
Abstract
Restricted diet therapy is the cornerstone of treatment in many hereditary metabolic disorders. This study evaluated the effects of dietary treatments for affected children on the dietary habits, lifestyle, quality of life, and stress levels of their mothers. The study included 50 mothers of children aged 2 to 18 years with phenylketonuria, organic acidemias, urea cycle defects, or galactosemia, and 32 mothers of healthy children. Mothers completed a demographic and lifestyle questionnaire, the Short Form-36 Quality-of-Life questionnaire, and the Perceived Stress Scale. More than half of the mothers in the patient group reported modifying their own diets to align with their child’s restrictions, while some adopted vegetarian or vegan diets. Many reported limiting social activities, and 18% had quit their jobs to manage dietary treatment. Mothers of affected children showed significantly higher stress scores and lower quality-of-life scores than controls.
Introduction
Dietary restrictions in hereditary metabolic diseases constitute the mainstay of treatment for many metabolic conditions, although the rules vary depending on the disease. For example, in amino acid metabolism disorders, the amount of amino acids consumed in the patient’s daily diet must be restricted; for this purpose, animal-based foods and high-protein foods such as legumes and nuts are excluded from the patient’s diet. While such highly restricted diets are essential for metabolic control, long-term dietary limitation requires careful monitoring to prevent growth impairment and micronutrient deficiencies.1-3 Inadequate dietary adherence may increase the risk of metabolic crises, which may contribute to increased parental concern.4-8
Specially prepared amino acid formulas and low-protein products such as reduced-protein milk, rice, flour, and flour-based products are used for these patients. It is necessary to prepare special foods for children both at home and at school/work, which consumes considerable time and effort.9,10 Since the management of this challenging process is primarily handled by mothers in many clinical and cultural contexts, mothers often serve as the main caregivers responsible for daily dietary management and monitoring of metabolic control. Therefore, focusing specifically on mothers provides a relevant perspective for understanding caregiver burden in this population. This caregiving role may lead to deterioration in quality of life, as well as increased sadness, anxiety, and depression.9,11-15 However, it remains unclear whether mothers of children with inherited metabolic disorders modify their own dietary habits or adapt family dietary patterns in response to the child’s restricted diet.
The aim of this study was to investigate whether mothers of patients with amino acid metabolism disorders (phenylketonuria, urea cycle defects, and organic acidemia) and carbohydrate metabolism disorders (galactosemia), who follow disease-specific restricted diets, modify their own dietary habits and limit their social activities, and to examine the potential effects of these factors on their quality of life and stress levels.
Materials and Methods
Study Groups
This cross-sectional and descriptive study was conducted between October 2022 and June 2023 at the Division of Pediatric Metabolism, Dokuz Eylül University, İzmir, Turkey, with the aim of investigating the dietary habits of mothers of children on a restricted diet. The a priori sample size was calculated using G*Power version 3.1.9.7 based on an independent-samples t test. Assuming a significance level of 0.05, 80% power, and a large effect size (Cohen’s d = 0.80), the required sample size was estimated as 52 participants in the patient group. The assumption of a large effect size was based on previous studies reporting substantial differences in stress and quality-of-life measures among caregivers of children with chronic metabolic conditions. The study included the mothers of 50 patients aged 2 to 18 years. As a control group, the mothers of 32 healthy children aged 2 to 18 years, who had no chronic physical or psychiatric diseases and visited the hospital for screening purposes (such as hyperlipidemia, hypothyroidism, or anemia screening), were included. For families with more than one affected child, the older sibling was included in the study. Definitive diagnoses of the patients were established through biochemical and genetic testing. Patients who had been regularly followed for at least 2 years with a diagnosis of classical phenylketonuria, organic acidemia, urea cycle defects, and classical galactosemia, were on a restricted diet and compliant with dietary treatment; who lived with their mothers; and whose diet was managed by their mothers were included in the study. Since the first 2 years after diagnosis represent the period during which families accept and adapt to the disease and dietary treatment, 16 only patients who had been on dietary treatment for more than 2 years were included. Patients on semi-restricted diets, those fed via nasogastric tube or gastrostomy, patients who had undergone liver transplantation, and those with other conditions requiring additional treatments or diets (such as genetic, autoimmune, allergic, or neoplastic disorders) were excluded. Moreover, mothers with chronic disorders severe enough to affect their daily activities were excluded, as such disorders may influence maternal quality of life. 17 In addition, mothers who had a disease requiring dietary restrictions themselves, those with psychiatric disorders such as schizophrenia, single mothers, and mothers who did not speak Turkish were also excluded from the study.
On the day of the patients’ outpatient clinic visit, after completion of the examination and laboratory workup, the mothers were asked to complete the investigator-prepared questionnaire, along with the Perceived Stress Scale (PSS) and the Quality-of-Life forms. The entire process was conducted face-to-face in a quiet room where the mothers could be alone, with the questions explained to them and sufficient time provided to respond. The interviews with the mothers were completed within 45 to 55 minutes.
Scales Used in the Study
Questionnaire Form
The questionnaire was developed by the research team based on a comprehensive review of the relevant literature and clinical experience in pediatric metabolic disorders. Content validity was evaluated using expert review and the Davis technique. Experts in pediatric metabolism and clinical nutrition assessed each item for clarity and relevance, and revisions were made accordingly. As the questionnaire was designed to explore specific dietary behaviors and social adaptations within this clinical population, formal internal consistency testing was not performed. However, items were discussed with participants during face-to-face administration to ensure clarity and consistent interpretation.
The first section (8 questions) included information on the sociodemographic characteristics of the child and the family. In the second section (17 questions), information on special diet preparation and dietary habits was collected; in the third section (4 questions), information on nutrition in out-of-home settings was obtained; and in the final section (6 questions), questions related to the mother’s individual health were asked during face-to-face interviews. Intake values were derived from self-reported frequency of consumption and represented estimated monthly consumption counts.
