
Abstract
Retrospective cohort study evaluating the association between time to antibiotic administration and clinical outcomes in pediatric sepsis using data from 6153 patients treated at 19 pediatric emergency departments between 2013 and 2016. Time to antibiotics was analyzed both as a continuous variable and as a dichotomized variable (≤60 vs >60 minutes from sepsis time zero). The primary outcome was 3- and 30-day all-cause mortality; secondary outcomes included use of vasoactive agents and intensive care unit and hospital length of stay. In adjusted analyses, longer time to antibiotics was associated with lower 30-day mortality but not with 3-day mortality or other secondary outcomes. Patients receiving antibiotics more than 60 minutes from recognition had a significantly lower risk of 30-day mortality. These findings suggest that rigid time-based antibiotic thresholds may not align with improved outcomes in pediatric sepsis and underscore the need for prospective studies to inform future guidelines.
Introduction
Pediatric sepsis remains a leading cause of morbidity and mortality in pediatric patients worldwide. Despite advances in critical care medicine, pediatric severe sepsis continues to affect approximately 1.2 million children annually with mortality rates ranging from 9% to 25%, depending on geographic location and available resources.1-6 Early recognition and prompt intervention are considered cornerstones of effective sepsis management. Current guidelines from the Surviving Sepsis Campaign and the American College of Critical Care Medicine recommend administration of broad-spectrum antibiotics within 1 hour of sepsis recognition.7,8 However, the evidence supporting the 1-hour antibiotic timing recommendation in pediatric populations remains limited and inconsistent. While several studies have demonstrated the benefits of early antibiotic administration in adult sepsis,9,10 the pediatric literature shows conflicting results. Some studies suggest improved outcomes with antibiotics administered within 1 hour, 11 while others have found no significant benefits until hours later in care of these patients.12,13
To address this gap in knowledge, we conducted a multicenter analysis using retrospective data from the Pediatric Septic Shock Collaborative (PSSC) to examine the relationship between antibiotic timing and outcomes in children with sepsis. By analyzing data from 19 pediatric emergency departments (EDs) across the United States, we sought to determine whether the currently recommended 1-hour window for antibiotic administration is associated with changes in survival and other clinical outcomes. This study represents one of the largest examinations of antibiotic timing in pediatric sepsis to date and provides real-world evidence to inform clinical practice guidelines and future prospective research design in this area.
Methods
Study Design and Setting
The PSSC was formed by a group of investigators within the Section of Emergency Medicine in the American Academy of Pediatrics (AAP) in collaboration with the Children’s Hospital Association (CHA). Experts in pediatric sepsis care with diverse, multidisciplinary backgrounds developed a comprehensive change package that was consistent with evidence-based guidelines that included sepsis-screening tools, educational resources, shared sepsis definitions, and recommended consistent data definition although individual sites could implement identification as their resources dictated.14,15 The key drivers of care included rapid recognition, escalation of care, first hour resuscitation goals, and transfer of care.
The PSSC was comprised of 19 US-based pediatric EDs. The ED sites had a median of 52300 (interquartile range [IQR] = 33000, 69100) annual visits. The affiliated hospitals, the majority (63%) of which were freestanding children’s hospitals, had a median of 289 (IQR = 159, 329) inpatient beds and 36 (IQR = 23, 43) intensive care unit (ICU) beds. Physician and nursing champions led the efforts at each local site. These leaders from across the collaborative used established models to collaborate in monthly virtual webinar sessions and twice annually at half-day, in-person sessions at national conferences. 16
Selection of Participants
The study period was from November 1, 2013 until May 31, 2016. The PSSC defined cases of presumed septic shock in ED patients at collaborative sites with any of the following a priori criteria: (1) any International Classification of Diseases codes consistent with severe sepsis or septic shock, (2) a positive sepsis screening tool plus treatment with a sepsis care bundle (defined as ≥1 parenteral antibiotic, ≥2 boluses of isotonic fluid, and obtainment of a blood culture), (3) sepsis care bundle treatment plus any of the following: use of vasoactive agent, lactate assessment, or ICU admission (directly from the ED or any floor-to-ICU transfers within 12 hours of ED admission), or (4) use of a septic shock order set. Patients were excluded from the collaborative database if they had already received antibiotics or 2 fluid boluses prior to ED arrival.
