
Abstract
With rising autism prevalence coupled with a shortage of trained specialists, pediatricians are caring for more patients with autism. However, pediatric residents experience gaps in autism knowledge and comfort in caring for these children. This study aimed to evaluate changes in autism knowledge and perceived confidence among residents after completion of a developmental-behavioral pediatrics (DBP) rotation, which included an asynchronous module on autism diagnosis. Participants were 79 categorical and combined pediatrics residents. Prior to and following completion of the autism module and clinical experiences in their DBP rotation, residents completed an objective measure of knowledge about autism in young children and rated confidence in autism diagnosis on a Likert scale. Residents demonstrated a significant increase in total autism knowledge from pre-rotation to post-rotation (P = .007). Perceived confidence of autism diagnosis also increased (P < .001). Findings demonstrate the potential for enhancing resident autism knowledge through asynchronous education combined with clinical experience.
Introduction
Autism prevalence is increasing with an estimated 1 in 31 children receiving a diagnosis in the United States. 1 Despite this increase in prevalence, the number of subspecialists with expertise in caring for patients with autism is limited. 2 The American Academy of Pediatrics projects that the ratio of developmental-behavioral pediatricians to US children will decrease from 1 to 100 000 in 2023 to 0.5-0.6 to 100,000 in 2040. 3 Workforce shortages coupled with increased patient volumes 4 contribute to significant wait times for developmental evaluations across the country. 5 In a survey of over 100 centers across the United States, over 60% of centers have wait times of 4 to 6 months or longer for autism diagnostic evaluations. 4 Delays in diagnosis may postpone early intervention, which can improve developmental outcomes and decrease challenging behavior. 6 To decrease wait times and increase access to diagnostic assessments, many institutions have implemented initiatives to train primary care providers in autism diagnosis, 7 although these programs note barriers in clinician implementation 8 and in health care systems and policies. 9
General pediatricians are on the front lines of caring for more autistic patients than ever before. Professional organizations, like the American Academy of Pediatrics and the Canadian Pediatric Society, have created guidelines for primary care providers to support autism care after diagnosis.10,11 Furthermore, families report the need for comprehensive, coordinated, and family-centered autism care from their primary care pediatricians. 12 Practicing pediatricians note discomfort when caring for the autism population, including limited perceived knowledge about the diagnosis and treatment of autism. 13 Primary care pediatricians have noted barriers in best caring for children with autism, including lack of confidence, time, knowledge of resources, access to specialists, confidence in managing medical and behavioral concerns, prior training in autism, and lack of knowledge about autism symptoms. 14 Overall, pediatricians need better training in autism diagnosis and management. 15 Programs to train primary care providers about autism have been effective in improving knowledge and confidence.7,16-18
With over 3000 pediatricians across the country completing their residency training each year, 19 intervening at the trainee level is an opportunity to impact care that patients will continue to receive for years. The Accreditation Council for Graduate Medical Education (ACGME) requires that pediatrics residency programs have a faculty member in developmental-behavioral pediatrics (DBP) and that residents complete 1 educational unit in DBP. 20 Pediatric residents also receive training regarding autism screening in primary care clinics. 11 Despite this dedicated autism training, pediatrics residents experience significant gaps in their autism knowledge 21 and comfort in caring for children with autism. 22 Some educational interventions have specifically targeted improving autism knowledge in residents.23-26 For example, resident autism knowledge and perceived confidence increased following participation in 1 time-limited session from a curriculum developed by the CDC (Centers for Disease Control and Prevention) and MCHB (Maternal and Child Health Bureau). 24 Furthermore, resident autism knowledge was found to improve following training on a structured autism assessment tool (ie, Screening Tool for Autism in Toddlers and Young Children). 25 A case-based curriculum was also noted to improve residents’ knowledge and confidence in various behavioral and mental health conditions, including autism. 26 Hine et al. 23 embedded a structured autism curriculum in the context of a standard DBP rotation during residency, which demonstrated significant increases in resident confidence following participation in their curriculum but did not measure change in objective autism knowledge. Furthermore, studies have demonstrated that combining e-learning with traditional learning methods has been shown to be more effective than only using traditional in-person learning methods in health education.27,28
While several studies22-26 have documented interventions to improve pediatric resident’s general autism knowledge and confidence in autism diagnosis, no studies to date have examined what aspects of autism knowledge improve with training. As such, the objective of the current study is to (1) examine changes in residents’ objective autism knowledge and perceived confidence in autism diagnosis of young children following participation in an asynchronous autism training module implemented as a standard part of the required DBP rotation and (2) characterize the specific domains of knowledge change following the DBP rotation. With improved knowledge and perceived confidence in autism evaluation and care of young children, the next generation of pediatricians will be better equipped to care for children and families affected by autism in their practice.
