
Abstract
We tested a modification of the dual pathway model using two sequential mediators between body dissatisfaction and binge eating: restricted eating and difficulties in emotion regulation replacing negative affect. A total of 435 college students completed an online survey. Results from path analyses indicated that the relationship between body dissatisfaction and binge eating was not mediated by restricted eating for neither women nor men. However, this relationship was mediated first by restricted eating and then by difficulties in emotion regulation for women only. Moreover, this relationship was mediated by difficulties in emotion regulation for both women and men. A post hoc analysis indicated that the above mediation results were still significant after adding negative affect into the model. No mediations through negative affect were significant. Clinical implications include the conceptualization and intervention of eating concerns within an emotion dysregulation framework.
The present study contributes to research describing risk factors for binge eating in college students by considering difficulties in emotion regulation as an additional mediator. Given the presence of binge eating on college campuses and the limited research on men in this area, the inclusion of difficulties in emotion regulation provides further explanation for this eating behavior in women and men. Furthermore, the role of difficulties in emotion regulation can inform clinical practice regarding assessment and intervention.Significance of the Scholarship to the Public
College represents a unique transition period in which students experience stressors that they may cope with by engaging in disordered eating behaviors. Indeed, the median age for the onset of eating disorders ranges from 18 to 21 years, which is considered within the traditional college age range (Hudson et al., 2007). Rates of eating disorders are estimated to range from 8% to 17% in college students (Eisenberg et al., 2011) that contrasts to adult lifetime prevalence rates of 0.28% to 0.85% (Udo & Grilo, 2018). Binge eating in particular is a problem on college campuses. Lipson and Sonneville (2017) found in a survey across 12 college campuses that the prevalence for binge eating was 49% in women and 30% in men. Binge eating is defined as the overconsumption of food within a discrete time period that is characterized by a loss of control (American Psychiatric Association, 2013). This behavior can include eating more rapidly than what is considered normal, feeling uncomfortably full, eating when not physically hungry, eating in isolation due to embarrassment, and feeling distressed about it afterward. The high rates of binge eating compared to general adult reports indicate that college students are an at-risk population who can benefit from early prevention, identification, and intervention for this disordered eating behavior.
Binge eating is related to low self-esteem (Herbozo et al., 2015), mood disorders (Becker & Grilo, 2015), self-harm, and suicide (Kostro et al., 2014). The mental and physical health consequences associated with binge eating stress the importance of studying risk factors that can be associated with the development of this disordered eating behavior. Men, in particular, can benefit from this research because they are often underdiagnosed and undertreated for eating disorders (Strother et al., 2012). This study aimed to examine the relationships among body dissatisfaction, restricted eating, difficulties in emotion regulation, and binge eating for both men and women.
The Dual Pathway Model for Binge Eating
Stice (1994) proposed a sociocultural dual pathway model that explained the developmental trajectory from body dissatisfaction to binge eating through two sequential mediators: restricted eating and negative affect. Whereas the original model included sociocultural influences on body dissatisfaction, we focused on the mediations between body dissatisfaction and binge eating. Therefore, body dissatisfaction was our first predictor. Figure 1, Panel A illustrates this abbreviated Stice (1994) original model. The original dual pathway model (Panel A) and the modified dual pathway model (Panel B) for binge eating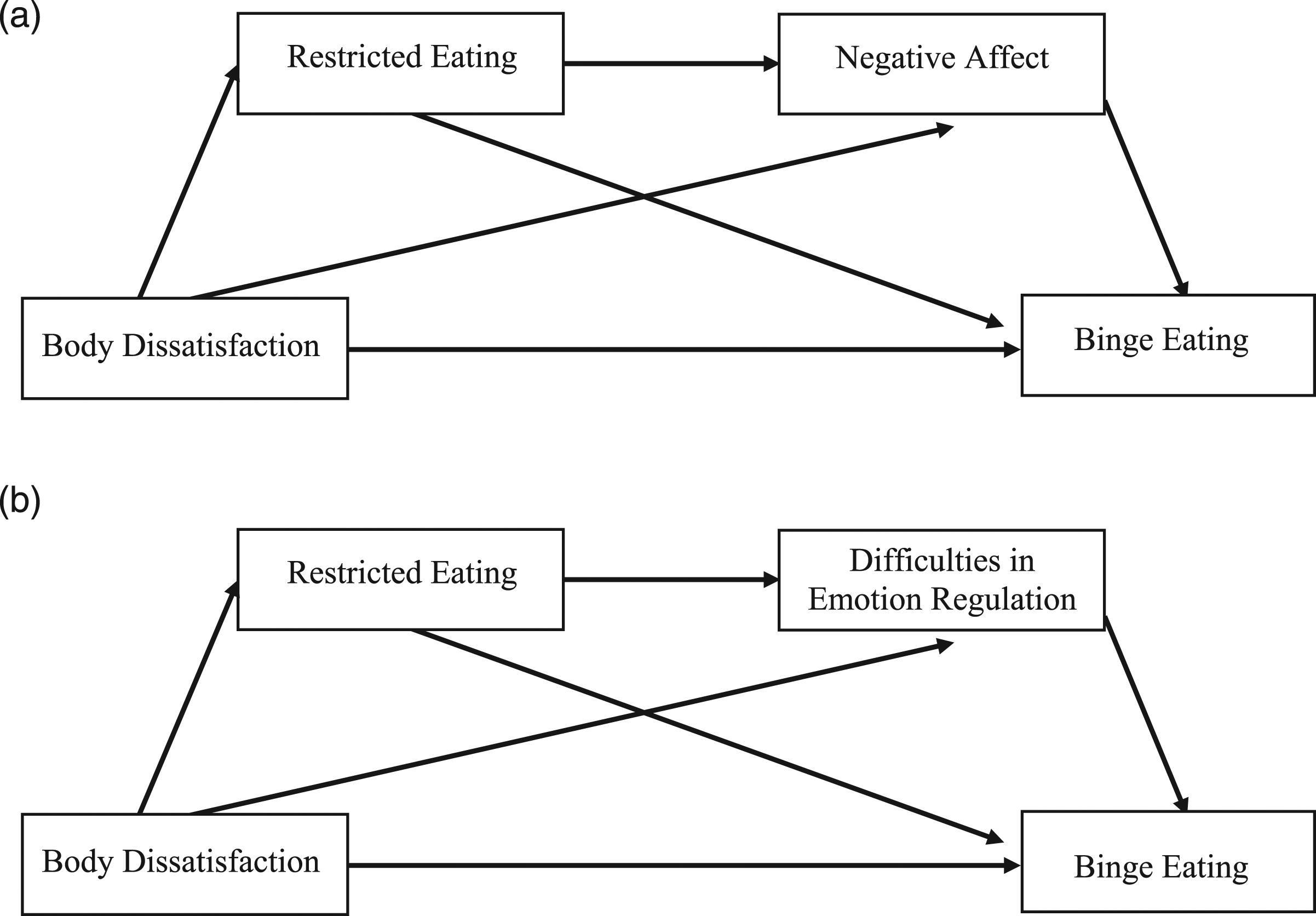
The first pathway was through the mediator of restricted eating, which can result in binge eating through two mediation mechanisms. One mechanism was that the relationship between body dissatisfaction and binge eating was mediated by restricted eating, as binge eating may be used to compensate for caloric deprivation related to restricted eating (Mathes et al., 2009; Polivy & Herman, 1985). Additionally, those who restrict their eating may also binge eat due to the abstinence-violation effect (Stice, 2001), in which one who lapses from a commitment, such as restricted eating, by uncontrollably engaging in the behavior they were originally trying to prevent (i.e., binge eating). The other mechanism was that the relationship between body dissatisfaction and binge eating was mediated first by restricted eating and then by negative affect. Those who engage in restricted eating may be at risk of experiencing negative affect because they may be in a starvation state or are otherwise cognitively controlling their eating instead of listening to their physiological cues for hunger and satiety. Then, they may binge eat as a distraction or for comfort to cope with their experience of negative affect (Stice, 2002). The second pathway was through the mediator of negative affect (Hawkins & Clement, 1984). Those who experience body dissatisfaction may experience negative affect because they are not measuring up to their ideal body. Once again, experiencing negative affect may result in binge eating because eating may be a distraction from feeling painful emotions and food may be used for comfort.