Perceived Stress Scale
This scale was developed by Cohen et al. 18 The 14-item scale is designed to measure the degree to which certain situations in a person’s life are perceived as stressful. Participants rate each item on a 5-point Likert scale ranging from “Never (0)” to “Very Often (4).” Scores range from 0 to 56, with higher scores indicating a higher perceived level of stress. There are no cutoff points used to classify stress levels. The validity and reliability study of the Turkish version of this scale was performed by Eskin et al. 19
Quality-of-Life Scale
In the study, the Short Form-36 (SF-36) scale, developed by Ware in 1987 and whose validity and reliability study in Türkiye was conducted by Koçyiğit et al, 20 was used to assess the quality of life of mothers of children diagnosed with phenylketonuria. The form, intended to evaluate participants’ overall quality of life and their quality of life in the past 4 weeks, was administered during participant interviews. The SF-36 scale consists of 2 main dimensions, physical and mental, and 8 subscales, each representing a separate health indicator. The SF-36 scale comprises a total of 36 questions, with each subscale scored between 0 and 100, where higher scores indicate better quality of life. The scores of the questions included in each subscale are weighted and summed to obtain the subscale score, and summary health scores are subsequently calculated from these subscale scores. 21 Missing items in the PSS and SF-36 questionnaires were handled according to standard scoring procedures. Participants with incomplete scale responses were excluded from the relevant analysis. The proportion of missing data was minimal and did not exceed acceptable limits.
Ethical Approval
Ethical committee approval for the study was obtained from the Non-Interventional Research Ethics Committee of Dokuz Eylül University Faculty of Medicine on October 26, 2022 (protocol number: 7560-GOA; decision number: 2022/34-29). The study protocol was designed in accordance with the Declaration of Helsinki. Informed consent was obtained from the patients’ parents at the time of participation.
Statistical Analysis
We used the SPSS version 20.0 package program for all analyses. Data were expressed as mean ± standard deviation or as percentages. The chi-square test was used to compare group proportions, and Fisher’s exact chi-square test was used if the expected values in any cell were below 5. The Shapiro-Wilk test was performed to evaluate the normality of continuous variables. For the comparison of group means, the Student’s t test was used; if the data did not follow a normal distribution, the Mann-Whitney U test was applied. Because monthly consumption counts were skewed, required versus actual within-family consumption frequencies were compared using the Wilcoxon signed-rank test. Spearman’s rho correlation analysis was conducted to investigate the correlation between the variables. A correlation coefficient (r value) of 0.10 to 0.29 was considered indicative of a low correlation, 0.30 to 0.49 a moderate correlation, and above 0.50 a strong correlation. Because multiple comparisons were performed for PSS, Physical Component Summary (PCS), Mental Component Summary (MCS), and SF-36 subscale scores, P values in Table 3 were additionally evaluated using the Holm-Bonferroni procedure. To account for sociodemographic differences between groups, separate multivariable linear regression analyses were performed for PSS, PCS, and MCS, including group status, maternal employment, maternal education, number of children, and household size as covariates. For all statistical analyses, a P value of less than .05 was considered statistically significant.
Results
Demographic and Clinical Features of Cohort
A total of 82 children and their mothers, including 50 patients and 32 controls, were included in the study. In the patient group, 34 patients (68%) were followed and treated for classical phenylketonuria, 8 patients (16%) for organic acidemia, 4 patients (8%) for urea cycle defects, and 4 patients (8%) for classical galactosemia. No significant differences were found between the patient and control groups in terms of the children’s age and sex, parents’ age, and mothers’ educational background (Table 1). Significant differences were observed between the patient and control groups regarding the mean number of children in the family, size of household, and number of mothers engaged in income-generating work. The sociodemographic characteristics of the patient and control groups are presented in Table 1. Several sociodemographic characteristics differed between the patient and control groups. These differences were considered in the interpretation of subsequent analyses.
Sociodemographic Characteristics of Patient and Control Groups.
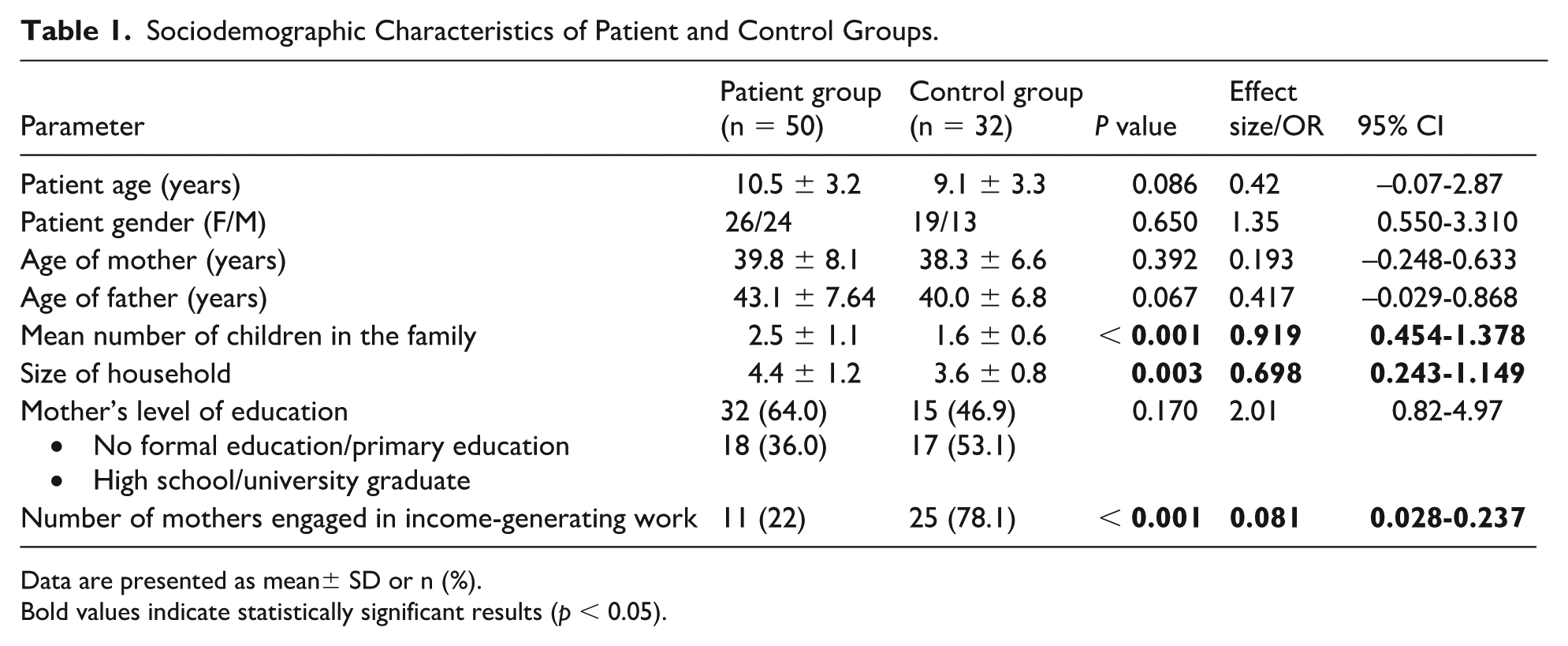
Data are presented as mean± SD or n (%).
