
Abstract
Campylobacter infection in children is a common bacterial illness that mostly causes gastroenteritis and typically presents with diarrhea that may or may not be bloody, emesis, or abdominal pain. However, pediatric cases of bacteremia are rarely reported. Our objective was to report our tertiary center experience with Campylobacter bacteremia in a pediatric population. This 16-year retrospective study was performed at a tertiary-affiliated pediatric medical center. Data were collected from all patients with Campylobacter bacteremia during the study period. We identified 37 pediatric patients with Campylobacter bacteremia. Most children (n = 30, 81%) had severe underlying medical conditions, including malignancy and primary immunodeficiency. Only 7 (18.9%) children were previously healthy. The median age was 6.8 years, and children with severe underlying medical conditions were older than previously healthy children (9 vs. 1.2 years, P = .02). Most children present with fever and/or gastrointestinal symptoms. Campylobacter jejuni was the most common species (n = 30, 81%), and most isolates tested for antibiotic susceptibility were susceptible to macrolides. While one child was hospitalized in the intensive care unit because of septic shock, the outcome for all children was favorable. Campylobacter bacteremia is an uncommon complication of Campylobacter infection in children and has been reported more frequently among immunocompromised patients. Most children present with fever or gastrointestinal symptoms. Even in this predominantly immunocompromised population, the outcome is generally favorable, with most cases resolving without complications. Macrolides remain the antibiotic of choice for Campylobacter infections, including bacteremia.
Keywords
Introduction
Campylobacter species are gram-negative, spiral-shaped bacteria, 1 and the incidence of infection in the past decade is on the rise. 2 Campylobacter infection in children is a common bacterial illness caused primarily by C. jejuni and Campylobacter coli. 3 The bacteria are typically spread through the consumption of contaminated food or water, particularly undercooked poultry, unpasteurized milk, and contaminated produce. Campylobacter infections cause gastroenteritis and typically present with diarrhea that may or may not be bloody, emetic, or abdominal pain. While the disease is self-limited in most healthy pediatric populations, severe infection with Campylobacter has been reported in certain populations, including immunocompromised individuals and those with underlying medical conditions.4,5 Among these complications, bacteremia has rarely been reported.
Because of its rarity, most reports on Campylobacter bacteremia (CB) in children are based on case reports or small case series.6,7 The largest study on CB in children was conducted over a 22-year period (1989-2010) and identified 76 episodes in children, with an overall incidence of 1.59 per 100 000 children per year. 8 Among the enrolled children, only 14 had an underlying risk factor for infection, whereas most children were previously healthy. 8 However, over the last few years, the prevalence of immunosuppressive conditions in the pediatric population has increased, with a prevalence of 2.6% among children in the United States. 9 While Campylobacter enteritis is the most commonly identified cause of foodborne illness in the United States, 3 we expect to see an increasing number of Campylobacter infections, including bacteremia, in immunocompromised children.
Thus, we aimed to report our tertiary center experience with CB in an era of 16 years to better understand the epidemiology, risk factors, optimal management strategies, and outcomes in a real-life pediatric population.
Methods
This retrospective study was conducted at Schneider Children’s Medical Center, a tertiary pediatric hospital. We enrolled patients younger than 18 years with at least 1 positive blood culture for Campylobacter species. For this study, only the first hospitalization for each bacteremic patient was recorded between 2008 and 2023.
All records of the patients with CB episodes were reviewed, and all demographic, epidemiological, clinical, laboratory, and treatment courses were collected.
Microbiological Methods
Blood was inoculated into Bactec Peds Plus/F (BD). Upon receipt in the clinical microbiology laboratory, all Bactec blood culture bottles were incubated in a Bactec FX incubator (BD) for up to 7 days. Once positive, the blood culture bottles were aseptically inoculated into blood agar, MacConkey, and chocolate agar (HyLabs Rehovot) and incubated for 18 to 24 hours at 37 °C and 5% CO2. A Gram-stained slide was also prepared and reported within 1 hour of positivity. Starting in 2014, blood cultures yielding gram-negative organisms were identified using matrix-assisted laser desorption ionization–time of flight mass spectrometry (MALDI-TOF MS), either directly from positive blood culture broth or from subcultured isolates. Prior to 2014, organism identification was performed using conventional biochemical methods.
After 24 hours of incubation of the positive blood culture broth in a microaerophilic environment, small gray colonies were noted on sheep blood agar and chocolate agar plates. The organism subspecies were identified by MALDI-TOF MS (Bruker Daltonics).
