
Abstract
Health care disparities stemming from language discordance have been well established, leading to increased morbidity and mortality. We sought to examine the effect of patient preferred language on time to rapid response activation and subsequent intensive care utilization. We sought to evaluate the association between patient preferred language and time to rapid response (RR) activation, intensive care unit (ICU) transfer rate, and intensive care utilization in a quaternary pediatric hospital. We conducted a retrospective observational study of pediatric patients with rapid response activation from January 2020 to June 2023. Demographic and clinical data, including time to rapid response, ICU transfers, and use of mechanical ventilation, non-invasive ventilation, and vasoactive support, were analyzed. Statistical comparisons were performed between English-speaking and language other than English (LOE) patients, with subgroup analyses for Spanish-speaking patients. Of 374 unique patients, 25% were using LOE. Time to rapid response activation was not significantly different between language groups. However, Spanish-speaking patients were more likely to be transferred to the ICU (P = .0047) and had longer hospital stays (10 vs 7 days, P = .0425). While language preference did not impact time to rapid response activation, Spanish-speaking patients had increased ICU transfers and prolonged hospital stays. These findings highlight the need for improved language-concordant care to mitigate disparities in pediatric critical care outcomes.
Introduction
While patients using a language other than English (LOE) are a growing population, significant disparities persist within the health care system with respect to access, efficient navigation, and communication. From 1980 to 2019, the US Census Bureau reports that the number of people who spoke a language other than English at home tripled from 23.1 million to 67.8 million.1,2 Studies have shown that language-discordant care may compromise the quality of care and increase the risk of morbidity and mortality.3-7 This morbidity and mortality risk appears independent of ethnicity and socioeconomic status.3,8 Language other than English has been independently associated with medical complexity, and children who utilize an LOE have prolonged length of stay (LOS). 9
Within a pediatric admission, caregivers utilizing an LOE are reported to experience lower-quality communication during rounds, are less involved in medical discussions, and can receive inconsistent interpretation services10-12 With this language barrier, children are at risk for clinical decompensation that may be missed. When a pediatric patient is admitted to the general pediatric floor and there is an increase in acuity or concerning clinical finding, a rapid response is activated 13 It has been established that patients using an LOE are more likely to be transferred to the intensive care unit (ICU) within 24 hours of admission, but there are no studies evaluating the intermediate step of the rapid response. 14 This study seeks to examine the association of patient preferred language on the time to respiratory rate (RR) activation, subsequent transfer to ICU, and intensive care utilization.
Methods
We conducted a retrospective observational study of all pediatric patients with a rapid response activation from January 1, 2020 to June 30, 2023. Patients were admitted to the general pediatric unit at an urban quaternary center in New York City. This study was reviewed and approved by our Institutional Review Board (HS #: STUDY-23-00814). Within our hospital system, approximately 25% of patients have non-English language preference. Similarly, approximately 30% of the population in our city speak a language other than English at home, most commonly, Spanish. 15
Our rapid response team was instituted in 2020 and had a gradual rollout through the calendar year. The team consists of the Pediatric Intensive Care Unit (PICU) charge nurse, a respiratory therapist, and either the PICU fellow or attending depending on availability. At the time of this data collection, rapid responses were triggered only by the primary health care team. During the daytime, the pediatric ward is covered by a pediatric hospitalist and team of residents. Specialty patients are cared for by a pediatric gastroenterologist, hepatologist, oncologist, or neurologist, with remaining patients treated by the hospitalists. Overnight, attendings are not in-house. We do not have any nurse practitioners or physician assistants on the pediatric ward. Our pediatric unit can take patients with bronchiolitis under the age of 2, without comorbidities, utilizing up to 2 L/kg of high-flow nasal cannula. The oxygen limitation on the ward is otherwise 4L via nasal cannula or up to 40% FiO2 via venturi mask. Patients with a tracheostomy are eligible for the floor if they are not rate-dependent on the ventilator and are otherwise on their baseline home settings. Patients with obstructive sleep apnea can use nocturnal non-invasive devices on the pediatric unit. Beyond this, patients go to the PICU.