Bold values indicate statistically significant results (p < 0.05).
Of the mothers in the patient group, 39 (78.0%) were full-time housewives, and 9 of them (18.0%) had quit their jobs to manage their child’s dietary treatment and other therapies regularly. Among the 9 non-working mothers, 2 had children with phenylketonuria, 3 with organic acidemia/urea cycle defects, and 4 with galactosemia. Five of these mothers had one child each with a metabolic disorder, while 4 mothers had 2 children with metabolic disorders. In the patient group, 39 mothers (78.0%) reported that their child’s dietary treatment imposed an additional financial burden on the family, and 31 of these mothers were not employed.
Findings on Special Diet Preparation and Dietary Habits
In the patient group, 5 children (10.0%) were not eating meals together with their families. In the control group, all children were eating meals together with their families. In the patient group, the mothers of 5 children who were not eating with the family stated that their children ate separately from the rest of the family during meals to prevent them from developing an interest in the family’s food. Among the mothers in the patient group, 39 (78.0%) reported feeling distressed because their children had to follow a restricted diet of natural foods.
The mothers of the patients reported preparing an average of 2.3 ± 0.7 different dishes per day for their affected child, 2.4 ± 0.8 different dishes for other family members, and a total of 3.7 ± 0.9 different dishes overall. Of the 46 mothers of children with amino acid metabolism disorders, 23 (50.0%) reported that they restricted the intake of protein-rich foods, which the rest of the family would normally consume, in a manner compatible with the patient’s diet. Among these mothers, a significant difference was observed between the amount of protein-rich foods they believed should be consumed monthly and the amount actually consumed in practice (Table 2). Intake values were derived from self-reported frequency data and represented estimated monthly consumption counts. Due to the skewed distribution of consumption frequencies, within-family comparisons were performed using a nonparametric paired test. Within-family comparisons of perceived required and actual monthly consumption frequencies were performed using the Wilcoxon signed-rank test. Across food groups, effect sizes were large (r = 0.88-0.90). Hodges-Lehmann paired-difference estimates were 7.5 (95% CI 6.0-9.0) for red meat products, 6.0 (95% CI 4.5-7.5) for chicken, 2.5 (95% CI 2.0-3.0) for fish, 22.0 (95% CI, 18.0-26.0) for eggs, 17.5 (95% CI 12.0-21.0) for milk, and 8.0 (95% CI 5.5-12.0) for legumes.
Among Mothers of Patients With Amino Acid Metabolism Disorders, Who Reported That Their Families Consumed Less Protein (n = 23), the Amounts of Protein-Rich Foods That They Believed Should Be Consumed in a Month Versus the Amounts Actually Consumed in Real Life.
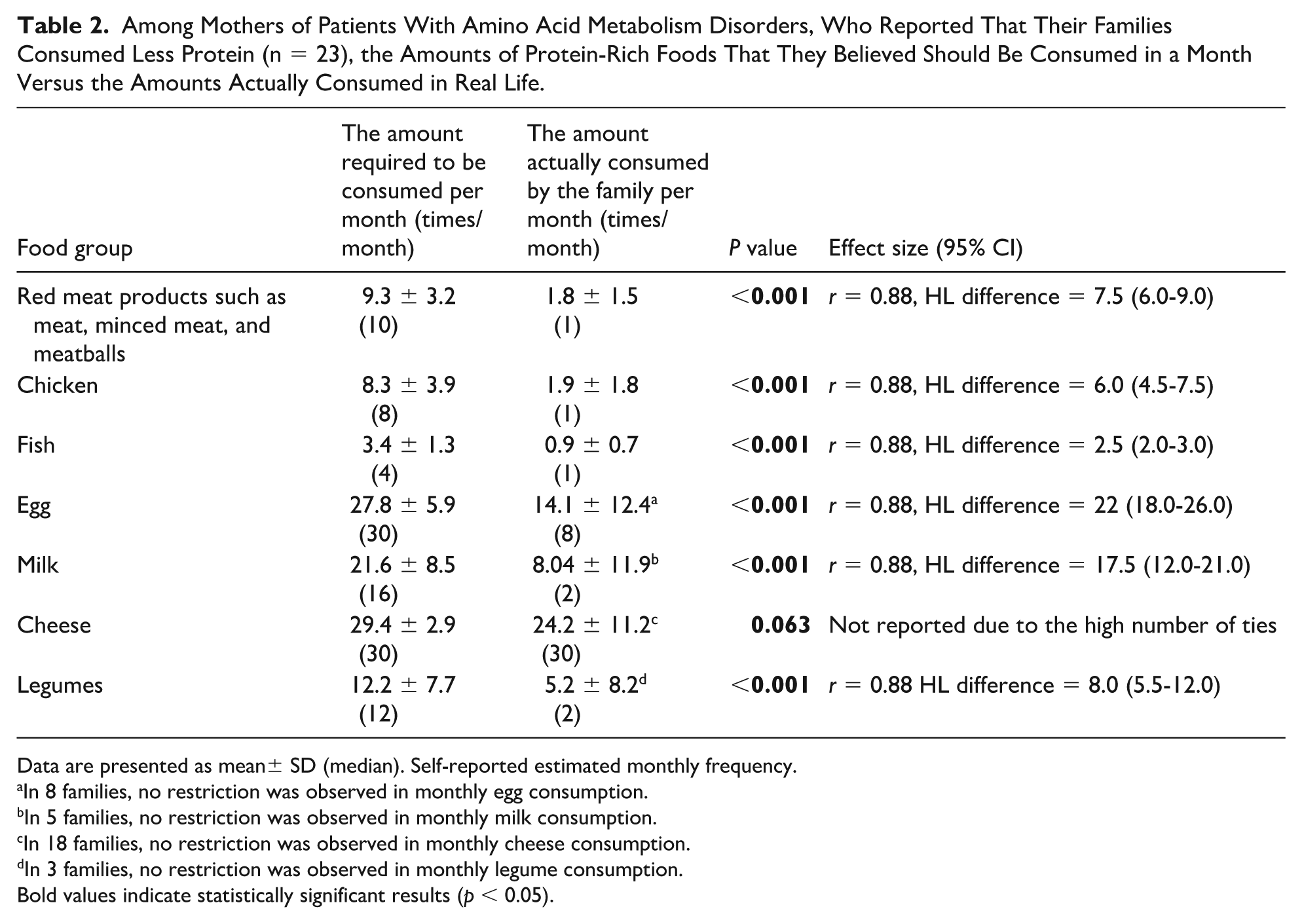
Data are presented as mean± SD (median). Self-reported estimated monthly frequency.
In 8 families, no restriction was observed in monthly egg consumption.
In 5 families, no restriction was observed in monthly milk consumption.
In 18 families, no restriction was observed in monthly cheese consumption.
In 3 families, no restriction was observed in monthly legume consumption.
Bold values indicate statistically significant results (p < 0.05).