Methods
Study Design
This prospective observational study with pre/post-test design was determined to be exempt by the Institutional Review Board (IRB). An asynchronous autism training module was developed to ensure that all pediatrics and combined pediatric residents would have a similar baseline level of knowledge regarding autism prior to participating in autism clinics on their DBP rotation. Between July 2022 and November 2024, all categorical pediatrics and combined pediatric residents rotating through the DBP rotation were eligible to participate. At our midwestern institution, combined pediatrics programs include medicine-pediatrics, triple board (psychiatry, child psychiatry, and pediatrics), child neurology, neurodevelopmental disabilities, and emergency medicine-pediatrics. All residents scheduled for the rotation were expected to complete the curriculum. The autism module was designed to fit into the existing scheduling and training structure.
Study Procedure
Residents completed a demographic survey and knowledge questionnaire prior to starting the rotation and autism module. Residents were instructed to complete the autism training module at the start of the rotation prior to any clinical encounters. Residents then participated in various clinics as part of their 4-week DBP block. Participants then repeated the knowledge questionnaire after completing the rotation and module.
Developmental-Behavioral Pediatrics Rotation
As part of the ACGME program requirements for pediatrics 20 residents participate in a 4-week ambulatory rotation designed to train residents in the basics of DBP that would benefit all pediatricians. At this institution, the DBP rotation includes a range of experiences, including specialty outpatient clinics, didactic training, and community-based experiences. Specialty outpatient clinics focus on a variety of neurodevelopmental and related disabilities, including autism, spina bifida, cerebral palsy, and Down syndrome. Regarding didactic training, lectures are designed to supplement clinical experiences. Some are live, while others are asynchronous. Topics include autism, developmental delays, basic behavior management training, and medication management of attention-deficit/hyperactivity disorder (ADHD). Community-based experiences include observations of applied behavior analysis (ABA), developmental preschool, and home-based early intervention. Details regarding autism-focused experiences are provided below.
Autism Training Module
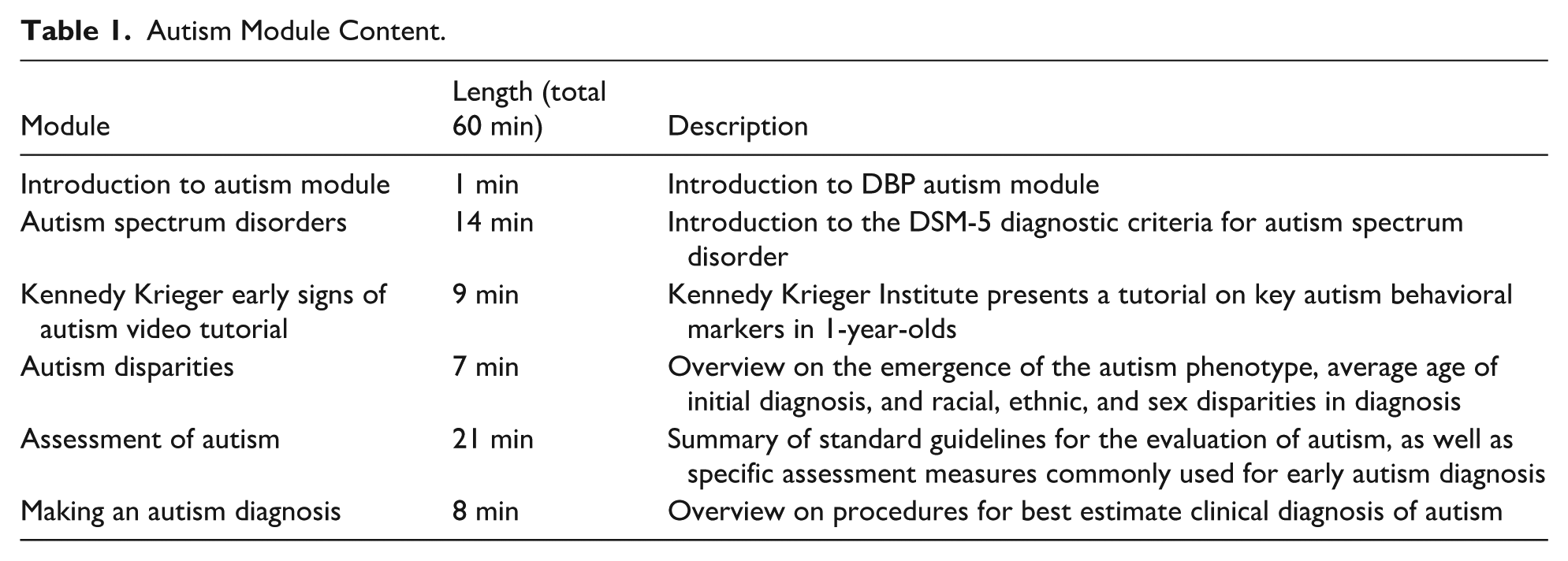
The autism module includes 6 videos, lasting 60 minutes total (Table 1). Autism module content was adapted from the primary care training program developed by the Early Autism Evaluation Hub system (for primary care physicians and clinicians) 18 with the goal of targeting basic autism diagnosis knowledge needed by all pediatricians. Topics addressed in the module include basic knowledge regarding autism, key behavioral symptoms in very young children (Kennedy Krieger Early Signs of Autism video tutorial), 29 disparities in autism diagnosis, evidence-based autism assessment methods (including review of the Autism Diagnostic Observation Schedule, Second Edition [ADOS-2], 30 the Screening Tool for Autism in Toddlers and Young Children [STAT], 31 and the TELE-ASD-PEDS [TAP] 32 ), and integration of clinical data to make an autism diagnosis.
