
Abstract
Hospitalized children experience educational disruption and reduced motivation during prolonged admissions. Despite the availability of in-hospital schools, many cannot participate due to illness severity or isolation precautions. This pragmatic, randomized crossover trial evaluated whether bedside virtual reality (VR) lessons improve intrinsic motivation among inpatients aged 5 to 25 years unable to attend the hospital school. Participants completed both VR-based educational sessions and standard of care (SOC) conditions on consecutive days. The primary outcome was intrinsic motivation, with secondary outcomes including educational self-efficacy, well-being, self-esteem, and parental experience. Of 156 enrolled patients, 100 were analyzed (mean age 11.5 [SD = 4.1 years]; 43.9% female). Intrinsic motivation scores were higher in the VR condition than SOC (P = .0048), and parental satisfaction was also greater (P = .0008). Bedside VR education represents a feasible, acceptable, and scalable adjunct to inpatient learning, supporting intrinsic motivation and caregiver satisfaction during hospitalization.
Keywords
Introduction
Pediatric patients with prolonged hospitalizations experience disruptions in their daily routine and school attendance, leading to decreased intrinsic motivation, educational self-efficacy, and long-term academic success.1-4 These disruptions also negatively impact a child’s well-being, social reintegration, and sense of normalcy. 4 Although in-hospital schools exist, many patients cannot access them due to illness severity, mobility limitations, isolation precautions, and treatment demands.1-3
Virtual reality (VR) is increasingly used in pediatric hospitals to reduce procedural pain and anxiety through immersive, gamified environments.5-7 These tools lack the side effects of pharmacologic anxiolytics and opioids and are accepted by hospitalized children and their caregivers.7-9 However, most clinical VR applications focus on symptom management rather than developmental or educational goals.8-11
Despite its promise, VR remains underutilized as a tool for enhancing intrinsic motivation during hospitalizations, and it is rarely used to improve academic engagement while hospitalized.5-7 Prolonged hospitalization diminishes motivation, as disruptions in routines, autonomy, and peer relationships undermine children’s sense of purpose and engagement.1,2 Virtual reality-based bedside education offers an affordable and scalable solution to support the mission of in-hospital schools in promoting psychosocial and academic success.
This study evaluated the effectiveness of VR as a learning adjunct for inpatient education, with the primary objective of determining whether VR-based bedside educational sessions improve task-specific intrinsic motivation compared with standard of care (SOC) among hospitalized pediatric patients. We hypothesized that bedside VR lessons would improve intrinsic motivation for pediatric patients unable to attend the in-hospital school compared with a standard day without instruction. Secondary objectives assessed the impact of bedside VR learning on educational self-efficacy, well-being, self-esteem, and parental experience.
Methods
Design
This was a pragmatic, randomized crossover trial conducted at a quaternary care, level 1 pediatric trauma center in Northern California. The hospital houses an in-hospital school operated by the local school district, which serves approximately 500 pediatric patients annually from diverse socio-economic and geographic backgrounds.
Each participant served as their own control to minimize variability related to clinical heterogeneity. The study used a 2-condition design in which participants received the bedside VR lesson as one condition and SOC without instruction as the other condition on consecutive hospital days, in randomized order. A washout period of approximately 1 day was observed between conditions, and surveys were administered independently after each session. The study adhered to the CONSORT guidelines for crossover trials. 12 The study protocol was reviewed and approved by the Institutional Review Board of the participating institution, and all procedures were conducted in accordance with the ethical standards of the Helsinki Declaration. Written informed consent was obtained from caregivers, and assent was obtained from minors when appropriate.
Participants
Eligible participants were inpatients aged 5 to 25 years who were admitted for at least 2 consecutive days and were unable to attend the in-person hospital school. Exclusion criteria included patients with a history of seizure disorder, current nausea, motion sickness, clinical instability, use of corrective glasses not compatible with the VR headset, current pregnancy, or inability to speak English. Participants were recruited sequentially using convenience sampling by trained research assistants (RAs), who approached patients in-person as they were admitted. 13 Written informed consent was obtained from caregivers, and assent was obtained from minors when appropriate.
Intervention
Participants randomized to the VR condition received a bedside educational session delivered entirely in VR using the Oculus Quest 2 headset (Meta, Inc., Menlo Park, California). Sessions were facilitated by a trained RA, who assisted with headset orientation, guided the experience, and provided educational support. Four educational software applications were used for the VR lessons: Titans of Space (DrashVR LLC, California), Leonardo da Vinci: Art and Innovation (Optima Ed Inc., Florida), The California Gold Rush (Optima Ed Inc., Florida), and Nature Treks: African Savannah (Greener Games, Telford, Shropshire, UK) (Supplemental Appendix A). These lessons were hosted the immersive VR platform Engage (Immersive VR Education Ltd., Waterford, Ireland).
Participants were offered a choice between science-focused or history-focused educational experiences. Science lessons included immersive “field trips” such as Titans of Space, in which participants toured the solar system, exploring planetary features like the atmosphere, surface conditions, and relative size of planets in a virtual environment. History lessons featured topics such as Leonardo da Vinci: Art and Innovation (Immersive VR Education Ltd., Optima Ed Inc.), allowing participants to explore da Vinci’s life, artwork, and inventions through interactive storytelling and virtual exploration.
Participants were allowed to select their preferred lesson, reflecting an autonomy-based model consistent with in-hospital school practices that emphasize individualized learning and patient choice. Preserving a sense of autonomy during hospitalization enhances engagement, motivation, and psychological well-being among pediatric patients.14,15 The same curated set of lessons was available for all participants, with facilitators adapting the discussions to the patients’ developmental levels. Each session lasted approximately 30 minutes and was delivered during standard school hours. After the VR intervention, participants completed surveys on intrinsic motivation, self-efficacy, well-being, and self-esteem, and then the RA concluded the session.
