
Abstract
Pediatric behavioral health (BH) conditions are present in approximately 20% of children. Primary care providers are assuming more aspects of their patients’ BH care and desire education about common BH conditions. A primary care BH Extension for Community Healthcare Outcomes (ECHO) program conducted bi-monthly tele-educational sessions to community pediatricians in a health network. Sessions provided best practice information about a variety of BH topics. Participants completed surveys about satisfaction with the educational program and self-assessment of confidence and competence in treating BH disorders before and after the ECHO program. Survey results showed providers reported increased knowledge and competence in many aspects of BH care including screening, providing education, management (BH strategies and medication), and knowledge of resources. A BH ECHO program is a promising approach to addressing the challenges primary care providers face in caring for youth with BH needs.
Introduction
Pediatric behavioral health (BH) conditions are common with an estimated 20% of all children identified with a BH condition annually. 1 Concerns about children’s mental health heightened during the COVID-19 pandemic, and in 2021, the American Academy of Pediatrics, the American Academy of Child and Adolescent Psychiatry, and the Children’s Hospital Association created a combined statement declaring a National State of Emergency in Children’s Mental Health. 2 The crisis in pediatric mental health highlights several health care disparities as children living in poverty and minoritized children have a higher rate of many mental health conditions and poorer access to care.2-4
Despite its high prevalence, the percent of children receiving treatment for pediatric mental health disorders is low, 1 and the availability of pediatric mental health providers is variable and sparse in many areas of the United States.5,6 Many children with BH conditions are managed by their pediatric primary care provider (PCP) because they are often the first and main contact for youth seeking BH supports. Primary care providers assume many aspects of BH care including evaluation for child/adolescent mental health disorders as well as providing ongoing treatment.7,8 Pediatric PCPs feel it is important to have a role in addressing BH needs; however, many have limited training in pediatric BH disorders9,10 and report varying levels of comfort and effectiveness in managing BH conditions in the primary care setting.7,8,11 Furthermore, pediatric PCPs note limited time and resources to appropriately support their patients’ BH needs.10,12
To address this area of need, institutions have implemented various strategies including integrating BH providers (ie, psychologists and therapists) into the primary care setting.6,13-15 However, not all primary care sites have access to pediatric BH providers, and, even when sites have integrated BH providers, the ratio of BH providers to the number of patients may not meet the practice’s needs. In addition, there may be patients with BH needs that do not want to see a BH provider or are unable to schedule with onsite BH providers due to insurance barriers. Therefore, PCPs need to be competent in managing BH needs commonly seen in primary care. Additional strategies are needed to address this gap in care.
One potential intervention is Project Extension for Community Healthcare Outcomes (Project ECHO), a collaborative medical education and care management model that provides education about best practices on a specific topic to community clinicians, allowing them to provide better care to patients in their community. This model involves a team of specialists (a “Hub team”) that facilitates longitudinal learning (programs often run for 6-12 months) with community PCPs. Educational sessions are conducted using teleconferencing platforms and use a combination of didactics and case-based learning to facilitate guided-practice (mentorship) on the desired topic. 16
Extension for Community Healthcare Outcomes programs are associated with enhanced provider education and improved outcomes for a variety of topics including substance use disorders, infectious diseases, and chronic disease.17,18 Programs consistently report high levels of PCP satisfaction, increased PCP knowledge, improvements in patient health, and cost-effectiveness, 19 and many studies have found the ECHO model can be used to improve access to best-practice BH care.19-21
There are fewer data on use of ECHO programs to support pediatric BH care. Several studies have shown that participation in pediatric BH ECHO programs is associated with improved pediatrician knowledge and confidence in treating various BH conditions.16,22-25 Findings in two pediatric BH ECHO programs have also demonstrated important practice changes among PCPs. Hostutler et al 25 described a BH ECHO program that included 20 PCPs who received education about a range of BH topics. In their study, participation in the ECHO program was associated with improvements in knowledge and competence, and review of EMR data showed significantly reduced rates of polypharmacy. Cinko et al 23 evaluated a BH ECHO program that included 2 small cohorts (n = 18; 23) of PCPs who received education on treatment of adolescent depression. The PCPs in this study were more confident in their treatment approach, and participation in the ECHO program was associated with decreased emergency department referrals. Prior pediatric BH ECHO programs have prioritized recruiting participants from rural practices, 24 underserved communities, and school-based health centers (SBHCs). 22 Others have focused on a narrow range of diagnostic topics 23 and included a small number of participants. 25 Data are limited evaluating pediatric ECHO programs that provide a wide range of educational topics including common BH concerns and psychiatric medication management and programs that support PCPs across rural, suburban, and urban settings.
Our institution created a pediatric primary care BH ECHO program to support PCPs practicing in rural and non-rural settings by providing education on diagnosis and management of a wide variety of BH conditions commonly treated in the medical home. We provided education about diagnosis, medication management, and behavioral supports for common topics including attention deficit hyperactivity disorder (ADHD), anxiety, depression, autism spectrum disorder (ASD), educational concerns, and disruptive behaviors. We hypothesized that PCPs’ self-reported confidence and competence in diagnosis, behavior management, and medication management of common BH conditions would improve after participating in the BH ECHO program.
Methods
This project was certified exempt (ie, approved) by the Institutional Review Board.