Autism Module Content.
Developmental-Behavioral Pediatrics Rotation – Autism-Focused Training
Following completion of the module, residents were scheduled for several autism-focused clinics serving children of all ages led by physicians or psychologists, including diagnostic interviews, comprehensive psychology-led autism evaluations, streamlined physician-led autism evaluations, and tele-assessment evaluations. Visits with physicians include new patient consultations and comprehensive autism evaluations including autism testing with the STAT. With psychologists, residents observe traditional in-person developmental assessments, including the ADOS-2; they also participated in virtual appointments utilizing the TAP, a telehealth autism assessment tool for young children. Residents were also scheduled in diagnostic interviews, which are comprehensive family interviews that focus on diagnostic criteria for developmental and behavioral conditions including autism. During clinics, information covered in the module was supplemented and reinforced through exposure to assessment administration and scoring, discussion of differential diagnosis, and diagnostic counseling and review of recommendations. Aside from autism-focused clinics, residents were also scheduled for experiences external to the institution. A local ABA center allows residents to observe for 2 hours, during which they are exposed to 1 to 2 therapists working with children enrolled at the center. Residents also participate in a tour of a local developmental preschool and observe a home-based early intervention appointment.
Measures
To assess change in confidence and objective autism knowledge, residents were directed to complete a survey at 2 time points: (1) prior to beginning their DBP rotation and (2) at the end of their DBP rotation.
Demographics and Confidence
Residents provided demographic information, including race, ethnicity, sex, training status, program type, and receipt of prior autism training. Residents were asked to rate their confidence by answering “I feel confident that I am able to make accurate ASD diagnoses in young children” on a 5-point Likert scale (with options: strongly agree, agree, undecided, disagree, strongly disagree).
Autism Knowledge Questionnaire
The Autism Knowledge Questionnaire (AKQ) is a 45-item multiple-choice questionnaire designed to measure knowledge about the diagnosis, evaluation, and management of young autistic children 33 (see Table, Supplemental Digital Content 1). Items were developed collaboratively by a team of clinicians and researchers with expertise in autism evaluation from Vanderbilt University Medical Center and Indiana University School of Medicine. Items were refined following feedback from an independent group of experts across the United States until consensus was obtained on all items. The AKQ produces a total knowledge score ranging from 0 to 45, in addition to 7 subdomain scores (general autism knowledge: range 0-5; autism screening: range 0-4; diagnostic consultation: range 0-6; diagnostic formulation: range 0-6; communicating feedback: range 0-4; clinical recommendations: range 0-10; and cultural competency range: 0-10).
Analysis Plan
Study data was collected using REDCap34,35 (Research Electronic Data Capture), a secure, web-based software platform hosted at Indiana University designed to support data capture for research studies, providing (1) an intuitive interface for validated data capture; (2) audit trails for tracking data manipulation and export procedures; (3) automated export procedures for seamless data downloads to common statistical packages; and (4) procedures for data integration and interoperability with external sources. Data were analyzed using SPSS (Version 29; IBM SPSS Statistics, Armonk, New York: IBM Corp). Descriptive statistics were calculated for clinician demographics and measures of knowledge and confidence. Change in perceived confidence in autism diagnosis was analyzed using non-parametric Wilcoxon signed-rank tests.
