
Abstract
The objective of this study was to examine the association between parental education and the occurrence of asthma, allergic rhinitis, and eczema in children, while accounting for potential confounding factors. Data were collected through questionnaires completed by 379 children aged 10 to 12. Maternal, paternal, and combined parental educational levels were assessed. Logistic regression models were used to evaluate associations with the odds of atopic diseases, adjusting for confounders. High parental educational level was significantly associated with a lower occurrence of allergic rhinitis in children (adjusted odds ratio [aOR] = 0.52, 95% CI: 0.27-0.99, P = .048), particularly when mothers had high, and fathers had low educational levels (aOR = 0.30, 95% CI: 0.13-0.71, P = .006). In addition, children with highly educated fathers were less likely to develop eczema (aOR = 0.56, 95% CI: 0.33-0.93, P = .028). These findings suggest that parental education influences atopic diseases in children, reflecting the complex role of social determinants of health.
Introduction
Over the past century, poverty in affluent countries has evolved. Advancements in sanitation, eradication of starvation, and widespread access to clean water have eliminated these as primary causes of death. However, individuals at the lower socioeconomic scale continue to experience worse health outcomes than those higher in the hierarchy. 1 This graded relationship, known as the “social gradient in health,” is not limited to the contrast between the rich and the poor, the edges of the social hierarchy. Instead, health improves step by step along the entire social scale. 2
This phenomenon revealed systematic differences in health that are unnecessary, unjust, and preventable. 3 The Commission on Social Determinants of Health (SDoH) concluded that health inequities arise due to disparities in daily life conditions and the uneven allocation of power, money, and resources, highlighting the profound impact of SDoH on disease prevalence and progression. 4 According to the World Health Organization (WHO), SDoH are “the conditions in which people are born, grow, work, live, and age, and the wider set of structural drivers that shape these conditions.” 5 These determinants include income, education, employment, food security, housing, neighborhood conditions, environmental factors, and access to health care services. 5 For example, low income is related to worse health conditions and higher health risk due to the deprivation of basic needs and limited access to health care services. 6 Higher levels of education improve health literacy and lead to better health status, while poor housing circumstances can induce serious health issues and negatively affect well-being.7,8 These examples describe determinants, known as intermediate determinants, that influence health outcomes directly by affecting living standards, opportunities, and access to resources. However, the definition of SDoH pertains not only to daily life conditions but also to all the forces and systems that form these conditions. These, also referred to as structural determinants, include social, economic, and political norms, forces, systems, policies, and agendas that manifest within countries under government authority and determine the conditions of daily life. 9
The impact of health inequities is particularly significant in children and adolescents, who have little control over their health and related factors. 10 This vulnerable group does not have an independent socioeconomic status (SES) but experiences social circumstances directly associated with their parents’ or caregivers’ SES. 11 Approaching SDoH through a life-course perspective that emphasizes the importance of critical periods or sensitive life stages (eg, childhood) and the accumulation of protective or harmful exposures over time, underscores the unique way that SDoH influence children’s and adolescents’ present and future health.10,11
Educational attainment follows an intergenerational pattern, meaning that parental education can affect a child’s health and well-being. Research has shown that infants born to mothers who did not complete high school have twice the risk of dying before their first year of life compared with infants with college-educated mothers. 12 Parents with higher educational levels are more likely to acquire healthier food and access quality health care services for their families. They also tend to foster attitudes, behaviors, and lifestyles that induce health and well-being. In addition, better-educated parents are more likely to enroll their children in high-quality schools, ensuring a better early peer environment. Improved childhood health and educational achievements set the basis for better future income in adulthood. Moreover, families with highly educated parents experience better family stability, fertility choices, and partner selection, all of which influence children’s health behaviors and educational outcomes. 13
The association between parental education and allergic diseases in children has been studied for decades, reflecting the role of education as a key SDoH. 14 Nevertheless, parental education remains a challenging determinant to study in isolation, as it is closely linked to socioeconomic, environmental, behavioral, and familial factors that may also influence the atopy risk. This complexity highlights multiple pathways through which SDoH affect health outcomes and underscores the need for a broader analytical framework. 9 Examining parental education while accounting for potential confounders is essential, although residual confounding cannot be entirely excluded.
The primary objective of the study was to investigate the impact of parental education on atopic diseases, specifically asthma, allergic rhinitis (AR), and eczema, in children aged 10 to 12 years. By analyzing the association between different parental educational levels and the incidence of these conditions, the study explored how SDoH, represented by education as a fundamental structural determinant and an important indicator of socioeconomic position, influence atopic diseases in children. Furthermore, the research examined a range of explanatory variables, such as sex, perinatal factors, health characteristics, and lifestyle patterns of children and their parents, as potential confounders of the association between parental education and atopic diseases. This study contributes to the broader research on the SDoH and their influence on health during childhood.