Extension for Community Healthcare Outcomes Program Development
The primary care BH ECHO program was developed by a multidisciplinary team including a pediatric psychologist, pediatrician, data analyst, and project coordinator. Funding for this pilot program was received through a BH grant from an outside financial institution. While planning the ECHO program, the team partnered with another children’s health system with a well-established BH ECHO program to review best practices and lessons learned. To determine the target population’s areas of highest interest, a needs assessment was developed by the ECHO team’s pediatrician and psychologist and distributed to PCPs in the institution’s primary care network. The needs assessment asked PCPs to rate their confidence in diagnosing and managing ADHD, anxiety, depression, and ASD in the primary care setting. The PCPs also rated their confidence in providing recommendations about commonly discussed topics including sleep, disruptive behaviors, feeding difficulties, disordered eating, self-harm, school difficulties, and trauma, among others. The questionnaire consisted of 35 questions in a Likert-scale format, with 3 additional questions to capture the providers’ practice location, years of experience, and role within the practice (physician, physician assistant, nurse practitioner, and psychologist).
The ECHO team reviewed results from the needs assessment and reviewed the existing literature about BH ECHO programs.23-25 The team’s clinicians (pediatric psychologist and pediatrician) led development of the ECHO program’s session topics. The goal was to include a variety of topics and prioritize areas where PCPs reported the lowest confidence in diagnostic and management skills. The curriculum topics incorporated information about diagnostic evaluation, behavioral management, and medication management for common BH disorders along with focused topics commonly discussed in primary care (Table 1). The ECHO team then identified content experts for the session topics. These experts formed the Hub team: multidisciplinary experts from psychology (psychologists in primary care, child clinical, autism, and school psychology), pediatrics (general pediatrician and developmental pediatrician), psychiatry, pharmacy, and social work.
Session Topics.
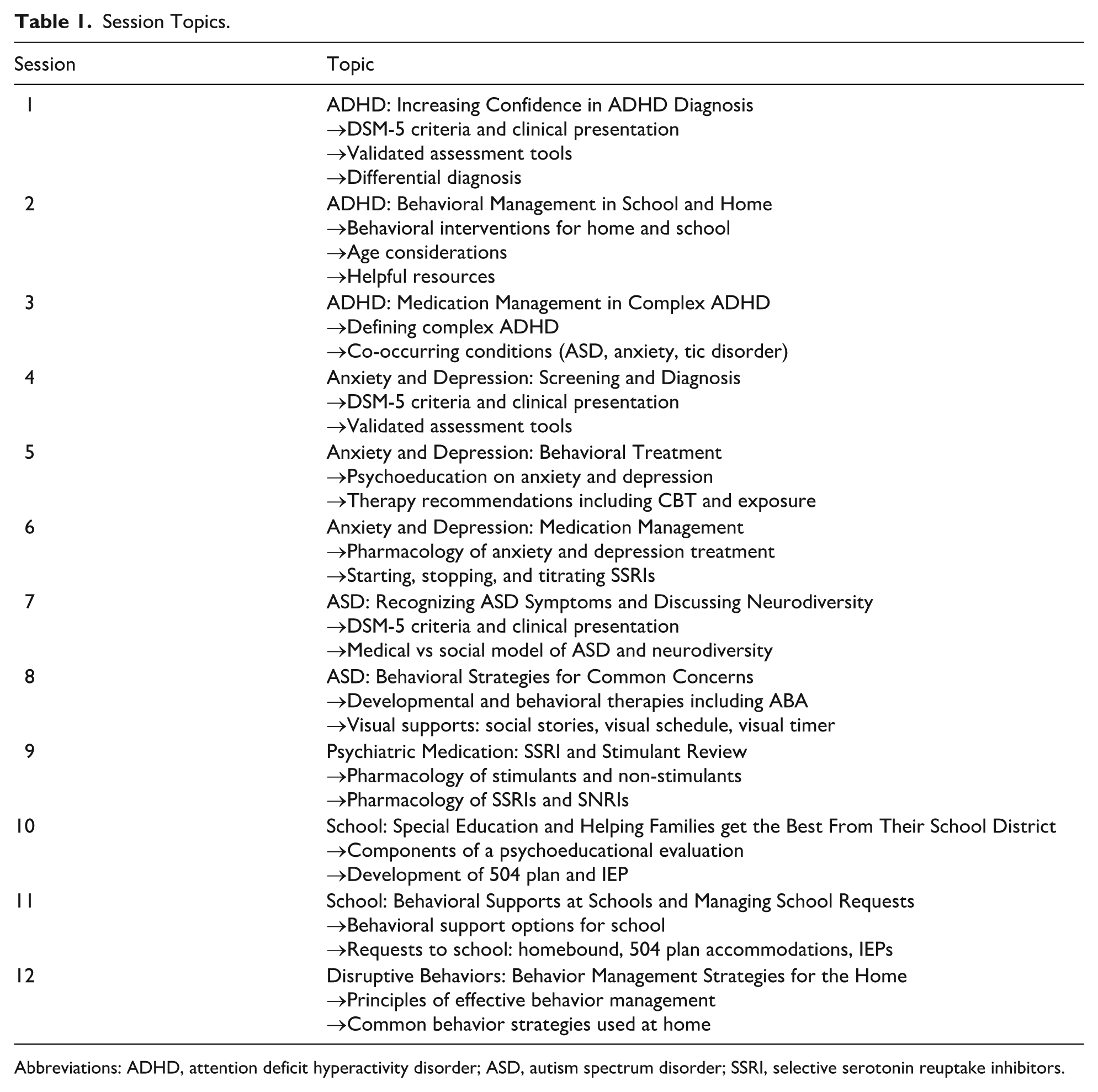
Abbreviations: ADHD, attention deficit hyperactivity disorder; ASD, autism spectrum disorder; SSRI, selective serotonin reuptake inhibitors.
