
Abstract
Lichen sclerosus (LS) is a chronic inflammatory dermatosis that is frequently underdiagnosed in pediatric patients, especially girls presenting with persistent urinary symptoms. We aimed to characterize the clinical features and treatment outcomes in children with LS who presented with urinary symptoms. This retrospective study evaluated 88 children diagnosed with LS at a pediatric nephrology center, all of whom presented with urinary symptoms. Diagnosis was based on clinical and dermatoscopic findings. The mean age at diagnosis was 6.0 years, with a median delay of 8 months. Dysuria (79.5%) and pyuria (87.5%) were the most common symptoms, although only 45.5% had confirmed urinary tract infections. Among 60 patients followed (mean duration = 16.8 months), topical pimecrolimus resolved symptoms in 88.3% and improved skin lesions in 66.6%. Lichen sclerosus should be included in the differential diagnosis for children with urinary symptoms. Clinical awareness and early diagnosis can lead to avoiding unnecessary investigations.
Introduction
Lichen sclerosus (LS) is a chronic inflammatory dermatosis that primarily affects the anogenital region, leading to epidermal atrophy, architectural distortion, and scarring. Although its exact pathogenesis remains unclear, contributing factors may include genetic predisposition, autoimmune processes, hormonal influences, infections, and mechanical trauma such as bicycle riding or frictional irritation.1-3
Lichen sclerosus affects individuals of all ages and sexes but shows a strong female predominance, with reported female-to-male ratios ranging from 1:1 to 10:1. In girls, LS displays a bimodal age distribution, peaking in the prepubertal and postmenopausal periods. Among children, LS is most commonly diagnosed in girls aged 4 to 6 years.1-3
In pediatric patients, especially girls, LS often presents with nonspecific urogenital symptoms such as dysuria, pruritus, vulvar pain, urinary incontinence, and recurrent urinary tract infections (UTIs). These symptoms are frequently misattributed to common pediatric urological conditions, leading to delays in diagnosis and unnecessary further invasive investigations, especially for recurrent UTIs. In addition, while symptoms may subside spontaneously after puberty, untreated LS may result in complications such as labial fusion, stenosis, or malignant transformation. 4
Timely recognition and treatment of LS is critical for symptom control, avoiding unnecessary invasive testing and preventing long-term sequelae. This study aimed to characterize the clinical features, diagnostic delays, and treatment outcomes of LS in children presenting with urinary complaints. Enhancing clinical awareness of LS in pediatric patients aims to minimize unnecessary invasive procedures.
Materials and Methods
Study Design and Participants
This retrospective study included 88 pediatric patients presenting with urinary symptoms to the Department of Pediatric Nephrology at Baskent University Adana Dr. Turgut Noyan Application and Research Center between 2018 and 2023. All patients were subsequently diagnosed with LS based on clinical and dermatoscopic evaluation. Urinary tract complaints included dysuria, pollakiuria refers to children who urinate 8 or more times per day, hematuria, and urinary incontinence, while genital symptoms included vulvar pruritis such as genital itching, whiteness, pain, and occasional bleeding. Symptom of whiteness is defined as a hypopigmented, pale, or porcelain-white discoloration of the affected genital skin observed during physical examination. Urinary tract infection is defined as urinary symptoms accompanied by significant bacteriuria (≥10⁵ CFU/mL of a single pathogen in a clean-catch urine sample or ≥104 CFU/mL of a single pathogen in a bladder catheterization), with or without pyuria. Pyuria is defined as ≥5 white blood cells per high-power field in centrifuged urine specimens examined under light microscopy.
Referrals to the Dermatology Department were made for suspected LS, and all patients were examined by the same experienced dermatologist. Additionally, 4 male patients initially referred to the Pediatric Surgery Department for phimosis were included following LS diagnosis. In accordance with pediatric guidelines, the skin biopsy was not performed, as the lesions were localized and responded to standard topical therapy. 5
Data Collection
Demographic data, clinical presentation, comorbidities, family history, diagnostic timelines, laboratory findings, treatment approaches, and outcomes were extracted from medical records. Diagnostic delay was defined as the time interval (in months) between the onset of symptoms reported by caregivers and the establishment of the LS diagnosis.
All patients received topical pimecrolimus as first-line therapy. Treatment response was monitored clinically. In cases of suboptimal response, therapy was escalated to topical tacrolimus or corticosteroids.