Each rapid response is evaluated by the team, and the disposition is based on clinical judgment. Criteria for activation include, but are not limited to, hemodynamic instability, unexplained change in mental status, acute drop in oxygen saturation or increase in FiO2 requirement, suspicion of acute bleeding, new major electrolyte or test abnormality, or concern about a patient’s condition. At the time of this submission, families could raise concerns to staff, but there was no formalized family-activation of a rapid response. A rapid response is required for all unplanned transfers to the ICU. At the time of this data collection, if a patient triggered Systemic Inflammatory Response Syndrome (SIRS) during a night shift when a pediatric hospitalist was not present, a rapid response was mandatory. Our hospital electronic medical record (EMR) automatically calculates SIRS as defined by the 1991 Society of Critical Care Conference, utilizing temperature, heart rate, RR, and white blood cell count. 16 A comprehensive list of activations was obtained through an internal hospital data warehouse query for rapid response activation notes. Following a rapid response, the responding nurse and physician write a clinical note in the EMR, serving as a trigger for the data pull.
Demographic data including preferred language, race, ethnicity, sex, and age were obtained through the EMR Face Sheet. These demographic entities are designated by the patients’ caregiver. Within our EMR, a pediatric patient’s language preference is dictated by the parental language preference, even if the patient prefers English. Clinical data including time of activation, time to activation, transfer to ICU, and ICU utilization were obtained through manual chart review. Time to activation was defined as the time differential between the time admitted to the pediatric ward and the time of activation.
The primary outcome was the time to rapid response from admission to the pediatric floor or transfer from the PICU. Secondary outcomes included association of patient acuity as measured by the Pediatric Early Warning Signs (PEWS) score (reference range = 1-9), 17 LOS, and ICU utilization including mechanical ventilation (MV), non-invasive ventilation, and vasoactive support. We noted the PEWS score at the time of rapid response and the highest PEWS score within 24 hours of the rapid response activation. If the PEWS score was not automatically available, we manually scored the patient.
To determine the time to statistical differences between English-speaking and LOE-speaking groups, we performed a univariable random-intercept linear regression model with log-transformed time to rapid response and adjusted for repeat measures. We performed multivariable random-intercept linear models that included English-speaking/LOE-speaking group, as well as potential confounding variables such as demographics and clinical patient characteristics. These methods were also applied to a 3-category exposure: English-speaking, Spanish-speaking, and non-English/non-Spanish-speaking.
We performed a chi-square test or Fisher’s exact test to compare binary outcomes of rapid response characteristics, use of MV, use of non-invasive ventilation, and use of vasoactive support between English-speaking/non-English-speaking groups, and the independent-sample t-test or Mann-Whitney test to compare PEWS scores and LOS between English-speaking/non-English-speaking groups. In addition, we examined the role of holiday staffing and time of day.
We used univariable negative binomial regression models with the number of rapid responses prior to first ICU admission to determine statistical differences between English-speaking and non-English-speaking groups, and English-speaking, Spanish-speaking, and non-English-speaking groups, respectively. Multivariable analyses were carried out using multivariable negative binomial regression models to include English-speaking/non-English-speaking group as well as potential confounding variables such as demographics and clinical patient characteristics.