The dual pathway model has received cross-sectional (Dakanalis et al., 2014; Welsh & King, 2016) and longitudinal support (Puccio et al., 2018; Stice & Van Ryzin, 2019). However, specific paths have been inconsistently supported. In particular, there are conflicting findings as to whether restricted eating is a predictor of binge eating (Dakanalis et al., 2014; Holmes et al., 2014; Ouwens et al., 2009; Stice, 2002; van Strien et al., 2005). Additionally, researchers have attempted to expand the model to further explain developmental paths. Negative urgency, a personality trait characterized by impulsivity, has been tested in the model as a moderator (Racine & Martin, 2016; Wenzel et al., 2014) and as an independent predictor (Puccio et al., 2018), but it remains to be seen where it fits into the model. The lack of consensus regarding negative urgency indicates that, although this can be a useful construct to study, more research is needed. van Strien et al. (2005), with the support of later research (Dakanalis et al., 2014; Ouwens et al., 2009), also found a lack of interoceptive awareness as a link between negative affect and binge eating. Conceptually, impulsivity and the awareness of emotional states are facets of the broader construct of emotion dysregulation (Gratz & Roemer, 2004). Since emotion dysregulation is a transdiagnostic factor associated with disordered eating (Mallorquí-Bagué et al., 2018), we built upon this previous research on impulsivity and interoceptive awareness by examining difficulties in emotion regulation in Stice’s (1994) model.
Modification of the Dual Pathway Model
Gratz and Roemer (2004) defined difficulties in emotion regulation as an integrative way to conceptualize emotion dysregulation in adults that consists of awareness and understanding of emotions, acceptance of emotions, ability to inhibit impulsivity and engage in goal-directed behavior, and access to effective emotion regulation strategies. In contrast, negative affect is the subjective experience of negative emotions, such as shame and fear (Watson et al., 1988). We made the argument that difficulties in regulating painful emotions, rather than simply their presence, could result in binge eating. The rationale for this modification was that we sought to explore how the management of emotions was related to binge eating. For instance, those who can effectively manage their negative feelings likely use adaptive coping strategies. However, those who binge eat may be unclear about their feelings and lack the skills to deal with them (Whiteside et al., 2007). Extant research has supported emotion regulation difficulties as a predictor of binge eating in women with eating disorders (Harrison et al., 2010; Mallorquí-Bagué et al., 2018), as well as college students (Whiteside et al., 2007). Furthermore, Harrison et al. (2010) found that those with eating disorders had more difficulty regulating their emotions compared to healthy controls who did not present with eating disorders.
Studies have revealed that emotion regulation difficulties accounted for the variance in binge eating over and above negative affect in college women and men (Ambwani et al., 2014; Lavender & Anderson, 2010) and adults seeking treatment for binge eating disorder (Gianini et al., 2013). These studies indicate that emotion regulation difficulties are an additional risk factor for binge eating and may be a more useful predictor compared to negative affect. Thus far, no existing study has examined difficulties in emotion regulation as a modification in the original dual pathway model. Therefore, we intended to be the first to explore whether a model with difficulties in emotion regulation could help further explain the associations between body dissatisfaction and binge eating.
Given the role of emotion dysregulation in eating disorders and the limited research examining specific aspects of this construct within the dual pathway model, we intended to expand the scope of this research. We modified Stice’s (1994) model by keeping restricted eating but proposing that difficulties in emotion regulation, in the place of negative affect, predict binge eating (see Figure 1, Panel B). Therefore, with restricted eating as a mediator, our first hypothesis was the same as that in Stice’s (1994) original model (i.e., the relationship between body dissatisfaction and binge eating would be mediated by restricted eating).
In linking restricted eating and body dissatisfaction with emotion dysregulation, there is evidence that those who restrict their eating may have difficulty regulating their emotions. In a nonclinical sample, Haynos et al. (2018) found that those who restricted eating had elevated difficulties in emotion regulation. Those who restrict eating can develop an obsession with food (Jones & Rogers, 2003) and this preoccupation can prevent them from focusing on internal states. They may experience less awareness and understanding of their emotions and lack access to adaptive emotion regulation strategies (Lavender et al., 2015; Racine & Wildes, 2013), resulting in potential binge eating in an effort to manage their emotions. Thus, the second hypothesis of this study was to support the mechanism from body dissatisfaction to restricted eating, to difficulties in emotion regulation, and then to binge eating. Specifically, there would be a positive relationship between body dissatisfaction and restricted eating, a positive relationship between restricted eating and difficulties in emotion regulation, and a positive relationship between difficulties in emotion regulation and binge eating.
Body dissatisfaction can also be associated with difficulties in emotion regulation. Those who experience body dissatisfaction may feel angry at themselves for failing to control their appearance and experience this anger as a dominating force in their mind, making it difficult for them to focus on other things. Sim and Zeman (2005) found in a sample of teenage girls that body dissatisfaction was associated with symptoms of emotion dysregulation. Sim and Zeman (2005) also observed that the relationship between body dissatisfaction and bulimic symptoms was partially mediated by emotion dysregulation variables for teenage girls. It is therefore likely that difficulties in emotion regulation might also be a mediator for the link between body dissatisfaction and binge eating for college students. Thus, the third hypothesis of this study was to support the modification of the pathway by which difficulties in emotion regulation would mediate the relationship between body dissatisfaction and binge eating. Specifically, there would be a positive relationship between body dissatisfaction and difficulties in emotion regulation, and a positive relationship between difficulties in emotion regulation and binge eating.
The dual pathway model was originally proposed for women and has been sparsely applied to men, but findings are inconsistent. In a study that tested results separately by gender, Womble et al. (2001) found that all the paths in the model were significant for women. For men, they found that the paths from body dissatisfaction to negative affect and dietary restraint (i.e., the two mediators) were not significant, but the paths from those mediator variables to binge eating were significant. In contrast, Mason and Lewis (2015) found support for a model that included impulsivity and food-related cognitions as additional mediators with men and women. Inconsistent findings may be due to methodological differences, such as varied measurement decisions (Womble et al., 2001), analyzing men and women together (Welsh & King, 2016), and having small sample sizes (Ruisoto et al., 2015). Given inconsistent findings for women and men and the paucity of rigorous examinations of this model with men, it was important for us to examine the modified model separately with women and men.