Statistical Analysis
Data were analyzed using SPSS version 25.0 (IBM Corp, Armonk, New York). Continuous variables were presented as means ± standard deviations or medians with interquartile ranges, based on distribution. Normality was assessed using the Kolmogorov-Smirnov and Shapiro-Wilk tests.
Ethical Approval
The study was approved by the Institutional Review Board of Baskent University (Project no: KA22/296) and supported by the university’s research fund.
Results
Demographic Data of Lichen Sclerosus Patients
Between January 2018 and December 2022, a total of 1018 pediatric patients presenting with urinary symptoms were evaluated for UTIs and voiding dysfunction at our center. Of these, 689 were female. Among the girls, 84 (12.2%) were diagnosed with LS. Including 4 boys diagnosed with LS due to phimosis, the total number of confirmed LS cases was 88.
The mean age at diagnosis was 6.06 ± 2.40 years. The median diagnostic delay (the time interval between the onset of symptoms and the establishment of LS diagnosis) was 8 months (mean = 8.42 ± 18.38 months). Contributing factors were identified in 78.4% of patients and included recurrent UTIs, mechanical trauma (eg, bicycle riding), comorbid autoimmune diseases, or a family history of LS or other autoimmune conditions (Table 1). Among the 9 patients with comorbid autoimmune disorders, autoimmune thyroiditis (n = 3), lichen planus (n = 2), and others (morphea, celiac disease, alopecia areata, psoriasis; n = 4) were reported. A positive family history of LS was noted in 3 patients; additional autoimmune conditions in relatives included autoimmune thyroiditis (n = 3), lichen planus (n = 2), psoriasis (n = 1), and alopecia areata (n = 1).
Demographic Data of LS Patients.
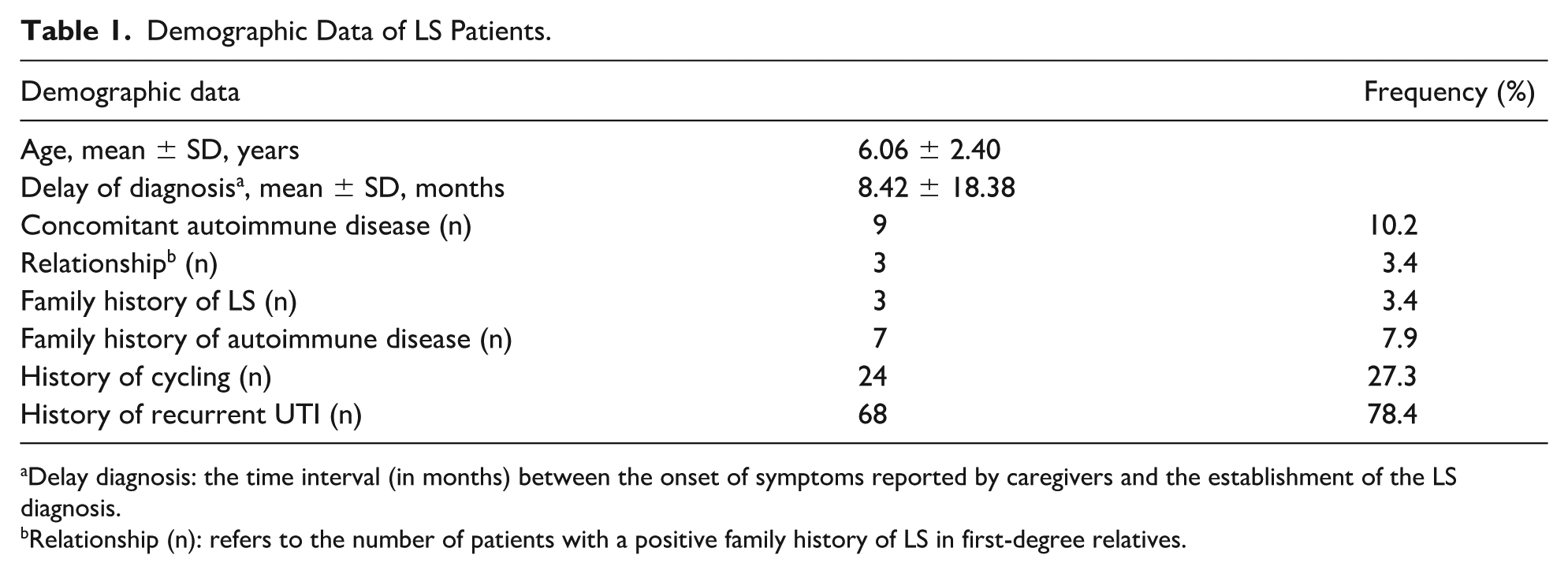
Delay diagnosis: the time interval (in months) between the onset of symptoms reported by caregivers and the establishment of the LS diagnosis.