The antimicrobial susceptibility of C. jejuni and C. coli isolates was tested and interpreted according to the guidelines of the Clinical and Laboratory Standard Institute (CLSI, M45-A3). 10 For non-jejuni/coli Campylobacter species, where CLSI breakpoints are not established, interpretations were based on the criteria proposed by the Antibiogram Committee of the French Society of Microbiology (CA-SFM). 11
Statistics
For descriptive statistics, continuous variables are presented as mean ± standard deviation (SD) or as median and interquartile range (IQR) according to their distribution, whereas categorical data are presented as the sum and percentages within the study group. Mann-Whitney U tests were used for ordinal and continuous variables that did not match the parametric criteria. Analysis was performed using the IBM Statistical Package for the Social Sciences (SPSS) version 24.0. Statistical significance was set at a P value of .05. This study was approved by the institutional Helsinki Committee, approval number 0026-24-RMC.
Results
During the study period, we identified 37 children with 37 episodes of CB: 25 males (67%) and 12 females (32%). The median age was 6.8 years (range: 3 weeks to 18 years). More than half of the episodes (51%) occurred during summer.
As shown in Table 1, the majority of children had significant underlying medical conditions, including malignancies (n = 19, 51%) and primary immunodeficiencies (n = 5, 13%). Only 7 (19%) children were previously healthy. Among the 16 children with acute lymphoblastic leukemia (ALL), 8 presented with severe neutropenia (absolute neutrophil count <500/µL). Children with severe underlying medical conditions including malignancy and primary immunodeficiency were older than previously healthy children (9 vs. 1.2 years, P = .019).
Demographic and Clinical Characteristics of Children With Campylobacter Bacteremia.
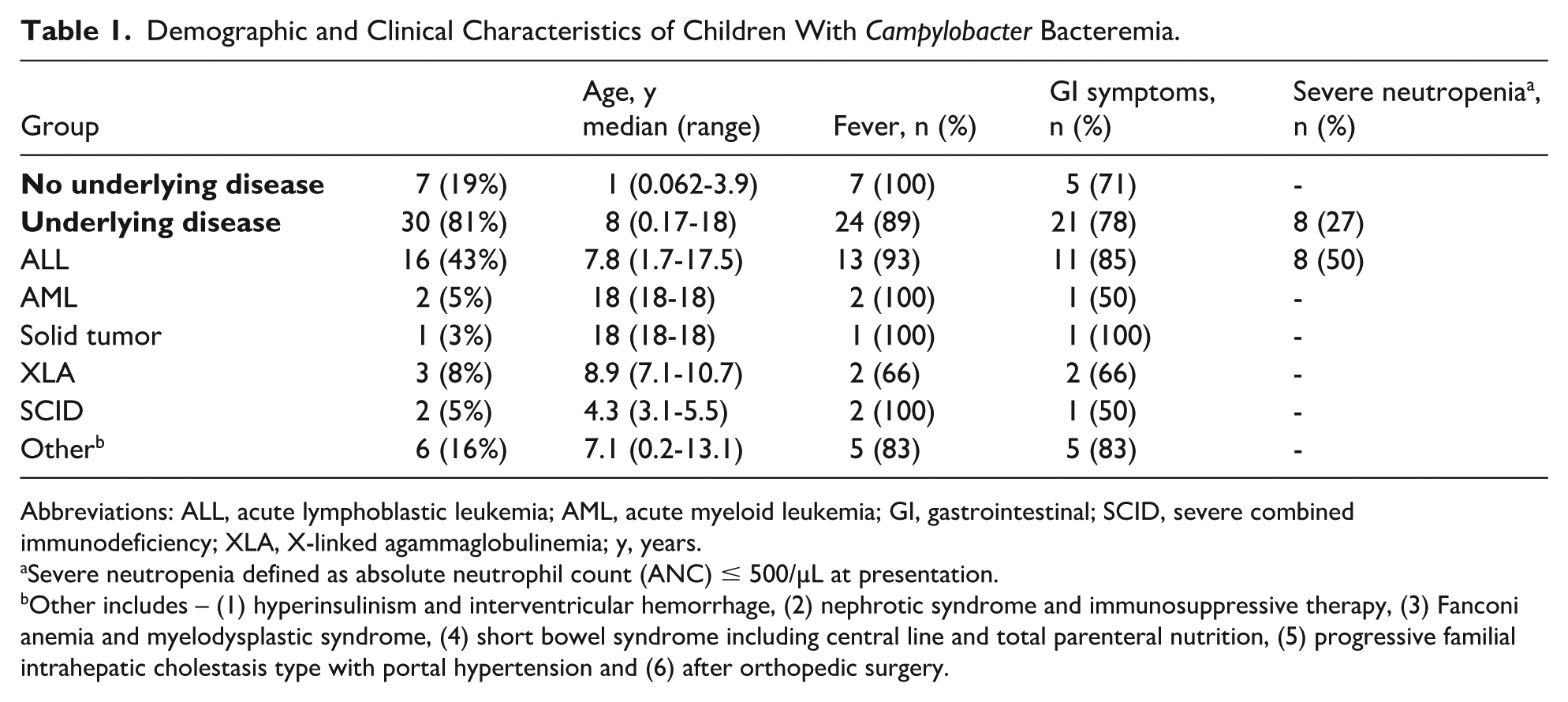
Abbreviations: ALL, acute lymphoblastic leukemia; AML, acute myeloid leukemia; GI, gastrointestinal; SCID, severe combined immunodeficiency; XLA, X-linked agammaglobulinemia; y, years.