This time frame corresponds to the active data collection period of the Pediatric Septic Shock Collaborative (PSSC), during which standardized definitions and data elements were used across all participating sites to ensure internal consistency. The collaborative concluded in 2016 and later informed the development of the Children’s Hospital Association Improving Pediatric Sepsis Outcomes (IPSO) initiative.
For this post hoc analysis of an existing database of patients, we include children with an age between 2 months and 21 years old. Infants younger than 2 months were excluded because their evaluation and management for possible sepsis are highly standardized, including nearly universal recommendations for empiric antibiotic administration, making them distinct from the broader pediatric population. The upper age limit of 21 years was defined by the PSSC and reflects the typical cutoff used by pediatric EDs and children’s hospitals, consistent with prior literature. 17 We excluded any patients with missing antibiotic administration timestamp data or sepsis time zero, as well as those who had received antibiotics before the sepsis criteria were met.
Interventions and Measurements
Site leaders screened their electronic health record for included ED cases and entered data for all included patients into a central, password-protected, data portal. The collaborative identified a priori data elements to be collected and standardized the definition for data elements, required submission of all data related to the primary outcomes, and had quality assurance logic checks to ensure appropriate data entry. Additional data on the collaborative’s secondary outcomes were also collected, as resources for data entry allowed, at each site. Data related to antibiotic administration included antibiotic initiation timestamps. Per PSSC definitions, a patient was classified as having an underlying medical condition if they had any of the following on review of their electronic health record: oncologic disease, sickle cell disease or asplenia, solid organ transplant, other hematologic or immunologic disorders, neuromuscular or cognitive impairment, epilepsy, gastrointestinal or liver disease, pulmonary disease, cardiac disease, renal disease, endocrine or metabolic disorder, rheumatologic condition, bone marrow transplant, malignancy, central venous access device, complex urogenital repair, neurologic dysfunction, or other forms of immunocompromise. 18 The PSSC and participating sites obtained institutional review board approvals and/or waivers (Baylor College of Medicine H23511). 18
Sepsis time zero was previously defined by the PSSC. 18 The antibiotic administration time was calculated as minutes from sepsis time zero.
As it has been recommended that antibiotics be administered < 60 min in children with concern for sepsis, 7 we dichotomized antibiotic timing as a predictor variable of ≤60 minutes versus >60 minutes. We also analyzed if antibiotic timing as a continuous variable was associated with the outcomes.
The primary outcome was 3-day and 30-day aggregate mortality during the index admission from any cause. Secondary outcomes included administration of any vasoactive agent (dopamine, norepinephrine, epinephrine, vasopressin, or milrinone), pediatric ICU length of stay (pLOS), and hospital length of stay (hLOS). We adhered to the Strobe guidelines for the reporting of observational studies.
Statistical Analysis
Differences in descriptive variables were analyzed using χ2 (binomial variables) or Wilcoxon Rank-Sum (continuous variables) as appropriate. Outcomes were analyzed using multivariable binominal regression (binomial outcomes) or quantile regression (continuous outcomes, skewed) as appropriate. The multivariable model included age, sex, and presence of an underlying medical condition as chosen a-priori. It also included hypotension at triage, which was found to be independent predictor of mortality on univariate analysis. Study site was included as a fixed effect to account for clustering across the participating pediatric EDs. Patients with missing sepsis recognition time or antibiotic administration timestamp were excluded, as these were required to calculate time to antibiotics. For other variables, the extent of missingness is shown in Tables 1–3. Regression models were performed using complete-case analysis. For binary outcomes, relative risks (RR) with 95% confidence intervals (CIs) were reported, while for continuous outcomes, median differences (MDs) in time with IQRs were provided. Statistical significance was defined as a P value less than .05. Data were analyzed using Stata Statistical Software: Release 17. 19
Baseline Demographics by Mortality Outcome.