Participants
This BH ECHO Program targeted pediatric PCPs from primary care offices across this institution’s rural and non-rural practices. Participants were recruited by disseminating information about the ECHO program at division meetings, provider meetings, through email, and through a primary care newsletter. While the target audience was pediatric PCPs, the program drew interest from other pediatric providers including pediatric psychologists (integrated primary care, autism, and child clinical), psychiatric advanced practice nurses (APNs), and SBHC clinicians (APNs and licensed clinical social workers [LCSWs]).
Extension for Community Healthcare Outcomes Program
The series was free, and providers earned continuing medical education credits and maintenance of certification part 2 credits. Twelve sessions occurred from July 2023 through January 2024. Each session was 60 minutes and included a didactic lecture presented by content experts on best practices for assessing and treating a BH condition followed by a case-based discussion. Participants joined the sessions virtually on Microsoft Teams, while the Hub team joined from a central location. Sessions were recorded.
Evaluation Measures
To evaluate the ECHO program, participants were asked to complete surveys throughout their experience including post-session (after each ECHO session) and post-program (at the conclusion of the 7-month educational program). Surveys were completed in REDCap26,27 and used a 5-point Likert scale (1—strongly disagree, 2—disagree, 3—neutral, 4—agree, and 5—strongly agree). In both surveys, questions about change in knowledge and confidence were asked using a retrospective post-approach to pre-approach to minimize recall bias. Survey questions were developed in this manner after a review of published literature describing the evaluation of other ECHO programs.25,28
The post-session surveys included 8 items that assessed change in knowledge of the session topic, impact of the didactic presentation, impact of the case conference discussion, applicability of content, likelihood to use session information in their work, and likelihood to recommend the session to colleagues (Appendix A). The post-program survey included 14 pairs of items (“before and after the ECHO program”) that assessed confidence and self-efficacy in use of screening tools, providing education to families, discussing behavior strategies, prescribing medication for various BH disorders, and knowledge of resources. Four questions asked about change in practice (Appendix B). All registered participants were asked to complete post-session and post-program surveys. Because participants held varying degrees and roles within pediatric care (ie, physicians, psychologists, APNs, and LCSWs), all post-program survey questions included an option to choose “N/A—outside my scope of practice.”
Analysis
Descriptive statistics were compiled for all responses to the post-session survey. The 5-point Likert scale responses to the post-program survey were treated as continuous variables and were paired for comparison by a Wilcoxon signed rank test. The Holm correction was applied to account for multiple comparisons. 29 Responses of “not applicable” (either due to the role of the respondent or the respondent not having attended the relevant session) were treated as missing.
Results
Participants
A total of 95 participants registered including 82 PCPs (MD/DO/APN/PA) practicing at 19/21 of the institution’s primary care offices. Additional registrants included 5 integrated primary care psychologists, 5 SBHC providers (PhD/PsyD, APN, LCSW), 2 psychiatry APNs, and 1 autism psychologist. The participants’ primary care practices represented a broad range of sizes, geographic regions, and patient demographics. Of the 19 primary care practices, 3 were rural and 16 were non-rural. Practice panel size ranged from 3357 to 12 163 patients. Eleven practices served patients with predominantly private insurance, while 2 practices had populations with >70% public insurance. There was a wide range of race/ethnicity across practices (Hispanic: 4%-60%, Black: 4%-85%, and White: 4%-77%). English was the preferred language for >80% of patients in all but one practice (Table 2). The average session attendance was 43 participants.
Practice Characteristics.