Among the mothers in the patient group, 27 (54.0%) reported that, in accordance with their child’s disease, they preferred foods low in protein or free of galactose in their own diet. Of these 27 mothers following a special diet, 17 had children with phenylketonuria, 8 had children with organic acidemia or urea cycle defects, and 2 had children with galactosemia. Meat products such as red meat and minced meat were avoided by 19 mothers; chicken and fish by 12 mothers; legumes and nuts by 8 mothers; eggs by 3 mothers; and milk and dairy products by 5 mothers. Of these mothers, 3 (6.0%) had adopted a vegetarian diet, and 2 (4.0%) had adopted a vegan diet. None of the mothers in the control group reported restricting any foods in their diet. Restricting foods in their diet caused difficulties in daily life for 10 mothers (20.0%).
The mean time to prepare dietary meals for the sick child was 2.1 ± 0.9 hours (minimum 1 hour-maximum 5 hours) per day. Nine mothers (18.0%) reported that preparing special dietary meals for their sick child was difficult or very difficult for them; 13 mothers (26.0%) stated that preparing dietary meals for their sick child forced them to reduce the time spent preparing meals for other family members. Mothers in the patient group spent 1.99 ± 0.9 hours preparing meals for the rest of the family, whereas mothers of healthy controls spent 2.47 ± 0.9 hours (P = 0.014).
Impact on Social Life
Twenty-nine mothers (58.0%) in the patient group reported limiting their out-of-home activities because it was difficult to find suitable foods for their child outside the home. When participating in activities outside the home, 35 mothers (70.0%) reported preparing their child’s meal at home in advance, which the child then ate on site, while the remaining 15 mothers (30.0%) indicated that they chose the most appropriate foods available at the location to ensure their child was adequately fed. Seventeen (34.0%) mothers reported avoiding hosting guests at home because it could affect their child’s diet.
Findings Related to the Mother’s Individual Health
Ten mothers (20.0%) in the patient group and three mothers (9.4%) in the control group had chronic disorders that did not affect their daily lives (P = .233). These disorders included asthma, hypertension, goiter, diabetes, Behçet’s disease, chronic hepatitis, treated bladder cancer (control group), mitral valve prolapse (control group), polycystic kidney disease, rheumatoid arthritis, sarcoidosis (control group), and ulcerative colitis. Four mothers were receiving psychiatric support due to their child’s disease, and one of these mothers was using antidepressant medication.
Findings From the Perceived Stress Scale and the SF-36 Quality-of-Life Scale
The PSS scores of the mothers in the patient group were significantly higher than those of mothers in the control group (patient group: 29.6 ± 11.9 vs control group: 9.5 ± 4.8, P < .001) (Table 3). Similarly, the SF-36 subscale scores of mothers in the patient group were significantly lower than those of mothers in the control group (Table 3); P values were additionally evaluated using the Holm-Bonferroni procedure for 11 comparisons. All results remained statistically significant after correction (P < .05). When comparing the PSS, SF-36, PCS, MCS, and subscale scores among mothers of the 4 different patient subgroups, no significant differences were observed between the groups.
Comparison of Perceived Stress Scale Scores, PCS and MCS Scores, and Their Subcomponents Between Patient and Control Groups.