Results
Participants
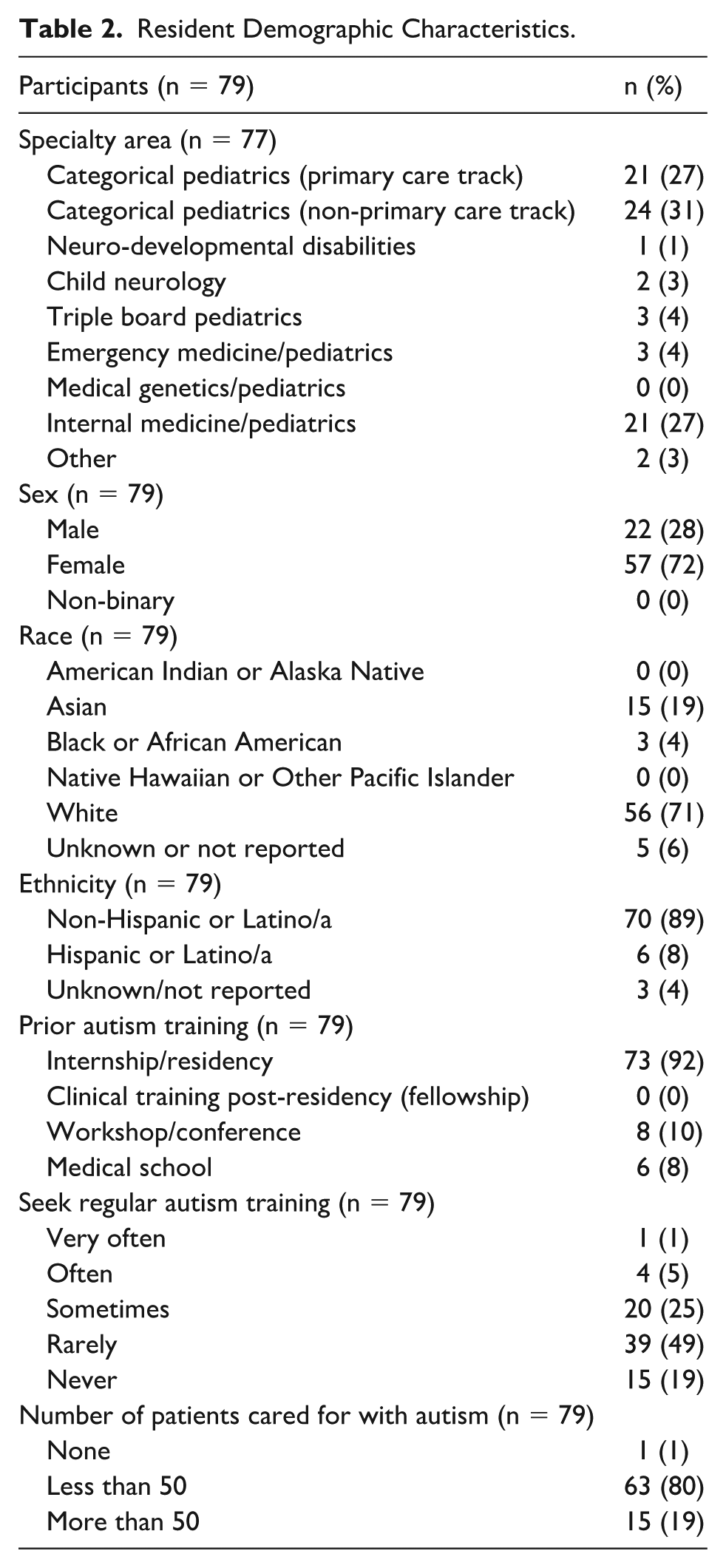
Participants were 79 pediatric residents from categorical and combined pediatrics residency programs (eg, internal medicine and pediatrics, pediatric emergency medicine, and child neurology). Participants were predominately female (n = 57; 72%), non-Hispanic (n = 70; 89%), white (n = 56; 71%), and from the categorical pediatrics program (n = 45; 58%). Table 2 shows all participant demographics.
Resident Demographic Characteristics.
Autism Knowledge
Residents demonstrated a significant increase in AKQ total autism knowledge from pre-rotation (M = 33.2, SD = 5.49) to post-rotation (M = 36.15, SD = 4.15; t(78) = −5.50, P = .007, Cohen’s d = .62; Table 3). Residents demonstrated an improvement in their total knowledge of the diagnosis, evaluation, and management of young autistic children.
Pre- and Post-Rotation Mean Scores (Items Correct) in Total Knowledge and Subdomains.
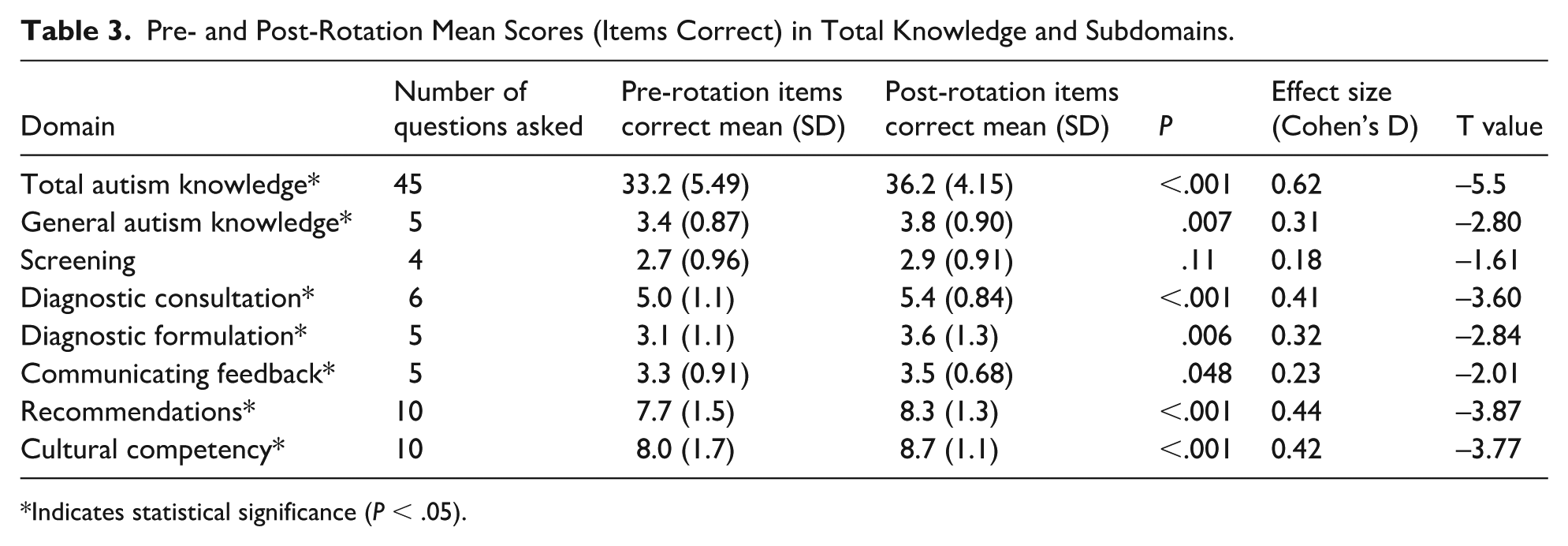
Indicates statistical significance (P < .05).