Methods
Study Design and Population
This observational cross-sectional study was conducted in Athens and Tripoli, Greece, with data collected at a single point in time for each participant between March and June 2024. The study is a secondary analysis of data collected during the PANACEA II study (Physical Activity, Nutrition, and Atopy in Children in Athens II), which was approved by the relevant institutional Ethics Committee. Schools were randomly selected from an official list provided by the national educational authorities. All the children in the fifth and sixth grades and their parents were requested to complete a questionnaire, including the standardized International Study of Asthma and Allergies in Childhood (ISAAC) questionnaire for children, 15 a semi-quantitative Food Frequency Questionnaire, 16 a Physical Activity Questionnaire for children, 17 and to self-report health history questions. The age group of 10 to 12 years was selected based on the PANACEA II study design, as this age group allows the use of the validated ISAAC questionnaire, facilitates standardized collection in the selected schools, and represents a stage when atopic diseases are well established and reliably assessed. We used only standardized questionnaires and distributed them across two cities with different socioeconomic and demographic profiles: Athens, the capital of Greece, and Tripoli, a smaller provincial city. In Athens, schools were randomly selected from areas with broadly recognized different socioeconomic characteristics (eg, central Athens’ neighborhoods with lower incomes and educational levels and higher immigrant populations, and northern suburbs generally associated with high-income, highly educated families). 18 Children with missing information on outcomes or explanatory variables were excluded from the analysis to ensure a homogeneous sample. The study followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. 19
Health Outcomes and Educational Levels of Parents
“Ever asthma” was defined as a positive answer to the question, “Has your child ever had asthma?” Similarly, with “ever allergic rhinitis” and “ever eczema.” Parents’ educational levels were examined separately (maternal and paternal educational levels) and combined (parental educational level). According to the National Education System of Greece, education is classified into primary, secondary, and tertiary. Table 1 presents the different levels of the National Educational System of Greece assigned to ISCED (UNESCO Institute for Statistics. International Standard Classification of Education)-11 levels, a standardized classification, to ensure comparability of the data with other studies. Primary and secondary educational attendance is considered mandatory by the Greek state. However, there was a small number of parents with primary educational attainment in the sample. Therefore, we merged this group with the group of parents with secondary education. As a result, educational levels were categorized into 2 groups: low educational level (mothers and fathers who have completed secondary education or lower) and high educational level (mothers and fathers who have completed tertiary education). Parental educational level (maternal and paternal education combined) was defined as the highest level completed by either parent. Two categories were established: low parental education (both parents with low educational levels) and high parental education (at least one parent with a high educational level). Parental education was used as an indicator of socioeconomic position. However, no data on income, occupation, or living conditions were collected.
National Educational System of Greece and ISCED 2011 Classification.
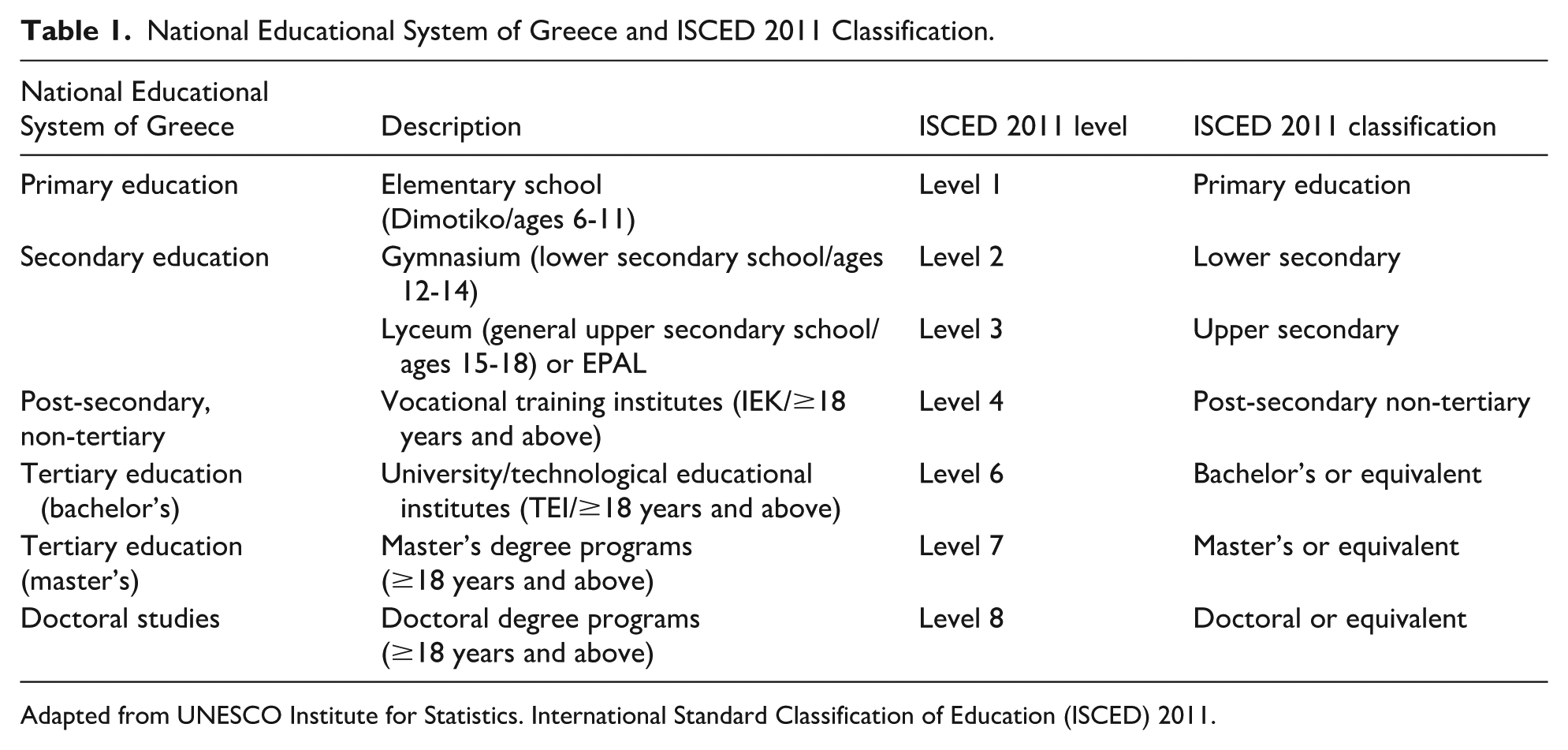
Adapted from UNESCO Institute for Statistics. International Standard Classification of Education (ISCED) 2011.
