
Abstract
Pediatric invasive Group A Streptococcus (iGAS) infections two years before, during, and a year after the Coronavirus Disease 2019 (COVID-19) pandemic were analyzed in an urban hospital in the Northeastern United States. Invasive GAS was diagnosed in 38 patients. There were as many infected children post-COVID as in the prior 4.5 years combined. The post-pandemic surge was most striking in late spring. The median age was youngest during the post-pandemic year at 2.3 years. During and after the pandemic, about half the children had concurrent virus detection, and two-thirds had no known chronic comorbidities, highlighting Streptococcus pyogenes’ potential for significant morbidity in healthy and young children. The spectrum of iGAS disease manifestations was similar among the 3 time periods, with soft tissue infections predominating overall. Of post-pandemic GAS isolates, 67% were emm1 and 33% were emm12. Preventive efforts of this grave disease at all ages should continue.
Keywords
Introduction
Invasive Group A Streptococcus (iGAS) infection is defined as isolation of Group A streptococcus from a sterile site.1-4 The disease is often severe, can be fatal, and can occur in healthy children.5,6 The spectrum of invasive infection includes complicated pneumonia, focal skin and soft tissue infections (SSTI) with bacteremia, bacteremia with no apparent focus, sepsis with or without shock, osteomyelitis and septic arthritis, necrotizing fasciitis, and toxic shock syndrome.1-4,7 Group A Streptococcus can produce exotoxins that serve as super-antigens. Its hyaluronic acid capsule is studded with M protein, coded by the emm gene, which inhibits opsonization and phagocytosis. 8 The emm gene is the basis for GAS serotyping and is a useful epidemiological marker to distinguish strains. 9
Prior to the Coronavirus Disease 2019 (COVID-19) pandemic, the Centers for Disease Control and Prevention (CDC) estimated 14 000 to 25 000 annual iGAS cases and 1500 to 2300 attributable deaths in the United States. 4 After COVID-19-related pandemic mitigation measures were lifted, iGAS was being reported at a higher rate in Europe and certain parts of the United States than in previous years.10-14 We describe pediatric iGAS epidemiology and characteristics before, during, and after COVID at our tertiary children’s hospital in New York City.
Methods
A retrospective chart review of patients, ages 0 to 18 years, hospitalized with confirmed and probable iGAS was conducted at our children’s hospital in a major metropolitan area in the northeast of the United States. We subdivided cases into 3 time periods: pre-COVID pandemic period (A), spanning 2 years, January 2018 through December 2019; during the COVID pandemic period (B), lasting 2.5 years, January 2020 through May 2022; and the immediate post-COVID pandemic period (C) spanning 1 year, June 2022 through May 2023.
Confirmed iGAS was defined by growth of GAS in culture, or its detection by polymerase chain reaction, from sterile sites. Probable iGAS included patients who presented in sepsis with no other explanation, and GAS growth was from throat or soft tissue culture. To identify patients, we obtained GAS isolates from our microbiology laboratory database. We also extracted electronic medical records from the hospital information system based on disease-specific International Classification of Diseases, Tenth Revision (ICD-10) codes.
The study received ethical approval from our hospital institutional review board (IRB) (approval #2023-06-14-MMC) on October 15, 2023. The IRB waived the need for a consent due to the retrospective nature of the study. Data were stored in password-protected computers and access to data was restricted to investigators. Data were collected and managed using the REDCap electronic data capture tool.
We analyzed and compared the number of iGAS cases, disease manifestations, patients’ demographics, concurrent illnesses, comorbidities, and hospital length of stay (LOS). Nasopharyngeal sample molecular testing, using BioFire Respiratory Panel 2.1 (BioMérieux, Salt Lake City, Utah), was performed from patients with upper respiratory tract infection symptoms pre-COVID, and from every admitted patient during and after COVID. Some GAS isolates were sent to the state laboratory for emm typing.