In the SOC condition, participants did not receive bedside educational instruction and instead engaged in unstructured activity during the designated time period of their choosing, such as watching TV, using a tablet, playing a game, or resting. Participants were asked to reflect on their typical hospital day and complete the same set of surveys that were administered after the VR education condition.
Outcomes and Measures
Patient demographics and primary admission diagnosis categories were collected, including age, gender, race, ethnicity, previous VR exposure, and primary admission diagnosis grouped into broad clinical categories. To account for affect as a covariate, the Positive and Negative Affect Schedule—Child (PANAS-C) was administered prior to the intervention (Supplemental Appendix B). 16 The PANAS-C consists of 10 items rated on a 5-point Likert scale (1 = very slightly or not at all to 5 = extremely), with 5 items assessing positive affect (eg, “Joyful” and “Happy”) and 5 assessing negative affect (eg, “Miserable” and “Afraid”). PANAS-positive affect (PA) and PANAS-negative affect (NA) scores were used as covariates in adjusted models.
The study’s primary outcome explored intrinsic motivation related to engagement with the educational activity (VR or SOC condition), which was measured by the intrinsic motivation inventory (IMI)—interest/enjoyment subscale (Supplemental Appendices C and D), a validated measure of task-specific intrinsic motivation reflecting interest and enjoyment. 17 This subscale includes 6 items rated on a 7-point Likert scale from 1 = not at all true to 7 = very true. Separate versions were used for the VR and SOC conditions, with identical structure but context-specific wording.
Secondary outcomes included educational self-efficacy, well-being, self-esteem, and parental experience. Educational self-efficacy was measured using a modified 6-item New General Self-Efficacy Scale (Supplemental Appendix E). 18 Each item was scored on a 5-point Likert scale ranging from 1 = strongly disagree to 5 = strongly agree. Well-being was assessed using the WHO-5 (World Health Organization-5) Well-Being Index (Supplemental Appendix F), 19 which includes 5 items rated on a 6-point Likert scale from 0 = at no time to 5 = all of the time.
Self-esteem was evaluated using a modified Rosenberg Self-Esteem Scale, with separate versions for children (<12 years) and adolescents (≥12 years) (Supplemental Appendices G and H).20,21 Both versions contain 5 items. The child version used a 4-point Likert scale from 1 = very true to 4 = definitely not true, while the adolescent version used 1 = strongly agree to 4 = strongly disagree.
Parental experience was assessed using a 7-item Parent Survey (Supplemental Appendix I), with items rated on a 7-point Likert scale from 1 = strongly disagree to 7 = strongly agree. The first 4 items addressed academic concerns, informed by measures of school functioning and reintegration such as the PedsQL School Functioning Subscale and the School Reintegration Questionnaire.22,23 The final 3 items assessed parental perceptions of the VR and SOC experience, including perceived value, learning, and overall satisfaction. All 7 items were analyzed individually and grouped into 2 composite scores: items 1 to 4 formed an “academic concern” score, and items 5 to 7 a “treatment satisfaction” score.
Sample Size
Given a typical mean score for the Intrinsic Motivation Inventory (Interest/Enjoyment subscale) of 5.7 (SD = 0.9), an alpha of 0.05, power of 90%, and a conservative improvement of 10% in their mean inventory score, the required sample size was calculated to be 71 patients. 24 To account for incomplete data and participant dropouts, the enrollment target was increased to approximately 150 patients.
Randomization
A pre-generated randomization allocation table was created using Excel (Microsoft Inc., Redmond, Washington). This table specified condition assignments according to the randomization scheme (1 = VR condition; 2 = SOC condition). The allocation table was imported into REDCap, which randomized participants to the order of study conditions.25,26 Randomization occurred after consent, prior to the first condition.
Blinding
Blinding of participants and facilitators was not feasible due to the visible use of the VR headset. However, the statistician was blinded to the study outcomes during analysis.
Statistical Analysis
All analyses were conducted in R (version 5.4.0) using the lme4 package. Linear mixed-effects models were used for all child outcomes (intrinsic motivation, educational self-efficacy, well-being, and self-esteem) to account for within-subject repeated measures. Each model controlled for the covariates of age, gender, PANAS-PA, and PANAS-NA, consistent with the analytic plan. Each outcome variable was modeled as the summed Likert-scale score and treated as continuous, following prior validation of these psychometric instruments. The primary outcome, intrinsic motivation, was analyzed using linear mixed-effect models with these covariates.
Secondary outcomes of educational self-efficacy, well-being (WHO-5), and self-esteem (child and adolescent versions) were analyzed using identical models and covariate adjustments. The specific VR lesson chosen by each participant (e.g., science- or history-focused) was not included as a covariate, as lesson selection was not hypothesized to influence outcomes. Because the self-esteem (child) scale exhibited a floor effect, an ordinal mixed-effects model was also tested as a sensitivity analysis.
For parent outcomes, paired t tests were used to compare mean scores between the VR and SOC conditions for each of the 7 individual items, as well as for the 2 composite subscales (items 1-4: academic concern; items 5-7: treatment satisfaction). Because some items violated normality assumptions, nonparametric Wilcoxon signed-rank tests were performed in parallel to confirm the robustness of results.
To evaluate potential period effects, mean outcome scores were compared between the first and second study periods. To assess potential carryover effects, the sum of outcomes across both periods was compared between participants randomized to the VR-first versus SOC-first sequence. A significant difference between sequences would indicate a carryover effect. These analyses were performed as sensitivity analyses to evaluate the assumptions of the crossover design.