Results
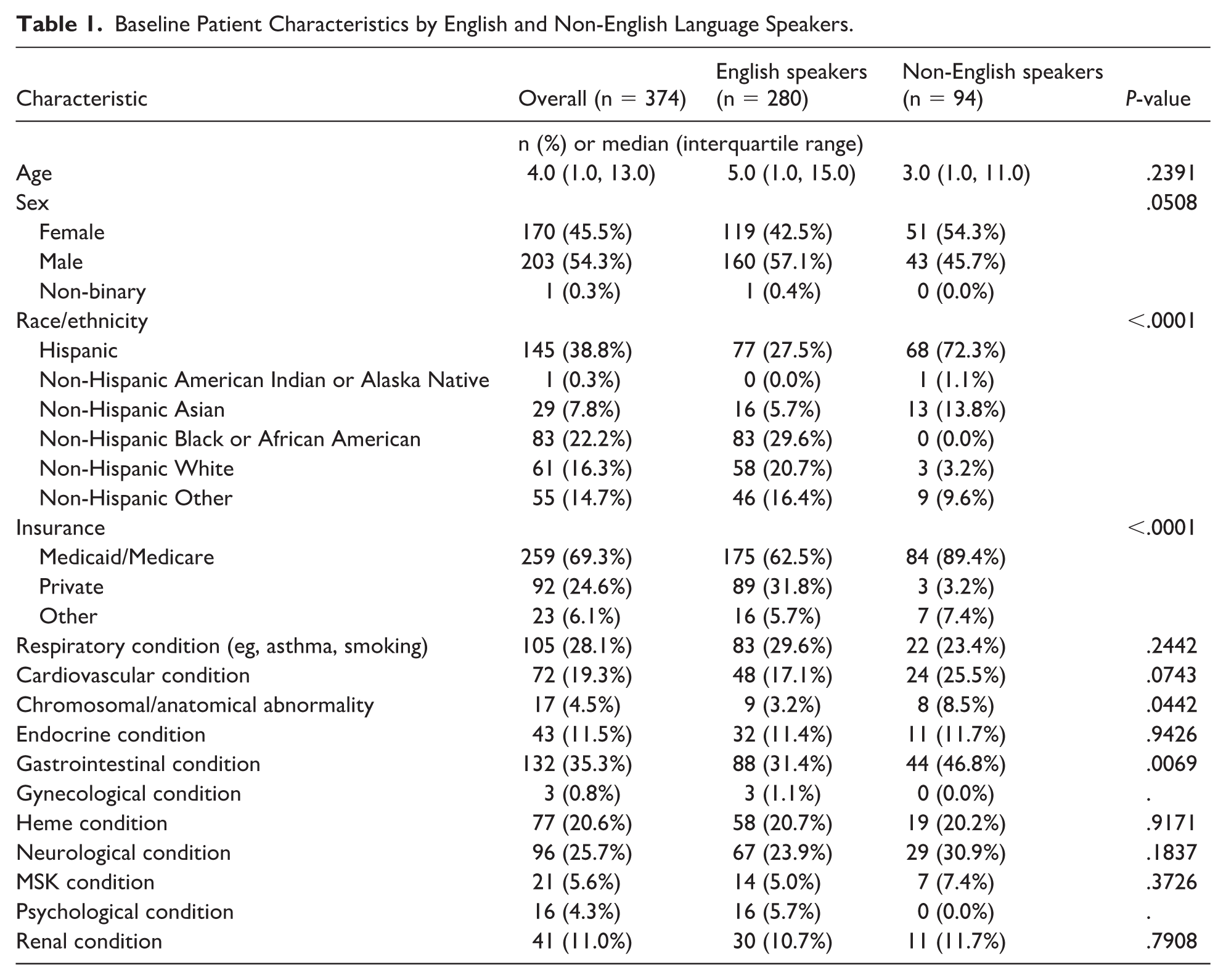
There were 432 rapid responses reviewed with 374 unique patients that met inclusion criteria (Table 1). Of these, 280 (75.0%) were English-speaking, and 94 (25.0%) were LOE-speaking. Language other than English includes Spanish, Arabic, Bengali, and Mandarin. Overall demographics included a median age of 4.0 years (1.0, 13.0) and 45.5% identified as female. The median PEWS score overall and for all individual language groups was 2.0 at the time of activation, and the maximal PEWS score within 24 hours of activation was 2.0 for all language groups. There were no statistically significant differences in rapid response activation for weekend or holiday staffing, or time of day. The LOE speakers were statistically more likely to have comorbidities of chromosomal abnormalities and gastrointestinal issues.
Baseline Patient Characteristics by English and Non-English Language Speakers.
