
Abstract
In this study, we examined data from 200 families to investigate whether family functioning and adolescent psychiatric symptomatology were associated with differential attendance in a family-based or individually focused intervention for Latino adolescents. Latent profile analysis was used to identify families, and regression models were used to examine whether profiles exhibited differential attendance. Overall, three latent profiles were observed. The first described families where parents and adolescents reported discrepancies on psychiatric symptoms and family conflict. The second profile described families with elevated adolescent psychiatric symptoms but no family conflict. The third profile described families with low family cohesion and high levels of adolescent psychiatric symptoms. For this third profile, attendance in family-based treatment was significantly higher than in individual treatment. Results indicate that a family-based intervention may be better able to address issues of poor family cohesion.
Efforts to promote healthy adolescent development have led to the design and testing of prevention programs (Mrazek & Haggerty, 1994; O’Connell, Boat, & Warner, 2009) that seek to reduce known risk factors. These may include behavior problems that first emerge in adolescence and can negatively affect educational achievement as well as sexual health, and can increase the risk of serious mental and substance use disorders as well as violence (Patel, Flisher, Hetrick, & McGorry, 2007). Early conduct disorder (McGee, Williams, Poulton, & Moffit, 2000), attention-deficit/hyperactivity disorder (ADHD; Barkley, Fischer, Smallish, & Fletcher, 2004), depression (Kelder et al., 2001), and poor family functioning (Dishion, Bullock, & Granic, 2002) have been found to predict these poor developmental outcomes during adolescence and young adulthood. Treatment programs can be designed to reduce or eliminate existing internalizing and externalizing behavior problems and family conflict in an effort to prevent the onset of serious mental and substance use disorders and HIV/AIDS (Donenberg & Pao, 2005).
Family-centered interventions have been shown to be efficacious in treating adolescent behavior problems (Kaslow, Broth, Smith, & Collins, 2012) and in preventing substance use disorders and risky sexual behaviors (Kumpfer & Alvarado, 2003; Lopez et al., 2008; Pantin et al., 2003). These family interventions have the potential for mobilizing and enhancing protective processes that can benefit the adolescent long after the treatment period. They can also teach parents to intervene against ecological stressors that negatively influence the child (Coatsworth, Santisteban, McBride, & Szapocznik, 2001).
When working with Latino clients, family therapy can be a particularly powerful intervention to identify and address the family process disruptions that may occur as a result of acculturation processes (e.g., adolescents acculturating faster than adults), acculturation stress, and immigration-related stressors (Cervantes, Fisher, Córdova, & Napper, 2012). Different rates of acculturation within the family can disrupt communication and conflict resolution, as well as lead to behavior problems in youth (Martinez, 2006; Santisteban, Mena, & Abalo, 2013). The important link between family functioning and mental health among Latinos has been well documented in the literature and has been observed among adults (see Fish, Maier, & Priest, 2015; Mulvaney-Day, Alegría, & Sribney, 2007) as well as adolescents (Prado et al., 2007). Consequently, family-based interventions have been found to be efficacious in preventing initiation of substance use and engagement in risky sex (Prado et al., 2007), even among Latino adolescent clients with the most concerning profiles (Santisteban, Mena, Muir, et al., 2015).
The use of family-based interventions, especially with Latino populations that tend to underutilize mental health services, lead us to ponder two critical questions: The first was whether we could identify unique profiles of participants based on psychiatric and behavioral symptoms, as well as family functioning, using a person-centered approach rather than investigating single variables in isolation; the second was whether the person-centered profiles that emerged would be associated with different attendance in two treatment interventions. The practicality of using a family-based intervention would likely be challenged when high conflict and low cohesion are prominent symptoms in the family, given that they have the potential to disrupt treatment participation (Santisteban et al., 1996). The identification of challenges to full treatment participation is important, given the literature that suggests that premature dropout has detrimental effects on treatment outcomes (Boggs et al., 2005; Kim, Munson, & McKay, 2012; Schroder, Sellman, Frampton, & Deering, 2009), and that ethnic minorities may be even more likely to terminate treatment prematurely (Austin & Wagner, 2006; Dumka, Garza, Roosa, & Stoerzinger, 1997; Perrino, Coatsworth, Briones, Pantin, & Szapocznik, 2001). Those clients who leave treatment early may not receive the active ingredients of a treatment, or the interventions may not have sufficient time to work, resulting in less than optimal intervention outcomes.
It is not surprising that research has shown that some of the mental and behavioral symptoms that are risk factors for subsequent negative outcomes, and are often targeted for intervention, have also been linked to premature termination (Castro et al., 2006). For example, psychiatric symptoms as well as low family cohesion have been found to predict inadequate participation in prevention and treatment.
Predictors of Premature Termination
Perrino et al. (2001) found that for minority families, family disorganization and low family cohesion can negatively affect participation in treatment, ultimately affecting the effectiveness of treatment. In a study of sociodemographic, child, and family-level correlates of retention patterns (i.e., nonattenders, variable attenders, and consistently high attenders) among minority families involved in a preventative intervention, Coatsworth, Duncan, Pantin, and Szapocznik (2006) found that families who experienced premature attrition from treatment had lower levels of family organization.
Empirical findings have been mixed on whether psychiatric symptoms affect treatment retention (Neumann et al., 2010). In psychosocial treatments for externalizing behaviors, higher problem severity has been linked to greater attrition (Galaif, Hser, Grella, & Joshi, 2001; Kapungo et al., 2011). Conversely, lower severity of internalizing behaviors has been related to greater attrition (Flannery-Schroeder, Choudhury, & Kendall, 2005). In a study examining archival medical records for child clients who received outpatient therapeutic services at a community mental health clinic (L. M. Miller, Southam-Gerow, & Allin, 2008), participants with more co-occurring psychiatric disorders attended more sessions. In a universal prevention study conducted in Germany, parents of children with higher levels of behavioral problems were more likely to participate in the intervention (Heinrichs, Bertram, Kuschel, & Hahlweg, 2005). However, in the Drug Abuse Treatment Outcome Study (Simpson et al., 1997) testing three different modalities of drug treatment programs, individuals with heavier drug use and higher levels of psychological dysfunction had lower retention rates. These studies were conducted with very different pediatric populations, and as such, the discrepant findings are likely because of differences in sample characteristics. The role of psychiatric symptoms and behavior problems, and their relationship to attendance in treatment among Latino clients, has not been well established.