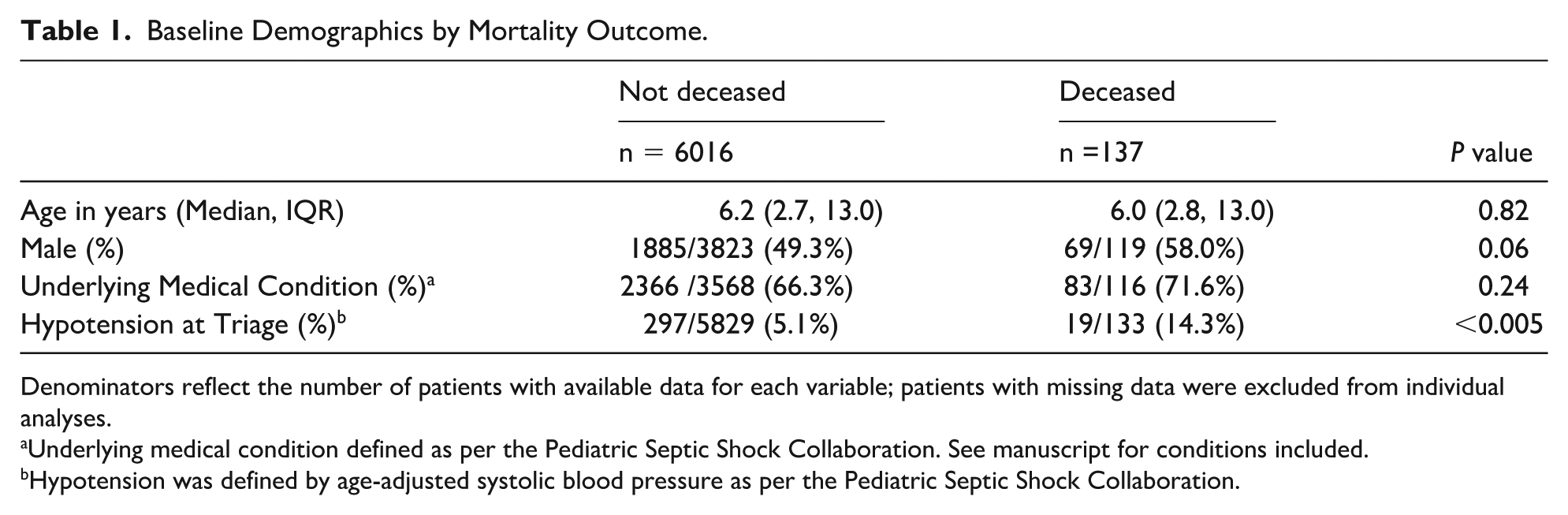
Denominators reflect the number of patients with available data for each variable; patients with missing data were excluded from individual analyses.
Underlying medical condition defined as per the Pediatric Septic Shock Collaboration. See manuscript for conditions included.
Hypotension was defined by age-adjusted systolic blood pressure as per the Pediatric Septic Shock Collaboration.
Patient Characteristics Stratified by Time to Antibiotic Administration.