In addition, a sensitivity analysis was performed comparing baseline characteristics between included and excluded participants using Fisher’s exact tests for categorical variables to assess for potential attrition bias.
Results
Participant Flow
A total of 156 pediatric inpatients were randomized (Figure 1). Seventy-nine participants were allocated to receive the SOC condition first, while 77 were allocated to receive VR first. All participants crossed over and received both conditions. Thirty-four participants dropped out of the study (15 randomized to VR-first and 19 to SOC-first), and 22 participants had incomplete data (15 VR-first and 7 SOC-first), resulting in a final analytic sample of 100 participants (47 VR-first and 53 SOC-first).
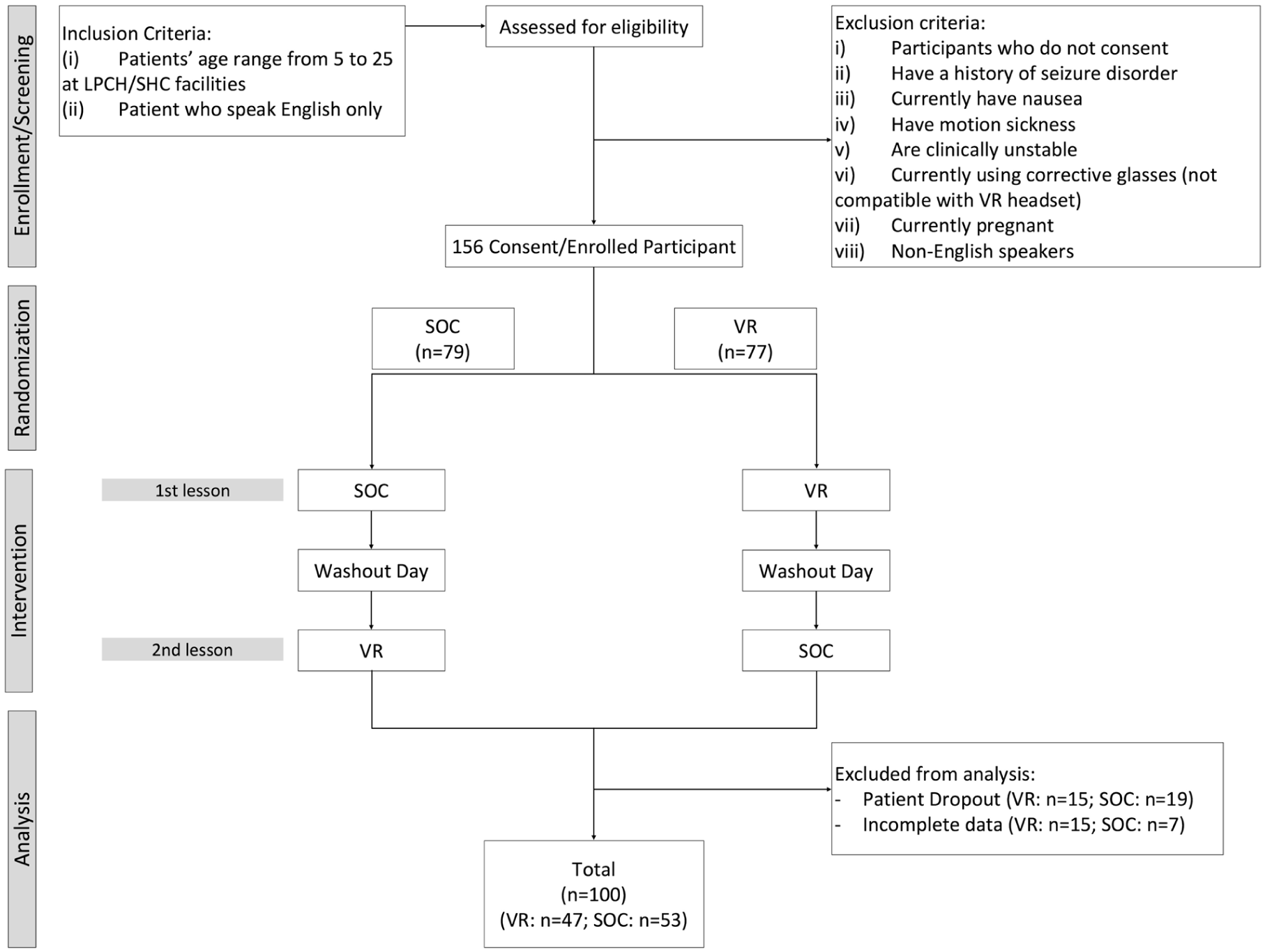
CONSORT flow diagram of participant enrollment, randomization, interventions, and analysis.
Among excluded participants, reasons included incomplete data (n = 22) due to either missing consent or data entry errors, and participant withdrawal (n = 34). There were no significant differences in baseline characteristics or randomized study arm (VR-first vs SOC-first) between included and those excluded from the analytic dataset due to incomplete baseline data (Supplemental Appendix J).
Recruitment
Participants were enrolled between October 17, 2023, and January 30, 2025. Surveys were collected on the same day following each condition. The trial was completed as planned, with no early termination.
Demographics
Among the 100 participants analyzed, the mean age was 11.53 (SD = 4.11 years) (range 5-20), with 52 children (<12 years) and 48 adolescents (≥12 years) (Table 1). Forty-three (43.9%) participants were female, 55 (56.1%) were male, and 2 (2.0%) had unknown gender. Participants represented diverse racial and ethnic backgrounds (Table 1). Prior exposure to VR varied: 36% had never used VR, 33% had used it 1 to 2 times, and 31% had used it greater than 3 times (Table 1).
Participant Characteristics.