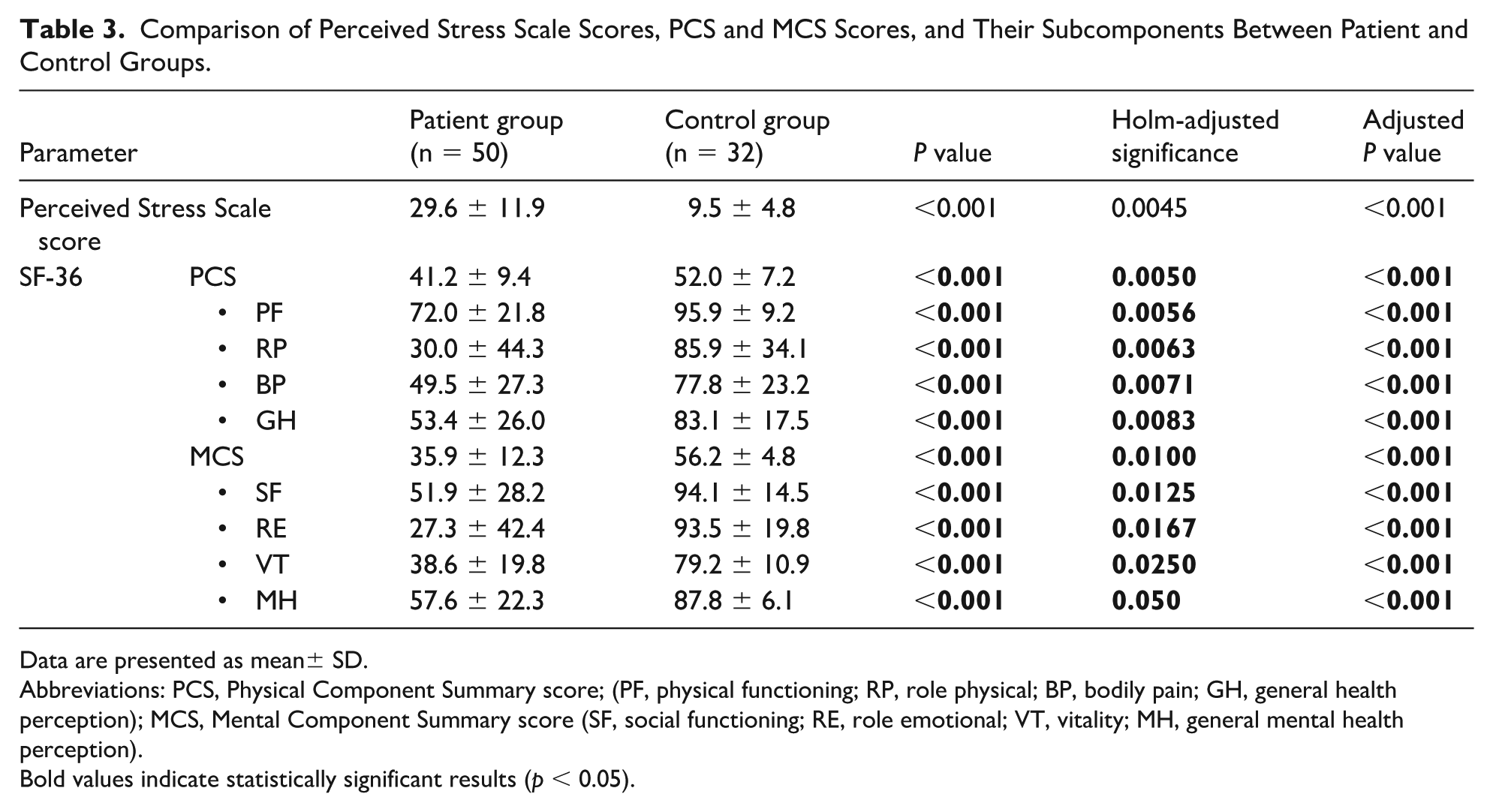
Data are presented as mean± SD.
Abbreviations: PCS, Physical Component Summary score; (PF, physical functioning; RP, role physical; BP, bodily pain; GH, general health perception); MCS, Mental Component Summary score (SF, social functioning; RE, role emotional; VT, vitality; MH, general mental health perception).
Bold values indicate statistically significant results (p < 0.05).
The group of mothers in the patient group (n = 50) was divided into subgroups according to parameters that potentially affect stress and quality of life, and their scores on the PSS, SF-36, PCS, MCS, and their subscales were compared. No significant differences were found among mothers with respect to the PSS, SF-36, and its subscales in relation to the mother’s educational background, the presence of a chronic disease in the mother (present vs absent), the mother’s dietary habits (vegan/vegetarian vs omnivorous), the number of children in the family (<2 vs >3 children), or the presence of more than one sick child in the family (present vs absent) (data not shown). The general health (GH) perception score of mothers engaged in income-generating work (n = 11) was significantly higher than that of non-working mothers (GH: 70.1 ± 13.9 vs 48.1 ± 26.9, P = .023).
To examine whether the observed differences between the patient and control groups could be explained by sociodemographic differences, multivariable linear regression analyses were performed for PSS, PCS, and MCS scores. Maternal employment status, maternal education, number of children in the family, and household size were included as covariates in each model. After adjustment, group status remained significantly associated with all three outcomes. Mothers in the patient group continued to have higher PSS scores and lower PCS and MCS scores than mothers in the control group. In addition, the number of children was independently associated with PSS and MCS scores, and household size was independently associated with MCS scores. These findings indicate that the between-group differences in perceived stress and quality-of-life summary scores were not attributable only to baseline sociodemographic differences (Table 4).
Adjusted Linear Regression Analyses for PSS, PCS, and MCS.