Explanatory Variables
A list of explanatory variables, well-known from the current literature, was included in the study: sex, delivery mode, prematurity, neonatal intensive care unit (NICU) admission, breastfeeding, early day-care attendance, exercise outside school, obesity, current parental smoking, parental history of atopy, and having older siblings. These variables were also examined as potential confounders of the association between parental educational level and the outcomes.
The part of the questionnaire for parents included questions regarding delivery mode (cesarean section vs natural birth), prematurity of the child (full-term vs premature), history of NICU admission of the child (yes/no), and breastfeeding (yes/no). Regarding day-care attendance, parents were asked whether their child attended nursery (from 2 months to 2.5 years old), pre-kindergarten (from 2.5 to 4 years old), or kindergarten (4-6 years old). After the age of 4, preschool education is mandatory in Greece. Therefore, we categorized 2 groups: early day-care attendance (<4 years old) and late day-care attendance (≥ 4 years old). The question “Is anyone currently smoking inside the house?” was used for the evaluation of the current parental smoking exposure of the child (yes/no). “Has the mother of the child ever had any of the following conditions: asthma, allergic rhinitis, or eczema?” and “Has the father of the child ever had any of the following conditions: asthma, allergic rhinitis, or eczema?” were the questions used to determine parental history of atopy. If either of the parents responded affirmatively to any of the 3 conditions, parental history of atopy was considered positive and was included as a combined binary confounder in all logistic regression models. Parents were also asked to report some physical measurements of their child, such as weight and height. Using these data, we calculated the body mass index (BMI) of the children to specify obesity. Children with a BMI ≥25 kg/m2 were considered obese. Finally, a list of all the children in the family by age was collected from the parents, from which we estimate whether the child had older siblings (yes/no). Among other questions, children were asked if they exercise outside school (yes/no).
Statistical Analysis
Four hundred nineteen children completed the questionnaire. After excluding 40 children with missing information on either outcomes or explanatory variables, the final study size was 379 participants. Descriptive statistics were used to summarize the prevalence of asthma, AR, and eczema in children as well as the distribution of parental education levels in the sample. Afterward, we examined the frequency distributions of a list of explanatory variables in groups defined by the presence or absence of health outcomes. The chi-square test and Fisher’s exact test (if any expected count was less than 5) were used to compare categorical variables between the aforementioned groups. Similarly, we assessed the distribution of the explanatory variables between children with high and low parental education. The P values were reported to indicate statistical significance.
In addition, we evaluated the associations between parental education and asthma, AR, and eczema in children using logistic regression models. Maternal and paternal education were considered separately, and the interaction between these two characteristics was investigated. Adjusted odds ratios (aOR) with 95% confidence intervals (CIs) were estimated for the associations between parental education levels and the outcomes. The model was adjusted for potential confounders described above. All reported probability values (P values) were based on two-sided tests and compared with a significance level of 5%. Statistical software R 4.2.2 was used for the statistical analyses.
Results
Characteristics of the Study Population
Overall, 379 of the 419 (90.4%) children were included in the study. Table 2 summarizes the sample characteristics. “Ever asthma” was reported by 6.3% of the children, while the prevalence of AR and eczema was 20.3% and 27.7%, respectively. In total, 74.9% of the children had at least one parent with a high educational level, while only 25.1% had both parents with low educational levels. 64.6% of the children had highly educated mothers, and 47.8% had highly educated fathers.
Summary of Sample Characteristic: Outcomes and Parental Education (N = 379).
