
Abstract
This study evaluated rates of psychiatric symptoms and mental health treatment utilization among National Guard service members during postdeployment. National Guard service members (N = 311) completed surveys assessing demographics, beliefs about mental health treatment, emotion regulation strategies, and psychiatric symptoms. Mental health treatment utilization was assessed at the 6-months follow-up. Postdeployment, 41.2% of the sample had psychiatric symptoms above the clinical cut-off for at least one symptom measure. This proportion increased at follow-up (53.5%). Alcohol use disorder (AUD) symptoms showed the largest increase (d = 0.66), although symptoms of depression and post-traumatic stress disorder (PTSD) also showed small magnitude increases. Among those with elevated symptoms postdeployment (n = 128), only 27.8% received mental health treatment at follow-up. Severity of depression, anxiety, and PTSD were higher among those who utilized treatment. The postdeployment period is a vulnerable one. Continued efforts to understand and address barriers to treatment for this population are warranted.
Keywords
The postdeployment period is a vulnerable one for National Guard service members. The combination of high rates of clinically elevated symptoms, increasing symptoms during the postdeployment period, and low utilization of mental health treatment in this population highlights opportunities for advocacy, prevention, and treatment delivery innovation.Significance of the Scholarship to the Public
High rates of psychiatric symptoms and low rates of mental health treatment utilization among United States military service members involved in Operation Enduring Freedom (OEF) and Operation Iraqi Freedom (OIF) have been documented for over a decade (Hoge, Auchterlonie, & Milliken, 2006, Hoge, Auchterlonie, & Milliken, 2006). In particular, military service members and veterans commonly endorse symptoms of depression, anxiety, post-traumatic stress disorder (PTSD), and alcohol use disorder (AUD; Seal, 2007, 2011). However, substantial variability has been reported in these estimates. Although the postdeployment period has been identified as a time of vulnerability (Sayer et al., 2010), rates of postdeployment mental health concerns among OEF and OIF service members and veterans have ranged widely. One of the earliest studies, conducted by Milliken (2007) based on a large cohort of returning OEF and OIF soldiers (N = 88,235), reported that 20.3% of active duty military (i.e., full time soldiers) and 42.4% of reservists (e.g., National Guard soldiers) showed elevated psychiatric symptoms reflecting a need for mental health care during the postdeployment period. Although they used a large population-based sample, the assessments were very limited in scope (e.g., two-item depression measure and four-item PTSD measure). Thomas et al. (2010) also assessed a large sample of returning service members (N = 18,305), with estimated rates of depression and PTSD ranging from 18.7% to 33.2%. In contrast, Interian et al. (2012) found that only 11% of returning National Guard soldiers scored positive for PTSD symptoms.
Estimates of postdeployment mental health treatment utilization have also varied considerably. Hoge et al. (2004) found that among returning Army and Marine soldiers who met criteria for major depression, generalized anxiety, or PTSD, between 13% and 21% received help from a mental health professional in the past year. These low rates of utilization differ markedly from Elbogen et al. (2013), who found that 69% of randomly sampled OEF and OIF veterans received psychiatric treatment (i.e., medications or psychotherapy) in the past year.
There are a variety of methodological features that may account for the variability in estimates of mental health concerns and treatment utilization. These include how cases are defined (e.g., symptom cut-offs and measures) and military subpopulations sampled (e.g., active component vs. reservist), among other factors (e.g., sample demographics; Kok, Herrell, Thomas, & Hoge, 2012; Thomas et al., 2010). Further, it is entirely plausible that estimates are accurately dynamic, and may change in response to a variety of cohort-related variables, such as the amount and type of combat exposure (Fulton et al., 2015). This highlights the need for ongoing research examining symptoms and treatment utilization that may provide more population-specific (e.g., focused on a particular subpopulation of service members) and cohort-specific (e.g., more recently returning soldiers) estimates that can inform policy and outreach efforts targeted toward specific groups of service members.
Studies investigating psychiatric symptoms and treatment utilization have often used cross-sectional designs (Elbogen et al., 2013; Interian et al., 2012; Kulesza et al., 2015). Although cross-sectional designs may facilitate larger sample sizes, longitudinal designs are ideal for studying the development of symptoms postdeployment and investigating longitudinal predictors of treatment utilization. In particular, longitudinal designs allow the assessment of changes in symptoms over time (e.g., immediately postdeployment and in the subsequent postdeployment period). A richer understanding of the trajectory of symptom change during the postdeployment period can directly inform intervention and outreach efforts (e.g., highlighting the need for outreach 6 months following deployment if symptoms increase during this period). Further, longitudinal models allow evaluation of the factors that predict treatment utilization during the postdeployment period. Such analyses have the potential to clarify factors that may be associated with health disparities (e.g., demographic variables such as gender, race and/or ethnicity that differentially predict treatment utilization; Wang et al., 2005). These models can also enrich our understanding of what may motivate individuals to utilize treatment (e.g., the presence of elevated symptoms), which can likewise inform efforts to reduce barriers to care (e.g., screening in primary care settings; Cornwell et al., 2018).
Variability in the specific estimates aside, the high rates of psychiatric symptoms paired with the potentially low rates of treatment utilization represents a treatment gap (Kohn et al., 2004), given the availability of evidence-based treatments to address mental health concerns common among returning military service members (e.g., depression, PTSD, and AUD; Elbogen et al., 2013; Thomas et al., 2010). This gap is particularly notable within military and veteran populations due to the availability of mental health treatment through military and Veterans Health Administration (VHA) providers and outreach efforts by VHA and other veteran service organizations (National Academies of Sciences, Engineering, and Medicine, 2018; Straits-Tröster et al., 2011).
It is particularly vital that research clarify factors that predict mental health treatment utilization in order to better target utilization efforts and reduce the treatment gap among returning OEF and OIF service members and veterans. Prior research has highlighted a variety of factors that predict postdeployment treatment utilization in these populations, including screening positive for mental health problems (Kehle et al., 2010), psychiatric symptom severity (Meis et al., 2010), readjustment stressors (Interian et al., 2012), race and/or ethnicity (Zinzow et al., 2015), stigma and career-related worries associated with receiving treatment (Stecker, Fortney, Hamilton, Sherbourne, & Ajzen, 2010), and beliefs about treatment (Fox et al., 2015; Kehle et al., 2010; Pietrzak et al., 2009). However, as with prevalence and treatment utilization estimates, the precise characteristics that do or do not predict utilization have varied across studies. For example, symptom severity has proven an inconsistent predictor of treatment utilization. Kulesza et al. (2015) found that anxiety and PTSD symptoms positively correlated with treatment utilization in a cross-sectional sample of young adult veterans. However, Interian et al. (2012) found that depression symptom severity, but not PTSD symptom severity, positively correlated with the likelihood for postdeployment mental health treatment in a cross-sectional sample of National Guard soldiers. Zinzow et al. (2015), on the other hand, found that depression, PTSD, and alcohol problems did not predict utilization in a cross-sectional sample of active-duty soldiers with sexual assault histories. Beliefs about mental health treatment are also inconsistent predictors of treatment utilization. Key beliefs assessed in prior research focus on the likelihood of benefit (e.g., “mental health treatment generally does not work”; Vogt et al., 2014). Although some cross-sectional studies have found a positive association between positive beliefs and treatment utilization (Kehle et al., 2010) or a negative association between negative beliefs and treatment utilization (Pietrzak et al., 2009), other studies have failed to find a relationship (e.g., for female OEF and OIF veterans; Fox et al., 2015). These inconsistencies highlight the need for additional research clarifying predictors of utilization. In particular, longitudinal studies using robust symptom measures assessing disorders most relevant for veterans, that are focused on particular military subpopulations (e.g., National Guard service members), may be valuable for understanding the postdeployment experiences of specific groups of veterans.