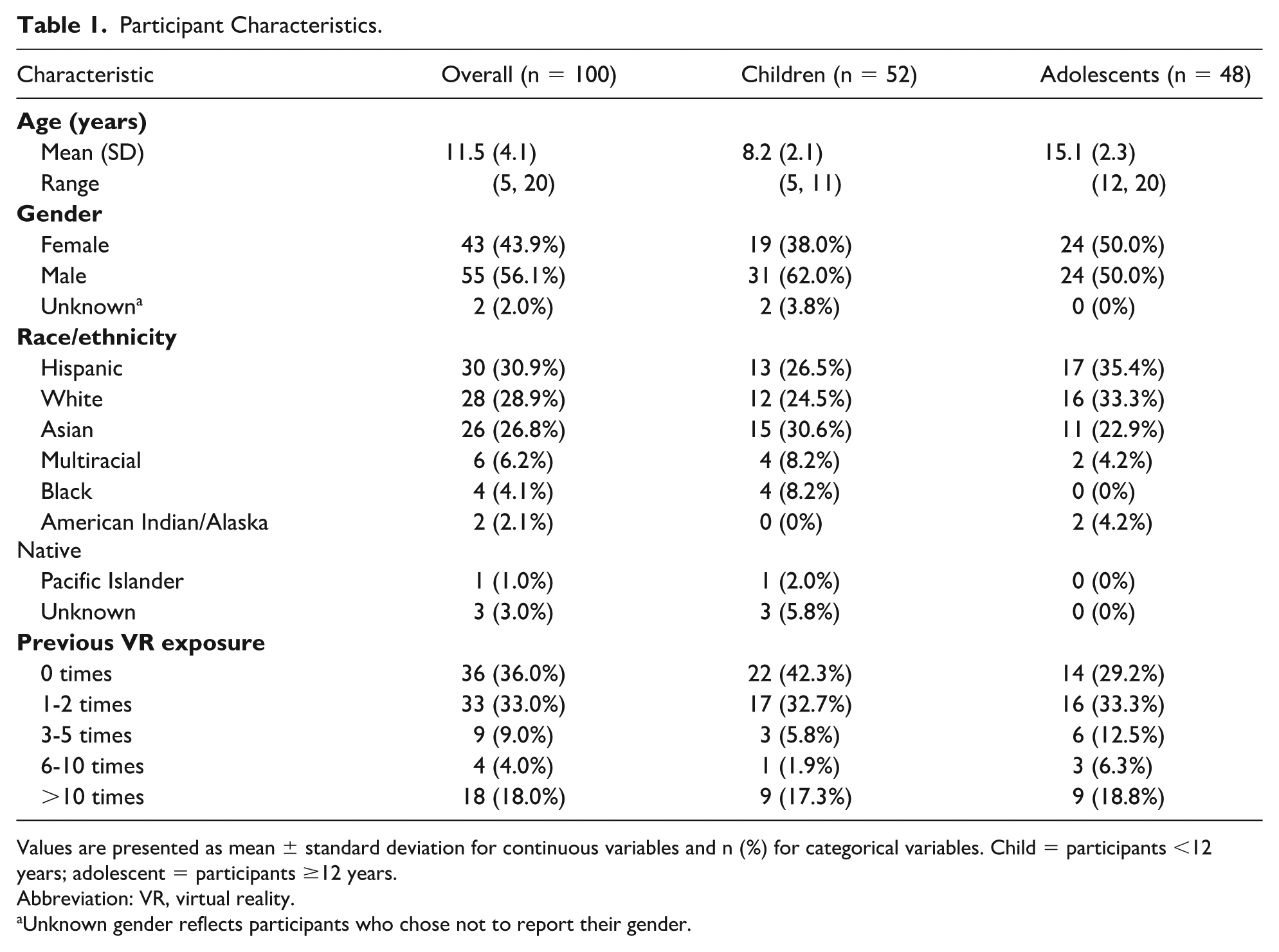
Values are presented as mean ± standard deviation for continuous variables and n (%) for categorical variables. Child = participants <12 years; adolescent = participants ≥12 years.
Abbreviation: VR, virtual reality.
Unknown gender reflects participants who chose not to report their gender.
Primary admission diagnoses were diverse, with the most common categories being oncologic (26.0%), gastrointestinal/hepatobiliary (18.0%), pulmonary/infectious (16.0%), and cardiac/cardiovascular (15.0%) (Table 2). The cohort included patients with primary admission diagnoses in both oncologic and psychiatric categories.
Primary Admission Diagnosis Categories.