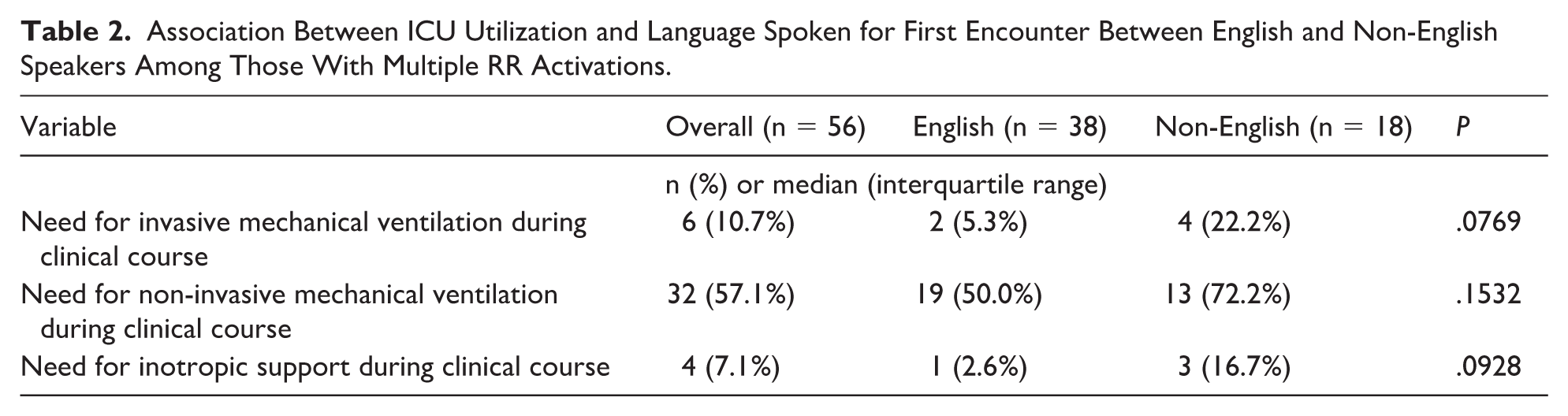
Overall, the median time to rapid response was 26.4 hours. Patients using an LOE had a median time to rapid response of 27.4 hours vs English-speaking patients with 26.4 hours, which was not statistically significantly different (Figure 1). Spanish-speaking patients were more likely than English-speaking patients to be transferred to the ICU during their admission. Conversely, non-English/non-Spanish-speaking patients were less likely to be transferred (P = .0047; Figure 2). The overall median LOS was 8 days (4.0, 17.0). The LOE-using patients had a significantly higher LOS compared to English-speaking patients (10 days [4.0, 26.0] vs 