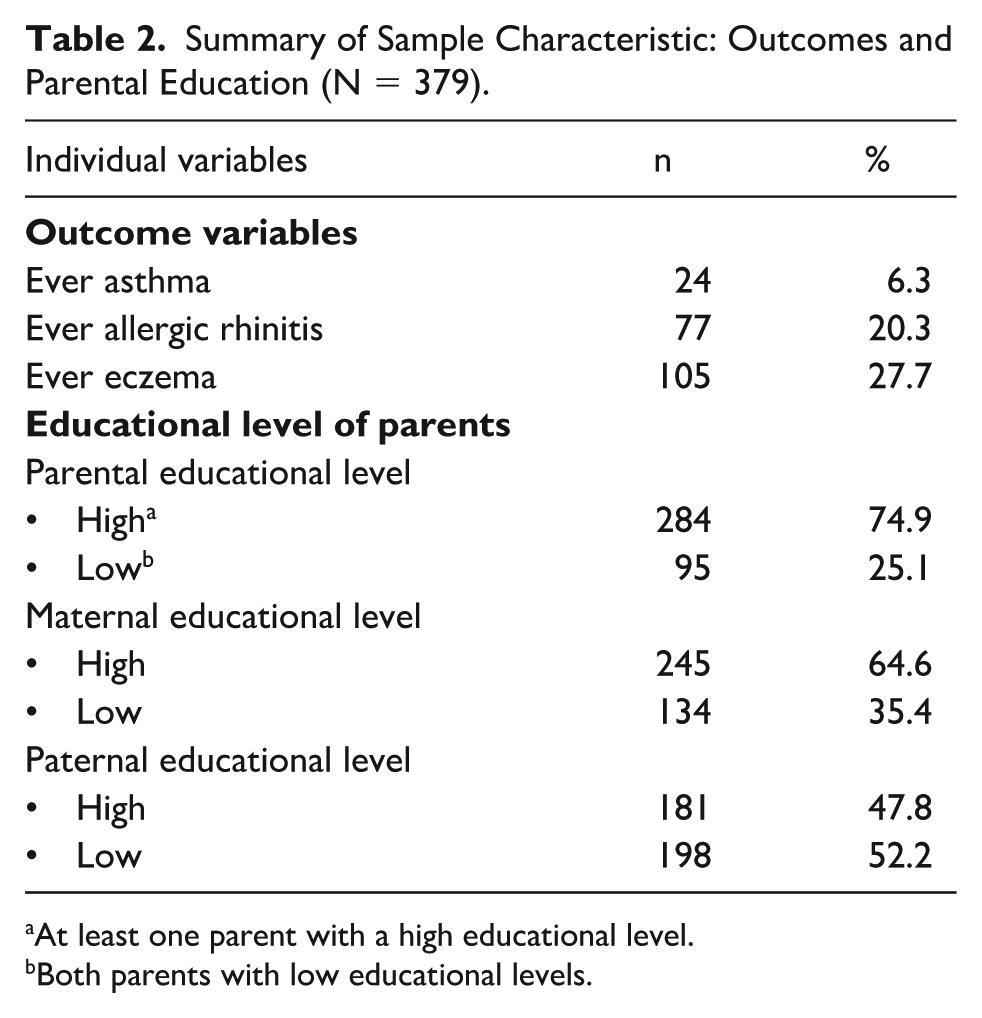
At least one parent with a high educational level.
Both parents with low educational levels.
Explanatory Variables by Health Outcomes
Results of the univariate analysis examining the distribution of the explanatory variables by outcome are presented in Table 3. Children with asthma had a significantly higher rate of NICU admission compared with those without asthma (20.8% vs 5.9%, P = .018), while having at least one older sibling in the family was significantly less common among children with asthma (79.7% vs 58.3%, P = .014). Parental history of atopy was consistently more frequent across all three conditions showing strong statistical significance, which means that children with “ever asthma” (79.2% vs 43.4%, P < .001) or “allergic rhinitis” (63.6% vs 41.1%, P < .001) or “eczema” (56.2% vs 41.6%, P = .011) were more likely to have a parent with atopy. Early day-care attendance was significantly less common among children with AR compared with those without (74.8% vs 63.6%, P = .049). In addition, exercise was more frequently reported among children with AR (94.8% vs 82.5%, P = .007), while current parental smoking was less common in this group (23.4% vs 38.1%, P = .016). Both associations were statistically significant. Breastfeeding was significantly more common among children with eczema (93.3% vs 82.8%, P = .009). All other variables, including sex, delivery mode, prematurity, and obesity, did not show statistically significant differences across the outcomes.
Distribution of Explanatory Variables by Outcome: Frequencies and Percentages.