Severe neutropenia defined as absolute neutrophil count (ANC) ≤ 500/µL at presentation.
Other includes – (1) hyperinsulinism and interventricular hemorrhage, (2) nephrotic syndrome and immunosuppressive therapy, (3) Fanconi anemia and myelodysplastic syndrome, (4) short bowel syndrome including central line and total parenteral nutrition, (5) progressive familial intrahepatic cholestasis type with portal hypertension and (6) after orthopedic surgery.
At presentation, most (92%) children had fever (≥38 °C), and 76% had gastrointestinal symptoms, including abdominal pain, diarrhea, or vomiting. The mean age of children presenting with gastrointestinal symptoms was lower than that of children without gastrointestinal manifestations (7 vs. 9 years), although this difference was not statistically significant (P = .3479). Only 1 child with X-linked agammaglobulinemia (XLA) presented without fever or gastrointestinal symptoms.
One child (3%) with T-cell acute lymphoblastic leukemia (T-ALL) fulfilled criteria for septic shock at presentation.
C-reactive protein (CRP) at presentation ranged from 0.03 mg/dL to 41 mg/dL, with a mean of 5.2 mg/dL and a median of 2.4 mg/dL.
As seen in Table 2, the most common species causing CB was C. jejuni, accounting for 84% of the cases, followed by C. coli (11%), and Campylobacter species (5%). The distribution of Campylobacter species was similar between previously healthy children and those with severe underlying medical conditions. Specifically, infections with C. jejuni and C. coli were observed in both groups.
Microbiological Characteristic.
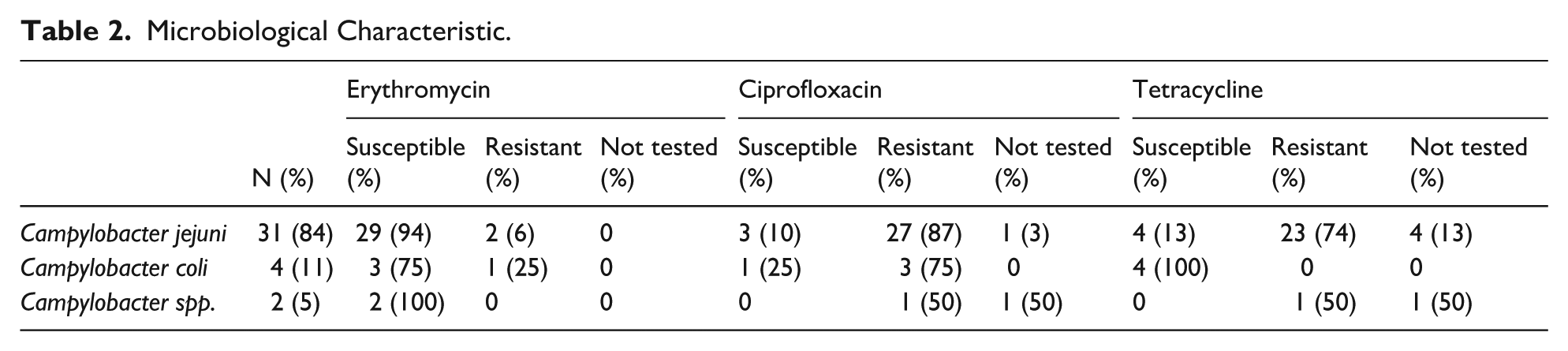
Susceptibility testing showed high resistance to ciprofloxacin (89%) and tetracycline (75%), while erythromycin resistance was rare (8%) across isolates.
Most of our patients (n = 22, 60%) were treated with macrolides alone or in combination with other antibiotics, based on the susceptibility profile. Seven (19%) children were treated with carbapenems; all of them had underlying immunosuppression, and 12 (32%) were treated with aminoglycosides.
Treatment duration varied but tended to be longer in patients with an underlying disease (median 14 days, range 4-42) compared to previously healthy patients (median 10 days, range 7-14; P = .14).