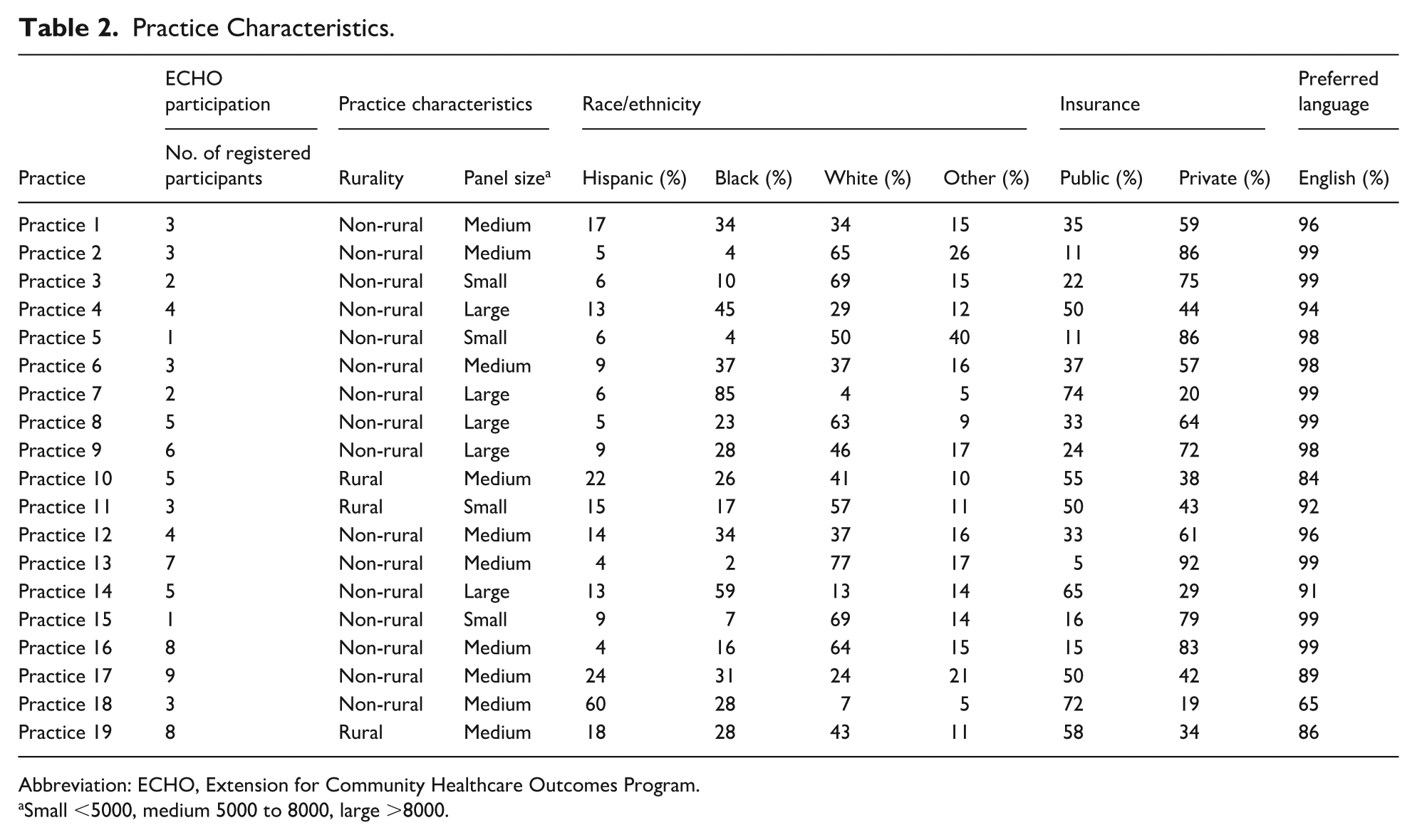
Abbreviation: ECHO, Extension for Community Healthcare Outcomes Program.
Small <5000, medium 5000 to 8000, large >8000.
Post-Session Survey
Thirty-six providers from 18 practice locations completed at least one of the post-session surveys, for a response rate ranging from 0% to 24%. In total, 73 surveys were returned, with a mean of 2 sessions rated per respondent (range = 1-7) and a mean of 7 surveys per session (range = 1-14). Only session 10 did not garner any responses. The respondents were mostly physicians with 71.2% identifying as an MD or DO, 19.2% identifying as an APN, and 9.6% identifying as a BH provider. Results of these post-session surveys are reported in Table 3.
Post-Session Survey Results.
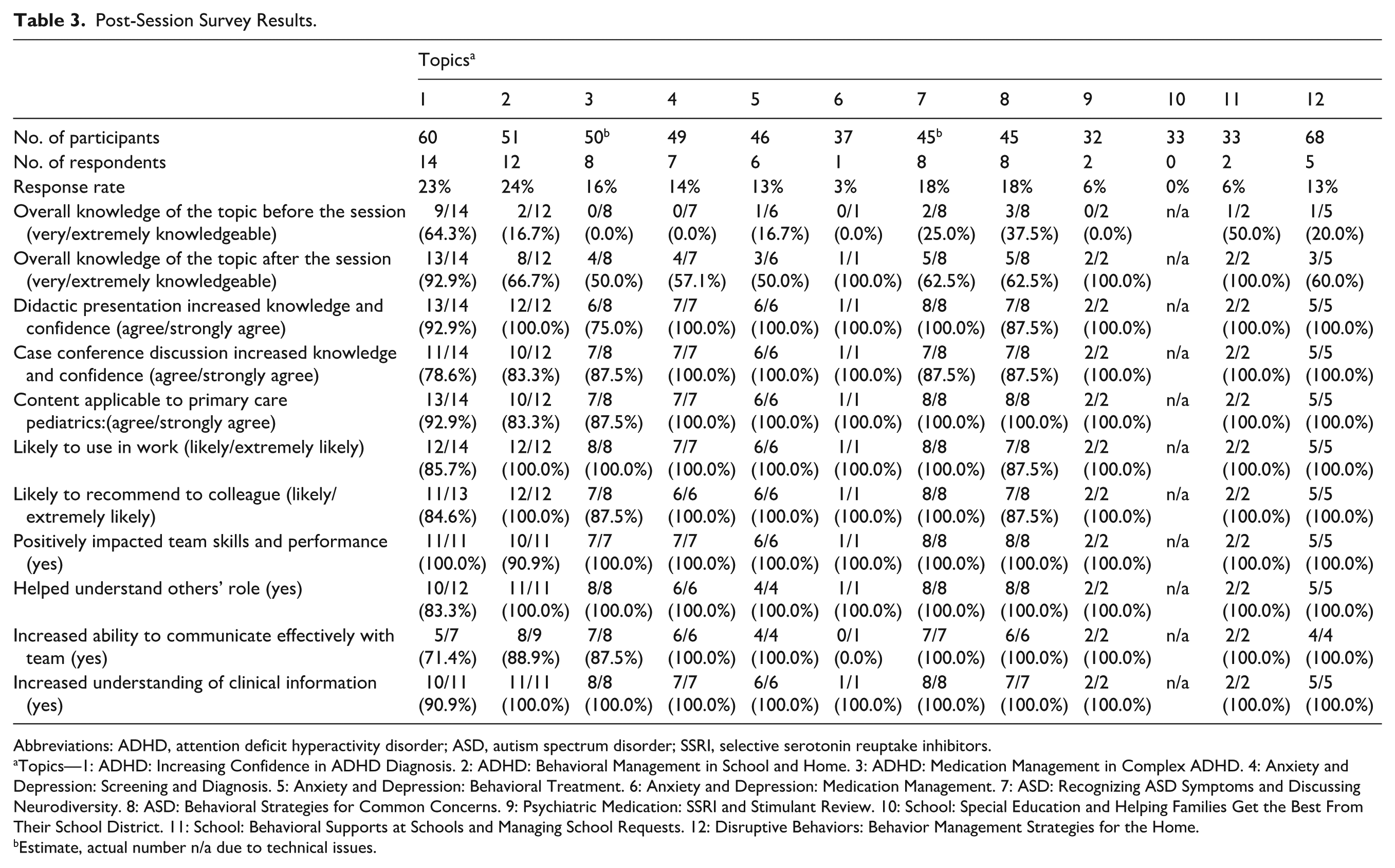
Abbreviations: ADHD, attention deficit hyperactivity disorder; ASD, autism spectrum disorder; SSRI, selective serotonin reuptake inhibitors.