The Present Study
In summary, we tested a modification of the dual pathway model with difficulties in emotion regulation in the place of negative affect. We proposed three mediation hypotheses for both women and men. The first hypothesis was that restricted eating would mediate the relationship between body dissatisfaction and binge eating. The second hypothesis was that the relationship between body dissatisfaction and binge eating would be mediated by restricted eating and then difficulties in emotion regulation. The third hypothesis was that difficulties in emotion regulation would mediate the relationship between body dissatisfaction and binge eating. For exploration purposes, a multiple-group analysis examined whether the modified model invariantly applied to women and men. Finally, we conducted a post hoc analysis that added negative affect to the modified model to see the unique contributions of negative affect and difficulties in emotion regulation.
Method
Power Analysis
We calculated the power for structural equation modeling (see Sloper, 2020) and set the power equal to .80, alpha to .05, and effect size to .10, .30, and .50 for small, medium, and large effect sizes. Results indicated sample sizes of 34, 137, and 1454 for the respective effect sizes. We therefore sought to detect small to medium effect sizes with samples of about 200 for women and 200 for men.
Participants
Participants consisted of 435 students, 230 women (52.9%), 205 men (47.1%), with ages ranging from 18 to 31 years (Mage = 19.17, SD = 1.61). Of these participants, 391 (89.89%) identified as White, 13 (2.99%) as African, African American, or Black, 24 (5.52%) as Asian, Asian American, or Pacific Islander, 22 (5.06%) as Hispanic or Latinx, 5 (1.15%) as American Indian or Alaska Native, 2 (0.46%) as Middle Eastern, 9 (2.07%) as multiracial, and 2 (0.46%) identified as other (Note: Some participants identified themselves as multiracial and selected multiple race options. Therefore, the total was more than 100 percent). There were 214 (49.20%) freshmen, 132 (30.34%) sophomores, 52 (11.95%) juniors, 36 (8.28%) seniors, and 1 (0.23%) graduate student. Participants were asked to provide their height in inches and weight in pounds. Body mass index (BMI) was calculated using the formula (weight/height [ ^ 2]) x 703. BMI ranged from 16.33 to 44.48 (M = 24.07, SD = 4.45).
Procedure
Participants were college students over the age of 18 years recruited from a Midwestern university through the Psychology Department’s research pool. Participants who met the age requirement were informed that the study was about binge eating in college students and that it would take less than 45 min to complete. They received a link to the online survey and signed an electronic informed consent form before filling out the survey. Students received research credit for participation in this study. Five hundred students responded to this survey. However, 18 participants had blank responses, 40 participants answered incorrectly one or more attention check items (e.g., “Please mark ‘true’ or ‘false’ for the following statement: one week has five days”), five did not identify as either women or men, and two participants under 18 years old were removed. Thus, the final sample size in this study was 435 participants.
Measures
Body dissatisfaction
The Body-Esteem Scale (BES) for Adolescents and Adults (Mendelson et al., 2001) is a 23-item measure of one’s satisfaction with their body and appearance. The BES has three subscales: Appearance, Weight, and Attribution. A sample item is, “I feel ashamed of how I look.” Items are rated on a 5-point Likert-type scale, ranging from 0 (never) to 4 (always), with higher scores indicating greater dissatisfaction with one’s body. Mendelson et al. (2001) found coefficient alphas of .92 (Appearance), .94 (Weight), and .81 (Attribution) in a sample of adolescents and college students. In this study, coefficient alphas were .93 for both women and men for the total scale. Construct validity was established by reporting positive correlations between global self-esteem and BES-Appearance, between actual weight and BES-Weight, and between social self-esteem and BES-Attribution in a sample of adolescents and college students (Mendelson et al., 2001).
Restricted eating
The Cognitive Restraint subscale of the Three-Factor Eating Questionnaire (Stunkard & Messick, 1985) is a 21-item measure to assess restricted eating. A sample item is, “How often are you dieting in a conscious effort to control your weight?” Participants are asked to rate items in a variety of formats: dichotomous (i.e., yes/no), Likert-type (e.g., 1 = not at all to 4 = very much), and frequency (e.g., 1 = rarely to 4 = always), with higher scores indicating greater restricted eating. Coefficient alpha was .82 in a sample of college students (Gow et al., 2010). In this study, coefficient alphas were .84 for women and .81 for men. Construct validity for this subscale was evidenced through moderate (r = .51) to strong correlations (r = .66) with the Restraint subscale of the Dutch Eating Behavior Questionnaire in young adult women (Laessle et al., 1989) and undergraduate women and men (Allison et al., 1992).
Negative affect
The Negative Affect subscale from the Positive and Negative Affect Schedule (Watson et al., 1988) measures negative mood states. Participants rate 10 mood descriptors (e.g. irritable and afraid) based on how they have felt in the past week. Items are rated on a 5-point Likert-type scale, ranging from 1 (very slight or not at all) to 5 (extremely), with higher scores indicating greater negative affect. Coefficient alphas ranged from .84 to .87 in samples of undergraduate college students (Watson et al., 1988). In this study, coefficient alphas were .86 for women and .90 for men. Construct validity was supported through positive correlations with measures of distress, depressive symptoms, and anxiety (Watson et al., 1988).
Difficulties in emotion regulation
The Difficulties in Emotion Regulation Scale (Gratz & Roemer, 2004) is a 36-item measure that assesses difficulties in emotion regulation. It has six subscales: Non-Acceptance of Emotional Responses, Difficulty Engaging in Goal-Directed Behavior, Impulse Control Difficulties, Lack of Emotional Awareness, Limited Access to Emotion Regulation Strategies, and Lack of Emotional Clarity. Sample items include, “When I’m upset, I have difficulty thinking about anything else,” and “I have no idea how I’m feeling.” Items are rated on a 5-point Likert-type scale, ranging from 1 (almost never) to 5 (almost always), with higher scores indicating greater difficulties in emotion regulation. Coefficient alphas ranged from .79 to .92 in a large sample of college students (Whiteside et al., 2007). In this study, coefficient alphas were .95 for women and .94 for men. Construct validity was evidenced through a negative correlation between difficulties in emotion regulation and beliefs about one’s efficacy in altering negative moods and emotional expressivity, and a positive correlation between difficulties in emotion regulation and experiential avoidance in a sample of undergraduate students (Gratz & Roemer, 2004).