Notably, in our institution, the treatment protocol for neutropenic fever is piperacillin/tazobactam combined with amikacin. Among the 8 children with ALL and neutropenic fever at presentation, all were treated empirically with this combination, and in all cases, only the first culture identified CB, while repeat blood cultures were all negative. After the identification of CB, the treatment was changed to macrolides in all cases.
Discussion
Herein, we describe the largest cohort of pediatric children comprising 16 years of follow-up on CB. Although CB is a severe disease with many potential complications, our data show a favorable course of disease and good outcomes even in a specific pediatric population with severe underlying diseases.
In contrast to prior medical literature on pediatric patients with CB, our data show that most hospitalized children have severe underlying chronic diseases, mostly hematological malignancies. Ben-Shimol et al 8 described the largest cohort to date in children with CB; however, out of 60 described children, 46 were previously healthy. We believe that the difference between the two studies lies in the nature of the two institutes; our center serves as an affiliated tertiary center, with many beds dedicated to oncological children. In contrary, Ben-Shimol et al 8 described a more common disease in Bedouin children who reside in the southern part of our country.
A retrospective review from an urban tertiary care hospital in Soweto and a rural mission hospital in Eastern Transvaal, South Africa, showed that most (84%) of the children with CB had malnutrition. 4 We believe that the discrepancy between our experiences and the literature partially lies in the differences between the study settings and hospitals. Our hospital is the largest affiliated center that cares for many chronically ill children and is based in an urban setting. As nowadays more children are treated successfully for different chronic medical conditions, we believe our study’s implications will be even more relevant.
In our study, which included many children with severe underlying medical conditions, most children presented with fever (92%) and gastrointestinal symptoms (76%), including abdominal pain, diarrhea, or vomiting. In the Ben-Shimol et al 8 series, only 64% of chronically ill children presented with fever, and less than half of the patients (43%) presented with gastrointestinal symptoms. Again, these two reports are different in the nature of pediatric population as was already mentioned.
CB can be severe, especially in immunocompromised patients. However, similar to what has been described in previous studies, most children had a benign disease course, no postinfectious immune phenomenon were noted, and none of the patients developed septic shock or required intensive care hospitalization. 8 This may be due to the early recognition of the infection and prompt supportive treatment with early microbiological isolation and proper antibiotic treatment.
As described in previous studies, the most common bacteria isolated in blood cultures was C. jejuni, followed by C. coli and other unidentified Campylobacter species.8,12 Although most isolates in our cohort were susceptible to macrolides, our study was not designed to evaluate the comparative effectiveness of different antimicrobial regimens. Notably, several severe cases required broad-spectrum or combination therapy, including carbapenems or aminoglycosides. Therefore, our findings should be interpreted with caution, and no definitive recommendation regarding first-line therapy can be made. Thus, the treatment of CB remains controversial.
Interestingly, the 8 patients with ALL-associated neutropenic fever were treated with piperacillin-tazobactam and amikacin upfront improved without sequelae or persistent bacteremia. This can be explained by the fact that even though it is not tested under CLSI recommendations, it is known that most strains are susceptible to aminoglycosides, and therefore, these children were most probably treated effectively from their presentation.
This study has several limitations, including its retrospective nature and relatively small number of cases. However, to the best of our knowledge, this is the largest series to report a cohort of chronically ill children. Moreover, our data are limited by the fact that they represent only a single institution, which limits its external validity and generalizability to other populations. Another limitation is the fact that data on high-risk food consumption was not collected in our study. Indeed, eating habits as well as international travel were found in the past to serve as possible exposure to Campylobacter infection.12,13
In conclusion, CB in children is a possible manifestation of Campylobacter infection, and in our center, it was found to primarily affect immunocompromised children. Despite the vulnerability of this patient population, the prognosis is generally positive, with most cases resolved without complications. Macrolides continue to be the preferred antibiotics for treating Campylobacter infections, including CB.
Author Contributions
LG: Conceived and designed the study; contributed to acquisition, analysis, and interpretation of data; drafted the manuscript.
AS: Contributed to acquisition of data; critically revised the manuscript.
DL: Contributed to conception; critically revised the manuscript.
EB: Conceived and designed the study; contributed to acquisition, analysis, and interpretation of data; drafted the manuscript.
SF: Contributed to conception; critically revised the manuscript.
HB-Z: Contributed to acquisition of data; critically revised the manuscript.
NS: Conceived and designed the study; contributed to acquisition, analysis, and interpretation of data; drafted the manuscript.
Footnotes
Ethical Considerations
This study was approved by the institutional Helsinki Committee, approval number 0026-24-RMC.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.