Investigating Predictors of Attendance in the Context of Family and Individual Treatments
In addition to the direct influence of family and individual psychiatric characteristics, it is helpful to also investigate the degree to which these variables may interact with different models of intervention. In our study of Latino adolescents, we compared two treatments: (a) Culturally Informed and Flexible Family-Based Treatment for Adolescents (CIFFTA), a family-oriented condition, and (b) an ecologically valid form of individual adolescent treatment designed at a training clinic. Partly because of the added burden of bringing multiple family members in for treatment, many family treatments include specialized engagement and retention strategies that can mitigate the possible negative impact of high symptomatology and family factors (Santisteban, & Szapocznik, 1994; Santisteban et al., 1996). Evidence-based family interventions (e.g., Liddle, 2010) often seek to identify and circumvent the family dynamics that are barriers to attendance, reduce negativity and hopelessness, and mobilize the caring and supportive nature of the family. Individually oriented adolescent treatment does not always concentrate on specialized techniques for keeping entire families in treatment, instead focusing on engaging individual clients and maintaining a one-to-one therapeutic alliance. The analysis of individual and family-level predictors of attrition in the context of individual and family interventions can help inform future treatments.
Although most studies have examined individual variables as predictors of engagement/retention in treatment, we implemented a person-centered approach whereby profiles based on multiple variables were examined as predictors of session attendance. This approach has the advantage of providing an examination of the variables of interest in the context of other important variables rather than examining the effects of these variables in isolation.
The purpose of this study was to identify whether patterns of psychiatric and behavioral symptoms, as well as of family functioning, can negatively affect attendance in a sample of Latino clients, and to investigate whether these factors have a differential impact on attendance in two distinct types of treatment: a family-based CIFFTA treatment and an individual treatment. Specifically, our research objectives were to (a) identify profiles of participants based on psychiatric and behavioral symptoms, as well as family functioning, and (b) determine whether attendance in the two treatment interventions differed across the identified profiles. We hypothesized that families in this study would have elevated psychiatric symptomatology and high levels of conflict, particularly because these correspond to the inclusion criteria for the study. This makes it that much more important that we understand the influence of high conflict or low cohesion on attendance. We believed that CIFFTA would result in higher rates of attendance among participants in this sample because this intervention addresses both the family systems and cultural factors that may be unique to the life experiences of these families. This study has potential implications for better understanding Latino clients and their families and identifying client profiles that may be associated with differential attendance in family-based versus individual treatment.
Method
Participants
This study was part of a randomized clinical trial testing the efficacy of a family-based treatment in reducing adolescent behavior problems, psychiatric symptoms, and family conflict among Latino adolescents (Santisteban, Mena, McCabe, et al., 2015). The present article is the first to examine factors that influence treatment attendance. Data were collected from 200 Latino adolescents and their families. To be included in the study, adolescent participants had to be between 11 and 14 years old, meet criteria for “likely” diagnoses on two or more behavior problems (including ADHD, conduct disorder, depressive disorder) on a diagnostic screening measure (DISC Predictive Scales; Lucas et al., 2001) and/or family conflict, and have at least one parent willing to participate. Participants were referred to treatment by school counselors and community treatment agencies. This study was reviewed and approved by the university institutional review board.
Demographic characteristics are described in Table 1. Adolescents were about 12.5 years old, on average, and had lived in the United States for approximately 10 years. Approximately 65% of the adolescents were born in the United States. Another 11% were born in Cuba, and the remaining 24% were born in Honduras, Nicaragua, Venezuela, Puerto Rico, Colombia, Mexico, Peru, Uruguay, El Salvador, Panama, Argentina, Dominican Republic, Costa Rica, or Ecuador. About 40% of the adolescents in the sample were female. Approximately 70% of the adolescents preferred English, and the remaining preferred Spanish. The language of preference was used to determine the language used for all assessments.
Demographic Characteristics of Adolescents and Parents
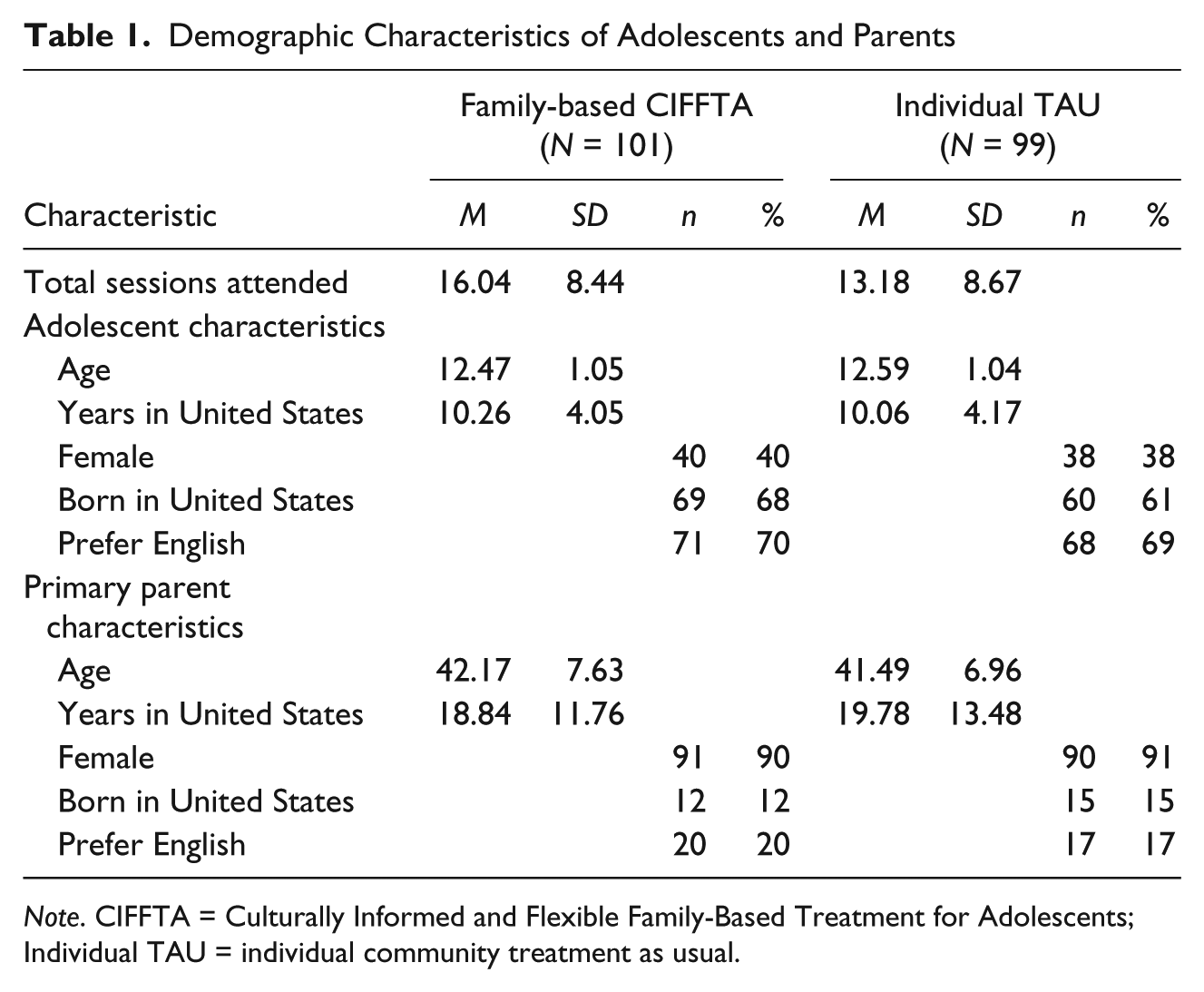
Note. CIFFTA = Culturally Informed and Flexible Family-Based Treatment for Adolescents; Individual TAU = individual community treatment as usual.