A further limitation of the existing literature has been the omission of constructs drawn from basic psychological science and social psychology that may prove to be important predictors of utilization. Emotion regulation strategies may be particularly relevant, given that these strategies could influence how an individual responds to and processes adverse experiences that could occur during combat. Gross and John (2003) identified two primary emotion regulation strategies, cognitive reappraisal (i.e., viewing an emotionally evocative situation in a way that influences its impact) and expressive suppression (i.e., inhibiting emotional expression). These constructs have direct relevance to military populations. Cognitive reappraisal strategies are foundational to many efficacious psychotherapies offered to veterans (e.g., cognitive therapy) and endorsement of emotional suppression values (e.g., emotional “toughness”) has been linked to elevated PTSD and depression symptoms among OEF and OIF veterans (Jakupcak et al., 2014). Use of these strategies have important psychological, physiological, and interpersonal consequences in the general population (Gross & John, 2003) and have been shown to predict amygdala activation in combat-exposed veterans (Fitzgerald et al., 2017). The link to amygdala activation is consequential, given the central role of the amygdala in the neurobiological underpinnings of PTSD symptoms (e.g., hyperresponsivity during the processing of both trauma-related and trauma-unrelated affective information; Shin et al., 2006). It may be that the use of certain strategies (e.g., emotional suppression) leads to a decreased willingness to utilize mental health care. To our knowledge, the potential link between emotion regulation strategies and treatment utilization has not been previously explored but may represent a psychological tendency that promotes or inhibits treatment receipt.
National Guard service members represent a military subpopulation that face unique challenges as reserve component members returning from deployment (e.g., feeling isolated from the military community, balancing demands of civilian employment and military service, financial hardship; Gorman et al., 2011; Riviere et al., 2011). In 2010, there were 362,015 Army National Guard service members, 26% of whom were racial and/or ethnic minorities and 14% of whom were female (U.S. Army, 2010). In recent estimates, National Guard service members showed the highest rates of death by suicide across all branches of the military (Department of Defense Suicide Event Report, 2016). Past research suggests that National Guard service members may be at increased risk for mental health problems relative to their active component peers postdeployment (Milliken et al., 2007; Thomas et al., 2010).
The current study sought to add to the literature on postdeployment mental health concerns and mental health treatment utilization among National Guard service members. Using a longitudinal design, we investigated changes in symptoms across several of the most common psychiatric conditions within military and veteran populations (i.e., depression, anxiety, AUD, and PTSD; Seal et al., 2007, 2011) assessed immediately postdeployment and 6 months later. In addition to assessing factors shown to predict treatment utilization in prior studies (i.e., demographic variables, psychiatric symptoms, treatment beliefs), we also assessed service members’ use of emotion regulation strategies.
Method
University of Wisconsin–Madison Institutional Review Boards approved study procedures.
Participants and Procedure
Data were collected as part of a larger study of mental health and social functioning among Wisconsin Army National Guard service members who were deployed to combat theaters during 2008 to 2010. The original study included three assessment points: before deployment (predeployment), immediately after return from deployment (postdeployment), and 6 months after deployment (follow-up). At each time point, participants were recruited for voluntary survey participation during pre- and post-mobilization training events held at the Army installation. Participants could complete the survey anonymously or could provide identifiers that would allow their data to be linked across time points. Due to differences in matched sample sizes across time points and based on previous literature identifying the post-deployment period as one of potential vulnerability as well as an opportunity for intervention or prevention, the present analysis examines postdeployment and follow-up data exclusively. All participants who had available symptom measures at postdeployment and treatment utilization data at follow-up were included.
Among the primary analytic sample (n = 311), the average age was 29.00 years (SD = 8.08). The majority identified as male (82.9%) with the remainder (17.1%) identifying as female (nonbinary gender identities were, unfortunately, not offered as a response option). In terms of race and/or ethnicity, the majority of the sample (88.6%) identified as non-Latinx White, 4.9% as Latinx, 3.2% as non-Latinx Black, 1.9% as American Indian or Alaskan Native, and 1.3% as Asian or Pacific Islander. The sample had an average of 13.55 years (SD = 1.73) of formal education. Participants had completed on average 1.55 deployments (SD = 0.67, range = 1–4).
At each time point, participants were provided with a verbal description of study procedures, given information regarding confidentiality, and informed they could withdraw from the study at any time without penalty. As noted, anonymous survey participation was offered. Response rates for survey completion (62%) were only available for the follow-up assessment. No compensation was provided for study participation at postdeployment. At follow-up, participants were eligible to be included in a raffle draw for three cash prizes of $100.
Measures
Demographics
Demographic data were assessed immediately postdeployment. Participants reported their age, self-identified gender, race and/or ethnicity, and years of education.
Treatment utilization
Consistent with prior studies on military samples (e.g., Elbogen et al., 2013), we conceptualized mental health treatment as including the use of psychiatric medications or mental health counseling. Two items assessed treatment utilization at follow-up. The first asked “Have you been in counseling or psychotherapy since your most recent deployment?” The second assessed pharmacotherapy, asking participants to indicate if they had taken any medications for mental health (e.g., depression and anxiety) since returning from deployment. For descriptive purposes, rates of utilization are reported separately for these two forms of mental health treatment. However, given our interest in utilization of any form of mental health treatment and in order to reduce the number of statistical tests conducted, responses from both items were combined into a single variable indicating whether any mental health treatment was received for use in longitudinal analyses. This variable was coded dichotomously (“1” if either psychotherapy or medications was utilized and “0” if neither was utilized).
Psychiatric symptom measures
Four widely used and validated questionnaires were used to assess psychiatric symptoms within four disorder domains, both immediately postdeployment and at follow-up. Established clinical cut-off scores were used to determine presence of symptom elevations.
