
Abstract

Educational Objectives
Recognize and differentiate the clinical and radiologic features of acute cerebellitis in pediatric patients, emphasizing the importance of early imaging and lumbar puncture in patients with fever, new-onset ataxia, and symptoms of intracranial hypertension.
Discuss the diagnostic approach and management strategies for suspected post-infectious cerebellitis, including the role of serologic testing, empiric treatment, and immunomodulatory therapy such as steroids when CNS infection is ruled out.
Case Report
A 13-year-old male with a medical history of attention-deficit hyperactivity disorder (ADHD) presented with a 1-week history of persistent headaches, nausea, vomiting, dizziness, and new-onset ataxia following recent pharyngitis, which was treated with intramuscular penicillin G. The patient denied experiencing visual disturbances, double vision, difficulty swallowing, hearing changes, or photophobia.
Physical examination revealed an afebrile adolescent with a heart rate of 87 beats/min, respiratory rate of 20 breaths/min, blood pressure of 143/92 mm Hg, and oxygen saturation of 97%. His weight was 123 lb14.4 oz (56.2 kg), and height 5′ 3.39″ (161 cm). He was alert and oriented to time, place, and person. Eye examination was notable for papilledema. Cranial nerve examination was normal, with no signs of nystagmus, tremors, dysmetria, or slurred speech. There was no photophobia. The neck was supple with no Brudzinski sign. No signs of adenopathy were noted. Oropharynx was clear. Lung auscultation was clear, and the heart showed no murmurs, rubs, or gallops. The abdominal examination was unremarkable with no tenderness, rebound, or guarding, and there were no masses or hepatosplenomegaly. Despite the reported swaying in his gait, no ataxia was observed on examination, with negative Romberg, finger-to-nose, and heel-to-shin testing.
Given the presence of papilledema, a computed tomography (CT) scan of the head and cervical spine without intravenous (IV) contrast was obtained. Computed tomography scan revealed no acute intracranial abnormalities, fractures, or malalignment. A lumbar puncture was performed, yielding colorless, clear cerebrospinal fluid (CSF) with a total nucleated cell count of 129/μL, elevated total protein of 82 mg/dL, and glucose of 55 mg/dL. Cerebrospinal fluid cultures and Gram stain showed no bacterial growth. Cerebrospinal fluid meningitis/encephalitis polymerase chain reaction (PCR) panel was negative. Magnetic resonance imaging (MRI) of the brain with and without IV contrast revealed bilateral cerebellar T2 hyperintensity, mild leptomeningeal enhancement, fourth ventricular effacement, and early obstructive hydrocephalus (Figure 1). Magnetic resonance imaging of the cervical, thoracic, and lumbar spine revealed no abnormal enhancement in the spinal canal. Laboratory results showed leukocytosis (11.17 × 10³/μL) with a left shift in neutrophils (80%). C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR) were normal. Lactate dehydrogenase (LDH) was 186 U/L, and uric acid was elevated to 7.9 mg/dL.