Binge eating
The Binge Eating Disorder subscale from the Eating Disorder Diagnostic Scale (Stice et al., 2000) assesses Diagnostic and Statistical Manual of Mental Disorders-IV (DSM-IV: American Psychiatric Association, 2013) diagnostic symptoms for binge eating disorder. A sample item is, “How many days per week on average over the past 6 months have you eaten an unusually large amount of food and experienced a loss of control?” Participants rate nine items in a variety of dichotomous (i.e., yes/no) and frequency formats (i.e., how many days per week…). Scoring provides tentative diagnoses of full threshold and subthreshold binge eating disorder. Higher scores indicate greater binge eating. The present study did not intend to diagnose participants with binge eating disorder and therefore used the total score. Coefficient alpha was .77 in a sample of undergraduate women and men (Lane & Szabó, 2013). In this study, coefficient alphas were .81 for women and .77 for men. Construct validity was established by positive correlations of binge eating scores with diagnoses of binge eating disorder through structured interviews (93% accuracy), as well as positive associations with scores on related constructs from the Eating Disorder Examination, Yale–Brown–Cornell Eating Disorder Scale, and Three-Factor Eating Questionnaire in a sample of adolescent girls and adult women (Stice et al., 2000).
Results
Preliminary Analyses
Missing data were analyzed and results indicated that the missing data were minimal, ranging from 0.05% (negative affect) to 1.66% (binge eating). Therefore, the mean replacement method in SPSS was used for missing data at the item level (Parent, 2013). After mean replacement, there were no missing data for all variables except BMI. Missing BMI values were handled by FIML in Mplus. Little’s missing completely at random (MCAR) test was then conducted at the scale level and a nonsignificant result indicated that data were missing at random, χ2(6, N = 435) = 3.57, p = .74.
Independent Samples T-Test Results for Women and Men
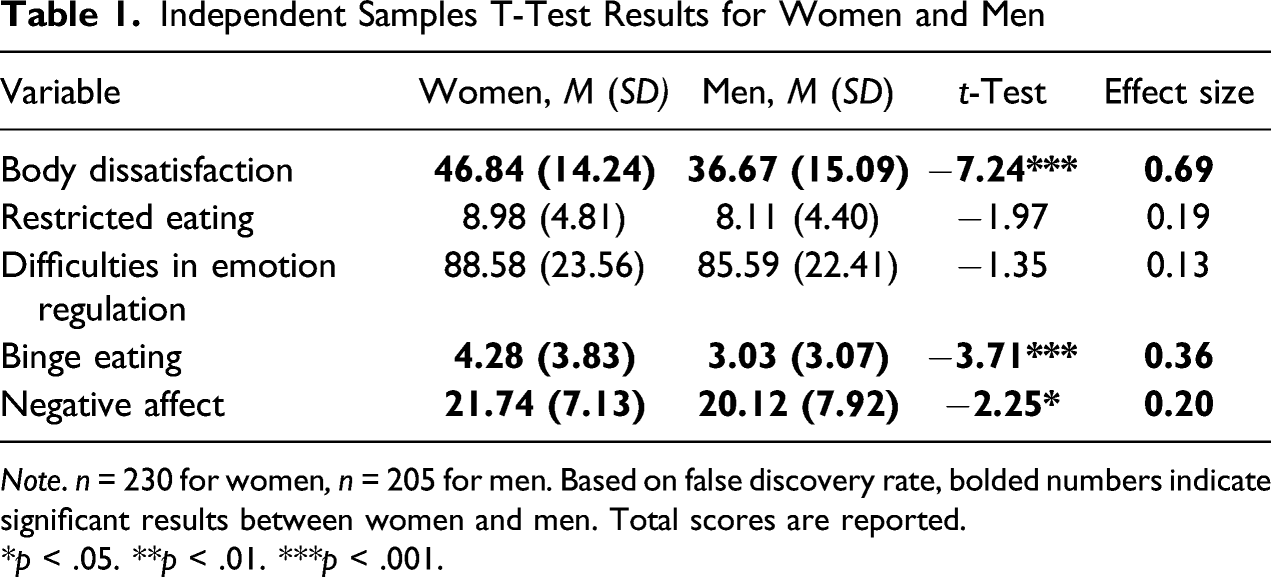
Note. n = 230 for women, n = 205 for men. Based on false discovery rate, bolded numbers indicate significant results between women and men. Total scores are reported.
*p < .05. **p < .01. ***p < .001.
Means, Standard Deviations, and Intercorrelations for Women
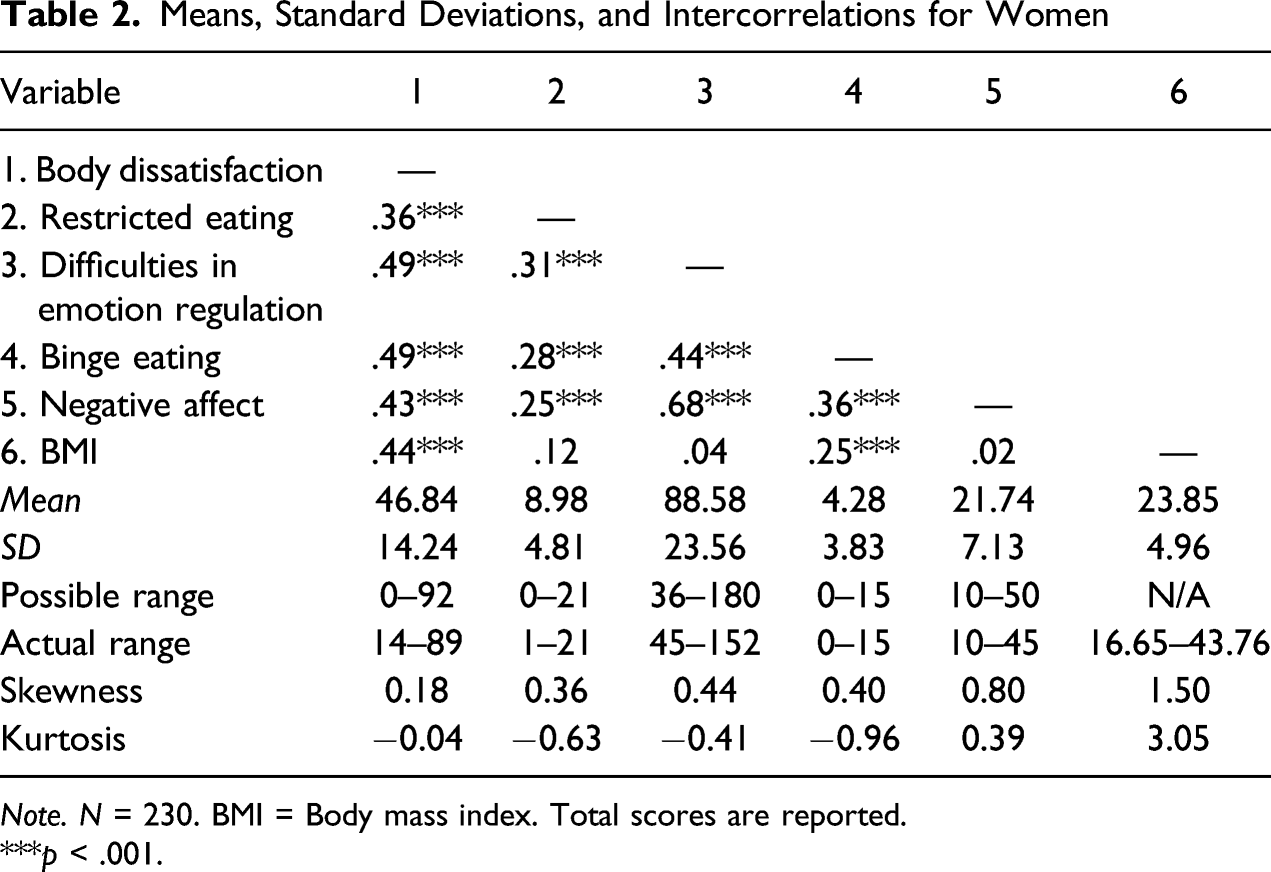
Note. N = 230. BMI = Body mass index. Total scores are reported.