Depression
The Beck Depression Inventory-II (BDI-II; Beck et al., 1996) is a 21-item measure assessing symptoms of depression. Participants indicated the degree to which they experienced various symptoms during the past 2 weeks on a 4-point Likert-type scale from 0 to 3. Item anchors vary across BDI-II items, with 0 reflecting an absence of symptoms (e.g., “I do not feel sad”) and three reflecting severe symptoms (e.g., “I am so sad or unhappy that I can’t stand it”). A higher score reflects greater depressive symptomatology. The BDI-II has shown high internal consistency and factorial validity (Dozois et al., 1998), including specifically in veteran populations (Palmer et al., 2014). A total score was computed by summing across all items (scale range = 0–63). Internal consistency was high in the current sample (α = .96). A score of 13 or greater has been recommended as a clinical cut-off optimizing sensitivity and specificity (Dozois et al., 1998) and was used in the present study to denote presence of clinically elevated symptoms.
Anxiety
The Generalized Anxiety Disorders–7 (GAD-7; Spitzer et al., 2006) is a 7-item measure assessing anxiety symptoms. Participants indicated the degree to which they experienced various symptoms during the past 2 weeks (e.g., “trouble relaxing”) from 0 (not at all) to 3 (nearly every day). The GAD-7 has shown high internal consistency as well as criterion, construct, factorial, and procedural validity (Spitzer et al., 2006). The GAD-7 has been widely used and shown to possess high internal consistency reliability and sensitivity to distress in veteran samples, specifically (Rudd et al., 2011). A total score was computed by summing across all items (scale range = 0–21). Internal consistency was high in the current sample (α = .91). A score of five or greater has been recommended as a clinical cut-off (Spitzer et al., 2006).
Alcohol Use
The Alcohol Use Disorders Identification Test (AUDIT; Babor, Higgins-Biddle et al., 2001) is a 10-item measure assessing alcohol use and effects. Example items include “How often do you have a drink containing alcohol?” and “Have you or someone else been injured as a result of your drinking?” Items are scored from 0 to 4, with 0 reflecting the absence of alcohol-related symptoms (e.g., never having a drink, no on being injured) and four reflecting elevated symptoms (e.g., drinking four or more times a week, someone being injured during the last year). The AUDIT has been widely used to detect problematic alcohol use and has shown concurrent, construct, and discriminant validity (Bohn, Babor, & Kranzler, 1995) and validated specifically in veteran samples (Bradley et al., 2003). Participants were asked to indicate the responses that best fit their drinking during the time they were consuming the most alcohol, either during the most recent deployment (postdeployment) or since returning from the most recent deployment (follow-up). A total score was computed following the published scoring recommendations (scale range = 0–40; Babor et al., 2001), with higher scores indicating a higher likelihood of problematic alcohol use. Internal consistency was acceptable in the current sample (α = .80). A score of eight or greater has been recommended as a clinical cut-off (Babor et al., 2001).
Post-traumatic Stress
The PTSD Checklist (PCL; Weathers et al, 1993) is a 17-item measure assessing symptoms of PTSD. The PCL-Military (PCL-M; Weathers et al., 1993), which has slightly altered wording for use with a military population, was used in the current study. Participants indicated the degree to which they have been bothered by various symptoms (e.g., “repeated, disturbing memories, thoughts, or images of a stressful experience from the past”) during the past month from 1 (not at all) to 5 (extremely). The PCL-M has shown high internal consistency and predictive validity in National Guard samples, specifically (Arbisi et al., 2012). A total score was computed by summing across all items (scale range = 17–85), with higher scores indicating higher PTSD symptoms. Internal consistency was high in the current sample (α = .94). A score of 50 or greater has been recommended as a clinical cut-off for military samples.
Total Number of Clinical Elevations
The total number of clinical elevations was computed by summing across elevations within the four symptom domains (scale range = 0–4).
Mental Health Help-Seeking Beliefs
Participants’ beliefs about mental health help-seeking were assessed at postdeployment via three dichotomously scored items (yes or no) created for the current survey, but similar in length and content to previous studies examining attitudes about mental health care (e.g., Fischer & Turner, 1970; Mojtabai, 2007). Items were: “I believe that those dealing with mental health issues can be helped by seeking treatment,” “If I personally were dealing with mental health issues, I would seek treatment,” and “I believe that mental health issues are best dealt with on your own, without professional help” (reverse scored). For the current study, we summed item scores (total possible points 0–3). Internal consistency reliability was slightly below the recommended range (α = .68).
Emotion Regulation Strategies
The Emotion Regulation Questionnaire (ERQ; Gross & John, 2003) was administered immediately postdeployment to assess participants’ tendency to use emotion regulation strategies of reappraisal and suppression. Items were rated on a 7-point Likert-type scale, ranging from 1 (strongly disagree) to 7 (strongly agree). Six items assessed reappraisal (e.g., “I control my emotions by changing the way I think about the situation I’m in”) and four items assessed suppression (e.g., “I control my emotions by not expressing them”). The ERQ has shown convergent and discriminant validity, as well as correlations with measures of well-being and interpersonal functioning (Gross & John, 2003). The ERQ has shown desirable psychometric properties specifically in military veteran samples (Boden et al., 2013). In addition to demonstrating acceptable internal consistency reliability, ERQ scores have been shown to change in response to PTSD treatment, with decreases in emotional suppression predicting decreases in PTSD symptoms post-treatment (Boden et al., 2013). Separate subscale scores were calculated by computing the mean across the reappraisal or suppression items (scale range = 1–7). Internal consistency reliabilities for each subscale were acceptable (αs = .84, .72, for reappraisal and suppression, respectively).
Analysis Procedures
Statistical analyses were conducted using the R programming language (R Core Team, 2018) and IBM SPSS Version 26 (IBM, 2019). Due to missingness in some variables above what is typically considered inconsequential (e.g., 5%; see Supplemental Materials Table 1), we created 10 datasets using multiple imputations. The fully conditional specification was implemented in SPSS, which is capable of handling both continuous and categorical variables (Enders, 2010). Unlike listwise deletion, the use of multiple imputation avoids loss of statistical power due to missingness and is robust to both missing completely at random (MCAR) and missing at random (MAR) assumptions (Enders, 2010). All statistical tests (i.e., p-values) were based on pooled estimates. For values that SPSS does not automatically pool (e.g., standard deviation for descriptive statistics), we took a simple average of analyses based on the 10 imputed datasets.
McNemar’s test for paired dichotomous data and paired t-tests were used to assess changes in psychiatric symptoms from postdeployment to follow-up. Cohen’s (1988) d was used as a standardized effect size reflecting symptom change and was calculated using methods common in meta-analysis (e.g., matched groups d; Borenstein et al., 2009). We interpreted the magnitude of d based on Cohen’s (1988) guidelines (i.e., ds = 0.20, 0.50, 0.80 reflect small, medium, and large effects, respectively). A correlation matrix was constructed showing the relationships between postdeployment variables with one another and treatment utilization at follow-up. A multivariate logistic regression model was used to examine treatment utilization at follow-up from all postdeployment variables in order to determine which, if any, predictors appeared most robust. Models were conducted on both the full sample and restricted to participants who met any cut-offs for elevated psychopathology at postdeployment. We calculated Nagelkerke’s R2 as a measure of variance explained and report odds ratios for interpretation of model coefficients. Based on the full sample (n = 311), we had 80% power to detect postdeployment to follow-up changes of d ≥ 0.16 and differences between groups (i.e., treatment utilizers vs. nonutilizers) of d ≥ 0.32. Based on the sample with clinically elevated symptoms (n = 128), we had 80% power to detect postdeployment to follow-up changes of d ≥ 0.25 and differences between groups (i.e., treatment utilizers vs. nonutilizers) of d ≥ 0.50. Power calculations were conducted using the “pwr.t.test” function of type “paired” or “two.sample” in the “pwr” package in R (Champley, 2018).