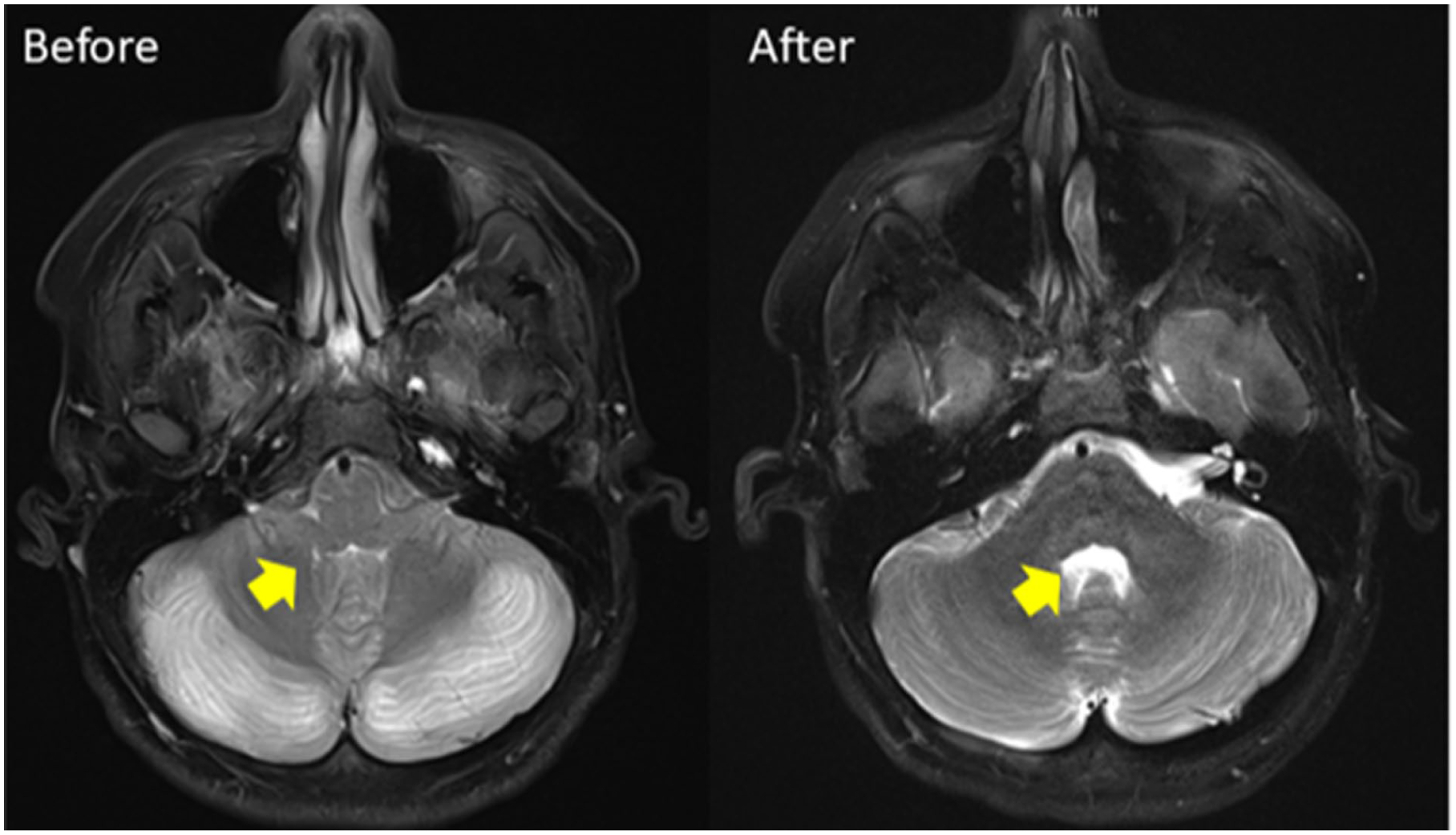
Head MRI before and after steroid treatment.
Discussion
Differential Diagnosis
The initial differential diagnosis for acute ataxia was broad, including intracranial tumors, abscesses, intoxication, metabolic disorders, hereditary degenerative diseases, meningitis, encephalitis, acute cerebellar ataxia, and acute disseminated encephalomyelitis (ADEM). 1
Meningitis was initially suspected, as CSF analysis demonstrated pleocytosis consistent with inflammation; however, the meningitis PCR panel returned negative. After obtaining cultures, empiric therapy with vancomycin, ceftriaxone, and acyclovir was initiated and maintained until an infectious cause was considered unlikely. In the context of MRI findings demonstrating cerebellar swelling and hydrocephalus, acute cerebellitis emerged as the leading diagnosis, given its potential to compress posterior fossa structures, acute hydrocephalus, and intracranial hypertension.2-4
The Condition: Acute Cerebellitis
Acute cerebellitis is a rare condition in children and adolescents, often triggered by infection or immune-mediated processes. The clinical presentation can range from mild, self-limiting symptoms to fulminant cerebellitis, which carries a higher risk of morbidity and mortality. Common symptoms include ataxia, dysmetria, dysarthria, nystagmus, tremors, slurred speech, and elevated intracranial pressure, resulting in headaches, vomiting, and changes in consciousness.4-9
The cause of acute cerebellitis remains unknown in nearly two-thirds of cases. However, infections, particularly viral agents, are responsible for about one-third of cases. Common pathogens include Epstein-Barr virus (EBV), Coxsackie B3, and respiratory syncytial virus (RSV). Bacteria, such as Streptococcus pneumoniae and Mycoplasma pneumoniae, have also been implicated. Other infectious agents include varicella zoster virus (VZV), herpes simplex virus-1 (HSV-1), influenza, rotavirus, cytomegalovirus (CMV), West Nile virus, Borrelia burgdorferi, and Salmonella typhi.1,4,9-12
Emerging evidence supports immune-mediated pathogenesis in some cases. Autoantibodies against neuronal antigens such as metabotropic glutamate receptor 1 (mGluR1), glutamate receptor delta 2 (GluRδ2), and myelin-oligodendrocyte glycoprotein antibody-associated diseases (MOGAD) have been identified in serum and CSF. These findings suggest post-infectious immune activation may contribute to cerebellar inflammation, often following respiratory or viral illness such as pharyngitis, although the pathogenic role of some autoantibodies remains under investigation and not all are clearly disease causing.13-15
Although many cases of acute cerebellitis are mild and self-limited, approximately 10% to 25% follow a moderate-to-severe course, with a subset developing life-threatening complications such as obstructive hydrocephalus, brainstem compression, or herniation due to increased intracranial pressure.5,16-18 Hospitalists should monitor for altered mental status, progressive ataxia, or new cranial nerve deficits by serial neurological examination.