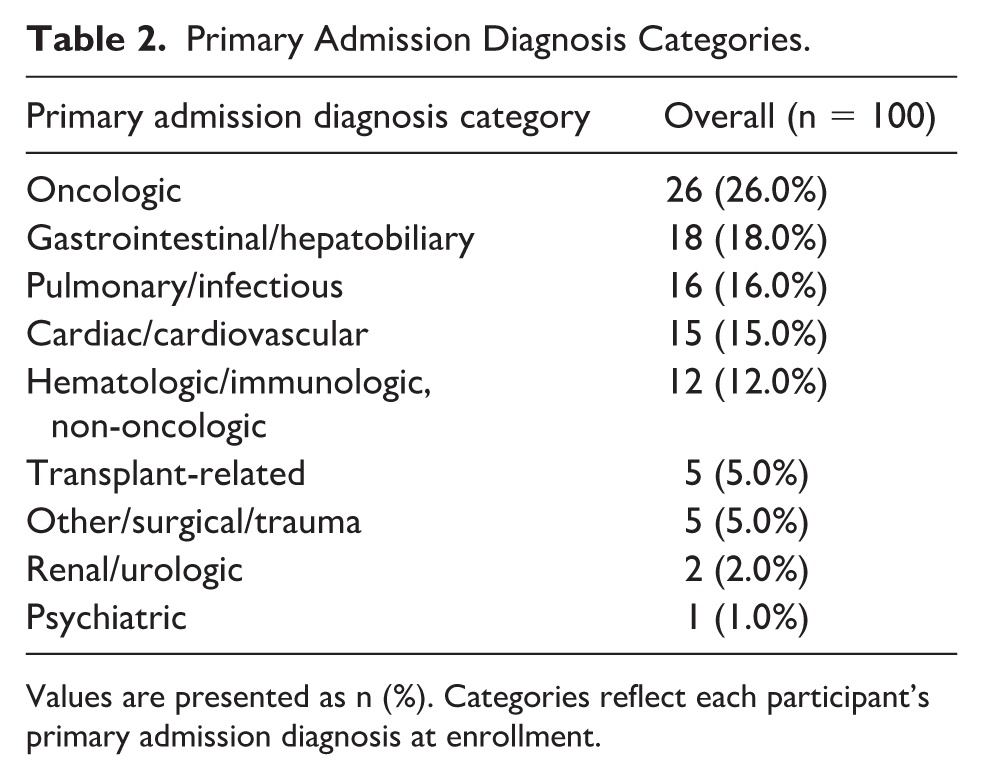
Values are presented as n (%). Categories reflect each participant’s primary admission diagnosis at enrollment.
Primary Outcome
Intrinsic motivation (n = 100) improved with VR compared with SOC (adjusted difference +2.80 units, P = .0048; β = 0.37; Cohen’s d = 0.43) (Table 3). The mean IMI total score ± SD was 35.6 ± 3.0 during the VR condition and 32.8 ± 2.8 during the SOC condition (Figure 2).
Primary and Secondary Outcomes.
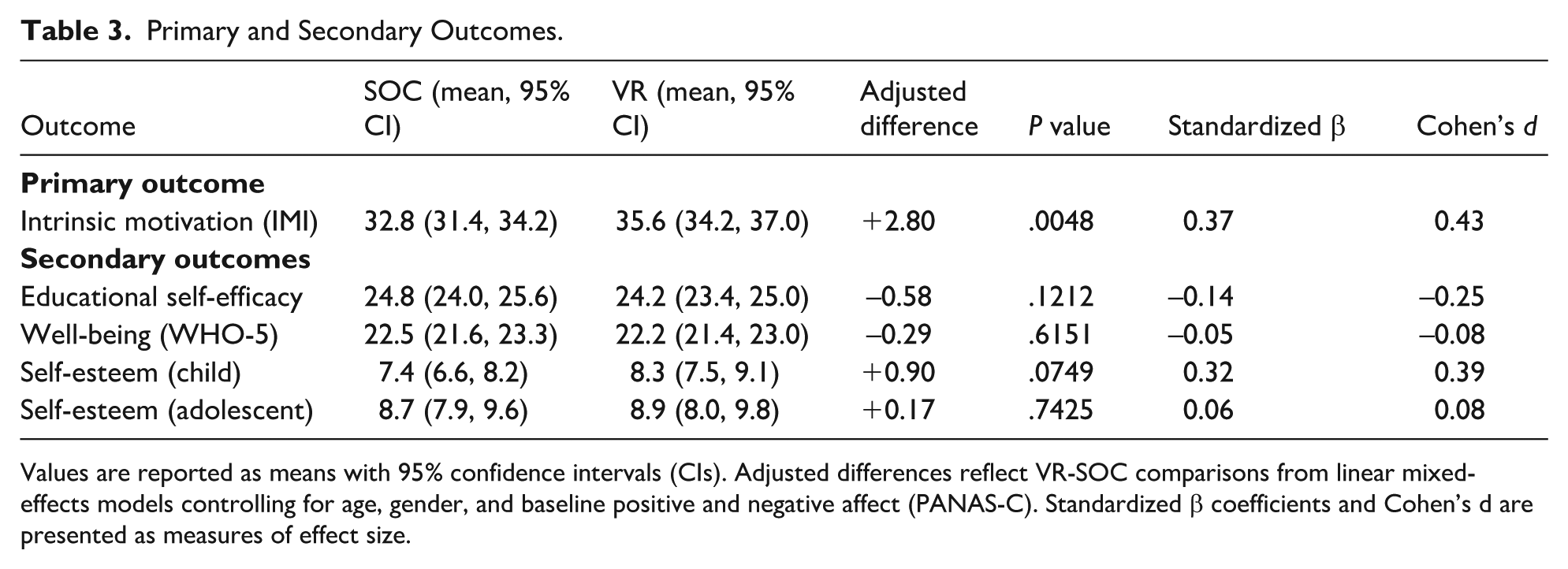
Values are reported as means with 95% confidence intervals (CIs). Adjusted differences reflect VR-SOC comparisons from linear mixed-effects models controlling for age, gender, and baseline positive and negative affect (PANAS-C). Standardized β coefficients and Cohen’s d are presented as measures of effect size.
