds of prediabetes during the postpandemic period as compared with the prepandemic period (OR = 1.62, 95% [1.07, 2.47]) (Table 3). There was no such trend among the non-Hispanic study participants.
Associations Between Observation Period, Patient Demographics, and Comorbidity Prevalence.
Section VI. Eating Disorders/Hyperphagia, ADHD, Mood/Mental Health Disorders and Patient Characteristics
Patients had significantly higher odds of eating disorder/hyperphagia (OR = 1.77, 95% [1.26, 2.50]), and ADHD (OR = 1.36, 95% [1.09, 1.69]) during the postpandemic period as compared with the prepandemic period after adjusting for patient characteristics (Table 2). Age group moderated the association between study period and occurrence of eating disorder/hyperphagia. Patients ages 6 years and older had significantly higher odds of eating disorder/hyperphagia during the postpandemic period as compared with the prepandemic period (Table 3). Age group and ethnic group had a moderating effect on the association between the study period and the occurrence of mood/mental health disorder. Patients ages 10 to <14 years (OR = 2.39, 95% [1.51, 3.79]), and non-Hispanic patients (OR = 1.44, 95% [1.07, 1.94]) had significantly higher odds of mood/mental health disorder during the postpandemic period compared with the prepandemic period (Table 3).
Section VII. Nonsignificant Comorbidity Findings
There were no significant interactions between study periods and demographic variables for the following comorbidities: hypertension, dyslipidemia, abnormal LFTs/NAFLD, and vitamin D deficiency.
Discussion
To our knowledge, this is the first study to assess the impact of COVID-19 on BMI and obesity-related comorbidities in children and adolescents presenting as new patients to a pediatric weight management clinic in the United States. This study demonstrates a significant increase in the percentage of new patients presenting with class 3 obesity during the 3-year period after the onset of COVID-19 as compared with the 3-year period prior, with an increase in the number of comorbidities per patient. In addition, a higher percentage of Black patients, non-Hispanic patients, and patients 14 years and older presented as new patients during the postpandemic period. Of the 21 comorbidities examined, there were notable increases in postpandemic diagnoses of prediabetes, ADHD, eating disorder/hyperphagia, and mood/mental health disorder.
The increased percentage of new patients presenting with class 3 obesity aligns with previous reports of increased obesity prevalence and BMI rate increase in pediatric patients during COVID-19.1-3 However, lack of a control group and referral bias with our study population of referred patients who showed up for their appointments limits generalizability of our findings. The change in median BMI z-score observed in our study (.11), while similar to the mean increase in BMI score (.13) observed in the general pediatric population, 1 is difficult to compare given differences in study measurements and duration. Furthermore, data regarding attenuation of obesity rates postpandemic is sparse and may be country specific.7,11,16,17 Additional studies are needed to determine whether the observed findings mainly affect patients with preexisting obesity or if they mirror general pediatric trends.
Given our retrospective study design, establishing causality between the postpandemic period and increase in obesity severity is challenging. However, many obesogenic factors were exacerbated during COVID-19, including decreased physical activity due to closure of recreational areas,27,28 worsened diet quality, 29 and increased screen time.30,31 These factors disproportionately affected Black, Hispanic, low-income, and child-containing households.32-35 The observed postpandemic increase in percentage of Black patients may reflect disparities in COVID-19 impact on obesogenic factors. However, the decrease in percentage of Hispanic patients was not predicted and contradicts studies showing an increase in obesity in this population,8,13 raising questions about COVID-19 impact on access to health care between different communities.
Although some studies have looked at the impact of COVID-19 on a single obesity-related comorbidity,18,19,36,37 no prior study has examined the effect of the pandemic on the prevalence of obesity-related comorbidities as expansively as ours. Our results showed a significant increase in percentage of patients with prediabetes after the pandemic onset; and that all age groups had greater odds of being diagnosed with prediabetes. Although our sample size for patients with T2DM was too small to produce statistically meaningful results, the increase in prediabetes diagnosis aligns with literature demonstrating an increase in new-onset T2DM during COVID-19.36-39 Further research is indicated to determine if the postpandemic period increase in prediabetes/T2DM is primarily due to weight gain or another underlying mechanism.
Our findings of increased odds of ADHD and eating disorder/hyperphagia diagnoses postpandemic are in line with studies that have found worsening of ADHD and BED symptoms during the pandemic.40-43 Increased screen time in children from all backgrounds could potentially explain our finding of increased odds of ADHD diagnosis across all demographic groups, as increased recreational screen time is associated with worsening ADHD symptoms.44,45 Meanwhile, our finding of increased odds of eating disorder/hyperphagia diagnosis in children and adolescents ≥6 years could be indicative of social factors influencing younger patients, such as younger children having less control over what they eat. However, comparison of our findings to the general population is difficult due to limited studies on postpandemic prevalence of ADHD and eating disorders. Further investigation is needed to determine if the prevalence in patients with obesity follows the same pre- and postpandemic trends as the general population.
Most postpandemic mental health literature focuses on only anxiety and depression.46,47 Despite inclusion of mood, anxiety, and psychotic symptoms and disorders in our study, our findings showed lower rates of mental health disorders and symptoms compared with global and national estimates of depressive and anxiety symptoms.46,47 Children and adolescents with familial support enabling access to a pediatric weight management clinic may be better able to address psychosocial factors contributing to mental health disorders. However, our study found that non-Hispanic patients and patients ages 10 to <14 years of age had increased odds of postpandemic mood/mental health disorder diagnosis. The impact of age may be due to increased influence of external factors, such as social media,30,48 biological factors, 49 or a combination. Meanwhile, mental health disorders have disproportionately impacted children and adolescents from higher-income households during the postpandemic period, 50 which may contribute to the observed effect of race on mental health.
Limitations of our study include lack of a control group, referral bias, medical provider variations in charting, potentially incomplete or missing documentation, and human error. In addition, most postpandemic data came from in-person visits, as many telemedicine visits lacked anthropometric measures, and not all telemedicine visits were retrievable. Lastly, not all patients had lab studies within the defined study period time range, fasting states could not be verified for some of the lab studies, and BP was not uniformly measured and observed across multiple visits as is recommended by clinical practice guidelines. 26
Conclusions
COVID-19 is associated with increased severity of obesity classification and higher prevalence of comorbidities in new patients presenting to a pediatric weight management clinic, with effects lasting at least 3 years after the pandemic onset. It is also associated with increased odds of diagnosis of prediabetes, ADHD, eating disorder/hyperphagia, and mood/mental health disorders in select demographic subgroups. Further research is needed to determine the complex interplay between COVID-19, pediatric obesity, and comorbidity prevalence that would inform targeted interventions addressing the worsening pediatric obesity epidemic. Future perspectives for this study include comparing rates of psychiatric disorders pre- and postpandemic in demographic and socioeconomic status matched patients with and without obesity.
Author Contributions
SMH: Investigation (lead); writing—original draft (lead); writing—review and editing (equal); formal analysis (supporting).
PD: Formal analysis (lead); writing—review and editing (equal).
NM: Conceptualization (lead); writing—review and editing (equal).
Footnotes
Acknowledgements
We thank Tamara John, MPH, CPHQ, for her assistance in data retrieval.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sector. The George Washington University School of Medicine and Health Sciences Health Services Summer Scholarship awarded to SH helped fund research efforts for this study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.