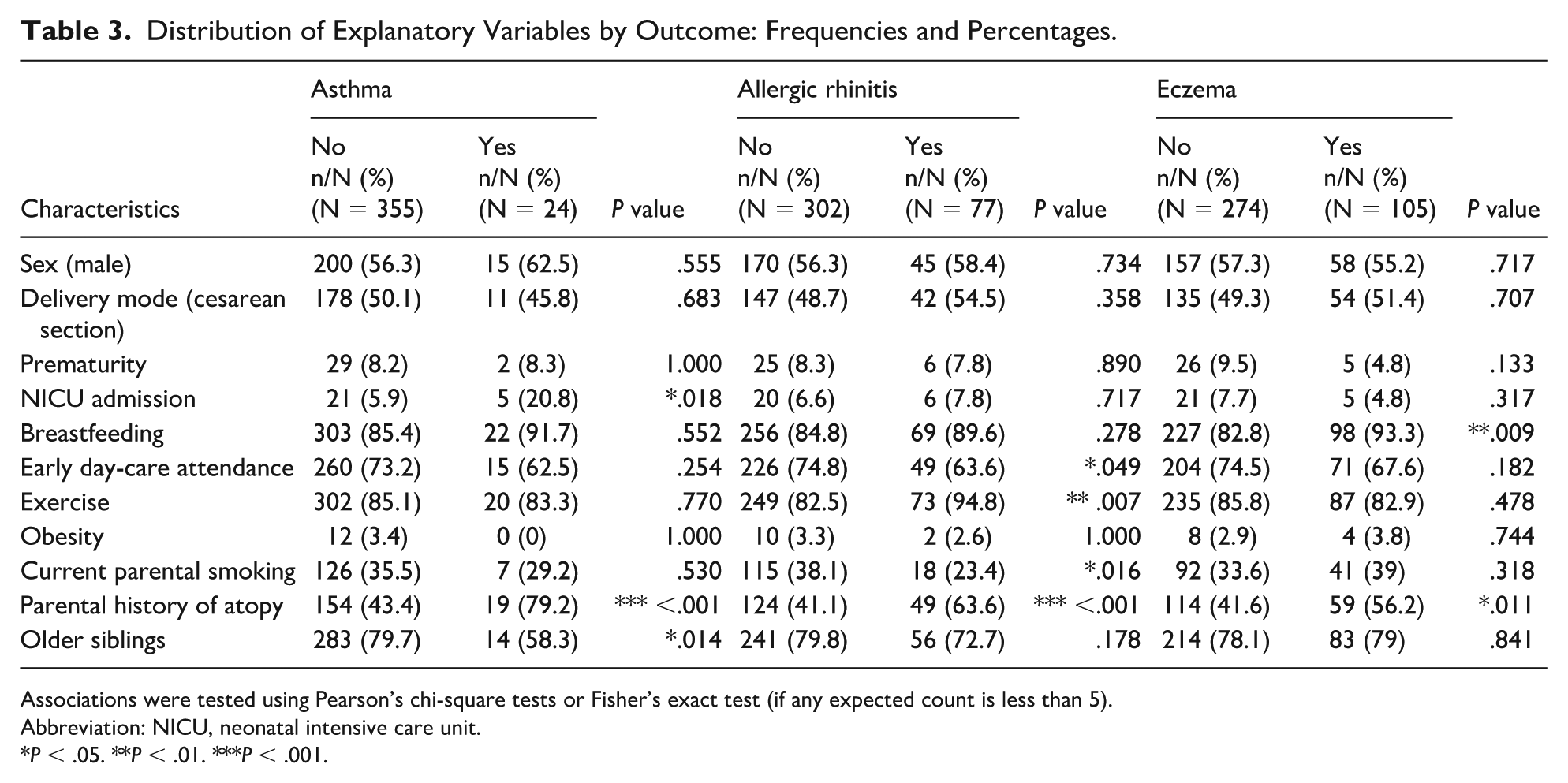
Associations were tested using Pearson’s chi-square tests or Fisher’s exact test (if any expected count is less than 5).
Abbreviation: NICU, neonatal intensive care unit.
P < .05. **P < .01. ***P < .001.
Explanatory Variables by Parental Educational Level
The distribution of the explanatory variables by parental educational level is shown in Table 4. Exercise participation was significantly higher (89.8% vs 70.5%, P < .001), and parental history of atopy was more frequent (51.1% vs 29.5%, P < .001) in children with at least one highly educated parent. Children with high parental education level were also more likely to be breastfed (88.4%) and attend day care at an earlier age (75.7%) compared with those with low parental education (77.9% and 63.2%, respectively). In addition, a higher trend in cesarean section (52.1% vs 43.2%) was shown in children with high parental educational level, and parental smoking (42.1% vs 32.7%) in children with low parental educational level, but the results were not statistically significant.
Distribution of Explanatory Variables by Parental Educational Level: Frequencies and Percentages.

Associations were tested using Pearson’s chi-square tests or Fisher’s exact test (if any expected count is less than 5).
Abbreviation: NICU, neonatal intensive care unit.
P < .05. ***P < .001.
Association Between Parental Education and Asthma
Table 5 presents aORs with 95% CIs for the association between parental education levels and asthma. The results indicate a trend of higher odds of asthma in children with high parental education, but the association was not statistically significant (aOR = 1.44, 95% CI: 0.41-5.005, P = .557). Maternal educational level was not associated with asthma in children (aOR = 1.23, 95% CI: 0.41-3.72, P = .701), nor was the paternal educational level (aOR = 2.43, 95% CI: 0.84-7.02, P = .098). The interaction term between maternal and paternal education for asthma was not significant (P = .605), suggesting that the effect of maternal educational level does not depend on the paternal educational level and vice versa. Therefore, the interaction term was not included in the logistic regression model.
Adjusted Odds Ratios (aORs) With 95% Confidence Intervals (CIs) for the Association Between Outcomes and Parental Education (High vs Low).