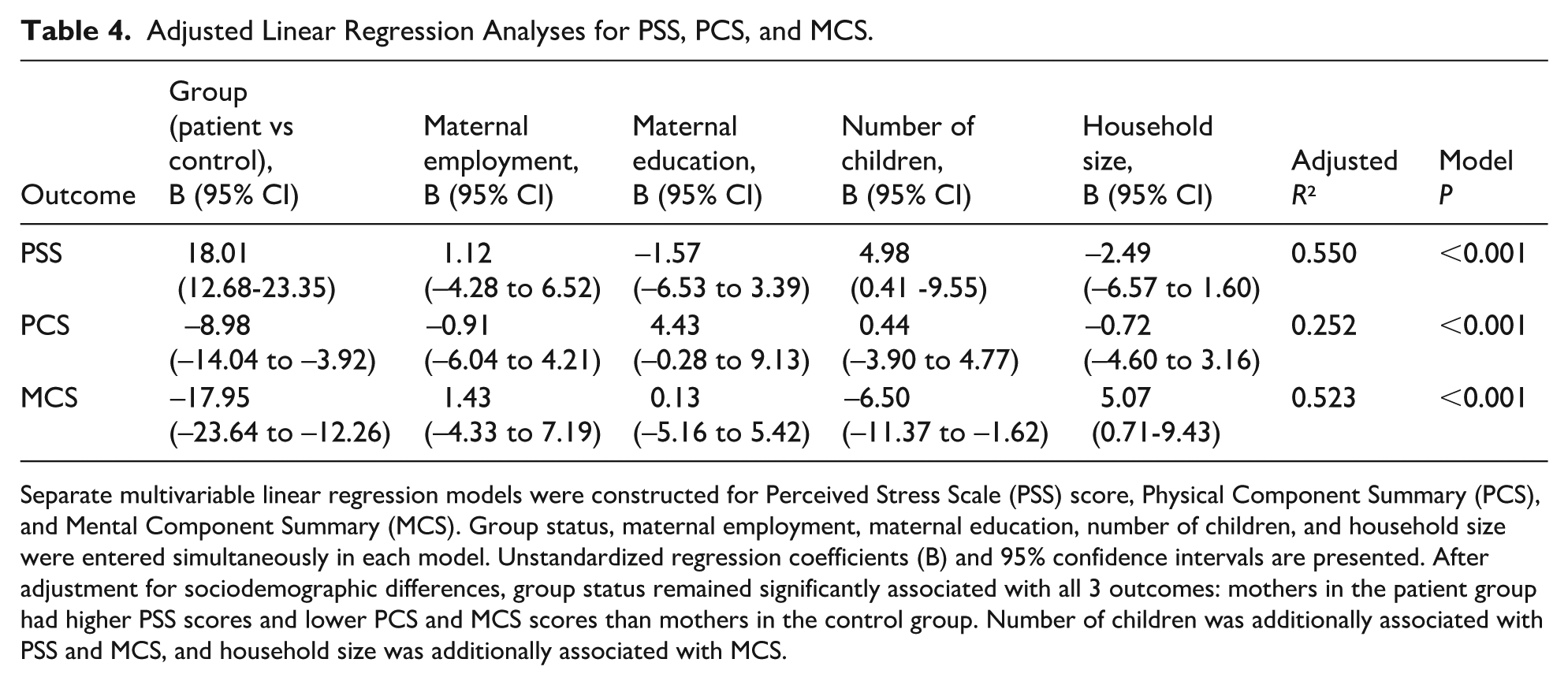
Separate multivariable linear regression models were constructed for Perceived Stress Scale (PSS) score, Physical Component Summary (PCS), and Mental Component Summary (MCS). Group status, maternal employment, maternal education, number of children, and household size were entered simultaneously in each model. Unstandardized regression coefficients (B) and 95% confidence intervals are presented. After adjustment for sociodemographic differences, group status remained significantly associated with all 3 outcomes: mothers in the patient group had higher PSS scores and lower PCS and MCS scores than mothers in the control group. Number of children was additionally associated with PSS and MCS, and household size was additionally associated with MCS.
Subgroup analyses were conducted on an exploratory basis to examine potential associations between maternal experiences and perceived burden. Mothers receiving psychiatric support due to their child’s disease (n = 4) and mothers who excluded certain foods from their diet despite liking them (n = 28) showed higher PSS scores and lower MCS scores than other mothers (Table 5). In addition, mothers who reported feeling distressed because of their child’s restricted diet (n = 39) had higher PSS scores than those who did not (P = .045) (Table 5). Given the small sample sizes in some subgroups, these findings should be interpreted with limited generalizability.
Exploratory Analysis of the Effects of Selected Nutritional and Maternal Health Variables on Perceived Stress Scale (PSS), PCS, and MCS Scores in Mothers in the Patient Group (n = 50).
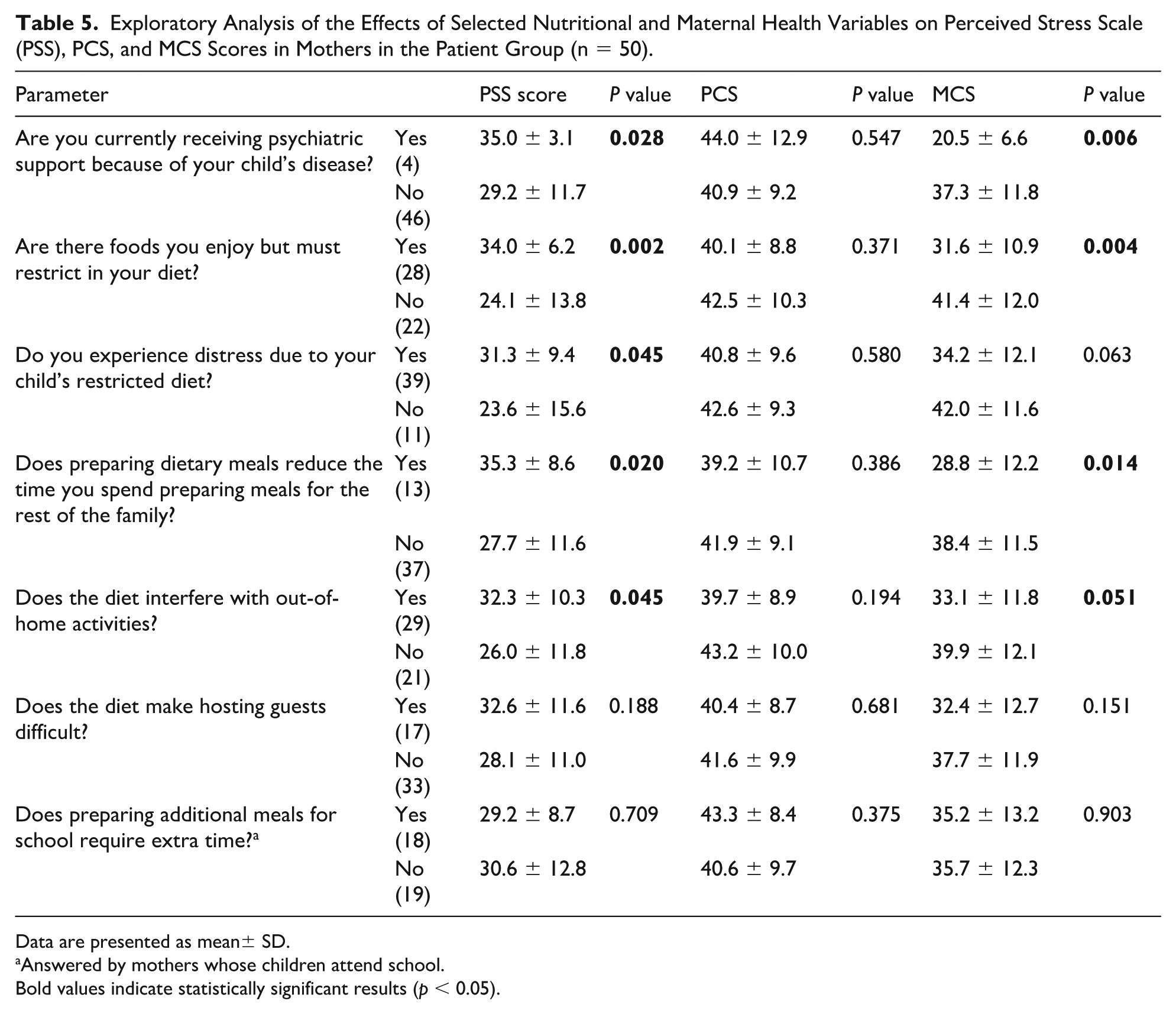
Data are presented as mean± SD.