7 days [4.0, 15.0]) (P = .0425; Figure 3). When comparing patients who had multiple rapid response activations, LOE patients descriptively had a higher proportion of MV, non-invasive MV, and vasoactive support (Table 2).
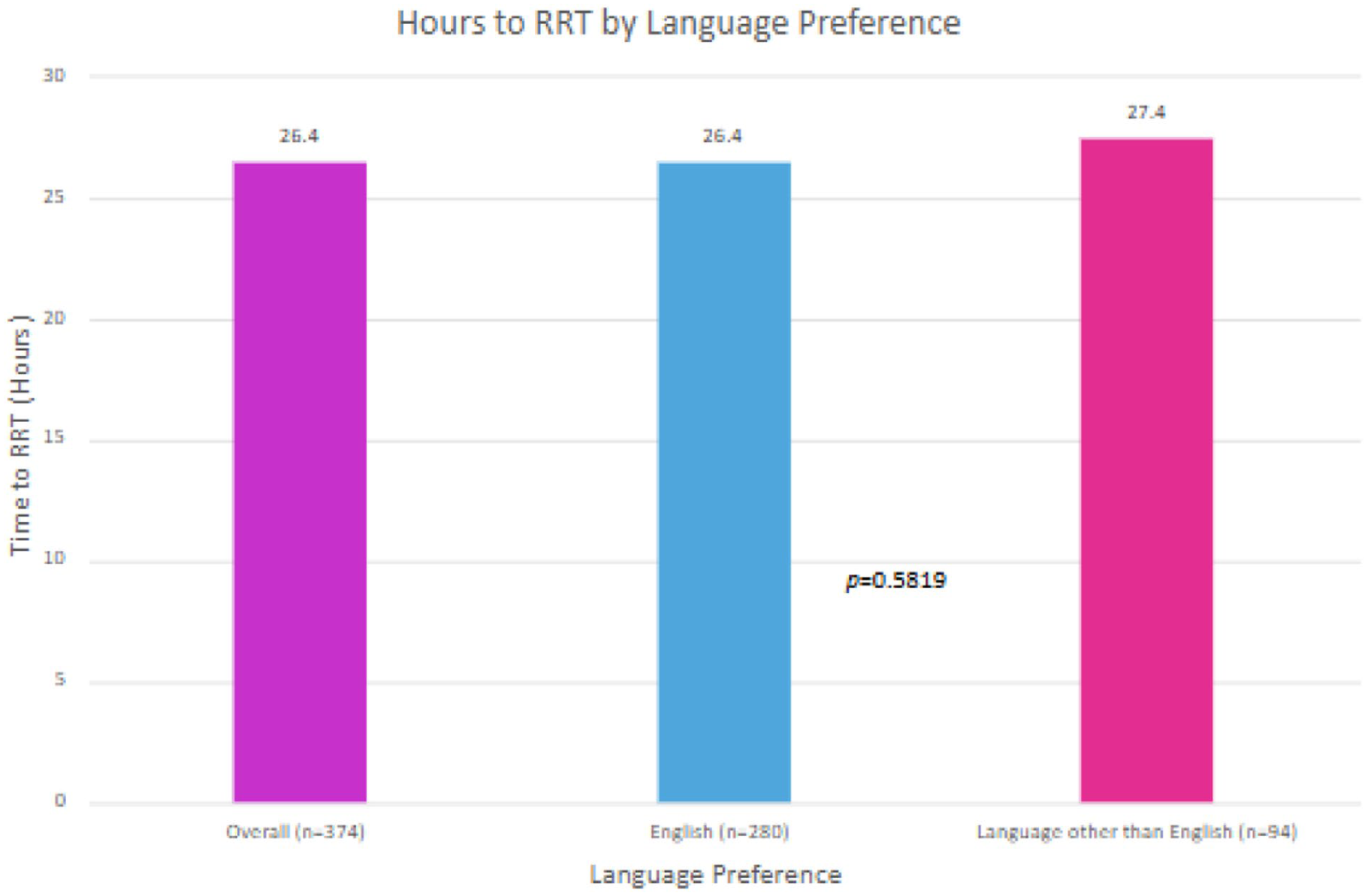
Association of language preference and time to RR. Overall, the median time to RR was 26.4 hours. The LOE patients’ time to RR was 27.4 hours vs English-speaking patients with 26.4 hours, which was not statistically significantly different.
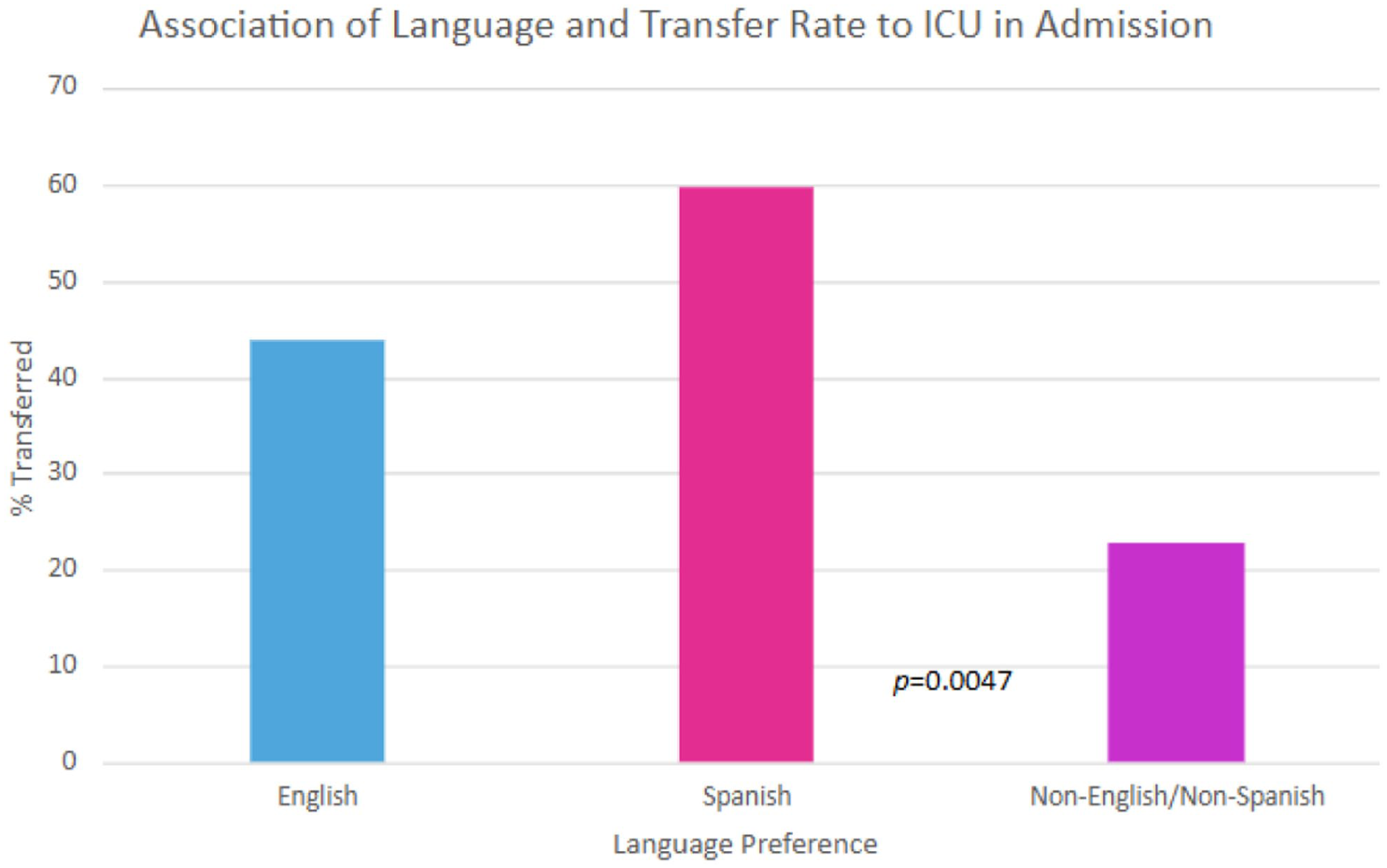
Association of preferred language to ICU transfer rate during admission. Spanish-speaking patients were more likely than English-speaking