Statistical analysis: We performed stratified analyses for key clinical variables. Continuous variables were reported as median with interquartiles, and categorical variables were reported as counts and percentages as appropriate. Age is presented as median with interquartile ranges (IQRs). Confidence intervals (CIs) were calculated for iGAS incidence rates and mean LOS. Chi-square test for independence evaluated the relationship between time-period and iGAS incidence rates. One-way analysis of variance evaluated the relationship between time-period and mean LOS. Calculations were performed using IBM SPSS Statistics. A P value of <.05 was considered significant. Given the descriptive nature of the study, no formal adjustment for confounders was performed.
Results
We identified 38 patients with iGAS: 9 in period A, 11 in period B, and 18 in period C. Five patients were categorized as having probable iGAS. Pediatric admissions’ census was 5588, 5266, and 2403 in periods A, B, and C, respectively. The incidence rate of hospitalizations due to iGAS was 0.16% in period A (95% CI: [0.074%, 0.31%]), 0.21% in period B (95% CI: [0.1%, 0.37%]), and 0.75% in period C (95% CI: [0.44%, 1.2%]). A χ2 test of independence showed these differences to be significant, X2(2, N = 13,257) =22.18, P < .001.
In the first winter after the pandemic restrictions ended, iGAS numbers surpassed those of prior winters of our study period. However, most iGAS cases occurred in the spring of the post-COVID period C, with 11 of 18 cases (61%) diagnosed between March and May 2023 (Figure 1).
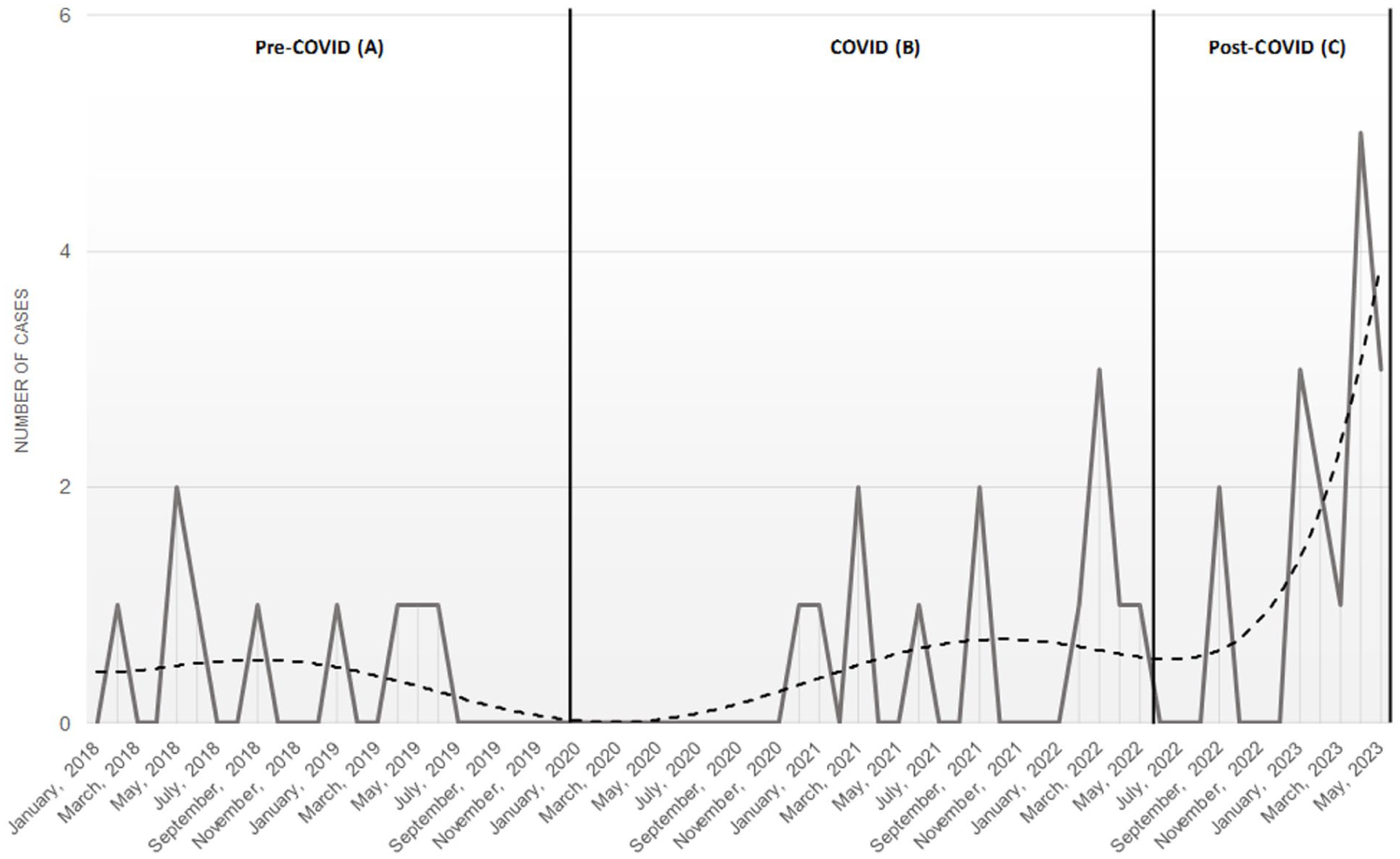
Invasive Group A Streptococcus case distribution over the 3 study periods’ months.
Median patient age was 2.6 years (IQR: 1.42-9.33 years) in period A, and 2.3 years (IQR: 0.83-6.61 years) in period C; in period B, the median age was 5.8 years (IQR: 1.08-6.75 years) (Table 1). In each period, the majority of patients were male.
Patient and Disease Characteristics of 38 Children with Invasive GAS Infections by Period of Study.
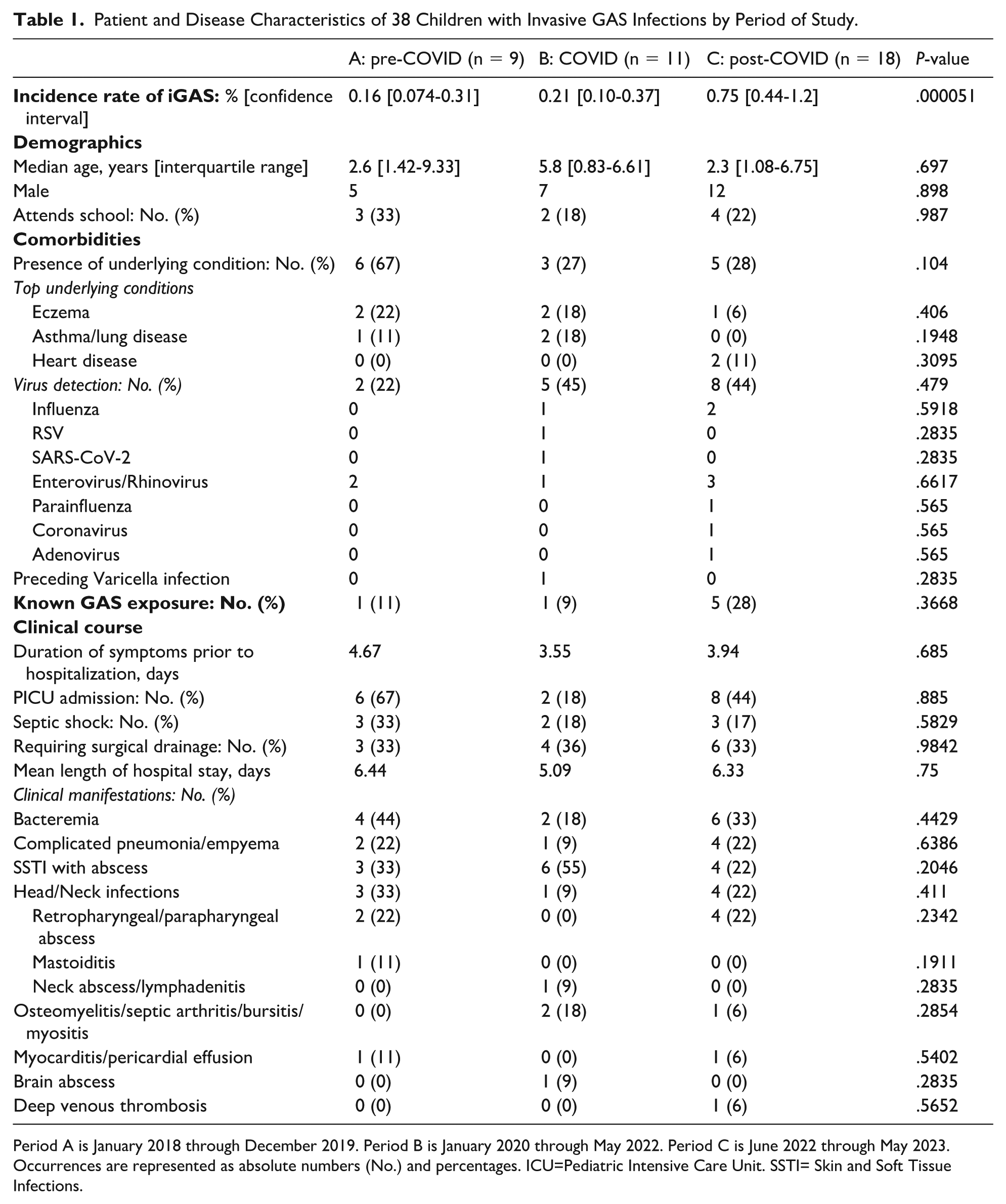
Period A is January 2018 through December 2019. Period B is January 2020 through May 2022. Period C is June 2022 through May 2023. Occurrences are represented as absolute numbers (No.) and percentages. ICU=Pediatric Intensive Care Unit. SSTI= Skin and Soft Tissue Infections.
During period A, 6 of 9 patients had underlying medical conditions. In contrast, the majority of children during periods B (8 of 11) and C (13 of 18) had no chronic problems. Eczema was the most prevalent comorbidity (13%), and all but one such patient had SSTI with abscess (Table 1).