With regard to specific knowledge domains, residents demonstrated a statistically significant increase in AKQ General Autism Knowledge (pre-rotation M = 3.4, SD = 0.87; post-rotation M = 3.8, SD = 0.9; t(78) = −2.80, P = .007, Cohen’s d = 0.31; Table 3). Residents were highly accurate on 2 items at both pre- and post-rotation; specifically, nearly 98% (n = 77) knew risk factors for autism prior to the rotation, and 96% (n = 76) knew how to respond appropriately to a family question regarding familial risk for autism (Supplemental Digital Content 2). Residents demonstrated an increase in accuracy on 3 items, demonstrating improvements in understanding of prognosis and initial age of reliable diagnosis (items 1, 3, and 4).
Residents also demonstrated a statistically significant increase in AKQ Diagnostic Consultation (pre-rotation M = 5.0, SD = 1.1; post-rotation M = 5.4, SD = 0.84; t(78) = −3.60, P < .001, Cohen’s d = 0.41; Table 3). Residents demonstrated a high level of knowledge (above 90% correct) at pre-rotation regarding when to refer and what to look for during observations (items 14 and 15, Supplemental Digital Content 2). Nearly 20% of residents demonstrated a change from incorrect to correct responses with regard to understanding of observational tools in clinical settings (item 13) and appropriateness of general pediatrician diagnosis (item 11).
Residents also demonstrated a statistically significant increase in AKQ Diagnostic Formulation knowledge (pre-rotation M = 3.1, SD = 1.1; post-rotation M = 3.6, SD = 1.3; t(78) = −2.84, P = .006, Cohen’s d = 0.32; Table 3). Residents were accurate at baseline regarding effective communication with concerned parents (item 20, Supplemental Digital Content 2). On the contrary, residents did not improve performance on a question regarding which behavior was most specifically associated with autism over global developmental delay (item 16). In total, 28% of residents learned the specifics of the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5) criteria and >20% of residents improved in diagnostic differentiation and next-step recommendations (items 17 and 18).
Residents also demonstrated a statistically significant increase in AKQ Communicating Feedback (pre-rotation M = 3.3, SD = 0.91; post-rotation M = 3.5, SD = 0.68; t(78) = −2.01, P = .048, Cohen’s d = 0.23; Table 3). Residents did well at baseline regarding common questions asked by caregivers, with 96% (n = 76) answering correctly prior to the rotation (item 24). In total, 34% of residents (n = 27) demonstrated increased knowledge about communicating DSM-5 severity levels (eg, item 21).
There was also a statistically significant improvement with regard to understanding of AKQ recommendations (pre-rotation M = 7.7, SD = 1.5; post-rotation M = 8.3, SD = 1.3; t(78) = −3.87, P < .001, Cohen’s d = 0.44; Table 3). In total, 100% of residents were correct at baseline about common comorbidities with autism (item 31, Supplemental Digital Content 2). In total, 25% (n = 20) of residents improved in knowledge of the role of genetics and autism (item 32). Nearly 23% (n = 18) improved on describing the difference between public school eligibility and medical diagnosis (item 34).
Lastly, residents displayed a statistically significant improvement in AKQ Cultural Competency (pre-rotation M = 8.0, SD = 1.7; post-rotation M = 8.7, SD = 1.1; t(78) = −3.77, P < .001, Cohen’s d = 0.42; Table 3). Nearly 23% (n = 18) of residents improved in describing possible reasons for autism sex differences, and around 20% (n = 15) improved in their understanding of racial biases in identification (item 43, Supplemental Digital Content 2).
The only domain that did not yield a statistically significant change was screening (pre-rotation M = 2.7, SD = 0.96; post-rotation M = 2.9, SD = 0.91; t(78) = −1.61, P = .11, Cohen’s d = 0.18; Table 3).