patients to be transferred to the ICU during their admission. Conversely, non-English/non-Spanish-speaking patients were less likely to be transferred (P = .0047).
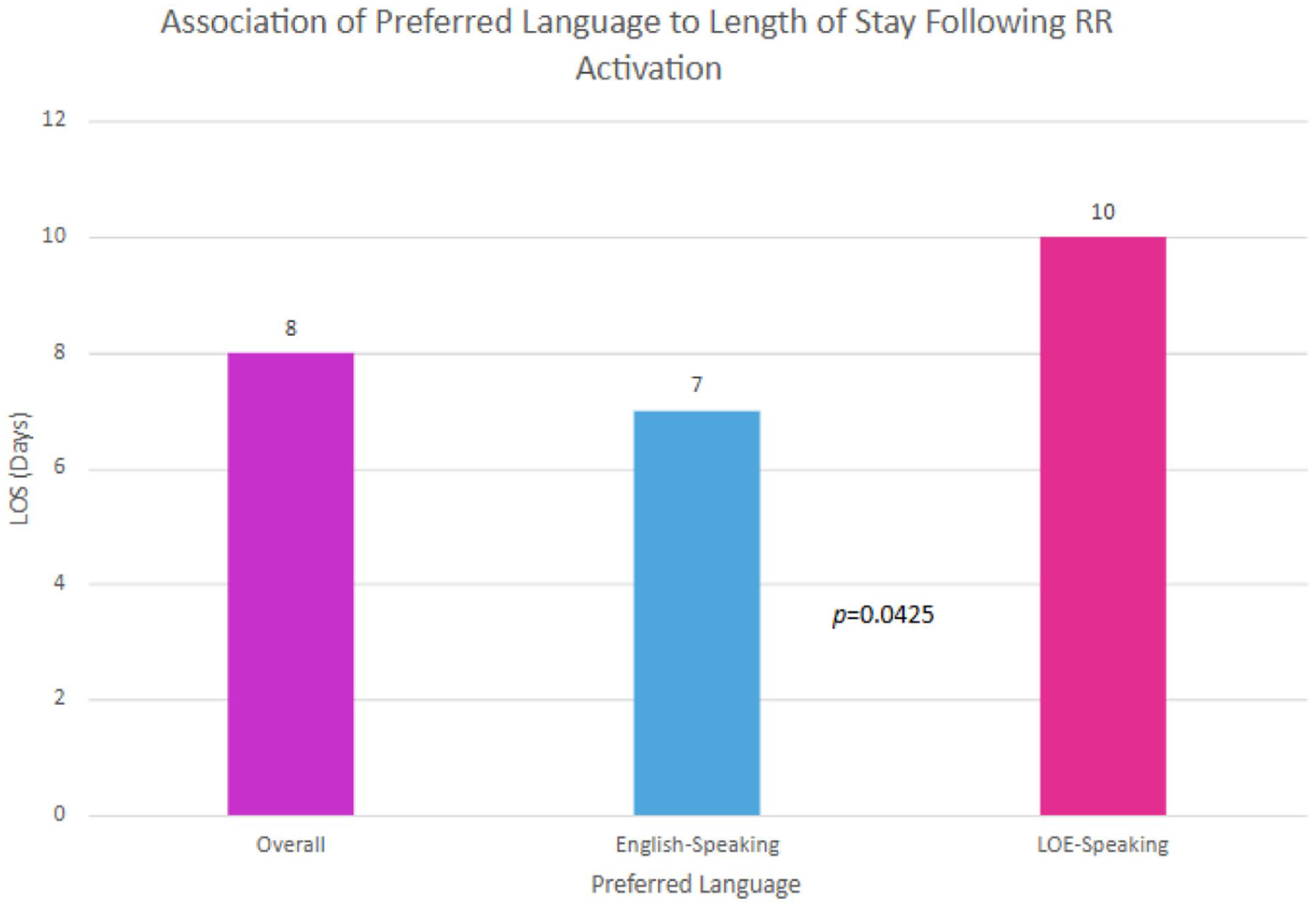
Association of preferred language to length of stay following RR activation. Overall median length of stay was 8 days (4.0, 17.0). The LOE patients had a significantly higher LOS compared to English-speaking patients (10 days [4.0, 26.0] vs 7 days [4.0, 15.0]) (P = .0425).
Association Between ICU Utilization and Language Spoken for First Encounter Between English and Non-English Speakers Among Those With Multiple RR Activations.
Discussion
Our study sought to test the hypothesis that LOE language preference would delay time to rapid response activation and increase both time to transfer to the ICU and intensive care utilization within an urban quaternary pediatric hospital. While we found that time to RR activation was not statistically different amongst the language groups, there were notable distinctions in clinical outcomes that are important, including LOS and transfer rate. Non-English as a preferred language may create barriers between clinicians and family, such that their needs are not effectively communicated. These findings provide important questions about how language barriers may influence patient care and outcomes in the pediatric ICU.