The primary parents (90% of the time it was the adolescent’s mother) were Cuban (27%), Nicaraguan (15%), or U.S.-born (14%); with fewer than 10% each from Honduras, Colombia, or Venezuela; and fewer than 5% each from Peru, Ecuador, Mexico, Puerto Rico, Guatemala, El Salvador, Argentina, Uruguay, Costa Rica, Panama, Chile, or Brazil. About 80% of the parents completed the assessments in Spanish, their preferred language. It should be noted that although fathers and other family members were often included in family sessions, the mothers typically completed the assessments.
Procedure
Figure 1 displays the number of participants who were screened, enrolled, randomized, and received the intervention. Families who were interested in participating had the research study explained to them and were asked to sign an informed consent. A total of 283 participants were screened. All participants who met screening criteria were scheduled for a baseline assessment. Once enrolled in the study, participants and their parents completed the baseline assessment interview (N = 200). Measures were administered in either English or Spanish based on participant preference and were collected separately for adolescents and parents. The assessment interview lasted approximately 2 to 2.5 hours.
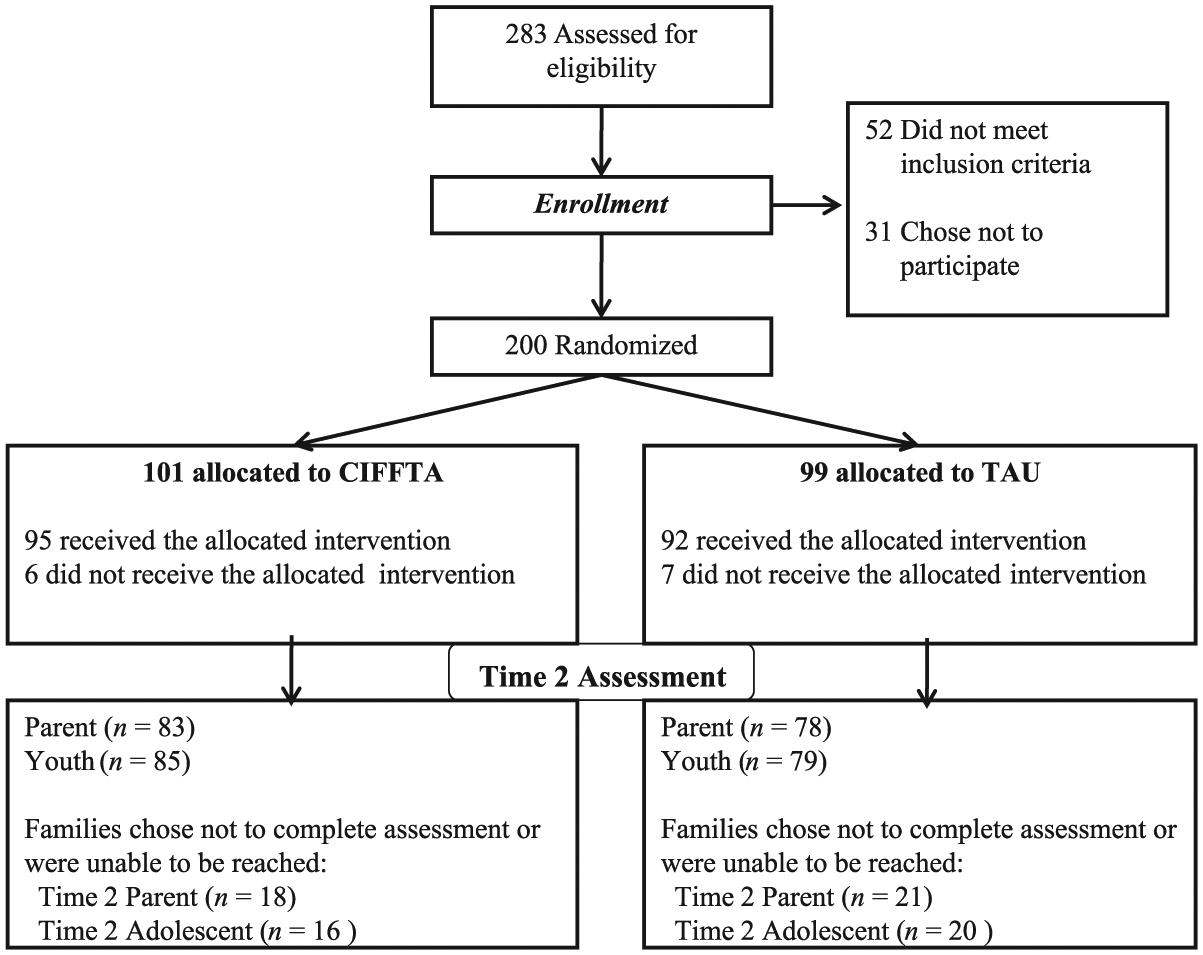
CONSORT table. CIFFTA = Culturally Informed and Flexible Family-Based Treatment for Adolescents; TAU = treatment as usual.