Answered by mothers whose children attend school.
Bold values indicate statistically significant results (p < 0.05).
Similarly, in the subgroup of 46 patients with amino acid metabolism disorders, mothers who reported that the rest of the family consumed fewer protein-containing foods than necessary due to the child’s restricted diet (n = 23) had significantly higher PSS scores than those who did not report this (n = 23) (PSS score: 33.9 ± 6.6 vs 26.0 ± 13.2, P = .018). In addition, the first group had significantly lower MCS, bodily pain (BP), social functioning (SF), and role emotional (RE) scores than those of the second group (MCS: 32.1 ± 9.9 vs 39.2 ± 13.4, P = .047, BP: 37.3 ± 22.4 vs 59.9 ± 27.2, P = .004, SF: 42.3 ± 19.5 vs 60.1 ± 32.0, P = .027, RE: 34.3 ± 20.5 vs 42.2 ± 18.9, P = .018).
Mothers who reported that preparing dietary meals for their sick child affected the time spent preparing meals for the rest of the family (n = 13) and that preparing special diets for their child limited their out-of-home activities (n = 29) had significantly higher PSS scores and lower MCS scores than those who reported no such effects (Table 5). A positive correlation was found between the mother’s time spent preparing dietary meals and the PSS score (rho = 0.391, P = .005), while negative correlations were observed with the MCS score (rho = –0.289, P = .042), the MCS subscales, namely RE (rho = –0.286, P = .046), vitality (rho = –0.352, P = .012), and SF (rho = –0.261, P = .068), as well as the PCS subscale, namely the GH score (rho = –0.316, P = .026). No significant correlation was observed between the mother’s time spent preparing dietary meals and the PCS score (rho = –0.257, P = .072).
Mothers who reported that their child’s restricted diet imposed an additional financial burden on the family (n = 39) had significantly lower PCS scores and lower scores in 3 PCS subscales—role physical (RP), BP, and GH—than those who reported no additional burden (PCS score: 39.4 ± 9.7 vs 47.3 ± 5.2, P = .013; RP: 24.3 ± 41.5 vs 50.0 ± 50.0, P = .049; BP: 45.5 ± 27.2 vs 63.9 ± 23.5, P = .047; GH: 48.6 ± 27.0 vs 70.3 ± 11.7, P = .021). While the first group demonstrated higher PSS scores and lower MCS scores than the second group, the differences did not reach statistical significance (PSS: 30.3 ± 10.3 vs 27.1 ± 14.8, P = .665; MCS: 35.7 ± 12.0 vs 36.8 ± 13.8, P = .770).
Discussion
In this study, we investigated the nutritional status of mothers caring for children with hereditary metabolic diseases requiring a restricted diet and examined whether the child’s diet was associated with mothers’ own nutrition and lifestyle, as well as their stress levels and quality of life. The results suggest that childcare responsibilities and dietary arrangements are linked to withdrawal from the workforce, limitations in social activities, and modifications in both maternal and family dietary patterns. These factors may be associated with higher stress levels and lower quality-of-life scores among mothers.
Having a child with a hereditary metabolic disease requiring dietary restriction complicates the life of the caregiving mother in many areas and affects her quality of life.10,12,14 In a study conducted in the United States involving families of 118 patients diagnosed with urea cycle disorders, 66% of parents reported that their careers were affected, 26% reported that they were unemployed, over 40% indicated that they had limited social interactions and spent less time with their other children, and 66% reported having no personal time. 5 Other studies have found that a significant proportion of mothers of phenylketonuria patients on a restricted diet experience social limitations,12,22-24 and that maternal unemployment is associated with higher anxiety scores. 23 Furthermore, a review of numerous studies demonstrated that maternal unemployment, educational background, and financial difficulties within the family adversely affect the quality of life of mothers of children with phenylketonuria. 25 To further examine whether these between-group differences could be explained by baseline sociodemographic differences, we performed adjusted regression analyses (Table 4). After controlling for maternal employment, maternal education, number of children, and household size, group status remained significantly associated with higher perceived stress and lower physical and mental quality-of-life summary scores (Table 4). In addition, approximately one-fifth of the mothers were not engaged in the workforce owing to their child’s disease, while 58% reported restricting their social activities outside the home. In addition, the GH scores of unemployed mothers were lower than those of employed mothers, and the PCS scores of mothers who stated that their child’s nutritional products imposed an additional financial burden on the family were lower than those of mothers who did not report such a burden. In studies conducted with families of patients with hereditary metabolic diseases, special dietary products have been reported to impose an additional financial burden on families,11,12,23,26 and financial difficulties among these families have been shown to place physical, social, and emotional burdens on mothers.7,12,14,27 All these findings reveal that the professional and social lives of mothers of children on dietary treatment are significantly affected.