Results
Psychiatric Symptoms Immediately Postdeployment and at 6-Months Follow-Up
Psychiatric Symptoms Immediately Postdeployment and at 6-Month Follow-Up
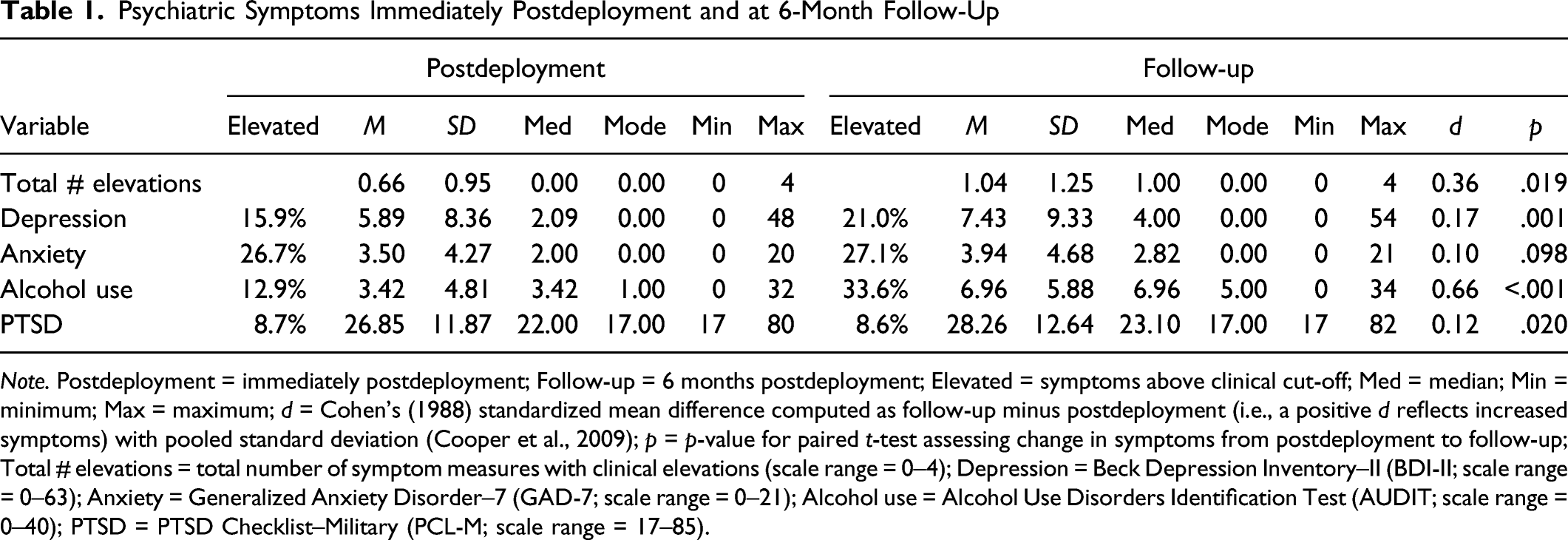
Note. Postdeployment = immediately postdeployment; Follow-up = 6 months postdeployment; Elevated = symptoms above clinical cut-off; Med = median; Min = minimum; Max = maximum; d = Cohen’s (1988) standardized mean difference computed as follow-up minus postdeployment (i.e., a positive d reflects increased symptoms) with pooled standard deviation (Cooper et al., 2009); p = p-value for paired t-test assessing change in symptoms from postdeployment to follow-up; Total # elevations = total number of symptom measures with clinical elevations (scale range = 0–4); Depression = Beck Depression Inventory–II (BDI-II; scale range = 0–63); Anxiety = Generalized Anxiety Disorder–7 (GAD-7; scale range = 0–21); Alcohol use = Alcohol Use Disorders Identification Test (AUDIT; scale range = 0–40); PTSD = PTSD Checklist–Military (PCL-M; scale range = 17–85).
At follow-up, 53.5% of the sample endorsed clinically significant psychiatric symptoms in at least one of the four symptom domains. Participants reported a mean of 1.04 (SD = 1.25) clinical elevations. Alcohol use disorder symptoms were most commonly elevated (33.6%) and PTSD symptoms were the least commonly elevated (8.6%).
There was a significant increase at follow-up in the proportion reporting elevations above the clinical cut-off on at least one of the four symptom measures (McNemar’s χ2 [1] = 14.35, p < .001). Participants also increased in the number of clinical elevations (d = 0.36, p = .019). 1 The largest increase in symptom total score was for AUD symptoms (d = 0.66, p < .001), although very small magnitude increases were also observed for depressive symptoms (d = 0.17, p = .001) and PTSD symptoms (d = 0.12, p = .020). No changes in anxiety symptoms were noted (d = 0.10, p = .098).
Treatment Utilization at Follow-up
A minority of the full sample (19.2%) reported receiving mental health treatment since their return from deployment. Among those reporting clinically elevated symptoms immediately postdeployment (n = 128), 27.8% reported receiving mental health treatment within 6 months postdeployment. Among those reporting clinically elevated symptoms at follow-up (n = 153), 31.6% reported receiving mental health treatment within 6 months postdeployment. Utilization rates at follow-up were higher for psychotherapy than for medications within the full sample (16.1% vs. 11.5%, McNemar’s χ2 [1] = 4.92, p = .030), among those with clinically elevated symptoms at follow-up (26.7% vs. 17.2%, McNemar’s χ2 [1] = 7.14, p = .011), but not among those with clinically elevated symptoms postdeployment (24.3% vs. 17.2%, p = .074).