Intervention Conditions
Following the assessment, participants were randomized into one of two treatment conditions: CIFFTA or individual community treatment as usual (ITAU). Both conditions were provided in a university clinic setting.
CIFFTA
CIFFTA is a multicomponent, adaptive, family-based treatment that addresses culturally relevant content (e.g., immigration and acculturation stressors), core family processes, and co-occurring adolescent disorders. CIFFTA consisted of a combination of family therapy interventions (e.g., engagement, parenting practices, improved parent–adolescent attachment), individual therapy interventions (e.g., motivational interviewing; W. R. Miller & Rollnick, 2002), and psychoeducational modules (e.g., acculturation, immigration-related parent-child separations, parenting practices, drug education, co-occurring psychiatric disorders, risky sexual behavior). CIFFTA is designed to address adolescent psychiatric symptoms and family conflict, which are risk factors for problem behaviors later in life including risky sexual behaviors and substance abuse. As an adaptive intervention, CIFFTA tailors the specific content to the family’s unique clinical or cultural characteristics at baseline. The initial phase of treatment focused on engagement, a critical component of the CIFFTA model.
In CIFFTA, three sessions were offered every 2 weeks, allowing for all three components (individual, family, and modules) to be provided every 2 weeks. A total of 101 participants were randomized to this condition, 95 of whom initiated treatment. The treatment was implemented over a 4-month period and was designed to deliver approximately 24 sessions per family. Throughout the duration of the trial, weekly clinical meetings were held for the therapists to provide formal supervision to all project team members. The intervention was delivered by six bilingual therapists: two doctorate prepared and four master’s prepared therapists with degrees in counseling, psychology, social work, or a related field. Therapists received a 3-day training workshop where they were oriented to the use of didactic material and treatment manuals, and observed videotaped sessions.
To encourage retention of families in treatment, CIFFTA therapists served as the primary contact for the families. They were responsible for scheduling sessions and maintaining engagement by reaching out to families who missed appointments and/or dedicating a session to reengaging the family if needed to ensure that family members’ needs were being met throughout the treatment. Treatment fidelity was evaluated using a treatment adherence manual and checklist developed specifically for the study. Randomly selected videotaped sessions were viewed and scored by at least one rater using the adherence manual and checklist. Interrater reliability and drift were measured by examining correlations between raters during initial training to assess interrater reliability and periodically throughout to assess drift. Overall, ratings demonstrated that therapists adhered to the model. Additional information on the evaluation of treatment fidelity is provided elsewhere (Santisteban, Mena, McCabe, et al., 2015).
ITAU
ITAU was designed to reflect the individually oriented services that youth with behavior problems typically receive in the community. This treatment was delivered by six bilingual therapists: one doctorate prepared and five master’s prepared. ITAU therapists were provided with a manual developed by the study team in conjunction with a university training clinic that delineated individually oriented services appropriate for the study population; these focused on ADHD, depression, and anxiety symptoms. The individual sessions with the adolescent were focused on alleviating symptoms associated with primary disorders identified at the intake assessment, depression, ADHD, conduct disorder, and/or high family conflict. Examples of treatments used by ITAU therapists included cognitive behavior therapy, interpersonal psychotherapy, social skills training, anger control training, problem solving skills, and assertiveness training. Approximately one time per month the therapist met with the parents of the adolescent to update them on the youth’s progress and to allow the parents an opportunity to voice any concerns they had regarding the youth. As with the CIFFTA condition, ITAU therapists served as the primary contact for the families and were responsible for scheduling sessions and maintaining engagement by reaching out to families who missed appointments. ITAU therapists were expected to hold three sessions every 2 weeks for an approximate total of 24 sessions. In all, 99 cases were randomized to ITAU, with 92 of those cases initiating treatment. As in the CIFFTA condition, ITAU therapists also received weekly supervision.
Measures
Attendance
Session attendance for both CIFFTA and ITAU was documented over the treatment phase, and the total number of sessions (including individual, family, and psychoeducational modules) was used as the outcome in this study. Sessions were approximately 1 hr in length (M = 61.29, SD = 11.45 min in CIFFTA and M = 72.41, SD = 21.65 min in ITAU). If participants arrived late to an appointment, therapists tried to accommodate them and their families and the session was counted for attendance purposes. However, if the therapist was unable to accommodate them, the appointment was rescheduled. If participants and/or families attended the rescheduled appointment, then their attendance was counted.
Baseline measures of family functioning and adolescent psychiatric symptoms were examined as predictors of attendance. These measures have been used with similar populations of Latino youth and families and have demonstrated evidence of reliability and validity in both English and Spanish. Many of the measures were originally designed for use with Latino populations, or Spanish translations were developed by the publishers. Raw scores on each of the predictors were converted into T-scores for the analysis to ease interpretation of profiles and facilitate comparisons. T-scores have a mean of 50 and a standard deviation of 10.
Family functioning
Family conflict and cohesion were assessed using the Family Environment Scale (FES; Moos & Moos, 1986), which includes 18 items presented in the form of a statement. Nine statements address family conflict and include statements such as “We fight a lot in our family” and “Family members often criticize each other.” The remaining nine statements address family cohesion and include statements such as “Family members really help and support one another” and “There is a feeling of togetherness in our family.” Participants rate each statement as either true or false. The number of items endorsed positively is summed to create scores on Conflict (α = .67 and .76 for parent and adolescent reports, respectively) and Cohesion (α = .76 and .75 for parent and adolescent reports, respectively) subscales.
Psychiatric symptoms/behavior problems
Both adolescents and parents reported on adolescent psychiatric symptoms/behavior problems. Parents reported using the Child Behavior Checklist for Ages 6 to 18 (CBCL; Achenbach & Rescorla, 2001). This measure has 112 symptoms listed in alphabetical order for which parents select one of three options: not true (as far as you know), somewhat or sometimes true, or very true or often true. In an effort to reduce participant burden, the subscales administered to parents were Aggressive Behavior, Rule-Breaking, Attention Problems, Social Problems, Anxiety/Depression, and Withdrawn/Depressed. Items from Anxiety/Depression and Withdrawn/Depressed were grouped into the Internalizing subscale (α = .87) and items from Aggressive Behavior, Rule-Breaking, Attention Problems, and Social Problems were grouped into the Externalizing subscale (α = .90).