Topics—1: ADHD: Increasing Confidence in ADHD Diagnosis. 2: ADHD: Behavioral Management in School and Home. 3: ADHD: Medication Management in Complex ADHD. 4: Anxiety and Depression: Screening and Diagnosis. 5: Anxiety and Depression: Behavioral Treatment. 6: Anxiety and Depression: Medication Management. 7: ASD: Recognizing ASD Symptoms and Discussing Neurodiversity. 8: ASD: Behavioral Strategies for Common Concerns. 9: Psychiatric Medication: SSRI and Stimulant Review. 10: School: Special Education and Helping Families Get the Best From Their School District. 11: School: Behavioral Supports at Schools and Managing School Requests. 12: Disruptive Behaviors: Behavior Management Strategies for the Home.
Estimate, actual number n/a due to technical issues.
In each survey, respondents were asked to rate their overall knowledge of the session topic before and after the session. Forty-four of the 73 paired responses to these 2 questions (60.3%) indicated increased knowledge of the session topic area after attending the session.
Attendees were appreciative of both the didactic presentation and case conference discussion within each session, with most agreeing that their knowledge and confidence strongly increased following the sessions. No respondents endorsed disagreement with these statements. Respondents rated other aspects of the sessions positively, with most stating that the information was applicable to primary care pediatrics, that they would use what they learned in their work, and that they would recommend the session to a colleague. Most respondents strongly endorsed that the information presented in the session positively impacted the teams’ skills, helped them understand the roles of other health care professionals, increased their ability to communicate effectively with other members of the team, and increased their understanding of the clinical information shared. When asked how the session could have been improved, many respondents preferred more frequent sessions, and several reported they wanted more focus on certain topics, with only very few suggesting less-frequent sessions.
Post-Program Survey
Of the 95 providers invited to complete the post-program survey, 22 associates from 13 practice locations responded, for a response rate of 23%. Ten of these providers responded only to the post-program survey, and 12 were also represented in the post-session survey data. Respondents to the post-program survey attended one to 12 sessions, with a mean of 6.7 sessions attended (median, 7). Sixteen of the respondents (69.6%) identified as a physician, 21.7% as an APN, and 8.7% as a psychologist.
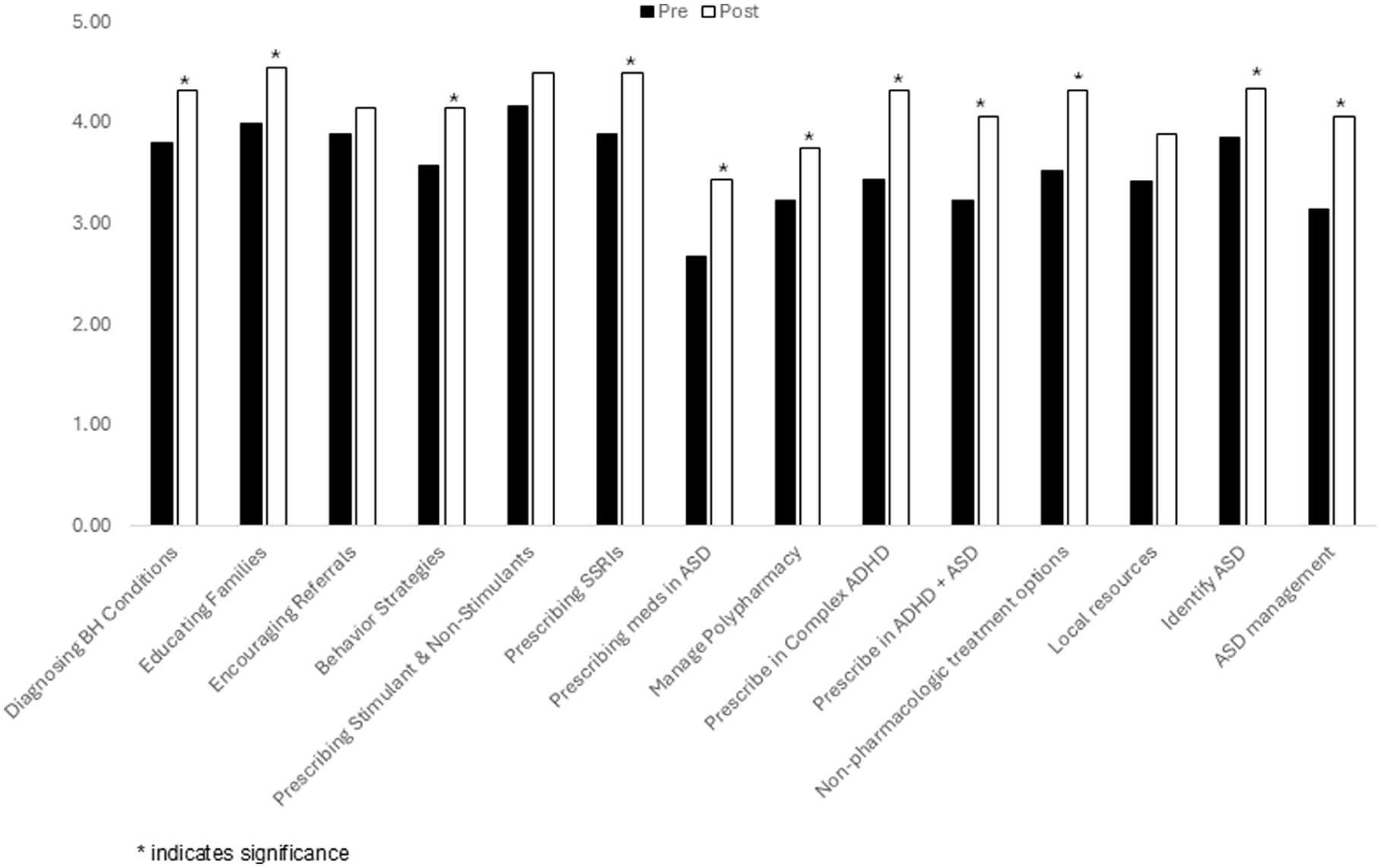