Relationship (n): refers to the number of patients with a positive family history of LS in first-degree relatives.
Clinical Findings
Dysuria was the most frequently reported symptom, initially present in 79.5% of patients and eventually in 100% during the disease course. Other urinary complaints included increased frequency, hematuria, and incontinence. Genital symptoms included genital itching (78.4%), whiteness, and occasional bleeding.
At the time of diagnosis, pyuria was observed in 87.5% of patients; however, only 45.5% had culture-proven UTIs. Escherichia coli was the most commonly isolated pathogen (Table 2). Approximately 25% of patients experienced recurrent UTIs during follow-up. Dysfunctional voiding was identified in 7 patients, commonly accompanied by constipation and daytime incontinence. All 7 had Dysfunctional Voiding Symptom Scores (DVSSs) >9, indicating clinically significant dysfunction.
Clinical Findings of LS Patients.
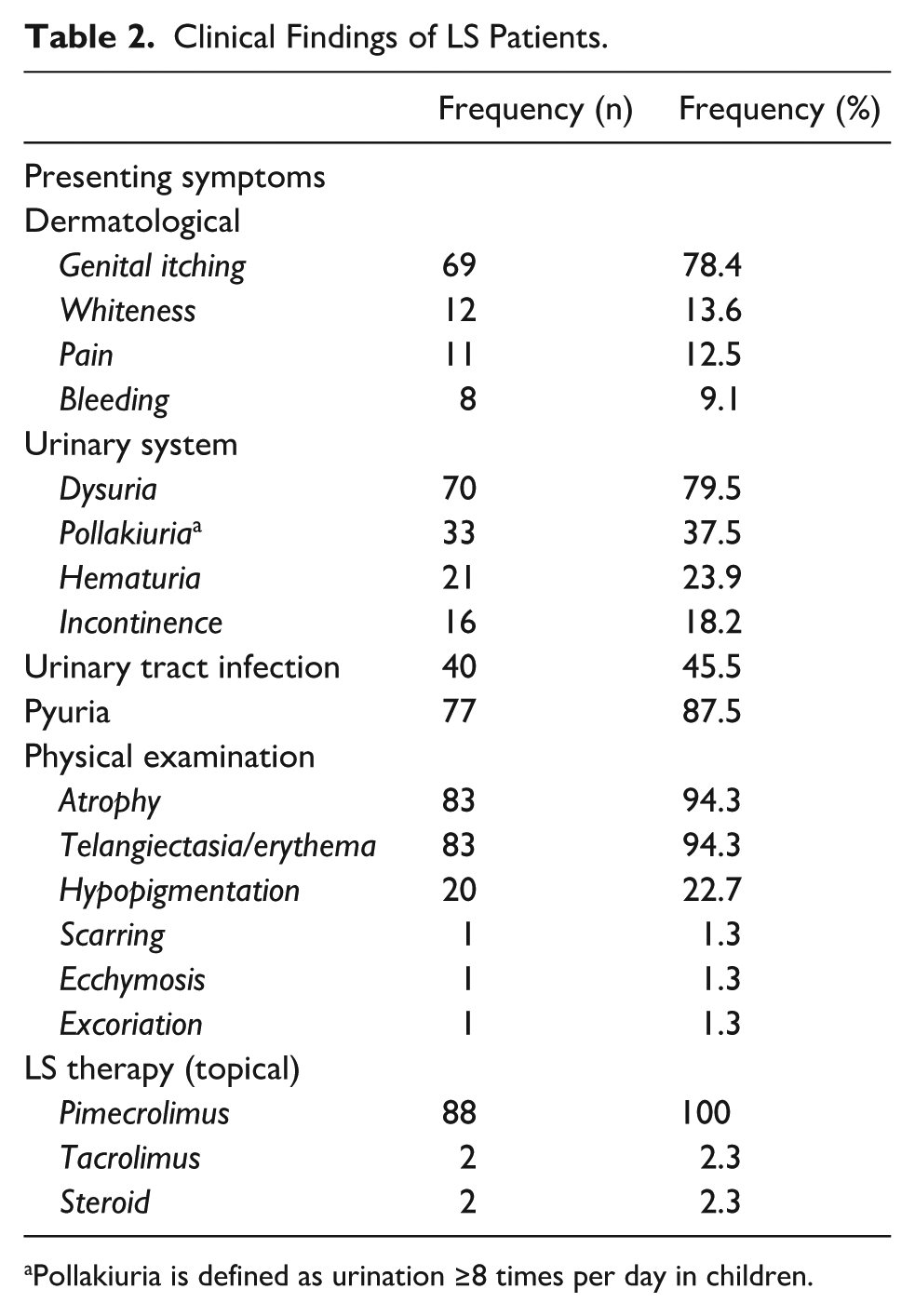
Pollakiuria is defined as urination ≥8 times per day in children.