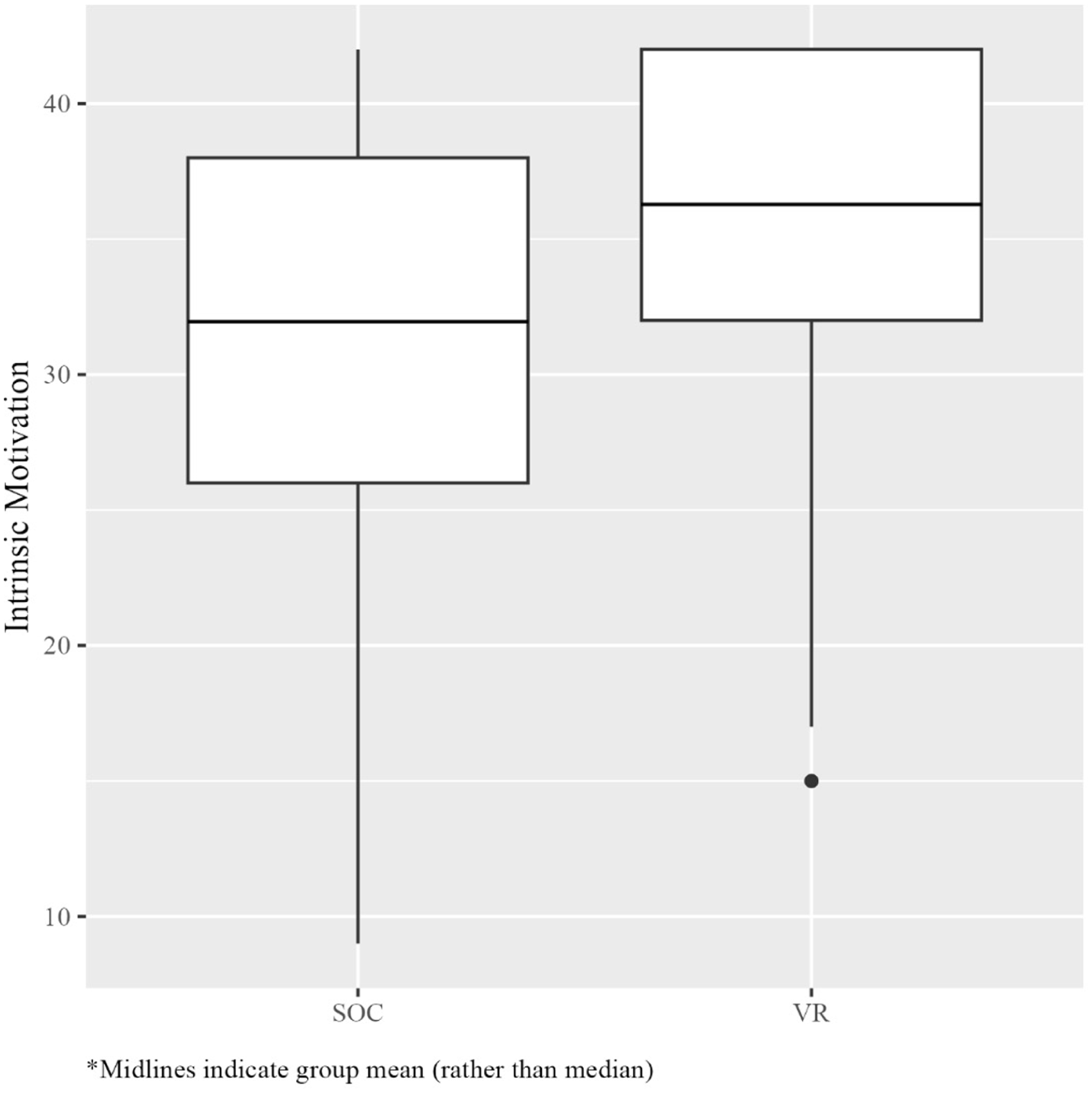
Intrinsic motivation scores by condition (VR vs standard of care). Boxplots display the distribution of intrinsic motivation inventory (IMI) sum scores for each condition. Midlines represent group means (rather than medians), and whiskers indicate the range of observed values. Participants reported significantly higher intrinsic motivation following the VR condition compared with the standard of care (P = .0048).
Secondary Outcomes
Educational self-efficacy did not differ between conditions (n = 100; P = .12) (Table 3). Similarly, there were no differences for well-being (n = 100; P = .62) (Table 3). Self-esteem analyses excluded 6 participants due to incomplete data. There were no differences in the child or adolescent versions (P = .075, P = .74, respectively) (Table 3).
Parent surveys were incomplete for 10 participants, providing 90 complete surveys from both conditions. There was no difference between conditions for the academic concern subscale (items 1-4; sum difference = −0.12, P = .8272). However, treatment satisfaction (items 5-7) was higher in the VR condition (sum difference = +1.49, P = .0008), with all 3 individual satisfaction items (items 5-7) demonstrating differences (P < .001) (Table 4).
Parent Survey Results Comparing SOC and VR Conditions.