The management of cerebellitis in children remains an area of ongoing discussion, with treatment strategies generally focused on addressing the underlying pathophysiology. This often includes the use of steroids and/or intravenous immunoglobulin (IVIG) to manage cerebellar swelling. In more severe cases, surgical interventions such as ventriculostomy, external ventricular drainage, ventriculoperitoneal shunt placement, or posterior fossa decompression may be necessary, particularly in the presence of obstructive hydrocephalus. Early administration of steroids may help prevent the need for surgical intervention. However, there is no established consensus regarding the type, dosage, and duration of steroid therapy.6,19-24
In addition, broad-spectrum antibiotics and/or antivirals are commonly administered to treat any potential concurrent central nervous system infections.
Hospital Course
In this case, an extensive workup was performed to evaluate potential infectious, autoimmune, and malignancy-related causes. Cerebrospinal fluid testing for cryptococcal antigen was negative, and serological tests for Bartonella, syphilis, and M pneumoniae were also negative. However, serum Mycoplasma IgG and IgM were positive, indicating a recent infection, although PCR for M pneumoniae in the CSF was negative. Initial blood cultures grew coagulase-negative staphylococci, but contamination was suspected, and repeat cultures were negative. Polymerase chain reaction tests for respiratory viruses, including HSV, CMV, and VZV, were all negative.
To assess an autoimmune process, tests for myelin oligodendrocyte glycoprotein (MOG-IgG1), neuromyelitis optica spectrum disorder NMO (NMOSD)/Aqp4 associated with aquaporin-4 (AQP4) antibodies, and glutamic acid decarboxylase (GAD65) were conducted, which showed negative findings. These studies were intended to exclude key entities within the differential diagnosis rather than to provide a comprehensive evaluation for autoimmune encephalitis or autoimmune cerebellitis. Notably, the patient’s clinical presentation, imaging findings, and overall course were not suggestive of autoimmune encephalitis based on the evaluation from the pediatric neurology team. Given the low clinical suspicion, additional neuronal antibody testing was not pursued, as it was unlikely to change diagnostic assessment or management. Furthermore, the pathogenic role of several reported neuronal autoantibodies remains incompletely established, and not all are clearly disease causing. The presence of cerebellar edema and hydrocephalus raised concerns for malignancy, such as lymphoma. To rule this out, an MRI of the cervical, thoracic, and lumbar spine was performed, which showed no abnormal enhancement in the spinal canal.
Final Diagnosis
Despite negative Mycoplasma CSF PCR, the positive serum Mycoplasma IgG and IgM suggested an acute infection. Schmucker et al 25 have reported cases of cerebellitis associated with M pneumoniae based on serology despite negative CSF PCR, highlighting the importance of serological testing in such cases.
Al-Zaidy et al 26 propose 2 mechanisms for M pneumoniae-associated neurological disease: direct central nervous system (CNS) infection and an immune-mediated response. Komatsu et al 27 have also suggested that antiganglioside antibodies may play a role in the immune-mediated mechanism. Since this patient had positive serology and these findings, it supports the diagnosis of post-infectious cerebellitis likely via immune-mediated response of M pneumoniae rather than direct CNS infection or primary autoimmune encephalitis.
The patient was treated empirically with vancomycin, ceftriaxone, and acyclovir until infectious studies returned negative. Following the initiation of IV methylprednisolone, there was significant clinical improvement, with resolution of headache, nausea, vomiting, and ataxia. After 5 days of IV methylprednisolone, a follow-up MRI showed complete resolution of cerebellar edema and fourth ventricular effacement. The patient returned to baseline and did not require rehabilitation.
Unfortunately, there was insufficient CSF to run additional autoimmune or encephalitis panels. Given the patient’s improvement and the resolution of inflammation on imaging, further lumbar puncture was deemed unnecessary. If symptoms recur, additional testing, including a repeat lumbar puncture, will be considered.
Conclusion
This case highlights the diagnostic and therapeutic challenges associated with acute cerebellitis in children. In a patient with recent pharyngitis and new neurologic symptoms, the differential diagnosis is broad, but cerebellitis must be considered, especially when imaging reveals cerebellar inflammation and hydrocephalus.
While CSF analysis is important, a negative infectious workup does not exclude post-infectious causes. Positive Mycoplasma pneumoniae serology in the setting of neurologic symptoms and MRI findings supports an immune-mediated cerebellitis, a diagnosis that has been increasingly recognized in recent literature.
Clinicians should maintain a high index of suspicion for infectious or autoimmune conditions in cases of acute ataxia, and early laboratory evaluation is important for proper diagnosis and management.
Author Contributions
Ito M drafted the majority of the manuscript, conducted the literature review, and organized the core structure. Wheeling K contributed to the patient’s clinical management and provided critical revision of the manuscript. As the attending physician responsible for the patient’s primary clinical management, Chaudry T provided senior authorship, intellectual oversight, and substantive editing of the manuscript. Reusche C and Edwards M contributed substantive editing and approved the final version.
Footnotes
Acknowledgements
The authors thank the pediatric wards group including Dr Richard Wheeling at University of Kentucky for their contribution.
Ethical Considerations
Our institution does not require ethical approval for reporting individual cases or case series.
Informed Consent for Ethnographic Research
Written informed consent to participate in this study was provided by the participants’ legal guardians/next of kin.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.