Clinical Course and Treatment Outcomes
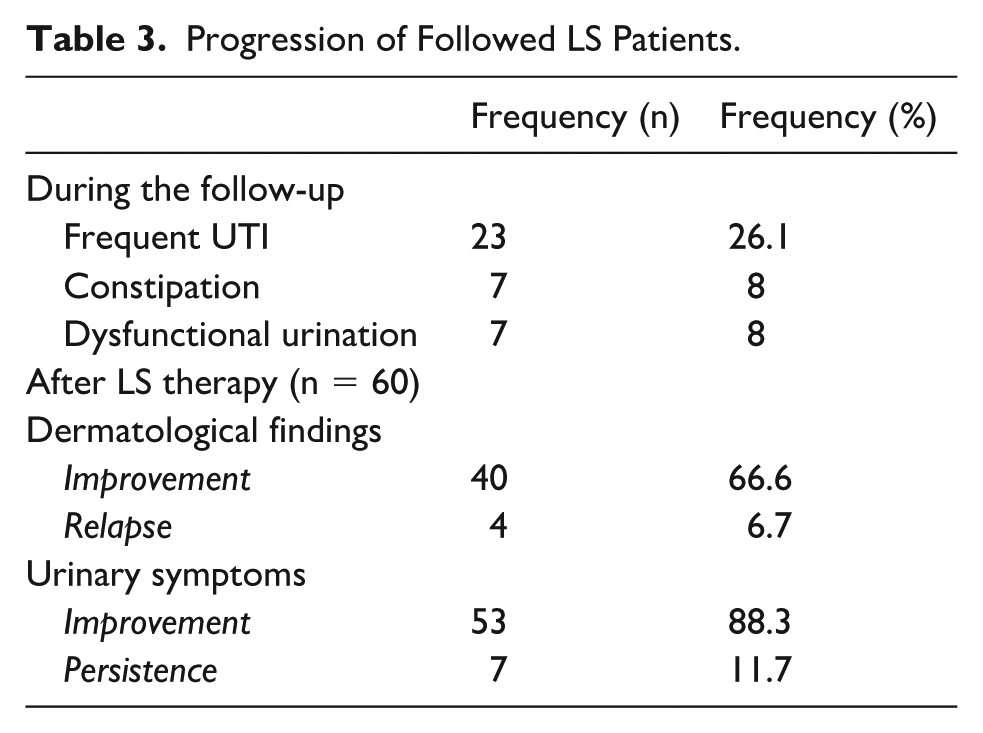
Sixty patients who received treatment for at least 3 months were evaluated for treatment response. The mean follow-up duration was 16.83 ± 23.1 months. All patients initially received topical pimecrolimus. In cases of inadequate response (n = 4), 2 were switched to topical tacrolimus and 2 to topical corticosteroids.
Recurrence of dermatologic symptoms occurred in 4 patients (6.7%). Persistent urinary complaints were noted in 7 patients (11.7%), all of whom had documented dysfunctional voiding. Despite continued symptoms, DVSS scores significantly improved over time.
Overall, 66% of patients showed marked improvement in dermatologic findings, while 88% reported complete or substantial improvement in urinary symptoms, particularly within the first 3 months of treatment (Table 3).
Progression of Followed LS Patients.
Discussion
This study highlights that LS is an underrecognized yet relatively common cause of urinary symptoms, particularly dysuria, in pediatric patients. Importantly, the majority of patients responded well to early diagnosis and topical treatment, avoiding unnecessary invasive procedures.