One of the key findings of our study is that Spanish-speaking patients were more likely to be transferred to the ICU compared to their English-speaking counterparts despite equivalent acuity. It is important to better understand the etiology of the increased transfer rate, as it is known that ICU transfers are associated with higher morbidity and mortality.3,4 The reasons for the increased transfer rate are likely multifactorial. Patients could be triaged incorrectly from the emergency department (ED) or outside transfers. This theory is supported by published research in which children with LOE-speaking caregivers were more likely to be under-triaged from the ED, where they were initially identified as low-resource requiring but ultimately required admission or high-resource utilization within the ED. 18
Additionally, patients with language barriers may not be able to effectively communicate their needs. This idea is supported by a qualitative study exploring the role of language in medically complex children. Parents within this study noted increased ease and ability to communicate with language-concordant medical teams. 19 Furthermore, they noted the challenges of medical professionals who falsely spoke in Spanish, which was concerning for the family and interfered with their ability to communicate with the medical team. 19 Parents also noted that they were not able to request an in-person interpreter or initiate an iPad interpreter, limiting their ability to initiate and advocate for medical care. Interpreter omissions and alterations may also lead to incorrect messaging and can compromise patient care. 20 At the time of this study, our hospital’s daily interpreter or dual language provider documentation rate was approximately 25%. Within our hospital system, clinicians are only permitted to speak an LOE with a patient and their family if they have been certified by the institution’s language services. At the minimum, patients should be addressed in their preferred language at least once a day and additionally with changes in clinical status or rapid response activation.
Increased LOS in non-English-speaking patients is consistent with previously published studies.9,21 Our findings show that LOE-speaking patients had a significantly higher median LOS compared to English-speaking patients. This is also likely multifactorial, as there can be delays in care plans, increased teaching required for discharge, and communication errors between the medical team and family. Extended hospital stays can also be resultant of increased comorbidities of these patients. Familial culture can also play an important role in communication with the medical team through multiple pathways, including information preferences, decision-making styles, family involvement expectations, and communication norms. Cultural backgrounds may shape who communicates with the team and the shared decision-making pattern,22,23 thus potentially influencing care.
While non-English-speaking patients showed a higher trend requiring increased ICU utilization with increased MV, non-invasive MV, and inotropic support, statistical significance was not reached. This study may have been underpowered, and future studies with larger sample sizes would be needed to conclusively determine this relationship.
While there was a statistically equivalent mean time to rapid response activation, as Spanish-speaking patients are transferred at higher rates, it could suggest that they had delayed recognition of deterioration. The question also arises as to why these patients score equally on the PEWS score when they are deemed to be sicker and transferred more often.
The limitations of this study include its retrospective nature, which is reliant on documentation accuracy and completeness, which may introduce bias. This study was also single-centered, so future studies will use a multi-center approach to better generalize to the greater public. Additionally, we report the preferred language of the patient from the EMR, which at our institution is usually accurate but does pose potential error. We do not have access to interpreter utilization or frequency of utilization due to a lack of consistent documentation in our hospital at the time of data collection. Implicit and explicit bias may contribute to observed differences in findings.
Despite these limitations, this study is important in that it highlights a potential determinant of clinical outcomes in pediatric patients. Future studies should focus on prospective designs to explore the impact of language barriers, communication quality, and patient outcomes. An important distinction will also be the level of English proficiency of the patient’s family and language concordance of the medical team, as well as interpreter utilization. Additionally, this study indicates the need for further research to examine the root of these disparities and allow for interventions to improve patient safety and outcomes. Standardized communication tools, such as visual aids or structured escalation checklists, may help mitigate language-related barriers in recognizing clinical deterioration. Future work should evaluate whether these interventions improve equity in rapid response activation.
Conclusion
While the patient preferred language did not significantly impact time to rapid response activation, it was associated with increased ICU transfers and prolonged hospital stays in pediatric patients. Our findings highlight the need for continued efforts to address language barriers in health care, as these barriers may limit our ability to provide exceptional care.
Author Contributions
Dr Rachel E. Moss conceptualized and designed the study, collected data, drafted the initial manuscript, and critically reviewed and revised the manuscript.
Dr Jan Fune collected data and critically reviewed and revised the manuscript.
Ms Catherine McDonough helped design data collection instruments, carried out initial analyses, drafted the initial manuscript, and critically reviewed and revised the manuscript.
Dr Shubhi Kaushik conceptualized the study and critically reviewed the manuscript for additional analysis.
Dr Sandeep Gangadharan conceptualized the study, supervised the study production, and critically reviewed and revised the manuscript for important intellectual content.
All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Footnotes
Ethical Considerations
This study was reviewed and approved by the Mount Sinai Institutional Review Board (HS #: STUDY-23-00814).
Consent to Participate
Consent-exempt study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statements
Data may be made available upon request.