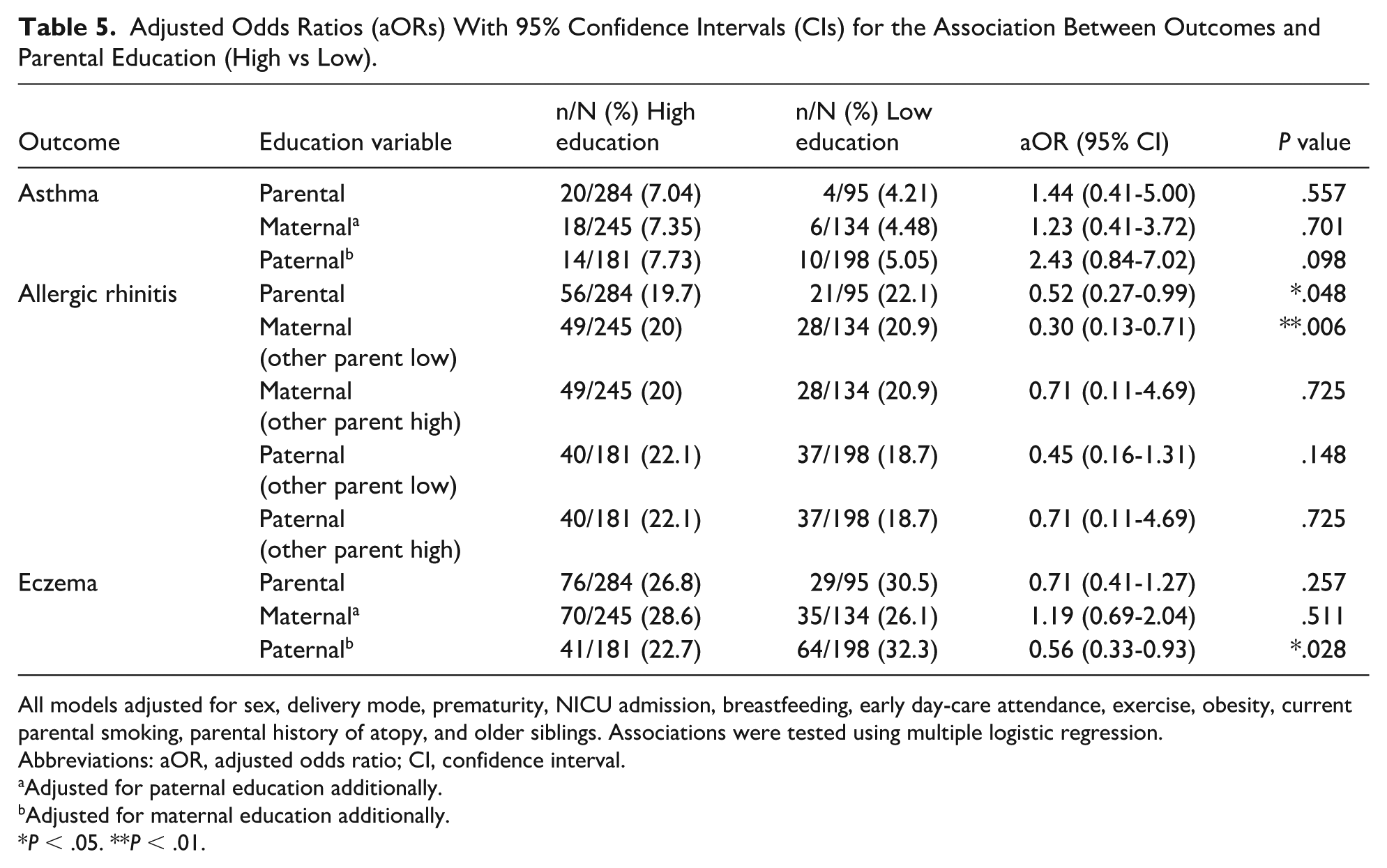
All models adjusted for sex, delivery mode, prematurity, NICU admission, breastfeeding, early day-care attendance, exercise, obesity, current parental smoking, parental history of atopy, and older siblings. Associations were tested using multiple logistic regression.
Abbreviations: aOR, adjusted odds ratio; CI, confidence interval.
Adjusted for paternal education additionally.
Adjusted for maternal education additionally.
P < .05. **P < .01.
Association Between Parental Education and Allergic Rhinitis
As shown in Table 5, high parental education level was significantly associated with reduced odds of AR in children (aOR = 0.52, 95% CI: 0.27-0.99, P = .048), but paternal educational level adjusted for high (aOR = 0.71, 95% CI: 0.108-4.69, P = .725) and low maternal education (aOR = 0.45, 95% CI: 0.16-1.31, P = .148) was not associated. In this case, a significant interaction between maternal and paternal education was observed (P = .015) in the logistic regression model, suggesting that the effect of the education of one parent depends on the education of the other parent. As a result, a significant effect of maternal education was observed, and the effect was stronger when the paternal educational level was low. Children with highly educated mothers and low-educated fathers have 70% lower odds of “ever allergic rhinitis” (aOR = 0.30, 95% CI: 0.13-0.71, P = .006).