Adolescents reported their clinical symptoms using the Youth Self-Report for ages 11 to 18 (YSR; Achenbach & Rescorla, 2001). Like the CBCL, the YSR includes 112 statements that the adolescents endorse using a similar 3-point rating scale: not true, somewhat or sometimes true, or very true or often true. As indicated above, a subset of items was used to create Internalizing (α = .90) and Externalizing (α = .90) subscales.
Acculturation
The Bidimensional Acculturation Scale for Hispanics (BAS; Marin & Gamba, 1996) consists of 24 items (12 for each cultural domain, Hispanic and non-Hispanic). The BAS provides two scores: one for the Spanish domain (Hispanicism) and one for the non-Spanish domain (Americanism), thus providing a measure of biculturalism. This scale has been tested among Latinos with high internal consistency for both the Hispanicism (α = .90) and Americanism (α = .96; Marin & Gamba, 1996) domains. Internal consistency reliabilities for each of the subscales were .88 on the Hispanicism scale and .97 on the Americanism scale for parents, and .91 for both Americanism and Hispanicism for the youth in this sample.
Analysis
Latent profile analysis was conducted using Mplus 7.11 (L. K. Muthén & Muthén, 2013) to examine whether different conceptually meaningful profiles of families emerged based on levels of family functioning and adolescent psychiatric symptoms. We then tested whether the resulting profiles had differential rates of attendance between the two treatment groups using finite mixture regression models (Grun & Leisch, 2008). Latent profile analysis is a useful analytic technique in family research because, unlike with traditional methods, researchers can describe meaningful subgroups of families and link these subgroups to developmental trajectories, risk, and intervention (Collins & Lanza, 2009; Henry, Tolan, & Gorman-Smith, 2005; B. O. Muthén, 2001, 2002). Fundamentally, latent profile analysis involves grouping cases based on their similarities on a single or multiple dimensions and generating groups that maximize similarity within the group and minimize similarity between groups. This technique builds on previous empirical work and is a good match for the purpose of this study, which was to isolate distinct configurations (i.e., subgroups) of psychiatric symptoms and family interactions and to examine whether subgroups were linked to attendance in the intervention (CIFFTA) and/or control (ITAU) conditions.
Three distinct steps were used in this study. First, latent profiles were created based on measures of family functioning and psychiatric symptoms. This involved determining how many profiles were appropriate; this was an iterative process whereby fit for models with fewer profiles was compared to fit for models with more profiles using the Vuong–Lo–Mendell–Rubin test (VLMR; Lo, Mendell, & Rubin, 2001). The VLMR test compares the fit of two nested models that differ by one profile. When the p value for the VLMR test is significant, the complex model fits significantly better than the simpler, more parsimonious model. A nonsignificant p value indicates that the model fit is not significantly different and therefore the more parsimonious model is preferred. Akaike information criterion (AIC), Bayesian information criterion (BIC), and entropy were also evaluated. Lower AIC and BIC values are preferred, whereas entropy values near 1 indicate better classification of people into profiles. Because model fit statistics may be inconclusive, profiles also had to be meaningful and consist of more than a few families to be retained. In the second step, the latent profiles were also used to test whether demographic and cultural characteristics differed by profile. Specifically, we tested whether the profiles differed by proportion of female adolescents, age, years living in the United States, and adolescent and parent levels of acculturation. Finally, the profiles were used to predict whether the total numbers of sessions for each profile were significantly different in the two intervention conditions. That is, we tested whether latent profile membership predicted differences in attendance for participants in CIFFTA and ITAU using finite mixture regression models.
Results
Latent Profile Analysis
Parent and adolescent reports of family conflict and cohesion and adolescent internalizing and externalizing symptoms generated three profiles of families. Models with one, two, three, four, and five profiles were compared and model fit comparisons are shown in Table 2. The model with three profiles was retained. Table 3 displays the mean T-scores and standard deviations for the three profiles. The first (Profile 1) consisted of 38 (19%) families in which parents and adolescent reported discrepant levels of family conflict and externalizing and internalizing symptoms. Specifically, the parents reported elevated symptoms compared to the adolescents. The second (Profile 2) consisted of 115 families (57%) in which parents reported typical family functioning and high adolescent psychiatric symptoms, and adolescents reported typical family and psychiatric functioning. The third (Profile 3) consisted of 47 families (24%) with poor cohesion and high psychiatric symptoms based on both parent and adolescent reports.
Model Fit Indices for One- to Four-Profile Solutions
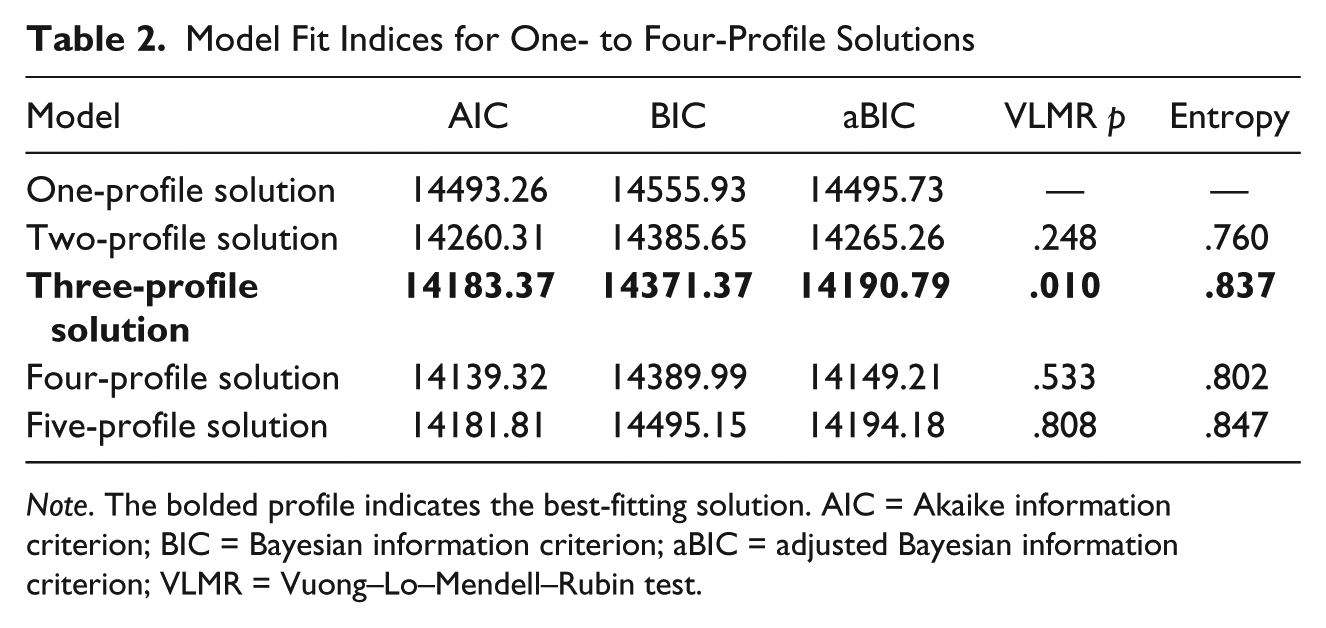
Note. The bolded profile indicates the best-fitting solution. AIC = Akaike information criterion; BIC = Bayesian information criterion; aBIC = adjusted Bayesian information criterion; VLMR = Vuong–Lo–Mendell–Rubin test.