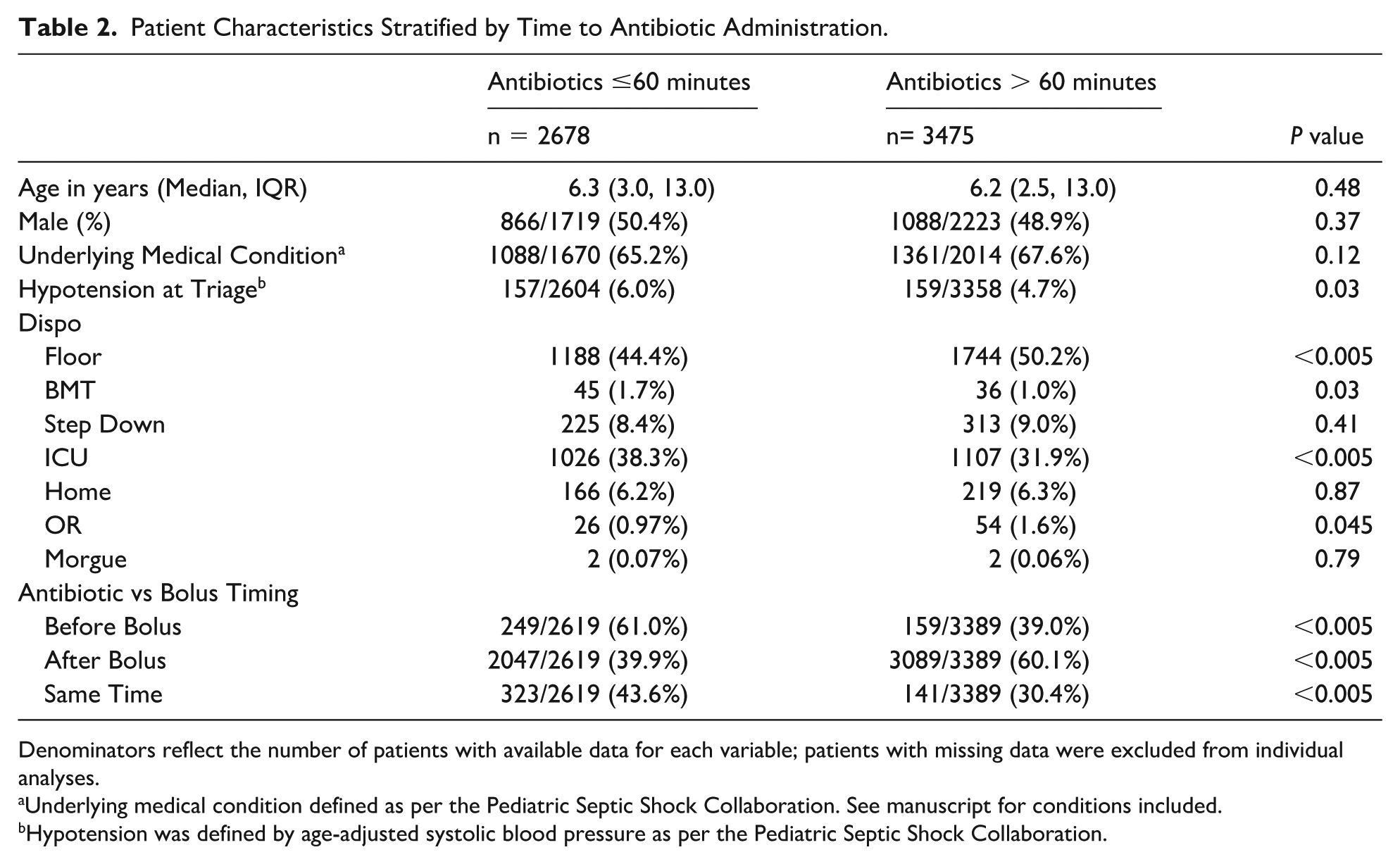
Denominators reflect the number of patients with available data for each variable; patients with missing data were excluded from individual analyses.
Underlying medical condition defined as per the Pediatric Septic Shock Collaboration. See manuscript for conditions included.
Hypotension was defined by age-adjusted systolic blood pressure as per the Pediatric Septic Shock Collaboration.
Adjusted Outcomes by Time to Antibiotic Administration.