Although the general population prevalence of LS ranges from 1 in 300 to 1 in 1000,6,7 true rates may be underestimated due to misdiagnosis and low clinical awareness, especially in children. 6 In prepubertal girls, estimates suggest a prevalence of 1 in 900.1-3 In our cohort, LS was diagnosed in 84 out of 689 girls (12.2%) presenting with urinary symptoms, suggesting a higher-than-expected frequency when appropriate screening and dermatological consultation are implemented.
The median diagnostic delay in our study was 8 months, which is shorter than reported in prior studies.8,9 This may reflect increased awareness among pediatric nephrologists and urologists over time, as previously noted by others.10,11 Enhancing awareness of LS across all pediatric specialties—including nephrology, urology, and general pediatrics—will be key to improving diagnostic accuracy and ensuring timely intervention.
Lichen sclerosus shows a clear female preponderance, with reported female-to-male ratios ranging from 1:1 to 10:1.1-4,12,13 In our cohort, only 4 of 88 patients were male, all referred due to phimosis and diagnosed based on dermatological examination revealing atrophic white plaques at the external meatus (Figure 1). While phimosis is a typical presentation in boys, clinicians should maintain suspicion for LS in males with genital discomfort, itching, or dysuria, especially in the presence of erosive or ulcerative lesions. 14

Atrophic white plaques in the external meatus of a male pediatric patient with a history of surgery for hypospadias and lichen scleroatrophic lesions.
Consistent with previous studies, our findings support an association between LS and autoimmune diseases.4,15 Both personal and family histories of autoimmune conditions were common, supporting the proposed autoimmune pathogenesis. Mechanical trauma—particularly from activities such as cycling—was also identified as a potential contributing factor.10,16-18
Urinary symptoms were prominent, with dysuria present in all patients during the disease course. While adults more often report genital itching and pain, dysuria appears to be a dominant feature in pediatric LS. 4 Characteristic dermatologic findings included vulvar atrophy, erythema, telangiectasia, and hypopigmentation (Figure 2A-D), consistent with the literature.8,10,19
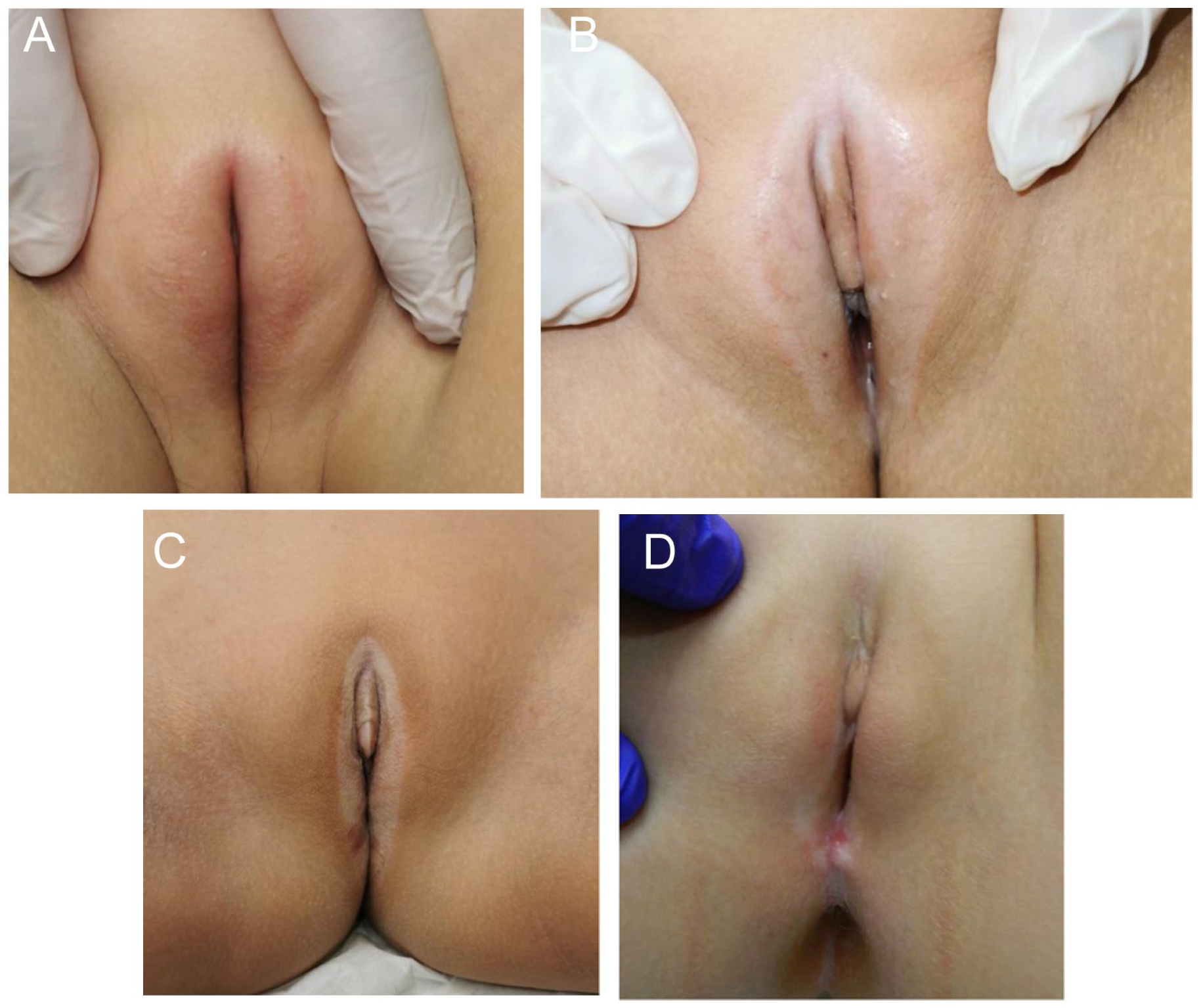
(A) Bilateral erythematous telangiectatic and atrophic plaques in the genital area of a female pediatric patient with lichen scleroatrophic lesions. (B) White plaques with yellowish cystic papules on top, showing bilateral telangiectatic and atrophic lesions in the genital area of a female pediatric patient with lichen scleroatrophic lesions. (C) Bilateral telangiectatic and atrophic plaques in the genital area of a female pediatric patient with lichen scleroatrophic lesions. (D) Bilateral telangiectatic and atrophic white plaques in the genital area of a female pediatric patient with lichen scleroatrophic lesions and erosive areas at the posterior commissure of the labia.