***p < .001.
Means, Standard Deviations, and Intercorrelations for Men
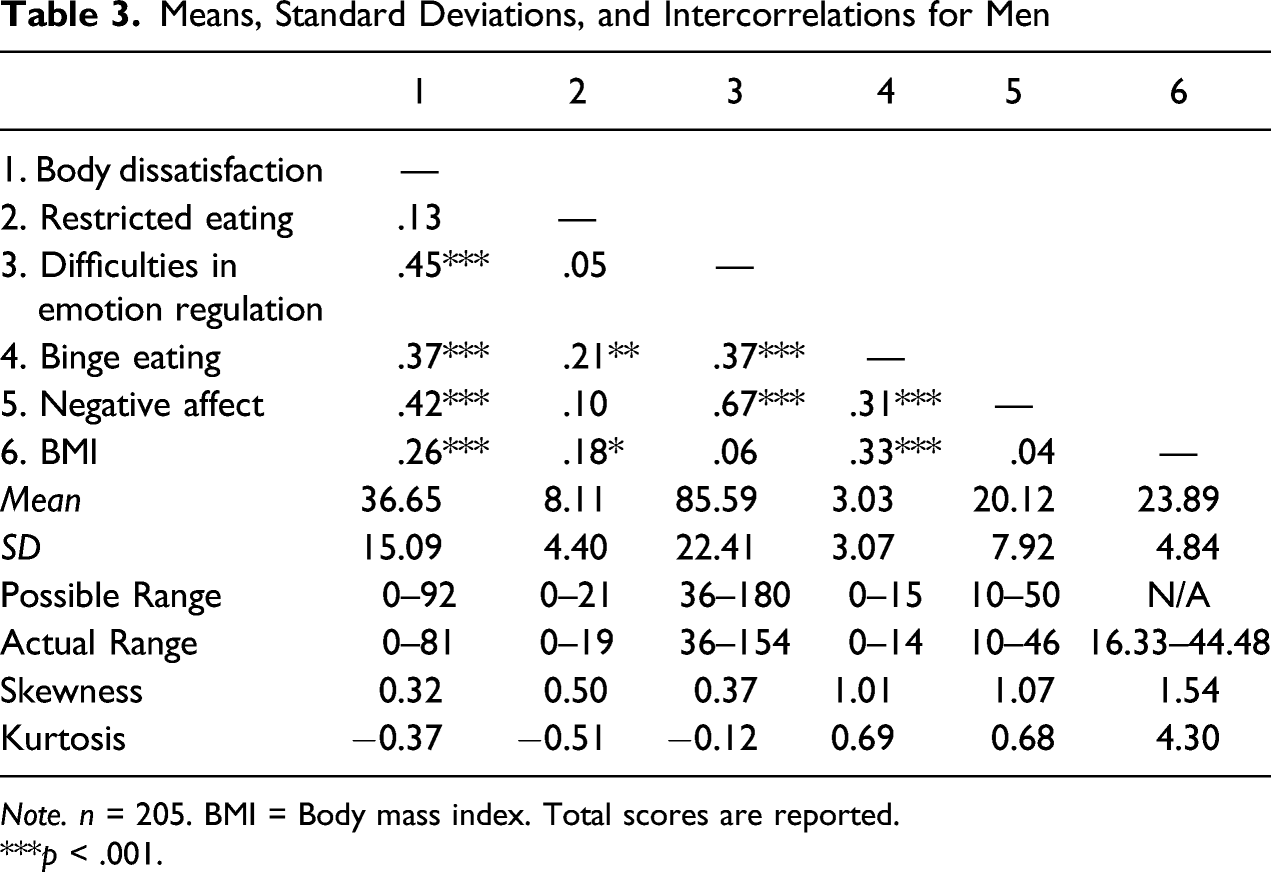
Note. n = 205. BMI = Body mass index. Total scores are reported.
***p < .001.
Mediation Analyses
Bootstrap Analyses of the Magnitude and Statistical Significance of Indirect Effects
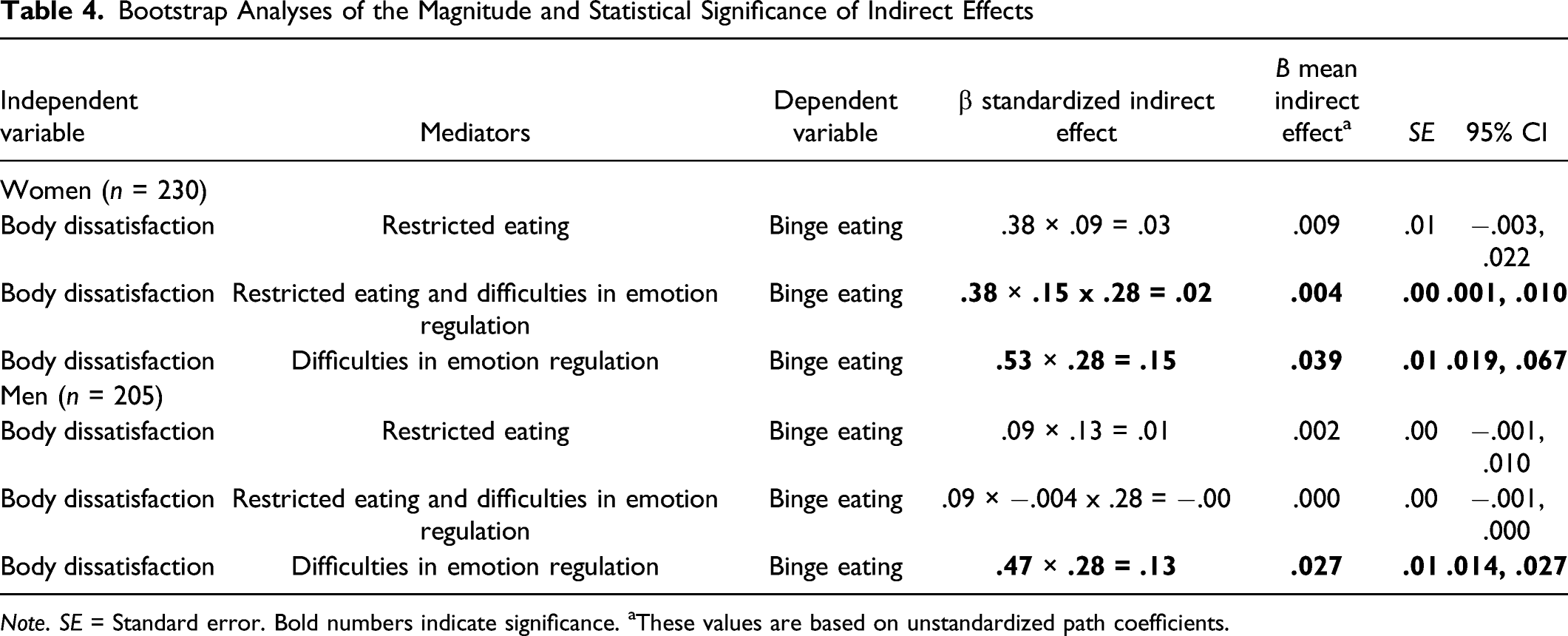
Note. SE = Standard error. Bold numbers indicate significance. aThese values are based on unstandardized path coefficients.
