
Abstract
Supervisees’ experiences in supervision vary remarkably. To capture such variability, Ellis and colleagues offered a framework for understanding and assessing inadequate, harmful, and exceptional supervision. Although their framework was supported, it did not offer a nuanced understanding of these supervision experiences. Using consensual qualitative research–modified, this study sought to obtain a rich description of inadequate, harmful, and exceptional supervision. Participants (N = 135) were presented with definitions and provided responses (n = 156) to open-ended questions describing their inadequate (n = 63), harmful (n = 30), and/or exceptional (n = 63) supervision experiences. Supervisees reporting harmful experiences described supervisors as neglectful and callous, whereas inadequate supervision reflected inappropriate feedback, unavailability, and unresponsiveness. Conversely, exceptional supervision involved safety, clinical paradigm shifts, and modeling specific techniques or theories. Implications for supervision research, theory, and practice are discussed.
We identified themes from trainees’ descriptions of their inadequate, harmful, and exceptional experiences in clinical supervision. The findings offer a nuanced understanding of supervisees’ lived experiences, illustrating how clinical supervisors went awry or went above and beyond, and suggesting strategies for promoting exceptional supervision and preventing harmful and inadequate supervision.Significance of the Scholarship to the Public
Introduction
Clinical supervision is the primary vehicle through which trainees acquire the necessary competencies for intervening effectively with diverse populations (Bernard & Goodyear, 2019). Thus, clinical supervisors play a critical role in fostering the development of tomorrow’s helping professionals (American Psychological Association [APA], 2015; Fouad et al., 2009) and yet, research suggests that trainees’ experiences with their supervisors and in supervision vary to a remarkable degree ( Ellis et al., 2014, 2015a). Moreover, across these varied experiences, supervisees seem overwhelmingly uninformed about what to expect from supervision and their supervisors (Cook & Ellis, 2021; Ellis et al., 2015a, 2015c). In fact, recent research suggests that supervisees’ perceptions of the quality of their supervision differs in significant ways, based on agreed upon behaviorally-based, objective criteria (Cook & Ellis, 2021; Ellis et al., 2014). Given the implications of such variability for both supervisees and their clients, significant empirical attention has been devoted to identifying the defining characteristics of both negative and positive supervisory experiences (e.g., Breese et al., 2012; Ellis et al., 2014, 2015c; Hendricks & Cartwright, 2018; Worthen & McNeill, 1996). A central theme is that a strong supervisory working alliance, defined as the emotional bond between the supervisor and supervisee, and their mutual agreements on the tasks and goals of supervision (Bernard & Goodyear, 2019).
Indeed, supervisees with negative supervision experiences tended to rate their alliances as weaker (e.g., Ladany et al., 2013; Ramos-Sánchez et al., 2002), and associated with more role conflicts and ambiguity (Ladany & Friedlander, 1995), more supervisor ethical transgressions (Ladany et al., 1999), and lower supervisor cultural competence (Hendricks & Cartwright, 2018; Inman, 2006). Moreover, in Magnuson et al.’s (2000) study on lousy supervision, supervisees described supervisors as incompetent, overly task-focused, insensitive to their developmental stage, and highly critical (cf. APA, 2015). Others found that supervisor dismissiveness and lack of empathy were related to counterproductive events (Gray et al., 2001) and conflict in supervision (Nelson & Friedlander, 2001). These supervisors were reported to be deficient in meeting the standards for adequate supervision established by the Competency Benchmarks: A Model for Understanding and Measuring Competence in Professional Psychology Across Training Levels (Benchmarks henceforth, Fouad et al., 2009) and the Guidelines for Clinical Supervision in Health Service Psychology (Guidelines henceforth, APA, 2015), thus failing to fulfill their dual responsibilities to supervisees and their clients. Overall, these results suggest that supervisors can fail their supervisees in multiple ways (Ladany, 2014). Such failures impede trainees’ disclosure in supervision (e.g., Mehr et al., 2015), self-efficacy (Gray et al., 2001), satisfaction with supervision (Ladany et al., 1999), and even whether they remain in the field (Ellis, 2017).
Conversely, supervisees reporting positive supervision experiences benefit from productive and strong supervisory working alliances (Bernard & Goodyear, 2019; Kangos et al., 2018). Supervisees in these optimal relational contexts have described their supervisors as credible and knowledgeable (Ladany et al., 2013), invested in supervision, committed to working through conflict, and proactive in initiating discussions about culture and the inherent power differential in supervision (Nelson et al., 2008). These supervisors also seem adept at providing constructive and developmentally appropriate feedback (Kangos et al., 2018), thereby striking an optimal balance between challenge and support in supervision (De Stefano et al., 2017). Supervisees with exemplary supervision experiences felt empowered and respected, articulated their relationships in terms of “warmth, acceptance, respect, understanding, and trust” (Worthen & McNeill, 1996, p. 26), and reported increased clinical learning, professional identity, and self-confidence (Breese et al., 2012; Ladany et al., 2013; Worthen & McNeill, 1996).
Although the extant research has facilitated an understanding of the nature and range of possible supervision experiences, the conceptual ambiguity in the literature is problematic. Per Ellis et al. (2014), different terms have been used to describe the phenomenon of supervision going awry, including negative supervision experiences (Ramos-Sánchez et al., 2002), ineffective supervision (Ladany et al., 2013), counterproductive events (Gray et al., 2001), and lousy supervision (Magnuson et al., 2000). The literature on superior supervision experiences is also equivocal, describing wise supervisors (Nelson et al., 2008), and effective (Ladany et al., 2013), excellent (Breese et al., 2012), and ideal (Hendricks & Cartwright, 2018) supervision experiences. The plethora of terms describing supervision experiences impedes efforts to consolidate the findings and compare them across studies (Ellis et al., 2014), as well as assess these experiences per the Benchmarks (Fouad et al., 2009) and Guidelines (APA, 2015).