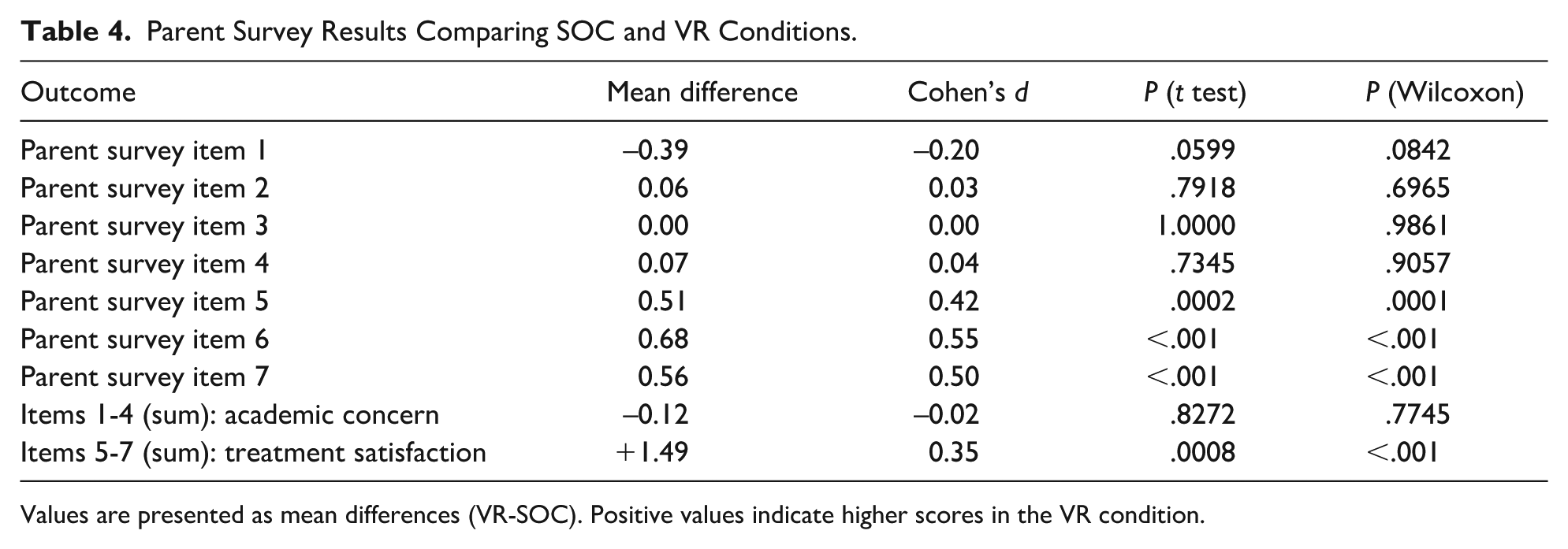
Values are presented as mean differences (VR-SOC). Positive values indicate higher scores in the VR condition.
Ancillary Analyses
Child self-esteem outcomes demonstrated a floor effect, with many participants endorsing the most positive response on all items. To address this limitation, an ordinal mixed-effects model was tested in addition to the primary linear mixed-effects model. The results were directionally consistent with the original analysis and remained statistically insignificant.
Crossover Analyses
To assess for period effects, mean outcome scores were compared between the first and second study periods. There were no significant differences across periods for any outcome, including intrinsic motivation, educational self-efficacy, well-being, or self-esteem, indicating no evidence of period effects (Supplemental Appendix K).
To evaluate potential carryover effects, the sum of outcomes across both study periods was compared between participants randomized to the VR-first and SOC-first sequences. No significant differences were observed between groups for any outcome, indicating no evidence of carryover effects or influence of condition order (Supplemental Appendix L).
Harms
No adverse events or withdrawals related to the intervention were reported.
Discussion
This crossover trial evaluated the impact of bedside VR educational sessions compared with SOC among inpatients at a children’s hospital. The primary outcome, intrinsic motivation, improved with VR compared with SOC, suggesting that immersive technology supports engaged learning during hospitalizations. These findings should be interpreted in the context of task-specific intrinsic motivation related to engagement with the VR educational activity, as measured by the IMI. Because this construct reflects interest and enjoyment in each activity, higher scores in the VR condition likely reflect the engaging and immersive nature of the educational experience. This aligns with the conceptualization of intrinsic motivation as inherently linked to the quality of the activity itself, rather than a fixed disposition toward learning. Secondary outcomes, including educational self-efficacy, well-being, and self-esteem, showed no differences between conditions. However, parents reported higher satisfaction during the VR condition, particularly on items related to treatment perceptions. No adverse events or safety concerns were reported, supporting the feasibility and safety of implementing VR as an adjunct to inpatient, bedside education. In addition, no significant period or carryover effects were observed, suggesting that the order of conditions did not influence outcomes. The 1-day washout period between conditions was therefore considered adequate for minimizing residual effects, particularly given the short-term and activity-based nature of the intervention.
Intrinsic motivation is a key driver of learning, persistence, and self-directed study. Hospitalization can diminish intrinsic motivation by disrupting children’s routines, autonomy, and social connections.14,27,28 In school-aged children, higher intrinsic motivation leads to stronger academic performance, greater classroom engagement, and improved self-regulation.27,29,30 Conversely, low intrinsic motivation is associated with disengagement, reduced persistence, and reliance on external rewards.27,31 Prolonged illness with time away from school can exacerbate this decline, compounding the academic and psychosocial challenges faced during hospitalization.2-4
In this study, bedside education delivered through VR improved intrinsic motivation related to the educational activity, suggesting that immersive environments may help reintroduce intellectual curiosity and a sense of engagement during hospitalization. Unlike passive activities without an educational component (eg, watching television or tablet use), the VR lessons required active participation with immediate feedback, which supports motivational processes.32,33 Given that teachers are a limited resource in pediatric hospitals and cannot provide individualized instruction for every inpatient, VR-based lessons may function as a practical and engaging bridge for patients awaiting bedside instruction. While not a replacement for in-person education, this approach can help maintain learning continuity and engagement until direct instruction is available.
These findings expand upon prior pediatric VR research, which has largely focused on pain and anxiety management, by demonstrating the role of VR in supporting academic engagement in the hospital.7,9,11 Virtual reality lessons offer a structured alternative to unstructured downtime in the hospital, complementing in-hospital schooling, particularly for patients unable to attend classroom activities in person. Because VR systems are already integrated into many pediatric hospitals for pain and anxiety management, expanding their use to include educational modules is scalable and logistically feasible. Existing infrastructure, trained staff, and institutional familiarity with VR platforms make educational applications a natural and sustainable extension of current practice.