Correlation Matrix of Postdeployment Variables and Treatment Utilization at Follow-Up
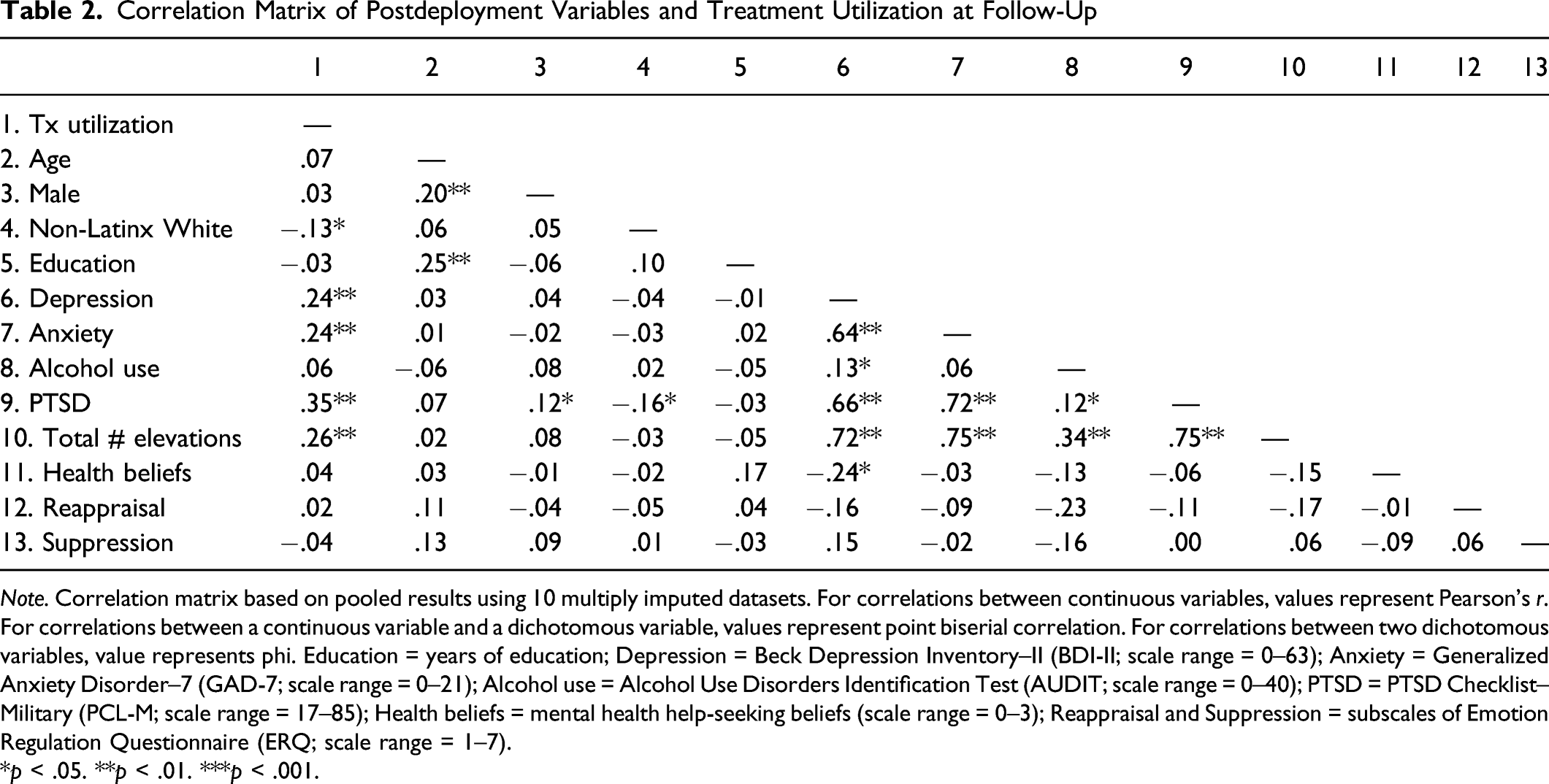
Note. Correlation matrix based on pooled results using 10 multiply imputed datasets. For correlations between continuous variables, values represent Pearson’s r. For correlations between a continuous variable and a dichotomous variable, values represent point biserial correlation. For correlations between two dichotomous variables, value represents phi. Education = years of education; Depression = Beck Depression Inventory–II (BDI-II; scale range = 0–63); Anxiety = Generalized Anxiety Disorder–7 (GAD-7; scale range = 0–21); Alcohol use = Alcohol Use Disorders Identification Test (AUDIT; scale range = 0–40); PTSD = PTSD Checklist–Military (PCL-M; scale range = 17–85); Health beliefs = mental health help-seeking beliefs (scale range = 0–3); Reappraisal and Suppression = subscales of Emotion Regulation Questionnaire (ERQ; scale range = 1–7).
*p < .05. **p < .01. ***p < .001.
We evaluated the assumptions of logistic regression, which included the dichotomous outcome, the linear relationship between predictor variables and the logit of the outcome, and the absence of multicollinearity when including multiple predictors (Cohen et al., 2003). Our outcome was dichotomous (i.e., treatment utilization). Scatterplots of significant continuous predictors of treatment utilization and the logit of treatment utilization appeared generally linear (Supplemental Materials Figure 1). As SPSS does not allow estimation of the variance inflation factor (VIF) for logistic regression, this was estimated using the original data set in R. In multivariate models with all predictors, VIF values suggested multicollinearity was not a substantial concern in either the full or clinical samples (VIFs < 3.5; Cohen et al., 2003).