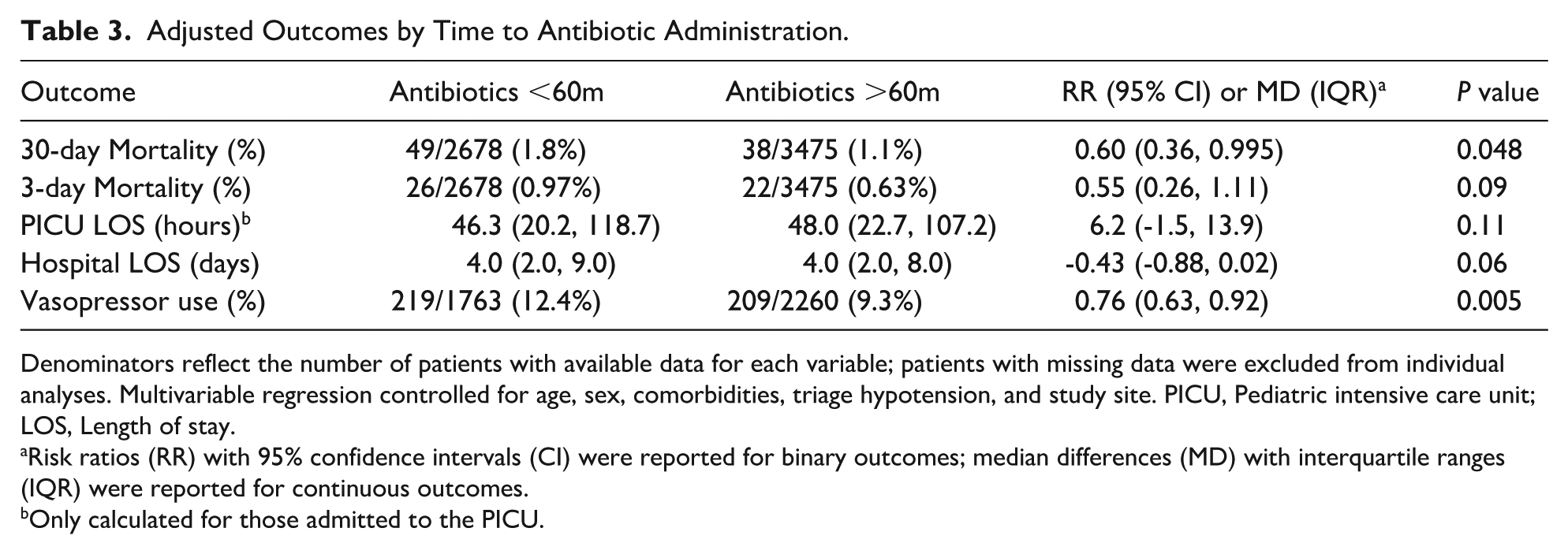
Denominators reflect the number of patients with available data for each variable; patients with missing data were excluded from individual analyses. Multivariable regression controlled for age, sex, comorbidities, triage hypotension, and study site. PICU, Pediatric intensive care unit; LOS, Length of stay.
Risk ratios (RR) with 95% confidence intervals (CI) were reported for binary outcomes; median differences (MD) with interquartile ranges (IQR) were reported for continuous outcomes.
Only calculated for those admitted to the PICU.
Results
Characteristics of Study Subjects
The PSSC database contained 6674 pediatric sepsis patients between 2 months and 21 years of age. ED sites had a median of 187 sepsis cases (IQR = 93, 411) and the percent admitted to the ICU was 43% (IQR = 24%, 55%) with a median hLOS of 4.0 days (IQR = 2.0, 8.0) and a 30-day mortality of 1.7% (IQR = 1.2%, 3.3%).
Of the 6674 patients, 2 (0.03%) were excluded for lack of sepsis timing data; 263 (3.9%) were excluded because they did not receive antibiotics or this information was missing; 8 (0.1%) were excluded due to the timing of antibiotics not being recorded; and 248 (3.7%) were excluded because they received antibiotics before meeting criteria for sepsis.
A total of 6153 patients remained for analysis (Table 1). The median age was 6.2 years (IQR = 2.7, 13.0), 49.6% were reported as male, and 66.5% had an underlying medical condition (Supplemental Table 1).
Primary Outcome
A total of 137 children (2.2%) died: 48 (0.8%) within 3 days and 87 (1.4%) within 30 days from the index admission. Demographics for patients who died vs. survived are shown in Table 1. While age, sex, and presence of an underlying medical condition were not statistically different, patients who were hypotensive at triage were more likely to die (P < .005). Mortality varied significantly by hospital site, median 1.9%, IQR (1.2%, 5.5%); P < .005.
In univariate analysis to determine co-variates, age (r2 = 0, P = .52) and sex (P = .80) were not found to be significantly correlated with timing of antibiotics as a continuous variable. However, they were retained in the multivariable model as they were chosen a priori based on clinical knowledge. Presence of an underlying medical condition (P < .005) and study site (P < .005) were significantly associated with antibiotic timing, supporting their inclusion in subsequent outcome analyses. Although hypotension at triage was not significantly associated with antibiotic timing (P = .21), its established association with mortality justified its inclusion in the multivariable model (Table 2).