Mean and Standard Deviations by Profile
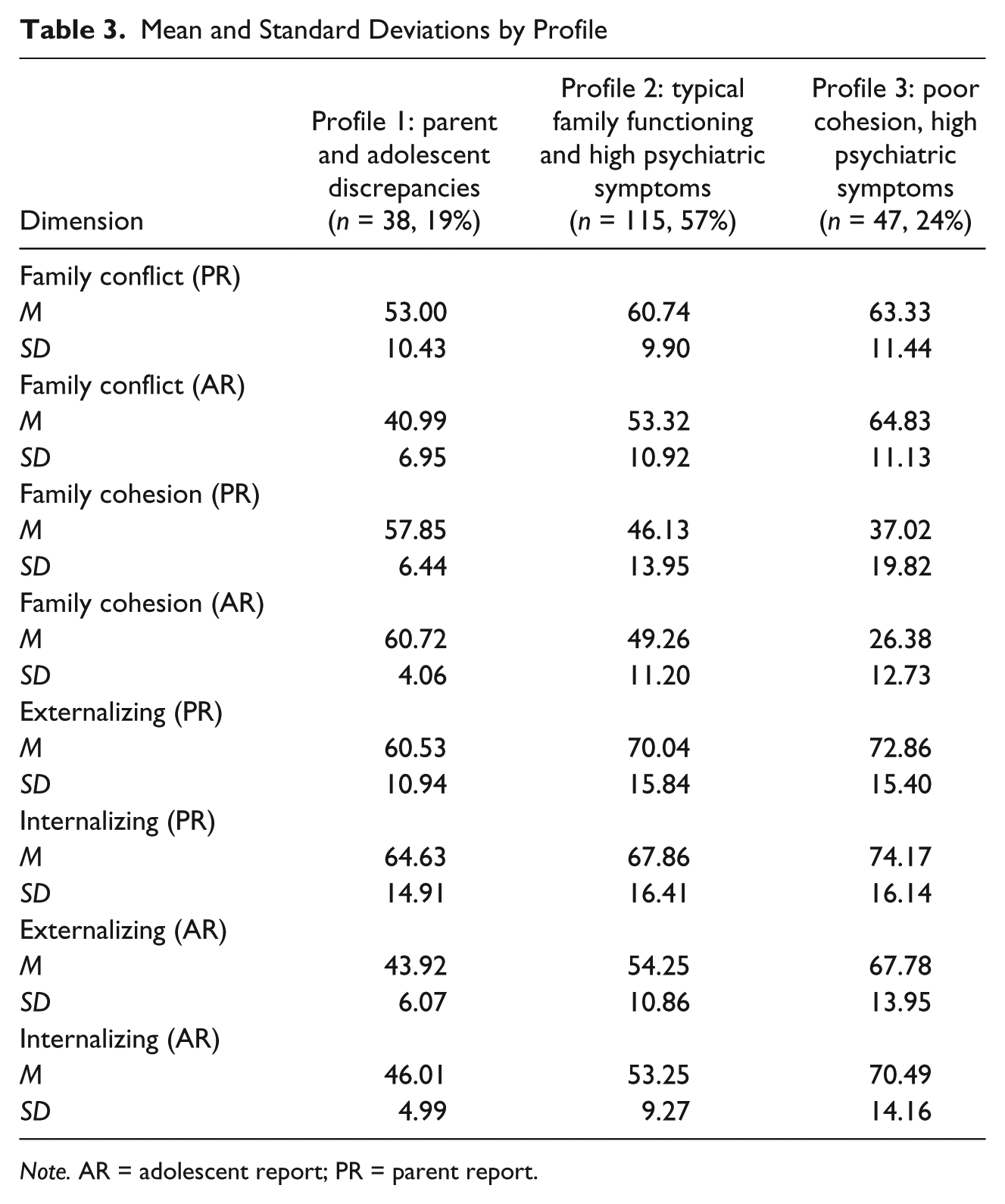
Note. AR = adolescent report; PR = parent report.
An examination of the demographic characteristics by profile revealed that families did not differ by adolescent age, F(2, 197) = 2.48, p = .086, η2 = .02, or by parent’s level of acculturation based on levels of Hispanicism, F(2, 197) = 1.29, p = .277, η2 = .01, or Americanism, F(2, 197) = 1.08, p = .342, η2 = .01. Profiles were different on adolescents’ level of Hispanicism, F(2, 197) = 5.53, p = .005, η2 = .05; Profile 3, the poor cohesion, high psychiatric symptom group, consisted of adolescents endorsing Latino cultural values to a lesser degree than adolescents in the parent and adolescent discrepancy group or the typical family functioning and elevated parent report of psychiatric symptom group. Moreover, profiles differed on adolescents’ level of Americanism, F(2, 197) = 3.88, p = .022, η2 = .04, with Profile 3 consisting of adolescents endorsing American cultural values to a greater degree than adolescents in the parent and adolescent discrepancy group. This finding was supported by differences in years living in United States, F(2, 197) = 3.85, p = .023, η2 = .04, with the poor cohesion, high psychiatric symptom group consisting of adolescents living in the United States longer than adolescents in the parent and adolescent discrepancy group.