Survey results showed a statistically significant difference between the respondents’ confidence before and after the ECHO sessions on 11 of the 14 paired survey questions (Figure 1). Respondents indicated that after participating in the ECHO program, they were better able to use screening tools and diagnose BH conditions (P = .04), provide education to families (P = .024), provide evidence-based behavioral strategies (P = .035), identify developmental differences seen in ASD (P = .036), and discuss ASD management including neurodiversity (P =< .001). Participants responding to questions about medication management indicated increased effectiveness in their ability to do the following: prescribe selective serotonin reuptake inhibitor for treatment of anxiety and/or depression (P = .022); prescribe psychotropic medication for autistic children (P = .030); manage patients with polypharmacy (P = .025); manage medications in children with ADHD and other co-occurring conditions such as anxiety, depression, and tic disorder (P = .013); and manage medications in children with ADHD and co-occurring ASD (P = .036). Participants also indicated increased knowledge about different non-pharmacological treatment modalities that are effective for BH conditions (P = .020). Finally, participants’ overall confidence rose from a mean of 3.64 prior to the program to 4.21 after the program, which represented a significant change (P < .001) (Table 4).
Post-program survey results.
Post-Program Survey Results.
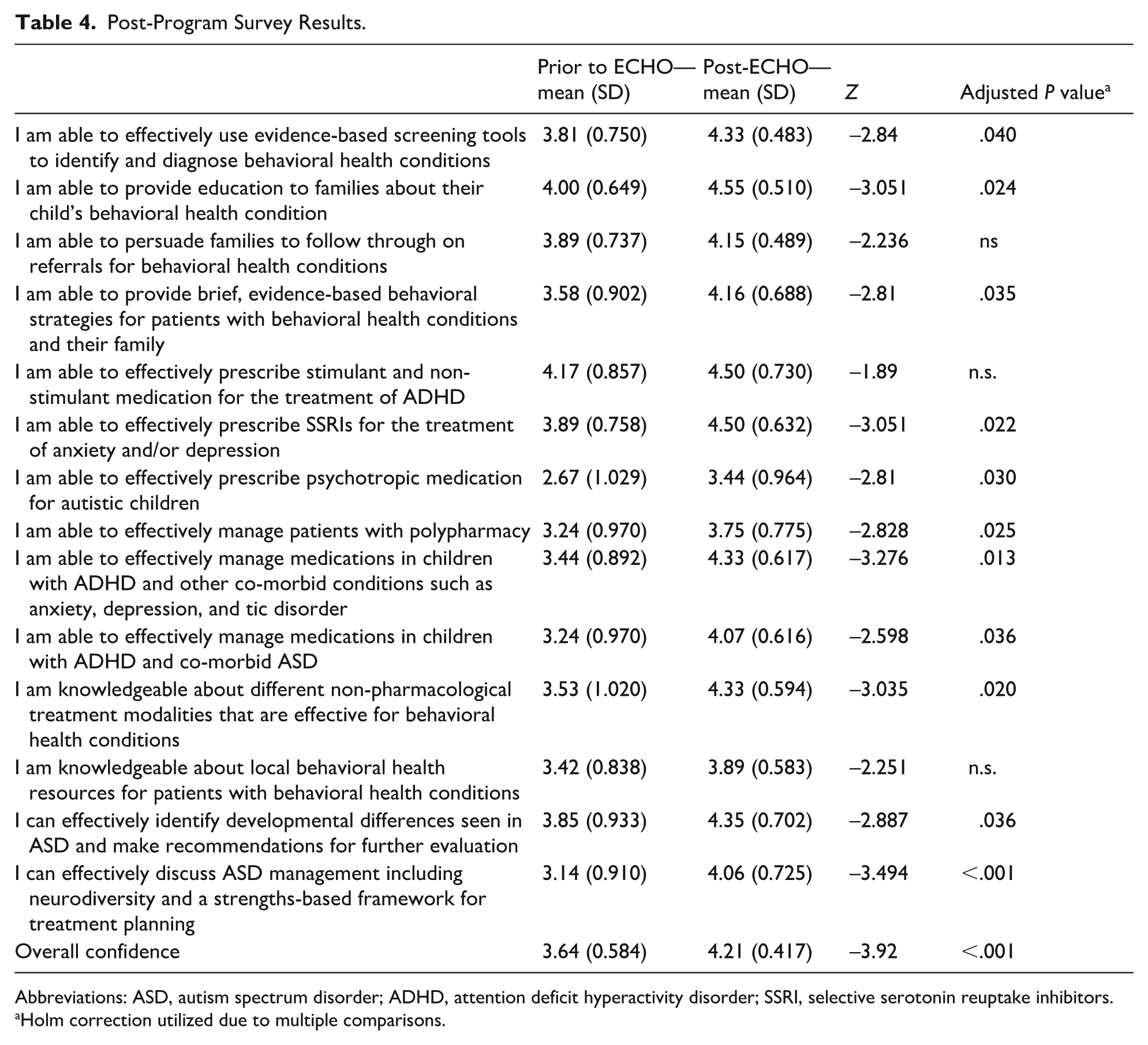
Abbreviations: ASD, autism spectrum disorder; ADHD, attention deficit hyperactivity disorder; SSRI, selective serotonin reuptake inhibitors.
Holm correction utilized due to multiple comparisons.
Discussion
Participation in this pediatric primary care BH ECHO program was associated with an increase in PCP’s self-reported knowledge of BH conditions and increase in confidence in diagnosis and management of common BH topics. These findings are noteworthy given that PCPs tended to endorse having moderate or high knowledge of the topic before the sessions and generally reported an improvement in their knowledge after the sessions (Figure 1).
More than 90% of PCPs reported the content was applicable to primary care pediatrics, increased their clinical knowledge, and that they were likely to use the information in their clinical work. This study adds to the existing literature showing BH ECHO programs positively impact PCP confidence in many aspects of BH care.19-21,23-25 Prior research shows PCPs’ desire to have a role in addressing BH needs in primary care, 30 and access to BH providers remains sparse in many areas of the country.5,6 These findings and those from prior research support the ECHO model as a viable way to improve access to high-quality BH care in the pediatric primary care setting. These ECHO programs can be part of broader efforts to support the large number of children requiring support for BH disorders. 2