Association Between Parental Education and Eczema
The prevalence of eczema was higher in children with low paternal education (32.3% vs 22.7%) compared with those with high paternal education. Moreover, as presented in Table 5, children with highly educated fathers have 44% lower odds of “ever eczema” (aOR = 0.56, 95% CI: 0.33-0.93, P = .028), which is statistically significant. Similarly to asthma, there was no significant interaction between maternal and paternal education (P = .334) in the logistic regression model for eczema, and the interaction term was not included in the model.
Discussion
This study investigates the relationship between parental education and atopic diseases, including asthma, AR, and eczema, in children. The results suggest that children with highly educated parents are less likely to develop AR. By examining maternal and paternal education separately (also checking for interaction between them), we found that children with highly educated mothers are significantly less likely to have AR, especially when they also have low-educated fathers. Furthermore, children with highly educated fathers were less likely to develop eczema.
We investigated various risk factors associated with an increased prevalence of atopic diseases in childhood. Our findings revealed that most of the children with asthma were hospitalized in the NICU after birth. According to existing literature, common causes for NICU admission, such as prematurity, low birth weight, and respiratory distress syndrome (RDS), are strongly associated with childhood asthma.20,21 Moreover, our study observed that most children without asthma had at least one older sibling. This finding is consistent with existing evidence suggesting that having older siblings protects against asthma, as early-life exposure to infections through sibling interactions may promote immune system maturation, shifting the immune response from a Th2-dominant, which is associated with atopy, to a Th1-dominant response. 22 A similar mechanism may also explain the observed inverse relationship between early day-care attendance and AR, as it also increases early-life microbial exposure and may promote immune maturation. Furthermore, a well-established risk factor for the development of atopic diseases in childhood is the parental history of atopy.23-25 In our study, this association was evident across all three conditions, as most of the affected children had at least one parent with a documented history of atopy. This relationship can be partly explained by genetic factors, such as filaggrin gene mutations that damage the skin barrier and contribute to eczema. 26
These risk factors for asthma, AR, and eczema are also influenced by educational level and could explain or alter the association between parental education and atopic diseases in children. According to our results, children with highly educated parents are more likely to be breastfed during infancy, enrolled in daycare at an earlier age, and exercise more. Overall, it appears that parental education is critical, as it promotes health-seeking behaviors and cultivates positive behavioral changes that influence children’s health, nutrition, and well-being.27,28 However, the effect of education on breastfeeding is ambiguous because workplace demands and societal norms for women may reduce duration in some contexts.29,30 Furthermore, higher parental education may also facilitate early daycare enrollment due to greater awareness of its benefits and higher family income.31,32 In addition, more educated parents are more likely to engage in health-promoting behaviors, like exercise, and their children follow their example.33-36 Finally, our results, in line with previous studies, showed that the prevalence of smokers is higher among parents with low educational level, exposing their children to tobacco smoke, a well-established health risk.37-40
The primary objective of our study was to investigate the association between parental educational level and atopic diseases in children. In line with previous studies,41,42 our results indicate no significant association between parental education and asthma. The existing literature highlights the complexity of the relationship between parental education, often used as a proxy for family SES, and childhood asthma. Some studies report a positive association.43-47 Many of these studies differentiate between atopic, usually comorbid with AR, and non-atopic asthma. The positive association between higher parental education and increased occurrence of asthma in their children has been predominantly observed in atopic asthma. The results align with the hygiene hypothesis, which posits that children from families with higher SES/more educated parents are more likely to grow up in more sterile environments that could trigger atopic sensitization. 48 Conversely, other studies have reported a negative association between parental education and asthma in children.49-52 Families with lower SES/less educated parents often face adverse household conditions, adopt health-compromising behaviors, and find difficulties in recognizing asthma symptoms or adhering to therapy. These challenges lead to uncontrolled asthma and a low quality of life for affected children.53,54
Regarding AR and eczema, the current literature is more consistent. Most studies report a higher prevalence of these conditions in children with highly educated parents.55-58 Several explanations for this positive association have been proposed, including the hygiene hypothesis. Another possible explanation is that high-SES individuals tend to report allergy symptoms and seek medical care more frequently compared with low-SES individuals, who are underdiagnosed. 59 However, a cross-sectional study in Denmark showed that while eczema was associated with higher parental education, AR was more prevalent in children with less educated parents. 60 These findings were supported by a German study suggesting that the lifestyle of high-SES parents protects children from developing atopic diseases, except for eczema. 61
In line with these findings, our study observed that children with highly educated parents, especially mothers, are less likely to develop AR. This observation deviates from the prevailing literature, which, based on the well-established hygiene hypothesis, suggests that AR is more prevalent among children of highly educated parents. On the contrary, we suggest that maternal education has a protective effect on AR. Higher-educated mothers may be more likely to be employed outside the home and, as a result, may enroll their children in day care at an earlier age. 12 Early attendance at day care has been associated with increased microbial exposure, which may contribute to immune system maturation and a reduced risk of AR.62,63 Our results support that early day-care attendance is a protective factor against AR in children. Furthermore, the significant interaction between maternal and paternal education level in relation to AR represents a novel contribution to the literature, suggesting that the educational profile of each parent cannot be considered in isolation when analyzing the risk of atopic disease.