For women, as seen in Figure 2 and Table 4, the path from body dissatisfaction to restricted eating was significant, but the path from restricted eating to binge eating was not significant. The first mediation hypothesis (body dissatisfaction → restricted eating → binge eating) was not significant. Next, the path from body dissatisfaction to restricted eating was significant, the path from restricted eating to difficulties in emotion regulation was significant , and the path from difficulties in emotion regulation to binge eating was also significant. The second mediation hypothesis (body dissatisfaction → restricted eating → difficulties in emotion regulation → binge eating) was significant. Finally, the path from body dissatisfaction to difficulties in emotion regulation was significant, and the path from difficulties in emotion regulation to binge eating was significant. The third mediation hypothesis (body dissatisfaction → difficulties in emotion regulation → binge eating) was significant. The modified dual pathway model for women (Panel A) and men (Panel B) after controlling for BMI.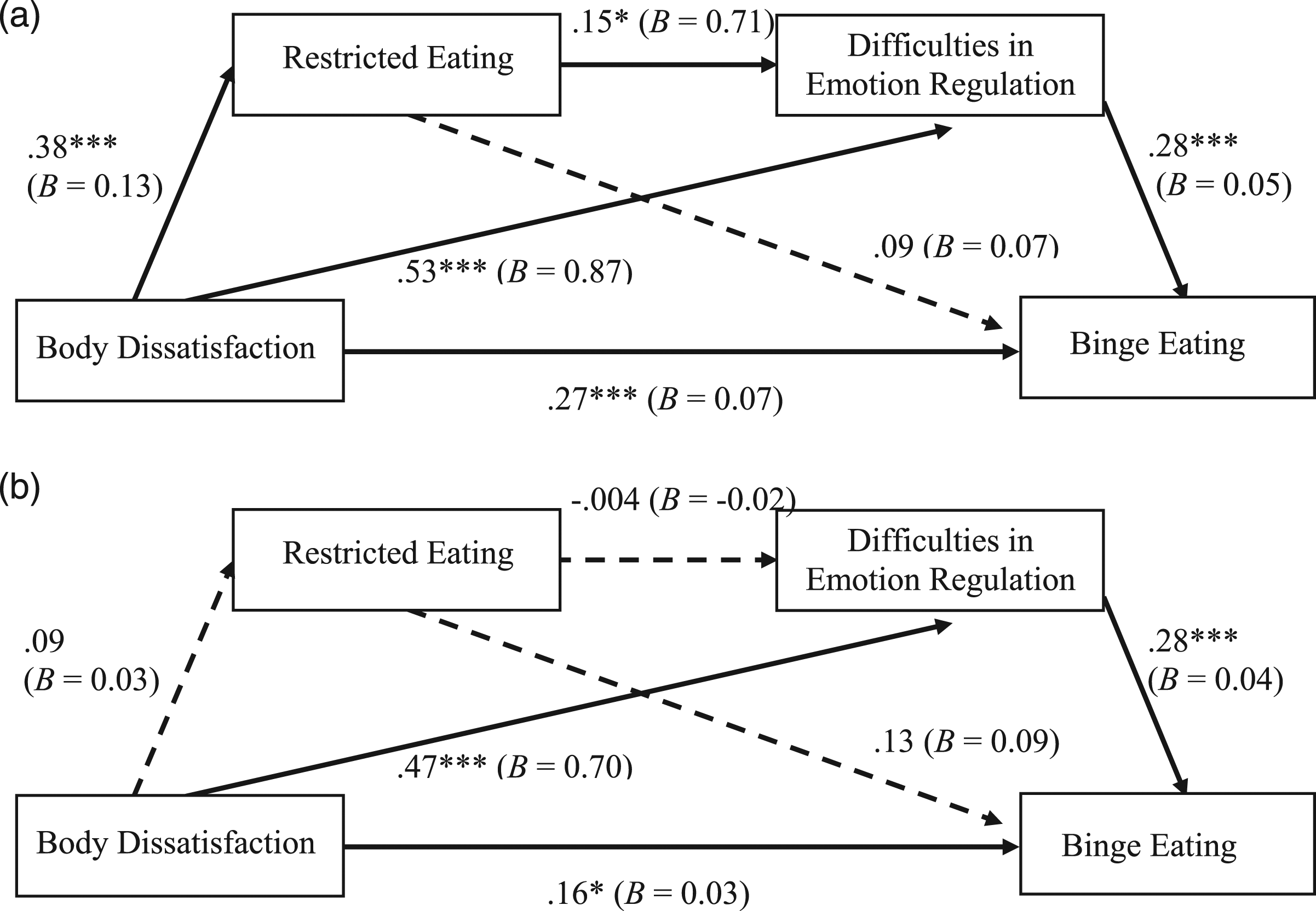
For men, as seen in Figure 2 and Table 4, the path from body dissatisfaction to restricted eating was not significant, and the path from restricted eating to binge eating was not significant. The first mediation hypothesis (body dissatisfaction → restricted eating → binge eating) was not significant. Next, the path from body dissatisfaction to restricted eating was not significant, the path from restricted eating to difficulties in emotion regulation was not significant, and the path from difficulties in emotion regulation to binge eating was significant. The second mediation hypothesis (body dissatisfaction → restricted eating → difficulties in emotion regulation → binge eating) was not significant. Finally, the path from body dissatisfaction to difficulties in emotion regulation was significant, and the path from difficulties in emotion regulation to binge eating was significant. The third mediation hypothesis (body dissatisfaction → difficulties in emotion regulation → binge eating) was significant.
Multiple-Group Analysis
A multiple-group analysis was conducted in Mplus (Muthén & Muthén, 2010) to examine whether each path in the mediation model was equivalent between women and men, controlling for BMI. One was the freely estimated model (i.e., freely estimated structural paths) and the other was the equally estimated model (i.e., constrained structural paths to be equal). The result for the freely estimated model was χ2(0, N = 435) = 0, p = 1.0, CFI = 1.00, SRMR = .00, RMSEA = .00. The result for the equally estimated model was χ2(6, N = 435) = 19.33, p = .004, CFI = .95, SRMR = .08, RMSEA = .10, CI [.05, .15]. A chi-square difference test was used to compare the two models, and a significant result, χ2(6, N = 435) = 19.33, p = .004, showed that structural paths were not invariant between women and men.