The absence of improvements in educational self-efficacy may reflect the limits of a short-term, single-session intervention, as self-efficacy is generally strengthened through repeated mastery experiences rather than isolated exposures.34,35 Participants in this study received only one VR educational session, which may not have provided sufficient opportunity to build confidence in their learning abilities or demonstrate sustained competence in academic tasks. In contrast, intrinsic motivation may be more sensitive to short-term engagement and novelty effects, which could explain why improvements were observed in motivation but not in self-efficacy. Similarly, well-being and self-esteem may require longer or more personalized interventions to demonstrate measurable changes, and high baseline scores in some participants may have limited the ability to detect improvements. These findings underscore the difficulty of capturing rapid changes in complex psychosocial constructs and suggest that repeated VR educational sessions delivered across longer hospital stays may be necessary to produce measurable changes in educational self-efficacy and related outcomes.
Parent-reported satisfaction was higher in the VR condition, emphasizing the value caregivers place on structured and enriching activities during hospitalizations. Family-centered care is a cornerstone of pediatrics, and parental perceptions strongly influence both child well-being and long-term adjustment.36-38 Providing parents with reassurance that their child is engaged, learning, and supported reduces caregiver stress and improves overall care satisfaction. 39 When caregivers feel their child’s developmental and educational needs are met, they report greater confidence in the hospital team and stronger trust in the treatment process.40-43 These findings highlight VR’s dual benefit in addressing both patient engagement and caregiver reassurance, reinforcing its potential within family-centered care frameworks.
This study had several limitations. First, it was conducted at a single, quaternary care pediatric center, so that, the findings may not generalize to other hospital settings with different patient populations or educational resources. Second, the crossover design introduces the potential for carryover effects, although a 1-day washout period was implemented to mitigate this risk. Third, convenience sampling may bias results toward patients more willing or able to participate. In addition, although attrition occurred, no significant differences were observed in baseline characteristics or randomized study arm between included and excluded participants, suggesting a low risk of selection bias. Fourth, the lesson content was limited to space, Earth, and nature; broader academic subjects may be necessary to fully support educational needs. In addition, participants were allowed to choose among these lesson topics, but the specific lesson selected by each participant was not systematically recorded. As a result, we were unable to evaluate whether lesson type influenced outcomes, and variation in lesson content may have introduced unmeasured heterogeneity in the educational experience. Future studies should track lesson selection to allow for analysis of potential content-specific effects on learning engagement and psychosocial outcomes. Fifth, the outcomes relied on self-report surveys, which may be subject to recall or social desirability bias. In addition, the child self-esteem measure demonstrated a floor effect, suggesting limited sensitivity in detecting changes in this outcome within the study population. The restricted response range of the Rosenberg Self-Esteem Scale child version (<12 years) may have constrained variability and reduced the ability to observe meaningful differences between conditions. Finally, the study measured only short-term outcomes, precluding assessment of sustained academic or psychosocial impact following discharge. Future studies may benefit from selecting alternative self-esteem measures with a broader range of response options or greater sensitivity to short-term changes in psychosocial constructs in hospitalized children. Longitudinal follow-up could also help determine whether gains in motivation persist after hospitalization or translate into improved school reintegration.
Conclusion
Bedside VR educational lessons improved intrinsic motivation in hospitalized children, while effects on self-efficacy, well-being, and self-esteem were not observed. High parent satisfaction highlights the acceptability and perceived value of the intervention. Virtual reality represents a feasible, safe, and scalable adjunct to in-hospital education, with the potential to mitigate the psychosocial and academic disruptions associated with hospitalization. By bridging periods when formal teaching is unavailable, VR can serve as an engaging, autonomy-supportive tool that promotes continued learning and normalcy in the inpatient setting. Future research should examine whether repeated VR sessions can amplify or sustain motivational benefits across longer hospitalizations and explore broader curricula.
Author Contributions
Faith Collins: This author conceived, planned, supervised, contributed, revised, approved, and is accountable for the final manuscript. Emily Moya: This author drafted, reviewed, edited, and is accountable for the final manuscript. Marcos S. Rojas-Pino: This author performed investigation, reviewed, edited, and is accountable for the final manuscript. Michelle Guzman-Hernandez: This author performed investigation, reviewed, edited, and is accountable for the final manuscript. Faaizah Arshad: This author performed investigation, reviewed, edited, and is accountable for the final manuscript. Ruth Feng: This author performed investigation, reviewed, edited, and is accountable for the final manuscript. Ellen Y. Wang: This author supervised, contributed, revised, approved, and is accountable for the final manuscript. Samuel T. Rodriguez: This author supervised, contributed, revised, approved, and is accountable for the final manuscript. Christian Jackson: This author performed statistical analysis, reviewed, edited, and is accountable for the final manuscript. Thomas J. Caruso: This author conceived, planned, supervised, contributed, revised, approved, and is accountable for the final manuscript.
Supplemental Material
sj-docx-1-cpj-10.1177_00099228261460362 – Supplemental material for Virtual Reality Education for Hospitalized Pediatric Patients Improves Intrinsic Motivation: A Prospective, Randomized Crossover Study
Supplemental material, sj-docx-1-cpj-10.1177_00099228261460362 for Virtual Reality Education for Hospitalized Pediatric Patients Improves Intrinsic Motivation: A Prospective, Randomized Crossover Study by Faith Collins, Emily Moya, Marcos S. Rojas-Pino, Michelle Zuniga-Hernandez, Faaizah Arshad, Ruth Feng, Ellen Y. Wang, Samuel T. Rodriguez, Christian Jackson and Thomas J. Caruso in Clinical Pediatrics
Footnotes
Ethical Considerations
This study received approval from the Stanford University Institutional Review Board (Protocol no. 68166). All procedures were conducted in accordance with the ethical standards of the Helsinki Declaration.
Consent to Participate
Written informed consent was obtained from all caregivers, and assent was obtained from minors when appropriate.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data supporting this study’s findings are not publicly available due to patient confidentiality restrictions but may be made available from the corresponding author upon reasonable request and institutional review board’s approval.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.