Regarding eczema, our results revealed a higher prevalence in families with lower paternal educational level, which aligns with studies from Turkey 64 and the United States 65 reporting that lower paternal education and socioeconomic disadvantage are associated with higher eczema frequency and severity in children. This contrasts with findings from Japan 66 that children whose fathers had a higher educational level had an increased risk of eczema. Our finding also contrasts with the hygiene hypothesis supported by the broader literature. This discrepancy may reflect population-specific socioeconomic and cultural characteristics, highlighting the importance of context when interpreting the relationship between parental education and atopic outcomes. 64 Further studies in Southern European and Mediterranean areas should be conducted to clarify specific environmental, regional, and cultural factors that influence the association between socioeconomic determinants and atopy.
In this context, the findings of the present study may be partly explained by cultural characteristics specific to Mediterranean populations, such as the Greek. Our results contradict the hygiene hypothesis, which suggests that higher parental education is associated with increased atopic risk due to reduced early-life microbial exposure. However, higher parental education in Greece is often linked with greater adherence to the Mediterranean diet, which has anti-inflammatory and immunomodulatory effects that may protect against allergic diseases.14,67,68 In addition, strong extended Greek family networks, which are a distinctive feature of Greek social organization, including frequent contact with grandparents, may increase early-life microbial exposures and promote immune maturation. 69 Together, these population-specific factors may attenuate or even reverse the associations predicted by the hygiene hypothesis, highlighting the importance of cultural context in interpreting socioeconomic gradients in atopic diseases.
The major limitation of this study is that, although standardized and widely validated instruments such as the ISAAC questionnaire were employed, the assessment of atopic outcomes was based on parental self-report rather than physician-confirmed diagnoses, which may have introduced recall bias. Nevertheless, the use of the ISAAC questionnaire, which was specifically developed for epidemiological research where clinical verification is not feasible, supports the reliability and international comparability of our findings. In addition, potential selection bias may exist, as schools were selected based on broadly recognized socioeconomic and demographic characteristics of the study areas rather than using a formal SES index or predefined selection criteria. Response bias also cannot be excluded, as parents with lower education levels may have been less likely to participate or complete the questionnaires. Furthermore, although the sample size was adequate, the number of asthma cases was relatively small, which may have limited the statistical power of the analyses and resulted in imprecise estimates. This limitation may have been further compounded by the inability to distinguish between atopic and non-atopic asthma. Moreover, the small number of parents with primary-level education required merging this group with those with secondary education, which may have obscured potential differences. Although several established confounders were included in the analyses, their selection was limited to the variables available in the questionnaire. Consequently, other relevant factors, such as household conditions, environmental exposures, or birth weight, were not assessed. In addition, parental history of atopy was treated as a combined binary variable, without differentiating between maternal and paternal, and thereby limiting a more detailed assessment of familial or genetic risk. Finally, although parental education is commonly used as an indicator of socioeconomic position, it does not fully capture all the dimensions of SES, such as income, occupation, or living conditions. To fully understand the socioeconomic dimension of allergic diseases in children, future studies should investigate additional proxies of family SES and assess parental characteristics separately for mothers and fathers, as their contributions to both socioeconomic environment and familial risk may differ.
This study expands the current evidence on the impact of parental education on atopic diseases in children and highlights the complex relationship between SDoH, such as education, and health outcomes. Our findings suggest that parental education influences atopic diseases in children differently depending on the disease and the parent. Thus, children with highly educated parents, especially when mothers were highly educated and fathers were not, were less likely to develop AR, and children with highly educated fathers are less likely to have eczema. Future research should clarify the different pathways through which SDoH influence health to help public health policymakers make targeted interventions that address disparities and promote health equity.
Author Contributions
ANT collected the data, drafted, and reviewed the manuscript. VK contributed to data acquisition. EV performed the statistical analysis and interpreted the data. GA, KD, and DM designed the study, supervised the work, and critically revised the manuscript. All authors have read and agreed to the published version of the manuscript.
Footnotes
Ethical Considerations
This study is a secondary analysis of data collected as part of the PANACEA II study (Physical Activity, Nutrition and Atopy in Children in Athens II), for which the authors were investigators. The study was approved by the Ethics and Research Deontology Committee of the National and Kapodistrian University of Athens (protocol number: 729/24-02-2023) and the Institute of Educational Policy (protocol number: 23/06-04-2023). For the accomplishment of the study, permission was issued by the Ministry of Education and Religious Affairs (protocol number: Φ15/41793/ΑΛ/45478/Δ1/21-04-2023, study extension protocol number: Φ15/115362/ΑΛ/120284/Δ1/25-10-2023). The study was conducted in accordance with the guidelines of the Declaration of Helsinki.
Consent to Participate
Written informed consent to participate was obtained from all parents or legal guardians of the children who participated in the study.
Consent for Publication
The written informed consent for participation obtained from all parents or legal guardians included information about the research purpose and the use of anonymized data, with assurance that no identifiable personal data would be collected or published. Therefore, additional consent for publication was not required.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data sets generated and/or analyzed during the current study are not publicly available due to privacy and ethical restrictions, but they are available from the corresponding author upon reasonable request.