On multivariable regression analysis, 30-day mortality was significantly correlated with time to antibiotics as a continuous variable (P = .03). Specifically, for every 1-minute increase in time to antibiotics, the relative risk of 30-day mortality decreased by 0.5% (RR = 0.995 [95% CI = 0.990-.999]). There was no association between antibiotic timing as a continuous variable and 3-day mortality (P = .08).
Multivariable regression analysis of antibiotic timing as a dichotomous variable (≤60 minutes vs >60 minutes) showed that children who received antibiotics in >60 minutes had a lower risk of 30-day mortality (RR = 0.60 [0.36-0.995]). There were no differences in 3-day mortality (Table 3).
Secondary Outcomes
For the entire cohort, the median pLOS for those who were admitted to the ICU was 47.1 hours (IQR = 21.6, 112.0) and the median hLOS was 4.0 days (IQR = 2.0, 9.0). A total of 428 (10.6%) of children required vasopressors of the 4023 observations that reported this outcome.
As a continuous variable, timeliness of antibiotics was not associated with pLOS (P = .20), hLOS (P = .07), or the need for a vasoactive agent (P = .12).
As a dichotomous variable, there were no differences between pLOS (P = .11) or hLOS (P = .06) for children who received antibiotics in ≤60 minutes versus >60 minutes. However, for patients who received antibiotics >60 minutes after sepsis time zero, the relative risk of needing vasopressors was 0.76 (IQR = 0.63, 0.92) compared with those treated in ≤60 minutes (Table 3).
We conducted a secondary analysis to assess whether the timing of the first fluid bolus influences the timing of antibiotic administration and its impact on outcomes (Table 2). The time to antibiotics from patient sepsis time zero was significantly different (P < .005) if the antibiotic was received before the first bolus (47.0 minutes [29.0, 86.5]), at the same time as the first bolus (40.5 minutes [24.0, 66.5]), or after the first bolus (73.0 minutes [47.0, 140.0]). Linear regression analysis showed that time to bolus was a significant predictor of time to antibiotic (r2 =0.37, p=<0.005). We did not control for time to bolus in the initial outcome analyses due to concerns about potential collinearity. However, we re-ran the analyses controlling for the timing of bolus administration relative to antibiotics (before/during/same time), and none of the results were significantly affected by the inclusion of this covariate. Additionally, neither time to bolus (P = .06) nor timing relative to antibiotics (P = .07) were independently associated with 30-day mortality.
Discussion
In this multicenter pediatric sepsis quality collaborative, longer times from sepsis recognition to antibiotic administration were associated with decreased 30-day any-cause mortality. Our results held when examining time to antibiotics as both continuous and dichotomous (≤ 60 versus > 60 minutes) variables. These findings were independent of first fluid bolus timing.
Current pediatric sepsis guideline recommendations call for antibiotics to be administered “as soon as possible, within 1 hour of recognition.” 7 However, many of the studies used to support this recommendation primarily analyzed the use of sepsis bundles, including antibiotics and fluid boluses, instead of examining bundle elements individually.20-23 Moreover, some of these studies employed bundles with a more generous time window for antibiotics or demonstrated no differences in mortality. 23 While Evans et al 24 found that bundle compliance was associated with lower risk-adjusted in-hospital mortality, none of the individual bundle elements, including antibiotics within 1 hour, were significant. Similar findings from the febrile neutropenia literature also suggest that strict adherence to a 60-minute benchmark for antibiotic administration may not be necessary for all pediatric patients, particularly those without severe illness at presentation.25-27
The few pediatric studies that have focused on antibiotic timing and mortality in pediatric sepsis have yielded somewhat conflicting results. A single-center study by Sankar et al demonstrated that antibiotic administration in less than 1 hour from recognition was associated with decreased in-hospital mortality in pediatric sepsis. Interestingly, when dichotomizing antibiotic timing at 2 hours, mortality did not differ. 11 Weiss et al 12 explored antibiotic delays in pediatric sepsis and found that only timing beyond 3 hours from sepsis recognition was significantly associated with PICU mortality, even when controlling for illness severity.