Multivariate Logistic Regression Model Predicting Treatment Utilization at Follow-Up From Postdeployment Variables in the Full Sample
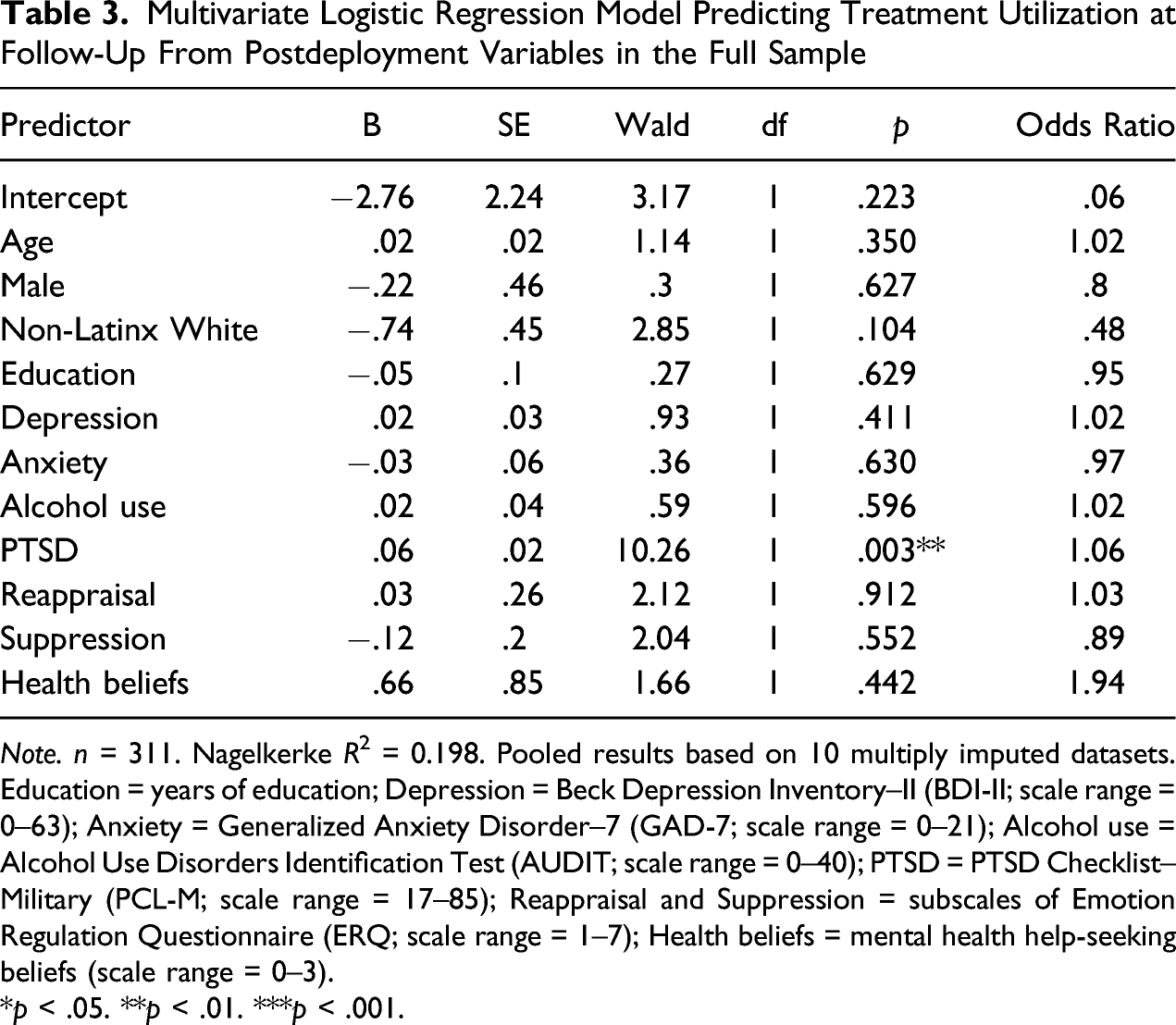
Note. n = 311. Nagelkerke R2 = 0.198. Pooled results based on 10 multiply imputed datasets. Education = years of education; Depression = Beck Depression Inventory–II (BDI-II; scale range = 0–63); Anxiety = Generalized Anxiety Disorder–7 (GAD-7; scale range = 0–21); Alcohol use = Alcohol Use Disorders Identification Test (AUDIT; scale range = 0–40); PTSD = PTSD Checklist–Military (PCL-M; scale range = 17–85); Reappraisal and Suppression = subscales of Emotion Regulation Questionnaire (ERQ; scale range = 1–7); Health beliefs = mental health help-seeking beliefs (scale range = 0–3).
*p < .05. **p < .01. ***p < .001.
Multivariate Logistic Regression Model Predicting Treatment Utilization at Follow-Up From Postdeployment Variables in the Sample With Clinically Elevated Symptoms at Post-Treatment
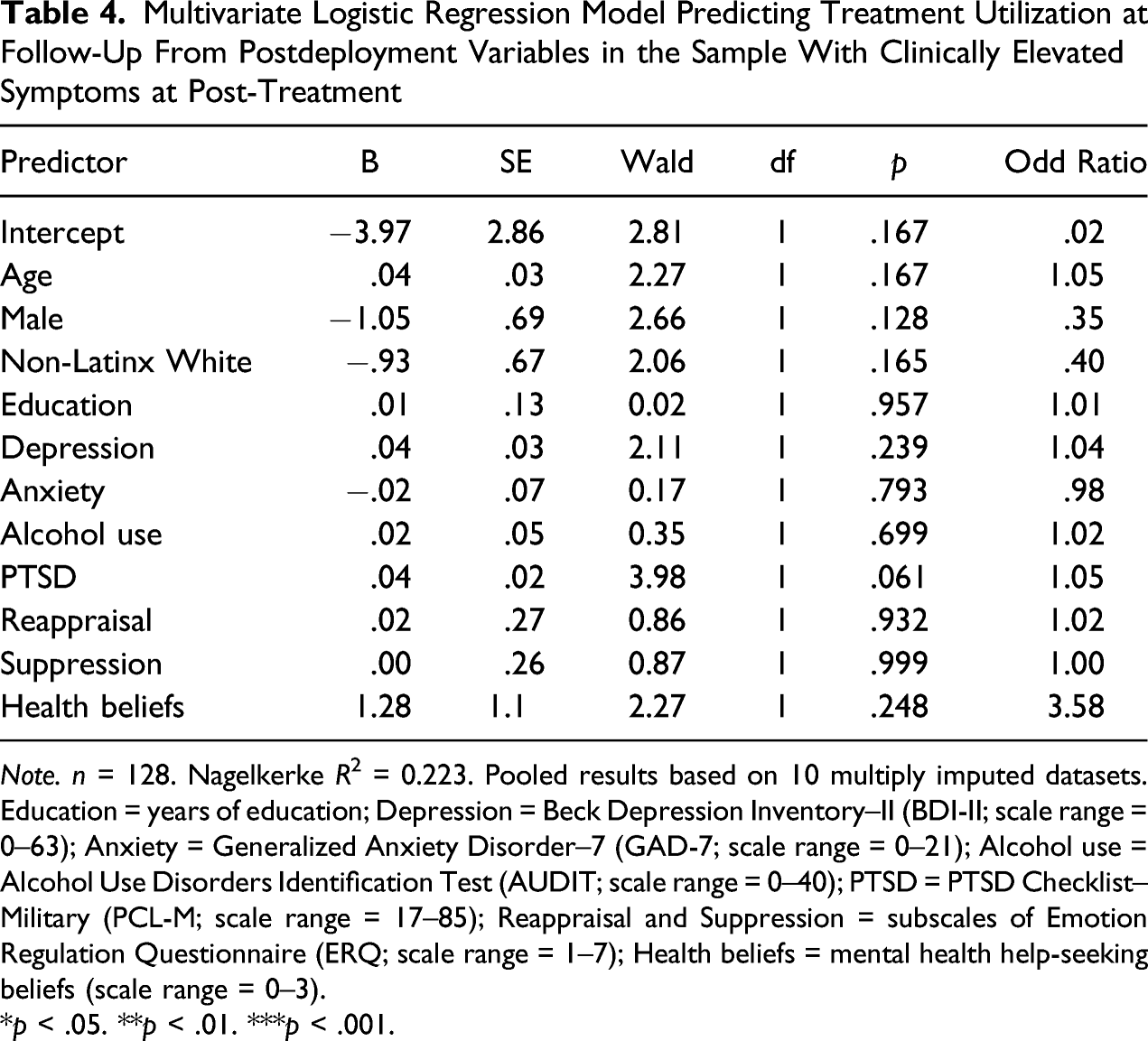
Note. n = 128. Nagelkerke R2 = 0.223. Pooled results based on 10 multiply imputed datasets. Education = years of education; Depression = Beck Depression Inventory–II (BDI-II; scale range = 0–63); Anxiety = Generalized Anxiety Disorder–7 (GAD-7; scale range = 0–21); Alcohol use = Alcohol Use Disorders Identification Test (AUDIT; scale range = 0–40); PTSD = PTSD Checklist–Military (PCL-M; scale range = 17–85); Reappraisal and Suppression = subscales of Emotion Regulation Questionnaire (ERQ; scale range = 1–7); Health beliefs = mental health help-seeking beliefs (scale range = 0–3).