Ninety-five PCPs from 19 of the institutions’ primary care practices participated in this BH ECHO program. These practices included patients from varying geographic regions with a wide range of demographic characteristics. This pool of participants differs from other successful BH ECHO programs that included fewer participants 25 and focused on rural practices only. 24 The current study also adds to the existing literature as it evaluates a BH ECHO program that provided education on a wide variety of BH topics. In this didactic curriculum, the high-yield topics of ADHD and anxiety/depression were reviewed over multiple sessions with separate didactics dedicated to assessment, behavioral treatment, and medication treatment of these diagnoses. Characteristics of complex ADHD were highlighted along with medication management strategies for this group. Two didactic sessions were dedicated to ASD and included information about recognizing autism characteristics, neurodiversity, and behavioral strategies for common concerns. The curriculum also dedicated sessions to other high-yield topics including school concerns (the special education system and behavioral supports) and disruptive behaviors. One session summarized psychopharmacology discussed during prior sessions.
Providing community PCPs education on a broad range of BH topics may improve care provided to families within the medical home. Given that families develop long-term relationships with their child’s PCP, this allows for early identification of BH conditions during primary care visits. For instance, a PCP can help families understand information about a suspected or confirmed BH condition, discuss treatment options including medication and BH strategies, and, in some cases, help guide families in how to access support from a BH specialist. In addition, with increased PCP knowledge about neurodiversity and use of a strengths-based approach to obtaining autism symptoms, PCPs may empower families to consider seeking evaluation and services when autism is suspected. 31 In this study, PCPs reported increased confidence using psychiatric medications for the treatment of anxiety and depression and increased confidence using polypharmacy to treat BH concerns. Given the prevalence of anxiety (15%) and depression (9%) among adolescent youth, 32 higher PCP confidence in the use of psychiatric medications for anxiety and depression may positively impact care for many patients. Attention deficit hyperactivity disorder is often accompanied by co-occurring BH conditions across all age groups (77% likelihood from preschool through high school). 33 Therefore, improving PCP confidence in managing complex ADHD may increase support for youth with ADHD and co-occurring diagnoses.