Predictors of Attendance
Finite mixture regression was used to predict attendance based on treatment type (CIFFTA or ITAU) separately for each profile defined previously. Specifically, we tested whether families in the various profiles attended the same number of sessions when assigned to the ITAU or family-based CIFFTA conditions. Session attendance was generally high for both conditions with participants in ITAU attending an average of 13 sessions and participants in CIFFTA attending an average of 16 sessions (Santisteban et al., 2014). Results of the analysis are presented in Table 4. For each profile, the intercept represents the expected attendance for ITAU families and the slope represents the expected change in attendance for CIFFTA families as compared to ITAU families.
Finite Mixture Regression Results
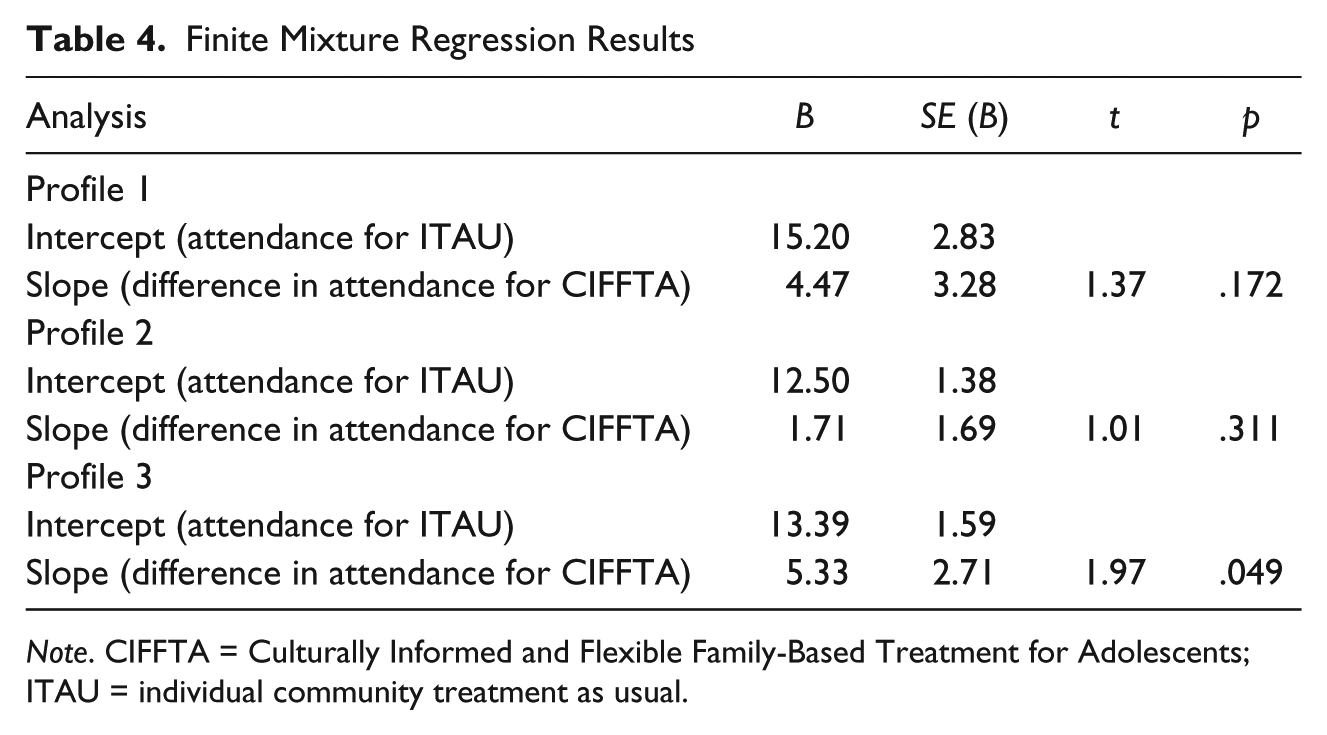
Note. CIFFTA = Culturally Informed and Flexible Family-Based Treatment for Adolescents; ITAU = individual community treatment as usual.
Among the profile of families where parents and adolescent reported discrepant levels of family conflict and externalizing and internalizing symptoms (Profile 1), the mean number of sessions attended in ITAU was 15.20 and in CIFFTA was 19.67 sessions. This difference was not statistically significant (B = 4.47, SE = 3.28, t = 1.37, p = .172). However, this effect is considered moderate (Cohen’s d = 0.55). Among the profile of families where parents reported typical family functioning and high adolescent psychiatric symptoms and adolescents reported typical family and psychiatric functioning (Profile 2), the mean number of sessions attended in ITAU was 12.50 as compared to 14.21 sessions in families randomized to CIFFTA. This difference was not statistically significant (B = 1.71, SE = 1.69, t = 1.01, p = .311) and corresponds to a small effect (Cohen’s d = 0.21). Last, in Profile 3, characterized by families with poor cohesion and high psychiatric symptoms based on both parent and adolescent reports, the mean number of sessions attended in ITAU was 13.39 as compared to 18.72 sessions for families randomized to CIFFTA. This difference was statistically significant (B = 5.33, SE = 2.71, t = 1.97, p = .049) and corresponds to a moderate effect (Cohen’s d = 0.66).
Discussion
This study is, to our knowledge, one of the first to use a person-centered rather than variable-centered approach when examining family and adolescent psychiatric factors that predict attendance in a prevention intervention for Latino adolescents. Our latent profile analysis identified three profiles of family subtypes based on parent and adolescent reports of adolescent psychiatric and family functioning variables; we subsequently tested whether members of these subtypes had differential attendance in family-based or individual treatment. The first profile consisted of families where parents and adolescents reported discrepancies on psychiatric symptoms and family conflict. The second profile consisted of families with elevated adolescent psychiatric symptoms but no family conflict. In these two profiles, attendance did not differ significantly based on whether families were randomized to a family-based treatment compared to individual treatment. Finally, the third profile consisted of families with low family cohesion and high levels of adolescent psychiatric symptoms. For this third profile, attendance in family-based treatment was significantly higher than in individual treatment.