A recent multicenter study from the Improving Pediatric Sepsis Outcomes collaborative sought to determine the association of antibiotic timing with 3-day and 30-day sepsis-attributable mortality for all children with sepsis. 13 In contrast to guidelines and the similar studies, they found that time from ED arrival to antibiotic administration was only associated with increased mortality (both 3-day and 30-day) beyond 330 minutes from sepsis recognition. Furthermore, children who received antibiotics in less than 30 minutes had higher mortality. Creedon et al 28 showed similar increased mortality in a single site study of patients who presented to the ED with septic shock and received antibiotics <60 minutes versus > 60 minutes. It is possible that in these studies, as well as in ours, children who received antibiotics more quickly were those who appeared more critically ill at presentation, prompting faster recognition and treatment. This likely reflects confounding by indication, where the sickest patients are treated most urgently yet have inherently higher mortality risk regardless of treatment timing. In the absence of consistent information about clinical severity, this counterintuitive pattern cannot be fully accounted for.
Although our results did not reveal an association between antibiotic timing and 3-day mortality, our findings add to the body of literature that calls into question the 1-hour recommendation for antibiotic administration in pediatric sepsis. Altogether, these results suggest that prospective studies examining antibiotic administration at distinct time intervals, especially beyond the 1-hour recognition mark, are warranted.
Our study is subject to several limitations beyond those inherent to retrospective analyses. Our study setting was limited to US-based pediatric EDs, and as such, findings may not be generalizable outside the United States, especially in more resource-limited areas. Case inclusion as defined by the PSSC was intentionally broad and potentially limited by use of diagnostic code 29 ; thus, our analysis included subjects across the spectrum of clinical severity for pediatric sepsis. The PSSC database did not include consistent data on illness severity; although we could not directly control for sepsis severity in our analyses, we did analyze several proxies to try to account for this limitation. While triage hypotension was not associated with mortality in our cohort, subjects who received vasopressors were more likely to receive antibiotics in <60 minutes, which could indicate that these patients were deemed more severely ill at the beginning of their clinical course. As the PSSC was a quality collaborative, sample sizes were not calculated, and it is therefore possible that differences in 3-day mortality or LOS exist with differing antibiotic administration times. In addition, our study was not designed to determine an optimal antibiotic timing threshold, and the limited number of mortality events precluded exploration of nonlinear relationships that might better characterize this association. Lastly, the study period predates more recent sepsis guidelines and quality improvement initiatives, which may limit generalizability to current practice patterns. However, there have been no new therapeutics or major changes in the acute management of pediatric sepsis during this time, and timely antibiotic administration remains a cornerstone of current sepsis care.
In conclusion, in this multicenter study of antibiotic timing in pediatric sepsis, longer times from sepsis recognition to antibiotic administration were associated with lower 30-day mortality rates. Prospective studies are warranted to examine different antibiotic timing intervals and their potential impact on outcomes in pediatric sepsis.
Author Contributions
A.B. contributed to the conception and design of the study, performed data analysis and interpretation, and drafted the manuscript. C.P., P.M., and E.M. contributed to the conception and design of the study and to data acquisition and interpretation, and critically revised the manuscript for important intellectual content. All authors approved the final manuscript and agree to be accountable for all aspects of the work, ensuring its integrity and accuracy.
Supplemental Material
sj-docx-1-cpj-10.1177_00099228251407402 – Supplemental material for Reevaluating the 1 Hour Benchmark: Associations Between Antibiotic Timing and Mortality in Pediatric Sepsis
Supplemental material, sj-docx-1-cpj-10.1177_00099228251407402 for Reevaluating the 1 Hour Benchmark: Associations Between Antibiotic Timing and Mortality in Pediatric Sepsis by Alexandra H. Baker, Christopher M. Pruitt, Paul C. Mullan and Elliot Melendez in Clinical Pediatrics
Footnotes
Ethical Considerations
The PSSC and participating sites obtained institutional review board approvals and/or waivers (Baylor College of Medicine H23511).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available through the Pediatric Septic Shock Collaborative. Access to the dataset is not at the discretion of the authors and may be requested directly from the Collaborative.
Supplemental Material
Supplemental material for this article is available online.