In our study, it was found that mothers restricted the time spent preparing meals for the rest of the family since they had to prepare separate meals for their affected children. In a study involving patients with phenylketonuria, some mothers reported that their daily meal preparation time had doubled, and the depression scores of mothers of children on a restricted diet were found to be higher than those of the control group. However, in that study, the impact of meal preparation time on mothers’ quality of life and stress levels was not evaluated. 23 In our study, mothers who reported that preparing dietary meals for their sick child affected the time spent preparing meals for the rest of the family and that preparing special diets for their child limited their out-of-home activities had significantly higher PSS scores and lower MCS scores than those who reported no such effects. In addition, a positive correlation was found between the time mothers spent preparing dietary meals for their affected child and their PSS scores, whereas negative correlations were observed with the MCS and its subscale scores. Studies have shown that preparing the diet of children with phenylketonuria takes an average of 1 hour and 24 minutes and is both exhausting and costly for mothers, 26 and additional time requirements have been associated with withdrawal from employment and social activities, along with adverse impacts on maternal mood, mental health, and quality of life.24,28
In our study, 54% of mothers in the patient group reported that, in line with their child’s condition, they preferred to consume foods that were either low in protein or galactose-free. Due to their child’s dietary requirements, three of these mothers had adopted a vegetarian diet, while 2 had switched to a vegan diet. Similarly, 56% of the mothers reported avoiding protein-rich foods they actually enjoyed, as these were incompatible with their child’s dietary regimen. Mothers who restricted their own diets had higher PSS scores and lower MCS scores than those who did not. Moreover, mothers who reported that other family members consumed less protein than required because of the child’s restricted diet (n = 23, 50%) had higher PSS scores and lower MCS scores than those who did not report such an effect (n = 23). A study conducted with families of children with phenylketonuria demonstrated that 58% of families consumed low-protein foods compatible with the child’s diet during shared meals. 23 Our study also revealed that the diets of both the mothers and the entire family were significantly influenced by the affected child’s diet and that this had an impact on the mothers’ psychological well-being. All these findings underscore the importance of monitoring the nutritional adequacy of mothers of children on restricted diets, as well as assessing their potential need for additional micronutrient supplementation, under the supervision of a professional team.
In the patient group, 78% of mothers reported feeling distressed due to their children following a diet restricted in natural foods, and these mothers had significantly higher PSS scores. Studies have also shown that mothers experience distress due to potential nutritional deficiencies resulting from their children’s restricted diet and that these families require professional support regarding the content of the prescribed diet, its preparation, the purchase of medical foods, insurance coverage, and the overall management of treatment.10,12,29
This descriptive, correlational, and cross-sectional study has several limitations. The first limitation is that the majority of the patient group consisted of patients with phenylketonuria, while the other patient subgroups were small in number. As the largest subgroup of patients receiving dietary treatment in our unit consisted of those with phenylketonuria, the study was designed accordingly. Conducting larger studies, either focusing on each patient group separately or including all patient groups collectively, would allow for the collection of more precise data. The second limitation is the difference in employment status between the mothers in the patient and control groups, which directly influenced the monthly household income. In larger studies with higher participation, including such parameters as exclusion criteria would enable a more homogeneous comparison between the groups. The third limitation is that, while mothers’ chronic diseases were asked, only those whose conditions did not interfere with daily living activities were included in the study. This may still have influenced the findings of this study. In future studies, specifically questioning symptoms such as pain and excluding mothers with chronic diseases that cause such symptoms would allow a clearer interpretation of the findings. In addition, some subgroup analyses were exploratory and based on small sample sizes, particularly in categories such as mothers receiving psychiatric support. Therefore, these findings should be interpreted cautiously and require confirmation in larger studies. The final limitation is that anthropometric data, macronutrient and micronutrient intakes, and body micronutrient levels of mothers who had modified their dietary preferences were not assessed. Although affected children are restricted from natural foods, the amino acid substitutions provided to them are enriched with vitamins, minerals, and trace elements, thereby preventing nutritional deficiencies. However, because no such supplementation is provided for mothers who restrict their own diets, these mothers are at a higher risk of developing micronutrient deficiencies.
In conclusion, mothers of children with inherited metabolic disorders requiring lifelong dietary restrictions may modify their own and family eating habits in response to their child’s nutritional needs. The demands of dietary management may be associated with limitations in social and professional activities and with higher perceived stress and lower quality of life among mothers. However, given the cross-sectional design, these findings should be interpreted as associations rather than causal relationships. These findings highlight the importance of a holistic, biopsychosocial approach that considers caregiver well-being in the management of inherited metabolic disorders. Routine screening of caregiver stress and quality of life, along with the provision of psychosocial support, nutritional counseling for mothers, and referral to mental health services when needed, should be considered in clinical practice. Future longitudinal studies with larger samples and multivariable analyses are needed to further clarify these relationships.
Author Contributions
All authors have made substantial contributions to the conception, design, acquisition, analysis, or interpretation of data, drafted or revised the article critically, approved the final version, and agree to be accountable for all aspects of the work.
Footnotes
Acknowledgements
The authors would like to thank all the mothers who participated in the study.
Ethical Approval
Ethical approval for the study was obtained from the Non-Interventional Research Ethics Committee of Dokuz Eylül University Faculty of Medicine on October 26, 2022 (protocol number 7560-GOA; decision number 2022/34-29).
Consent to Participate
Written informed consent was obtained from all participating mothers.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data supporting the findings of this study are available from the corresponding author upon reasonable request.