A person-centered approach provides a more realistic test of variables by investigating them in the context of other important variables rather than in an isolated fashion. It is interesting that this difference in the method of categorizing families makes it slightly more difficult to compare our person-centered findings with previous findings that examined psychiatric and family variables in isolation. Although much is known about the importance of attendance to treatment outcomes, less is known about how clinical and family characteristics can predict attendance, particularly among Latinos. By delimiting the study to Latino families, we focused more fully on this understudied population and the possible role of acculturation. The findings of this study should have relevance to the work of counseling psychologists and therapists treating Latino clients and their families.
Profiles of Families Emerging From the Analyses
We retained three profiles based on measures of family conflict, cohesion, and measures of adolescent psychiatric symptoms. The profile that included the most families (57%) was Profile 2, in which parents reported typical family functioning and high adolescent psychiatric symptoms, whereas the adolescents reported typical family and psychiatric functioning. This family profile is one in which parents seek services for their adolescent’s behavior problems and do not report that the adolescent’s problems have affected the family in a negative way, whereas the adolescents do not report significant issues. This group of families had the lowest overall number of counseling sessions and there was no significant difference between the family and individual treatment conditions. This finding was not particularly surprising given that family functioning in this profile did not appear to be affected by the adolescent’s psychiatric symptoms. In other words, both family-based and individual treatment appeared to be equally appealing to families who did not experience problematic family functioning. It should also be noted that although some of the research in the field suggests that high externalizing symptoms might lead to fewer sessions whereas high internalizing might lead to higher numbers of sessions (Flannery-Schroeder et al., 2005; Galaif et al., 2001; Kapungo et al., 2011), within each of our profiles, internalizing and externalizing symptoms tended to move together, leading to families being categorized as showing either high or low adolescent psychiatric symptoms.
The second most common profile of families (24%) was Profile 3 in which the adolescent and parents reported low family cohesion and high adolescent symptoms. Based on previous research showing that among minority families low family cohesion has been shown to negatively affect treatment participation (Perrino et al., 2001), one might have expected fewer sessions in both conditions. On the other hand, if the family model was well equipped to address this lack of family cohesion, it might effectively retain the families. Many evidence-based family therapies, including CIFFTA, emphasize that to work with families with high levels of conflict or low cohesion, one must have advanced training in reestablishing emotional connections within the family and handling negativity and blaming. Making this profile of families even more interesting was the fact that the adolescent endorsed behavioral items on an acculturation scale that suggested a more “assimilated” life (i.e., feeling more comfortable in a U.S. American than in a Latino context). The finding that Latino families containing highly assimilated adolescents reported lower family cohesion is consistent with the findings on intrafamilial parent–adolescent acculturation gaps or discrepancies (Cervantes et al., 2012; Martinez, 2006; Santisteban et al., 2013). The finding that families in the CIFFTA condition had significantly more counseling sessions than those in the individual condition may reflect that it is capable of addressing both low family cohesion and acculturation-related issues within the family. Indeed, part of CIFFTA’s innovation was to create family therapy interventions that address both family- and culture-related processes through psychoeducational modules such as the “acculturation module” and the “parenting module” (which includes culture-related content; Santisteban et al., 2013). It would also make sense that in individually focused treatment, the therapist may not be able to identify or work directly on these gaps in acculturation and their negative effects on the family.
The fewest families were classified in Profile 1 (19%), which was characterized by very discrepant views regarding the adolescent’s symptoms and family symptoms. Parents and adolescents disagreed in their reports, with parents endorsing high severity of problems and adolescents reporting low severity. In theory, this lack of agreement would lead to very fruitful discussions in family counseling sessions, trying to reach consensus on what is occurring in the family prior to bringing about change. This family profile had the most overall number of sessions. Although the difference between family and individual conditions was not statistically significant, given that the effect size suggested that the mean difference between the two treatment conditions was moderate in size, future research should consider including larger samples to address any potential concerns with adequate statistical power to detect a significant effect.
These findings suggest that, in working with Latino families, it may be quite helpful to consider how high conflict and low cohesion affect the family and how culture-related experiences may affect conflict and cohesion. It is a key assumption of the CIFFTA treatment that therapists must be prepared to identify and address the unique culture-related stressors that Latino families bring into therapy. In both the individual and the family conditions, therapists were sensitive to how unique cultural experiences of the families contribute to their symptom profiles. The uniqueness of CIFFTA, however, is that these cultural elements are brought directly into the content of therapy with specific modules that address these cultural factors such as immigration, acculturation, and discrimination-related stress.
Limitations and Future Research
It is important to recognize the limitations of this study. First, a larger total sample size would have resulted in larger profile sizes, providing greater power to detect differences between profiles as well as the potential to yield more distinct profiles. It is possible that with a larger number of families in each profile the differences in Profile 3 may have been statistically significant. In addition, the latent profiles were defined solely on family conflict and cohesion and adolescent internalizing and externalizing symptoms. It is possible that the addition of other family functioning variables (e.g., parenting, attachment, familism, stress) may have resulted in different subsets of families. We do believe that one of the strengths of this study is that it included child and parent reporters rather than having findings solely based on parent reports. By using a person-centered approach, this study may have identified a clinically important type of family that is characterized by a substantial discrepancy between parent and child perceptions of problems. Perhaps most important in terms of limitations, our findings concerning attendance do not inform us about the efficacy of the interventions. Future research should consider how differential attendance between these interventions could be linked to a range of therapeutic outcomes.
Implications for Practice
It is helpful for clinicians to know at the onset of treatment that certain family characteristics can affect attendance and that an adaptive treatment such as CIFFTA may be able to target these characteristics with specialized family-focused and culturally informed interventions. By seeking to identify the family processes behind certain types of intense conflicts (e.g., acculturation-related conflicts between parents and adolescents, parent age-appropriate monitoring of peers), an intervention can be much more targeted to the unique family circumstances. The family therapist may be able to work early in therapy to improve family organization and cohesion overall or may try to short-circuit the manner in which those family factors negatively affect attendance. These findings can ultimately be used to inform therapists’ practices with Latino clients and families experiencing psychiatric and/or behavior problems as well as problematic family functioning.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Support for this research was received from the National Institute on Drug Abuse Grant R01 DA027920 and R25 DA026401 and by Center of Excellence for Health Disparities Research: El Centro, National Center on Minority Health and Health Disparities Grant P60MD002266. Its contents are solely the responsibility of the authors and do not necessarily represent the official views of the National Institutes of Health.