Perceived Confidence in Autism Diagnosis
There was a significant increase in perceived confidence of autism diagnosis (Z = 5.854, P < .001), with an overall shift from pre-rotation median of 2 (Disagree) to post-rotation median of 3 (Undecided; Table 4). Prior to the rotation and module, 38 of 79 (48%) residents responded 2 (Disagree); after the rotation, 34 of 79 residents (43%) responded 3 (Undecided). Most residents (n = 47) reported an increase in perceived confidence in autism diagnosis, and some reported an unchanged level of confidence (n = 28) (Figure 1). Only 4 residents reported decreased confidence, who all changed responses from “agree” to “undecided” (Figure 1).
Perceived Confidence in Autism Diagnosis (n = 79).
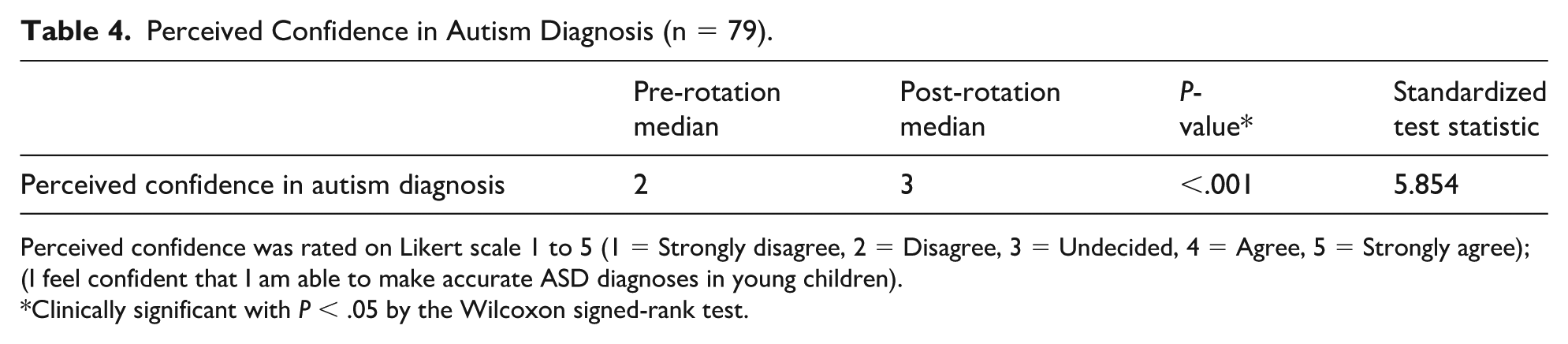
Perceived confidence was rated on Likert scale 1 to 5 (1 = Strongly disagree, 2 = Disagree, 3 = Undecided, 4 = Agree, 5 = Strongly agree); (I feel confident that I am able to make accurate ASD diagnoses in young children).
Clinically significant with P < .05 by the Wilcoxon signed-rank test.
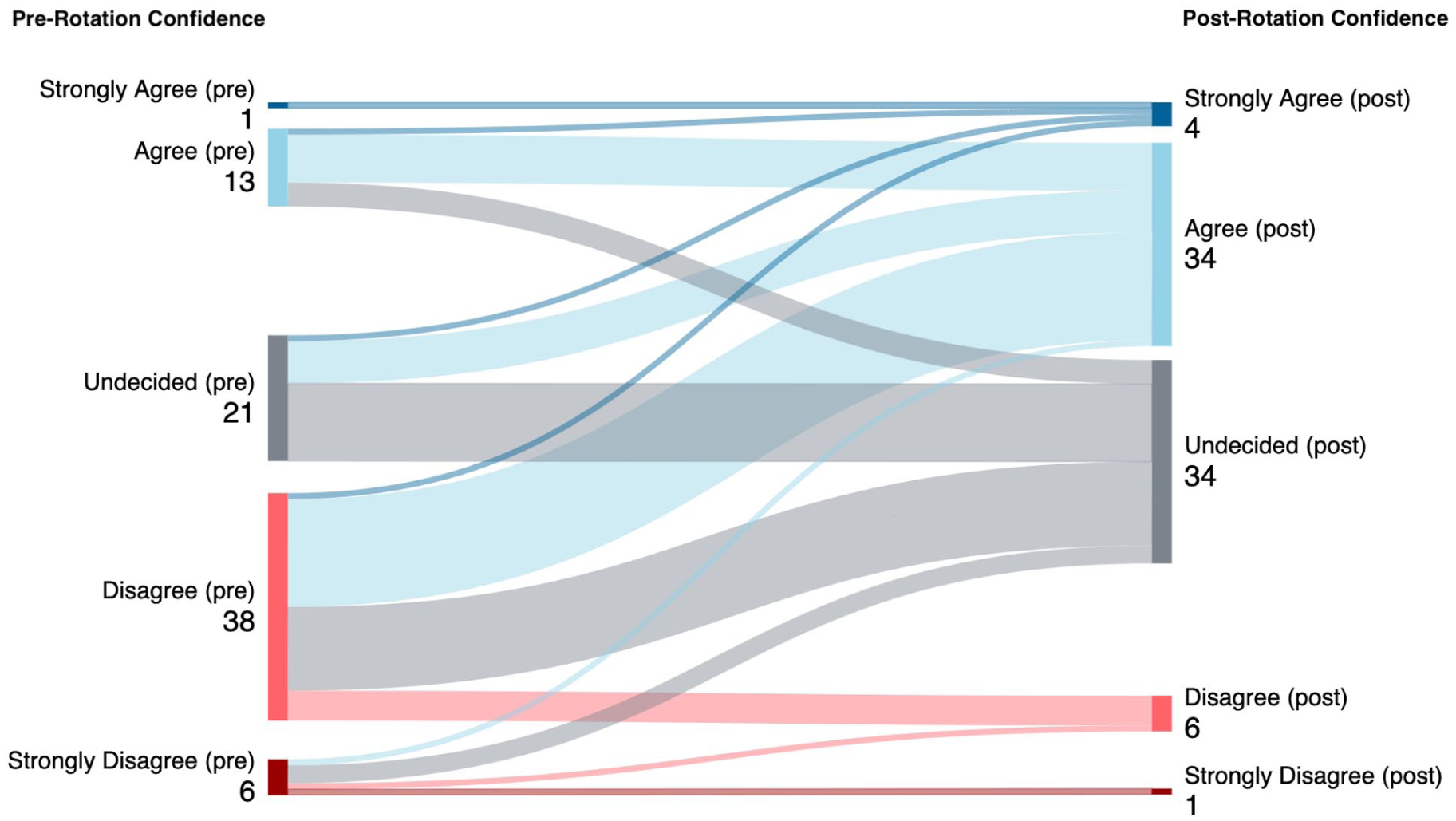
Perceived confidence in autism diagnosis pre-rotation and post-rotation in a Sankey graph. The graph demonstrates changes in responses.
Discussion
Rising rates of autism coupled with limited numbers of specialists have led to an increased awareness about the vital need to train the next generation of pediatricians in autism care through residency programs. In this study, we aimed to evaluate change in residents’ objective autism knowledge and perceived confidence following participation in a required 4-week DBP rotation, which was enhanced with an autism-specific asynchronous training module. To our knowledge, this is the first study that simultaneously evaluates pediatric residents’ change in confidence and specific domains of objective autism knowledge.