Because this was an exploratory analysis, the modification indices from the equally estimated model were used to identify which paths contributed to this difference. One path (body dissatisfaction → restricted eating) was identified to be potentially different between women and men. Thus, this path was set up to be freely estimated. The result for this revised equally estimated model (i.e., freely estimating this path) was χ2(5, N = 435) = 9.57, p = .09, CFI = .98, SRMR = .05, RMSEA = .07, CI [.01, .13]. Then, a chi-square difference test was used to compare this revised equally estimated model (i.e., χ2 = 9.57) with the freely estimated model (i.e., χ2 = 0). A nonsignificant result, χ2(5, N = 435) = 9.57, p = .09, showed that the only structural path that was not invariant between women and men was this path from body dissatisfaction → restricted eating. Specifically, this path was significant for women (β = .38, p < .01) but not significant for men (β = .09, p = .22).
Post Hoc Analysis
In order to determine whether difficulties in emotion regulation was a unique mediator, we added negative affect to the modified model in order to see the unique contributions of negative affect and difficulties in emotion regulation, after controlling for the effect of the other variable (Figure 3). For women, the mediation of body dissatisfaction → restricted eating → difficulties in emotion regulation → binge eating was still significant, as was body dissatisfaction → difficulties in emotion regulation → binge eating. For men, the mediation of body dissatisfaction → difficulties in emotion regulation → binge eating was still significant. Therefore, the significant mediation effects still remained the same after controlling for negative affect. However, no mediation effects through negative affect were significant for women or men. The post hoc analysis results for the modified dual pathway model after controlling for BMI for women (Panel A) and men (Panel B).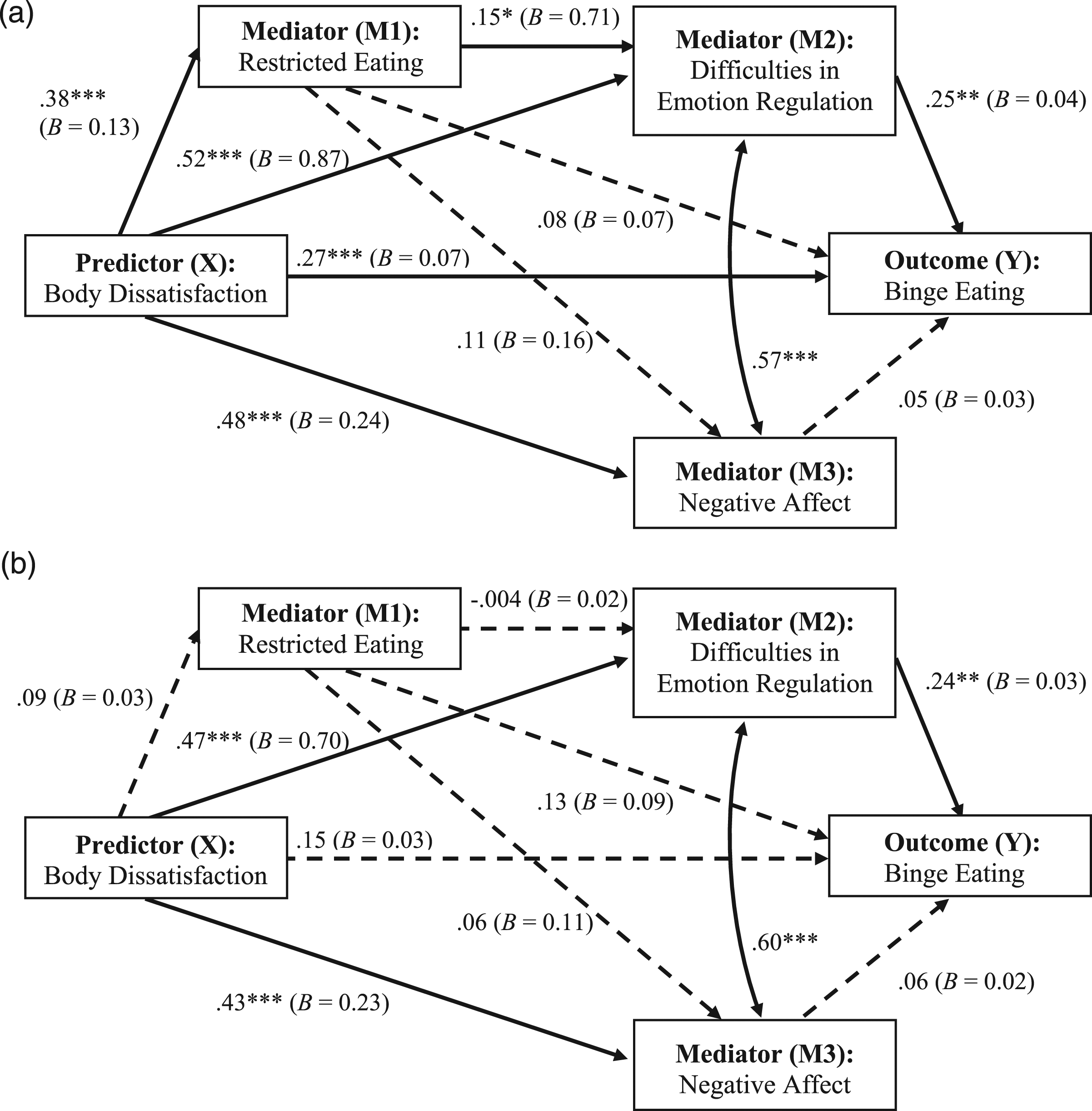
Discussion
We sought to test three mediation hypotheses as well as explore gender differences between women and men in a test of a modified dual pathway model, with difficulties in emotion regulation in the place of negative affect. We made the argument that the management of negative affect (i.e., difficulties in emotion regulation) would be a more salient variable than simply the presence of negative affect in predicting binge eating. Overall, difficulties in emotion regulation were a significant mediator in the modified dual pathway model, although there were notable gender differences for these findings.
The first mediation hypothesis (i.e., body dissatisfaction → restricted eating → binge eating) was not supported for women or men, although the zero-order correlations between restricted eating and binge eating were significant for both. After controlling for the effects of body dissatisfaction and difficulties in emotion regulation, the link between these variables became nonsignificant in the model. The lack of support for this mediation is consistent with previous studies (Ouwens et al., 2009; Stice, 2002). Interestingly, body dissatisfaction was significantly associated with restricted eating for women, but was not significant for men. This may be because men endorse a drive for muscularity as well as thinness (Morrison et al., 2003). Men in this sample may have been less likely to restrict eating in response to body dissatisfaction owing to a desire to gain mass. These results are also consistent with results found by Markey and Markey (2005), who observed that although women, regardless of BMI, engaged in dieting in order to achieve a thin ideal, men in their sample had greater BMI and yet engaged in less restricted eating. Therefore, men may be less likely to restrict their food intake in response to body dissatisfaction due to different reasons to engage in this behavior.
The second mediation hypothesis (i.e., body dissatisfaction → restricted eating → difficulties in emotion regulation → binge eating) was supported for women but not for men. These results provide evidence for difficulties in emotion regulation being an important factor to examine in the development of binge eating with notable gender differences. For women, restricted eating related to body dissatisfaction could be associated with psychological vulnerabilities, such as impaired concentration and emotional vulnerability due to physiological changes (Haynos & Fruzzetti, 2011). These vulnerabilities can in turn relate to difficulties in emotion regulation, which can then result in the use of binge eating in an attempt to regulate their emotions.