*p < .05. **p < .01. ***p < .001.
Discussion
The current study examined psychiatric symptoms and mental health treatment utilization among National Guard service members immediately postdeployment and 6 months following return from deployment. Immediately postdeployment, a large proportion of the sample (41.2%) reported symptoms meeting the clinical cut-off for at least one of four symptom categories (depression, anxiety, AUD, and PTSD). At follow-up, the majority of the sample (53.5%) reported symptoms meeting the clinical cut-off for at least one of four symptom categories. These rates are significant, particularly given a potential for under-reporting of symptoms (i.e., due to social desirability bias) and the possibility that individuals with severe psychopathology may not have been present to complete the surveys. The largest increase in symptoms was observed for AUD (d = 0.66), although very small but statistically significant increases in depression (d = 0.17) and PTSD (d = 0.12) was also observed. Consistent with prior studies (Milliken et al., 2007; Riviere et al., 2011; Thomas et al., 2010), this pattern of findings demonstrates the high rates of psychiatric symptoms immediately upon returning from deployment among service members and highlights the 6 months postdeployment period as a vulnerable time for this population. The notable increase in AUD symptoms endorsed during the period of heaviest use after return from deployment is particularly striking, with 33.6% of the sample reporting clinically elevated symptoms at follow-up. Several prior studies have highlighted elevations in AUD symptoms among National Guard service members in particular (Blow et al., 2013; Thomas et al., 2010). It cannot be ruled out that the increase in AUD rates reflect reduced access to alcohol during deployment in certain regions, and subsequently increased access in the home community postdeployment.
Despite high rates of psychiatric symptoms, utilization with mental health treatment was relatively modest during the postdeployment period. Only 27.8% of the 128 participants with clinically elevated symptoms immediately postdeployment engaged with mental health treatment within 6 months following their return home. Although many service members did receive treatment, the majority of those with elevated symptoms did not. As an important point of comparison, a recent nationally representative survey of men in the general population found that 41.0% of those experiencing anxiety and depression symptoms received treatment in the previous year (i.e., took medication for anxiety or depression, spoke with a mental health professional; Blumberg et al., 2015). Thus, the treatment gap for National Guard service members appears to be larger than that of men in the general population. This is particularly notable, as veterans tend to have increased access to mental health resources (e.g., VHA or other military-related health care options), making it less likely that financial concerns played a role in the low rates of utilization. Indeed, per the Defense Authorization Act of 2008, the vast majority of National Guard service members who serve on active duty are entitled to 5-years of VHA benefits (VHA, 2011). Nonetheless, National Guard service members may face unique barriers to accessing treatment after a combat deployment that are greater than those faced in the general population, such as increased difficulty taking time away from civilian employment postdeployment (Stecker et al., 2010). Logistical barriers may also be present for Wisconsin National Guard service members living in rural areas (Stecker et al., 2013).
Aside from psychiatric symptom severity, 3 only race and/or ethnicity predicted later treatment utilization, and this was seen only in the full sample (i.e., not when restricted to those with clinically elevated symptoms, potentially due to decreased statistical power in the subsample). 4 The general lack of nonsymptom predictors of treatment utilization supports universal efforts to screen for mental health problems and facilitate treatment access for National Guard service members. The fact that race and/or ethnicity predicted treatment utilization in the full sample is intriguing, particularly given that the direction of this effect suggested that racial and/or ethnic minority National Guard service members may be more likely than their non-Latinx White peers to utilize treatment. This finding is in stark contrast to disparities in health care utilization observed in the general population (e.g., lower rates of mental health care among racial and/or ethnic minorities; Wang et al., 2005). However, this finding is in keeping with several recent, large-scale analyses that suggest racial and/or ethnic disparities in mental health treatment may be reduced or even reversed among veterans, with racial and/or ethnic minority veterans engaging with mental health treatment at similar or higher rates than non-Latinx White veterans (Bensley et al., 2017; Glass et al., 2010; Goldberg et al., 2020). 5
The current results contrast prior cross-sectional studies demonstrating a link between beliefs about treatment and treatment utilization (Fox et al., 2015; Stecker et al., 2013). Although it is possible that beliefs about treatment are truly not associated with treatment utilization in National Guard service members when examined longitudinally, it is perhaps more likely that our assessment missed key aspects of these beliefs. In particular, the current study did not directly assess mental health stigma (e.g., perceived public stigma related to mental health treatment seeking, “My peers might treat me differently”; Kulesza et al., 2015) which has been more widely shown to predict treatment utilization in both veteran and civilian populations (Kulesza et al., 2015; Vogel et al., 2007; Vogt, 2011). In contrast, the lack of association between cognitive reappraisal and emotional suppression strategies with all study variables, including treatment utilization, may imply they are not in fact particularly important constructs for understanding patterns of distress and treatment utilization in this population. Other sources of variance (e.g., combat experience and social support) may be more important and worth investigating further in future work.
Limitations
Several important limitations are worth noting. As the current sample was restricted to Wisconsin Army National Guard service members, findings may not generalize to other military or veteran samples. For example, the high rates of AUD symptom elevations in the current sample (33.6% at follow-up) are considerably higher than past-year probable AUD estimates in the general veteran population (14.8%; Fuehrlein et al., 2016). This may be due to differences between recently returned National Guard and other veterans, but may also be related to the culture of heavy alcohol use in Wisconsin (Wisconsin Department of Health Services, 2018) or our assessment of symptoms during the period of heaviest use. Of note, data from the Centers for Disease Control and Prevention (n. d.) indicates that Wisconsin has the second highest rate of binge drinking in the United States (24.4%). Other aspects of the results (e.g., psychiatric symptoms and treatment utilization) may be influenced by practices within the Wisconsin National Guard (e.g., offering of reintegration programming; Gunter-Hunt et al., 2013). On the other hand, it is likely that some aspects of the Wisconsin National Guard experience (e.g., challenges with reintegration into family life; Lapp et al., 2010) are not unique to Wisconsin or the National Guard but rather are common across service members (Bowling & Sherman, 2008). Low racial and/or ethnic and gender diversity in the current sample also limits generalizability. The reversed racial and/or ethnic disparity in treatment utilization observed in the full sample should be interpreted cautiously as a result and replicated in future samples with larger numbers of racial and/or ethnic minority participants. The unknown response rate for the postdeployment assessment further compounds questions of generalizability and is not possible to evaluate. It is also possible that individuals with severe symptoms were not present at the re-integration events, leading to under-estimates of psychiatric morbidity. It may be that psychiatric symptoms were under-reported immediately postdeployment, given the military context in which they were being collected (although the high rates of symptom endorsement argue against this possibility).