Limitations
There are several limitations to this study. This was the institution’s first ECHO program, and there were unique challenges and learning opportunities. While participants were originally granted protected time to attend ECHO sessions, organizational changes occurred several months into the program and resulted in loss of this protected educational time. Subsequently, timing of sessions shifted, and it is suspected that this impacted session attendance and survey completion moving forward. Also, the program did not include incentives for survey completion, which could have helped increase motivation and response rate considering PCPs’ busy schedules. The PCPs in this study were part of an academic medical center, which may limit generalizability of findings. Many of the PCPs’ primary care practices have BH providers (ie, integrated psychologists or therapists) in their clinics, which may impact baseline knowledge and comfort with BH information when compared with PCPs without BH providers on site (ie, of the 19 clinics, 13 have a BH provider on site).
In addition, the post-program survey reflected each PCP’s individual perspective of their growth before and after participating in the ECHO program, but the treatment dose (eg, the number of ECHO sessions attended) varied across the PCPs. A criterion for eligibility to complete the post-program survey was that a PCP attended at least one session of the ECHO program. Thus, PCP responses to the post-program surveys reflect varying levels of learning experiences (eg, one PCP attended 80% of the sessions, another PCP attended fewer than 30% of the sessions). It should be noted that if PCPs encountered a question on the post-program survey regarding a session they did not attend, the PCP was able to select “not applicable, did not attend session on this topic.” Furthermore, if a BH provider encountered a question about medication management, the provider was able to select “not applicable, out my scope of practice.”
Another important limitation of this study is that all surveys evaluated participants’ perception of knowledge gained during the BH ECHO program. Surveys did not obtain objective information about knowledge gained or participants’ clinical application of perceived improvements. Furthermore, this study did not include patient or practice-level data such as type or volume of BH diagnoses managed in primary care, referrals to psychiatry or emergency medicine, or prescribing information; all could strengthen conclusions about the effectiveness this educational program. Previous published data on ECHO programs consistently show that this telemedicine, case-based, longitudinal mentorship model is effective in improving PCP knowledge and competence; 16 however, there are limited published studies on patient-level and community-level outcomes.17,18
Future Directions
This body of research would benefit from future studies evaluating participants’ perceived improvements in knowledge and objective information about change in knowledge, application to clinical practice, and patient-level outcomes. Similar to Hosutuler et al, 25 future research exploring participants’ prescribing practices would inform how ECHO programs may improve access to best practices on medication management for common BH disorders. Future studies could also focus on PCP referral practices to psychiatry and other BH services. This remains critically important in the setting of a shortage of specialty BH providers. Future research could evaluate the optimal duration of ECHO programs and what specific BH content is most desirable to PCPs and most effective at improving PCP competence. For instance, one could compare longer and more comprehensive programs to shorter and more content-focused programs. In addition, research should examine the longitudinal impact of participating in an ECHO program by evaluating participant confidence and knowledge several months or 1 year after participation. Research can also examine if programs that include refresher sessions would help to maintain the skills PCPs learned. Finally, future research can investigate the best way to maintain and improve PCP engagement and attendance in ECHO sessions. The nature of ECHO sessions is virtual, and PCP engagement in a session may vary based on the demands of their clinic day, feeling of connectedness to the group, and the topic being discussed. Researchers can explore if there are differences in outcome measures for varying cohorts of participants (eg, combining community and tertiary hospital-based PCPs; large cohort vs small cohort).
Conclusion
Overall, BH ECHO programs are a promising approach to addressing challenges PCPs report in caring for youth with BH needs. The ECHO model is a viable way to improve access to high-quality BH care and evidence-based practice in the pediatric primary care setting. This study found that education received through BH ECHO programs can improve PCP confidence and competence in treating children and adolescents with a range of BH conditions. Behavioral health ECHO programs may be an important strategy to address the known shortage of BH specialty providers and improve care for children in all communities.
Author Contributions
Meghan Harrison: conceptualization, methodology, writing; Meredith Sherretz: methodology, survey development, data analysis, writing; Amy Geyer: conceptualization, methodology, writing; Amanda Lewis: data analysis, writing; Allen Garcia: conceptualization, methodology, writing.
Supplemental Material
sj-docx-1-cpj-10.1177_00099228261455063 – Supplemental material for Improving Primary Care Providers’ Confidence in Management of Behavioral Health Disorders Through Use of the ECHO Model
Supplemental material, sj-docx-1-cpj-10.1177_00099228261455063 for Improving Primary Care Providers’ Confidence in Management of Behavioral Health Disorders Through Use of the ECHO Model by Meghan Harrison, Meredith Sherretz, Amy Geyer, Amanda M. Lewis and Allen Garcia in Clinical Pediatrics
Supplemental Material
sj-docx-2-cpj-10.1177_00099228261455063 – Supplemental material for Improving Primary Care Providers’ Confidence in Management of Behavioral Health Disorders Through Use of the ECHO Model
Supplemental material, sj-docx-2-cpj-10.1177_00099228261455063 for Improving Primary Care Providers’ Confidence in Management of Behavioral Health Disorders Through Use of the ECHO Model by Meghan Harrison, Meredith Sherretz, Amy Geyer, Amanda M. Lewis and Allen Garcia in Clinical Pediatrics
Footnotes
Acknowledgements
None.
Ethical Considerations
This study was reviewed by the institution’s IRB and given an exempt status—IRB #2007259-5.
Consent to Participate
Yes, consent received.
Consent to Publication
A waiver of written consent was approved by the IRB, and participants were made aware that survey data would be used to disseminate information learned from this program.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: TD Bank Behavioral Health Grant, Grant #8709884001.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data will be shared upon reasonable request made to main author.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.