The association between LS and recurrent UTIs has been previously documented. 20 In our study, 87.5% of patients had pyuria, although only 45.5% had culture-confirmed infections, suggesting that LS-related inflammation may mimic UTI symptoms. Thus, LS should be considered in girls with persistent dysuria and sterile pyuria.
Incontinence and voiding dysfunction were also prevalent. Local inflammation and pain may exacerbate voiding symptoms.21,22 Lichen sclerosus may not only mimic urinary conditions but also perpetuate them via irritation and treatment challenges.22-24 In our patients with documented dysfunctional voiding, concurrent management—including urotherapy—resulted in improvement of both urinary and dermatologic outcomes, as evidenced by declining DVSS scores.
Topical corticosteroids are the standard treatment for LS. However, calcineurin inhibitors such as pimecrolimus and tacrolimus offer effective alternatives with favorable safety profiles and lower risk of atrophy and secondary infections, especially in children. 4 Our findings confirm the efficacy of pimecrolimus in the majority of cases, with early symptom relief often occurring within the first 3 months. A small proportion of patients required escalation to other topical agents due to inadequate response or recurrence.
Limitations of the study include its retrospective design, relatively small sample size—especially for dysfunctional voiding—and lack of a control group. Additionally, the follow-up duration was variable. Nonetheless, this is one of the few studies in a pediatric nephrology setting to systematically assess LS in children presenting with urinary symptoms.
Conclusion
Lichen sclerosus is an often underdiagnosed but important cause of urinary symptoms—particularly dysuria and recurrent UTIs—in pediatric patients. Raising awareness and ensuring early diagnosis not only improve clinical outcomes but also help avoid unnecessary invasive investigations. Therefore, pediatricians, nephrologists, and urologists should maintain a high index of suspicion for LS in children presenting with persistent dysuria, recurrent UTIs, or sterile pyuria. Optimal care requires a multidisciplinary approach, including dermatology consultation and management of associated voiding dysfunction. In conclusion, by ensuring timely diagnosis and intervention, clinicians can prevent unnecessary investigations and improve the long-term quality of life for pediatric patients with LS.
Author Contributions
AN and BA contributed to conceptualization. AN, BA, GP, and MD contributed to methodology. BA, GP, HÖG, MD, and AN contributed to data collection. AN and BA contributed to data analysis. BA contributed to writing—original draft preparation. BA, MD, and AN contributed to writing—review and editing. All authors contributed to the approval of the final draft. AN contributed to supervision.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statements
No data sets were generated or analyzed during the current study.