Internal consistency reliability was below the recommended cut-off for the mental health help-seeking measure, which may have reduced the accuracy of ratings and attenuated associated with treatment utilization. Although examination of the average inter-item correlations (rs = .32 to .50) suggests the items showed a recommended degree of internal consistency based on this alternative metric (rs = .10 to .50; Clark & Watson, 1995), it still would have been preferable to include a longer and previously validated mental health help-seeking measure (e.g., Vogt et al., 2014). In addition, key predictors of treatment utilization assessed in previous studies (e.g., mental health stigma; Kulesza et al., 2015) were not included.
Implications for Practice, Advocacy, Education/Training, and Research
Practice
At a basic level, our findings highlight the postdeployment period as a time of elevated risk for National Guard service members in terms of mental health symptomatology. Because early intervention may reduce the persistence of mental illness (Goldberg et al., 2019; Wang et al., 2005), the initial months after the return home may be a critical time for intervention. The high rates of psychiatric symptoms, which increased at follow-up, highlight potential difficulties associated with reintegration following a combat experience (Sayer et al., 2010) and supports continued attention to primary and secondary prevention efforts. These might include family-focused interventions (Sherman & Larsen, 2018) and other approaches aimed at supporting the tasks of reintegration (e.g., creating shared meaning, redefining roles, and managing strong emotions; Bowling & Sherman, 2008).
Advocacy
Given the treatment gap observed, ongoing efforts to engage returning service members in treatment are warranted. Both the Department of Defense and the VHA have implemented relevant programs and procedures in recent years, including postdischarge outreach efforts (Straits-Tröster et al., 2011), peer support programs (Hebert et al., 2008), universal postdeployment mental health screening (Hoge et al., 2006), integration of mental health services within primary care (Cornwell et al., 2018), and public awareness campaigns (e.g., Veterans’ Crisis Line; Knox et al., 2012). As reported by Goldberg et al. (2019), the reduced delay to mental health treatment among post 9/11 veterans relative to pre 9/11 veterans may be due to some of these factors. Efforts to increase public awareness and decrease stigma of PTSD may be part of why associations appeared particularly robust for PTSD symptoms, at least in the full sample. Rigorous epidemiological, and ideally, experimental studies evaluating specific efforts can further help to clarify the most effective methods for increasing treatment utilization.
Research
It is important to continue to identify barriers to treatment amenable to intervention (Mojtabai et al., 2011). Such barriers may vary across military subpopulations, demographics, and a variety of other factors, necessitating that research be conducted with sensitivity to individual- and group-level differences. Our results suggest that beliefs about mental health treatment utilization are not a primary barrier to access for National Guard service members, at least as assessed in the current sample. However, future studies in this population should clarify the role of stigma as a predictor of treatment utilization, along with other candidate barriers identified previously (e.g., logistical barriers, emotional readiness, and beliefs about treatment efficacy; Stecker et al., 2010, 2013). It would also be valuable to assess other military-specific factors that may relate to willingness to seek treatment, such as endorsement of military beliefs (e.g., ideal of mental toughness; Zinzow et al., 2013), aspects of veteran identity (e.g., warrior ethos Hack et al., 2017), and postdeployment social support (Polusny et al., 2011). Mobile health approaches (e.g., delivery through telehealth and smartphone applications; Knox et al., 2012; Sherman & Larsen, 2018) may be particularly relevant for addressing distance from care facilities as a logistical barrier among National Guard service members living in rural areas.
It is certain the experience of military service and postdeployment varies based on service members’ identity variables. Our results indicated, for example, that racial and/or ethnic minority status was associated with increased treatment utilization. As found in previous work (Glass et al., 2010; Goldberg et al., 2020), military veterans may be a population who do not demonstrate racial and/or ethnic disparities in mental health treatment engagement found in the general population. Future studies should examine what proximal factors are responsible for this reduced disparity (e.g., access to military health care coverage and universal screening; Bailey et al., 2017; Hoge et al., 2014), to inform broader efforts to reduce health disparities in the general population. It is crucial that future work closely examine the experiences of racial and/or ethnic minority National Guard service members and other military veterans to more fully characterize their military service and postdeployment experiences. Such efforts could build upon prior work showing that experiences of racism during military service account for variance in PTSD symptoms in Asian American Vietnamese veterans (Loo et al., 2001). Work in this area can be used to guide intervention and prevention strategies designed to create a more inclusive and equitable military experience.
Education and training
Ultimately, insights gained from ongoing research in this area can be integrated into formal education and training opportunities in order to increase treatment utilization among military veterans. Clinicians and trainees can become better attuned to factors that may promote or inhibit veterans’ likelihood of engaging in treatment, as well as get involved in efforts to reduce barriers to treatment (e.g., stigma reduction and novel treatment delivery efforts).
In summary, the current study adds to the literature as one of few to use a longitudinal design to examine postdeployment psychiatric symptoms and treatment utilization among National Guard service members, who may be particularly vulnerable during this period (Riviere et al., 2011; Thomas et al., 2010). Results highlight postdeployment as a period of increased risk to mental health. This is especially concerning in light of the large number (72.2%) of National Guard service members in our sample with elevated symptoms postdeployment who did not receive care at follow-up. Clarifying treatment barriers specific to this group and continuing efforts to engage returning service members in mental health treatment continue to be critical activities to reducing the psychiatric risks associated with military deployment.
Supplemental Material
sj-pdf-1-tcp-10.1177_00110000221074019 – Supplemental Material for Post-Deployment Treatment Gap: Symptoms and Treatment Utilization Among Returning National Guard Soldiers
Supplemental Material, sj-pdf-1-tcp-10.1177_00110000221074019 for Post-Deployment Treatment Gap: Symptoms and Treatment Utilization Among Returning National Guard Soldiers by Simon B. Goldberg, Anthony W. P. Flynn, Maleeha Abbas, Megan E. Schultz, Michele Hiserodt, Kathryn A. Thomas, Kasey Kallio, and Mary F. Wyman in The Counseling Psychologist
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
M.F.W. was supported in part by fellowship funding from the U.S. Department of Veterans Affairs. S.B.G. was supported by the University of Wisconsin–Madison, Office of the Vice Chancellor for Research and Graduate Education with funding from the Wisconsin Alumni Research Foundation. Research reported in this publication was also supported by the National Center For Complementary & Integrative Health of the National Institutes of Health under Award Number K23AT010879 to S.B.G. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. The authors wish to acknowledge the time and effort put forth by the service member respondents and study team members at the Zablocki VA Medical Center, Milwaukee, and W.S. Middleton Memorial Veterans Hospital, Madison, WI, and the resources provided by those institutions. The authors acknowledge that the data set used for this study belongs to the VA. The authors are grateful to Scott A. Baldwin for providing statistical consultation. This content does not represent the views of the U.S. Department of Veterans Affairs or the United States Government.
Supplemental Material
Supplemental material for this article is available online.
Notes
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.