Respiratory viral detection was more common during periods B (45%) and C (44%) (Table 1); all children with a co-detectable virus had symptomatic upper respiratory tract infections. Influenza was detected in ~8% overall. Influenza vaccination rates were 50%, 18%, and 39% in periods A, B, and C, respectively. A recent close contact with GAS pharyngitis was most frequently reported in the post-COVID period.
The difference in mean LOS among the 3 time periods was not significant: 6.44 days in period A (95% CI: [2.49, 10.4]), 5.09 days in period B (95% CI: [1.88, 8.31]), and 6.33 days in period C (95% CI: [4.12, 8.54]) (Table 1).
During COVID, 55% of patients had SSTI with abscess, most of whom had preceding local trauma. The proportion of bacteremia, complicated pneumoniae, musculoskeletal (osteomyelitis, arthritis, myositis, bursitis), and head and neck infections did not vary among the 3 periods (Table 1). About one-third of patients in each period required invasive procedures. There were no fatalities.
Emm typing was performed on 10 isolates. One was emm26 identified by the CDC from the blood isolate of an infant visiting the United States during COVID, and presenting in septic shock following varicella infection abroad, complicated by GAS brain abscess. The remaining 9 were post-pandemic isolates: emm1 was identified in 6 patients, 3 of whom had bacteremia, 1 had pneumonia, and 2 had deep neck infections. Emm12 was detected from the other 3 patients, 1 each with bacteremia, SSTI, and osteomyelitis.