As anticipated, we found that residents demonstrated a significant increase in total autism knowledge from pre-rotation to post-rotation. This suggests that the content and experiences delivered during the DBP rotation are targeting key areas of knowledge about autism diagnosis in young children. Regarding specific domains, residents demonstrated a significant increase in General Autism Knowledge, Diagnostic Consultation, Diagnostic Formulation, Communicating Feedback, Recommendations, and Cultural Competency. Several of these domains were specifically targeted in the content of the asynchronous autism training module, notably General Autism Knowledge, Diagnostic Formulation, and Cultural Competency. While Communicating Feedback and Recommendations were less clearly targeted through the modules, it is expected that these topics are discussed and observed during scheduled clinical experiences, which may account for the significant increase in knowledge in these domains. There were no statistically significant changes in resident understanding of developmental screening. It may be that residents have a higher baseline exposure to screening, as the American Academy of Pediatrics (AAP) guidelines emphasize the importance of developmental screening in well visits 11 which residents frequently encounter and utilize during their ACGME-required primary care continuity clinics. 20
Given that the asynchronous module was adapted from training developed for primary care clinicians, it is noteworthy that our study revealed improvements in specific domains of autism knowledge. In a study examining the training of primary care providers, no significant changes were found before and after the training with regard to General Autism Knowledge, Diagnostic Consultation, or Diagnostic Feedback. 18 It may be that primary care providers seeking out specific training in autism have a greater baseline knowledge and interest regarding caring for autistic children in contrast to general pediatrics and combined pediatric residents, who may have limited exposure, experience, and interest in autism.