However, men might not have responded to body dissatisfaction with restricted eating, followed by difficulties in emotion regulation because they may have desired to gain weight (Morrison et al., 2003) or engaged in other weight control behaviors, such as excessive exercise (Strother et al., 2012; Weltzin et al., 2005). Therefore, restricted eating was not significantly related to difficulties in emotion regulation for men. Additionally, it is important to note that all direct paths to and from restricted eating were not significant for men. These results imply that men might have different mediation pathways (e.g., through internalized bullying) for the link between body dissatisfaction and binge eating. For example, men with body dissatisfaction might be vulnerable to internalizing previous bullying experiences related to their body and may respond by manipulating their bodies to become larger (Strother et al., 2012).
The third mediation hypothesis (i.e., body dissatisfaction → difficulties in emotion regulation → binge eating) was supported by the results for women and men. These results build upon Sim and Zeman’s (2005) results from a sample of adolescent girls in order to illustrate the ways in which difficulties in emotion regulation appear to be associated with binge eating as a means of coping with the painful emotions related to body dissatisfaction. Women and men who are dissatisfied with their bodies may have challenges with emotion regulation. Therefore, they may be vulnerable to engaging in binge eating as a maladaptive emotion regulation strategy (Whiteside et al., 2007). The post hoc analysis demonstrated that, after setting up negative affect and difficulties in emotion regulation to control for one another, the hypotheses supported by the modified model still held, whereas none of the mediations through negative affect were significant. Therefore, it appears that difficulties in emotion regulation can be an important factor in explaining how body dissatisfaction relates to binge eating over and above negative affect, further echoing previous research (Ambwani et al., 2014; Lavender & Anderson, 2010).
Altogether, these results indicate that the original dual pathway model for binge eating may not fully explain how body dissatisfaction is related to binge eating. In particular, negative affect may not provide a complete picture. The modified dual pathway model, which includes how negative affect is managed through abilities, including awareness of emotions and resisting impulsive behaviors, appears to better explain how body dissatisfaction is related to binge eating. These results contribute to the literature about binge eating by supporting difficulties in emotion regulation as an important factor. Furthermore, we suggest that future dual pathway model research examining binge eating behaviors should incorporate emotion regulation difficulties.
Limitations
There were several limitations to this study. First, there may have been a self-selection bias for participants, as students who were interested in the topic of body image may have been more likely to participate. Second, this was a nonclinical sample and future research should try to examine the modified model in a clinical sample to explore the role of difficulties in emotion regulation for people with eating disorders. Third, the measures in this study were self-report, so participants may have been vulnerable to socially desirable responses. Therefore, future studies should consider social desirability and examine whether results are consistent after controlling for this factor. Fourth, the Eating Disorder Diagnostic Scale used the DSM-IV criteria for binge eating. Although the only difference between the items on this scale and the DSM-5 (American Psychiatric Association, 2013) criteria is the length of time (i.e., past 6 months vs. 3 months), this may have affected the self-reported binge eating scores.
Fifth, data were collected from a predominately White, Midwestern university. The lack of racial diversity in this sample may prevent these results from being generalized to other college students. For instance, empirical results consistently report that African American women experience less body dissatisfaction and endorse preference for larger bodies compared to women of other racial groups (Altabe, 1998; Padgett & Biro, 2003). Shuttlesworth and Zotter (2011) found that African American women with a stronger ethnic identity that included valuing larger bodies were less likely to engage in restricted eating but more likely to engage in binge eating. These studies were cross-sectional, limiting the ability to identify causal relationships among the variables. Future research can implement cross-lagged models to examine causal directional paths among variables. Finally, we suggest that other researchers replicate our model to ensure our results were not due to this specific sample only.
Implications for Practice, Advocacy, Education/Training, and Research
These results have several implications for counselors. However, given our predominantly White sample, these implications may be limited to White college students. First, our results indicated that the development of binge eating looks different for women and men. It is important for counselors to recognize these gender differences when assessing risk for binge eating. For instance, contrary to women, restricted eating for men was not associated with body dissatisfaction, negative affect, emotion regulation difficulties, or binge eating. Therefore, restricted eating may not be as salient a risk factor for men. Second, the mediation results indicating that difficulty in emotion regulation was still a significant mediator but negative affect was not after controlling for the other for both women and men suggest that counselors should focus on not just identifying negative affect related to body concerns, but more importantly, assess how clients identify and deal with their emotions. We suggest that counselors can utilize a framework that prioritizes emotion regulation difficulties over negative affect when conceptualizing clients’ problems and developing treatment goals.
College men may benefit from advocacy efforts to spread awareness about binge eating for this group. For instance, outreach presentations can be given to student-athletes, fraternities, and student organizations. Since eating problems may be thought of as “women’s disorders” (Strother et al., 2012), men may benefit from the knowledge that they can also experience difficulties related to binge eating. Outreach efforts can normalize eating concerns men may have and reduce their shame for having a “woman’s disorder,” hopefully increasing their chances of seeking support. Additionally, college men can be made aware that if they have difficulty regulating their emotions in response to body dissatisfaction, they can be at risk for binge eating.
For education and training, clinicians who work with these concerns can be educated about how to identify and work with emotion dysregulation. One option is to use the Difficulties in Emotion Regulation Scale (Gratz & Roemer, 2004) with clients to track their treatment progress. Clinicians can also be trained on how to use emotion regulation interventions for those at risk. Clyne and Blampied (2004) implemented an emotion regulation skills training for women with a binge eating disorder. At follow-up, participants no longer met criteria for a binge eating disorder. Clinicians who effectively teach these skills may aid their clients who are at risk for eating disorders. Furthermore, counseling trainees, who are unlikely to treat eating disorders early in their training, can be taught how to use this emotion dysregulation framework as they begin to work with clients who present with body-related and eating concerns. For instance, they can conceptualize that a woman who counts calories may be at risk to restrict her food intake and be vulnerable to experiencing strong feelings.
The current study indicates directions for future research. First, the results support difficulties in emotion regulation as a construct to further examine in the development of binge eating. This study hypothesized and found support for a path from restricted eating to difficulties in emotion regulation for women. It still remains to be examined whether difficulties in emotion regulation may predict restricted eating. Future research can examine the directions of causality among these variables using a cross-lagged model with longitudinal data. Alternative models depicting a circular relationship among restricted eating, difficulties in emotion regulation, and binge eating should also be tested. Second, the result that the modified model was not gender invariant indicates further avenues to be explored for the development of binge eating in men. For example, men endorse different reasons for engaging in restricted and binge eating compared to women (Markey & Markey, 2005). The result that restricted eating was not a significant mediator for men provides opportunities to examine other mediators, given that the direct association between body dissatisfaction and binge eating was still significant in the modified model. Other mediators such as bullying and substance use are also worth examining (Strother et al., 2012; Tanofsky et al., 1997). For instance, it may be possible that men who use anabolic steroids to gain muscle mass are at risk for binge eating (Baum, 2006).
Overall, this study provides evidence for the utility of difficulties in emotion regulation as a component of the dual pathway model for binge eating. These results provide important insights into understanding the relationships among predictors of binge eating for both women and men.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Notes
This study was presented at the 128th Annual Convention of the American Psychological Association, August 2020, Washington, D.C.