Discussion
Invasive GAS infections in our urban hospital in New York City increased significantly in the year after COVID-related distancing ended, with almost as many infected in that 1 year as in the prior 4.5 years combined. Similar to CDC’s trend reports during the height of COVID restrictions, we had only 1 iGAS patient in 2020. Between April 2021 and May 2022, while the pandemic was ongoing but public schools reopened, we identified 10 such children, with their median age oldest at 5.8 years. The lowest median age was post-pandemic—lower than other reported iGAS post-pandemic surges,12,13 but not statistically different from our pre-pandemic cohort median.
Most children with iGAS in our study were healthy. The most common comorbidity, eczema, as well as equally frequent preceding local trauma, potentially increased patients’ risk for GAS invasiveness, as pre-existing skin lesions and micro skin tears are thought to serve as entry points for invasive disease.3,4
Post-pandemic, the severity of iGAS disease, and its spectrum of clinical manifestations and outcomes did not seem to change. Hospital LOS was similar to pre-pandemic years.
Group A Streptococcus infections tend to have a seasonal pattern, with the majority occurring in winter and early spring. We noted a shift in this usual pattern in the post-pandemic period where the peak of cases was noted in late spring. Almost doubling of cases in spring 2023 following the 2022-2023 winter uptick has not been reported in the United States to date. A change in typical seasonality of another pathogen, RSV, was reported during 2020-2021, when peaks shifted to the spring. 15
A proposed mechanism for iGAS’ seasonal predilection is concurrently circulating viruses during high-incidence periods, along with more time spent indoors. 4 It is postulated that influenza and other viruses aid GAS with tissue invasion. 16 Only about half of our patients during and after COVID had concurrent viral detection, and predominantly not influenza.
Exposure to children with pharyngitis, a major reservoir of GAS, has also been recognized as a significant risk factor for invasive GAS infections. During COVID-19, with social distancing and school and daycare closures, there was a marked reduction in circulating viruses as well as iGAS disease. This likely led to an overall decreased immunity to these pathogens. The subsequent surge in iGAS cases can be partly explained by this large vulnerable population of children.
Post COVID, our invasive infections were mostly emm type 1 followed by emm12. In France, emm1 was most common in post-pandemic iGAS, 17 whereas in the Texas and Colorado outbreaks, emm12 was dominant.10,13
Our study provides a detailed comparison of iGAS patients in COVID-related time periods that has not been previously described in the United States, demonstrating that the various manifestations of disease did not alter post-COVID despite the major spike in the number of cases. It highlights the dependence of iGAS on exposure and immunity, a shift in the typical seasonality of this pathogen after COVID, and that the causative emm types were those historically associated with invasive disease. The study has several limitations. The patients are from a single center, and their number is small, making it difficult to infer clinically significant differences in disease manifestations. Furthermore, the study was not designed to adjust for potential confounding factors such as crowded living or overall GAS rates in the community. Emm typing was not performed from all periods, limiting comparison of strain prevalence over time.
Awareness, prompt diagnosis, and treatment of GAS-related disease cannot be emphasized enough. Hand hygiene and adequate ventilation are suggestions to help mitigate spread. 18 The study alerts general and emergency pediatric practitioners about this serious infection that once thought rare, may not be as rare after COVID, and once thought a winter disease, may be occurring in warmer months. In addition, insight into emm types in our environment at the time is valuable information to experts in the field. It is vital to expand on research into how viruses play a role in GAS invasiveness. While waning immunity may promote streptococcal epidemics, potential fitness advantages of certain strains continue to be explored. 19
Author Contributions
All listed authors made substantial contributions to the conception, design, execution and analysis of the data of this study.
Footnotes
Ethical Considerations
This study received ethical approval from the Maimonides Medical Center IRB (approval #2023-06-14-MMC) on October 15, 2023. This is an IRB-approved retrospective study, all patient information was de-identified and patient consent was not required. Patient data will not be shared with third parties.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.