Results suggest that, on average, residents’ perceived confidence in making an autism diagnosis increased following participation in the rotation. These results suggest that residents feel more confident in their skills as a result of the rotation while also beginning to recognize the importance of training in autism. However, the median change for perceived confidence remained at undecided, suggesting additional training would be required to ensure general practitioners have adequate skills required to independently diagnose autism and provide management and resource support.36,37
Limitations and Future Directions
Several important limitations to this study should be considered when interpreting the findings. First, because our goal was to provide the training to all residents, we did not have a no-training control group; this design limits our ability to fully isolate the impact of the training module from the autism-focused clinical experiences and broader DBP rotation experience. Additionally, we cannot account for what residents may be learning outside their DBP rotation, such as in additional didactics, case conferences, clinician discussions, or board preparation. Future research may consider the use of a control group or other designs (eg, targeted assessment of knowledge immediately after module review) in an effort to isolate the impact of the module itself as well as the additive contribution of each various aspect of the DBP educational experience. Furthermore, this study did not assess differences in how residents may have viewed the module, whether module videos were viewed in order and the timing of viewing in relation to clinical experiences. During this study, residents were only asked about perceived confidence in autism diagnosis, not in the management of autism or the general care of autistic children. The latter question may be more relevant to pediatric residents who will be involved in providing ongoing care to autistic children in primary and subspecialty care but may not be involved in the diagnostic process. Importantly, it should also be noted that confidence in autism diagnosis may not be associated with autism diagnostic ability or changes in practice behaviors, as some primary care pediatricians have noted confidence in identifying symptoms but do not actually engage in diagnostic evaluation or demonstrate a lack of competency in making the diagnosis. 38 There could also be social-desirability bias, as residents may want to show improvements during training, although it is unlikely that residents remembered their initial responses from several weeks prior. Finally, the sample size is small, especially when considering differences between categorical pediatric residents and those in combined pediatrics programs. Each combined program presents a unique experience, and it would be helpful to assess differences between programs in order to tailor training needs in the future.
Future research is needed to address study limitations as well as to assess resident knowledge retention and practical use of knowledge (ie, competency) in clinical practice. For example, future work may examine changes in resident diagnostic skill through gathering baseline observational data at the start of the rotation and comparing it to performance at the end of the rotation. These data may include resident’s ability to competently complete a thorough developmental history or co-score standardized assessment instruments. A follow-up assessment once residents have completed training and are actively practicing in the community would allow for understanding how knowledge is retained over time, although careful measurement of additional training that residents may engage in would be a necessary consideration. Finally, understanding whether exposure to the autism module may be associated with the specialty that the residents ultimately enter could be useful in understanding how to build the DBP workforce.
Conclusion
This study demonstrates that a 4-week DBP rotation enhanced with an asynchronous autism training module improved pediatric resident autism knowledge, including overall knowledge and in many knowledge domains, as well as confidence in autism diagnosis. This demonstrates the potential for asynchronous module education combined with clinical experiences to improve autism knowledge in pediatric trainees. Focused comprehensive training of future pediatricians is essential to ensuring excellent care for children with autism.
Author Contributions
AA: contributed to analysis and interpretation of data; drafted manuscript.
AP: contributed to acquisition and analysis of data.
JH: contributed to conception; contributed to interpretation of data.
RMK: contributed to conception and design, contributed to acquisition and interpretation of data.
BE: contributed to conception and design, contributed to acquisition, analysis, and interpretation of data; drafted manuscript.
All authors: drafted, critically reviewed, revised manuscript; approved the final manuscript as submitted and agree to be accountable for all aspects of work.
Supplemental Material
sj-docx-1-cpj-10.1177_00099228261457335 – Supplemental material for Pediatric Residents’ Knowledge and Confidence in Autism Diagnosis: Impact of an Asynchronous Training Module Embedded Within a Developmental-Behavioral Pediatrics Rotation
Supplemental material, sj-docx-1-cpj-10.1177_00099228261457335 for Pediatric Residents’ Knowledge and Confidence in Autism Diagnosis: Impact of an Asynchronous Training Module Embedded Within a Developmental-Behavioral Pediatrics Rotation by Asna Asrar, Angela Paxton, Jordan Huskins, Rebecca McNally Keehn and Brett Enneking in Clinical Pediatrics
Supplemental Material
sj-docx-2-cpj-10.1177_00099228261457335 – Supplemental material for Pediatric Residents’ Knowledge and Confidence in Autism Diagnosis: Impact of an Asynchronous Training Module Embedded Within a Developmental-Behavioral Pediatrics Rotation
Supplemental material, sj-docx-2-cpj-10.1177_00099228261457335 for Pediatric Residents’ Knowledge and Confidence in Autism Diagnosis: Impact of an Asynchronous Training Module Embedded Within a Developmental-Behavioral Pediatrics Rotation by Asna Asrar, Angela Paxton, Jordan Huskins, Rebecca McNally Keehn and Brett Enneking in Clinical Pediatrics
Footnotes
Acknowledgements
The authors thank their colleagues at Vanderbilt University (Liliana Wagner, PhD; Jeffrey Hine, PhD; Paige McArdle, PhD; Madison Hooper) who developed the Autism Knowledge Questionnaire (AKQ). Erin Coffman, PhD, provided support with data visualization. The authors are grateful for the participation of the pediatric residents in this training program and in research activities. The authors also thank the leadership of the Indiana Early Autism Evaluation Hub system for their contributions to the module content. Mary Ciccarelli, MD, is a co-director of the hubs and contributed to the creation of the AKQ.
Ethical Considerations
The study (#17283) was determined to be exempt by the Indiana University Institutional Review Board (IRB) on July 7, 2022.
Consent to Participate
A study information sheet was provided prior to survey completion. All data were anonymized.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statements
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.