Inadequate, Harmful, and Exceptional Supervision
To address these issues, Ellis (2001) put forth and subsequently tested (Cook & Ellis, 2021; Ellis et al., 2014, 2015a) a unified framework for understanding and assessing inadequate and harmful supervision experiences. Inadequate supervision constituted instances when the supervisor is unable or unwilling to enhance the professional functioning of the supervisee, monitor the quality of the professional services offered to the supervisee’s clients, serve as a gatekeeper to the profession (Bernard & Goodyear, 2019)… or fails to provide the minimal level of supervisory care as established by his or her discipline or profession (Ellis et al., 2014, p. 439).
Harmful supervision reflected supervisory practices that result in psychological, emotional, and/or physical harm or trauma to the supervisee… The two essential components of harmful supervision are: (a) that the supervisee was genuinely harmed in some way by the supervisor’s behaviors, or (b) the supervisor’s behavior is known to cause harm, even though the supervisee may not identify the behaviors as harmful (Ellis et al., 2014, p. 440).
Sometimes described as “wow supervision that was the best, profound, powerful, exceptional, or inspirational” (Ellis et al., 2015a, p. 623). Ellis et al., 2015a conceptualized exceptional supervision as a composite consisting of supervisors (a) clearly exceeding criteria for minimally adequate supervision; (b) implementing extant clinical supervision best practices; (c) developing and maintaining a collaborative professional supervisory relationship that maintains appropriate professional boundaries and exemplifies humility, respect, genuineness, mutual caring, transparency, and flexibility; and (d) attaining and using a deep understanding of and respect for supervisees’ (and their clients’) cultural identities to promote their sense of empowerment, profound insight, and professional development. For context, Ellis et al. defined minimally adequate supervision based on and consistent with the criteria delineated in the clinical supervision standards (e.g., supervisor meets regularly with supervisee and offers formative and summative feedback; APA, 2015) and the Benchmarks (Fouad, 2009). Thus, adequate supervision is a prerequisite for exceptional supervision.
In addition, Ellis et al.’s (2014) empirically derived taxonomy differentiates de facto (i.e., supervisor behaviors or actions meet specific objective criteria) from self-identified supervision experiences (i.e., identified by supervisees). The taxonomy includes 16 de facto inadequate supervision descriptors, 21 de facto harmful supervision descriptors (Ellis et al., 2014), and 36 de facto exceptional supervision descriptors (Ellis et al., 2015a; for abbreviated descriptors see Ellis et al., 2014, 2015a). Ellis and colleagues also denoted harmful classification criteria that were more protective of supervisees (vs. supervisors) such that any occurrence of harmful supervision was classified as de facto harmful supervision—supervisee protective, a rating of 2 (rarely describes) or greater on a 7-point Likert-type scale, from 1 (not at all describes) to 7 (totally describes). For context, this approach was distinguished from a supervisor conservative one, where a rating of 5 (often describes) or greater was required to meet criteria for harmful supervision. When a supervisee protective approach was applied, the rates of de facto current and overall harmful supervision nearly doubled. Ellis et al., 2014, 2015a; and Ellis et al., 2015a also observed large discrepancies between supervisees’ perceptions of the supervision they were currently receiving (self-identified inadequate, harmful, or exceptional supervision) and the supervision they were actually receiving based on the de facto classifications.
Research Goals and Questions
Ellis et al., 2014, 2015a investigations advanced the field’s knowledge of supervision experiences. Specifically, they put forth and subjected to empirical scrutiny a taxonomy with operational definitions of inadequate, harmful, and exceptional supervision, which had not existed previously. Indeed, empirically derived supervision constructs and frameworks have been rare (Bernard & Goodyear, 2019). Although Cook and Ellis (2021) and the studies by Ellis and colleagues highlighted the prevalence of inadequate, harmful, and exceptional supervision as well as the discrepancies in supervisee self-identified experiences compared to the de facto criteria, they did not offer a nuanced understanding of these subjective experiences collectively. Rich descriptions of these phenomena may inspire training environments that prevent inadequate and harmful supervision and foster exceptional supervision, meeting supervisees’ and clients’ needs more effectively (APA, 2015; Fouad et al., 2009).
Building on the work of Ellis and colleagues, we aimed to: (a) qualitatively explore and describe supervisees’ subjective experiences of receiving inadequate, harmful, and exceptional supervision collectively; and (b) triangulate our qualitative findings with those of Ellis and colleagues to evaluate their framework and refine our understanding of the phenomena of interest. The broad question guiding this study was, what is the nature of supervisees’ supervision experiences? More specifically, we asked: (a) How do supervisees describe their inadequate, harmful, and exceptional supervision experiences? (b) What supervisor actions and inactions do supervisees characterize as inadequate, harmful, and exceptional? and (c) How do our qualitative findings map onto the quantitative results of the previous research by Ellis and colleagues?
Method
Research Design
Consensual Qualitative Research-Modified (CQR-M; Spangler et al., 2012) was used to understand the breadth of supervisees’ subjective experiences of inadequate, harmful, and exceptional supervision as defined by Ellis et al. (2014). CQR-M is an exploratory and discovery-oriented approach that is optimal for analyzing open-ended responses (Spangler et al., 2012). Like consensual qualitative research (Hill et al., 1997), CQR-M explores participants’ experiences and grounds the analysis and the findings in their words. Beyond its exploratory purposes, it is also well-suited for methodological triangulation, which incorporates multiple views to offer a deeper understanding of specific phenomena (Denzin, 1978). Given our dual aims of description and triangulation, CQR-M was ideal for this study.
Participants
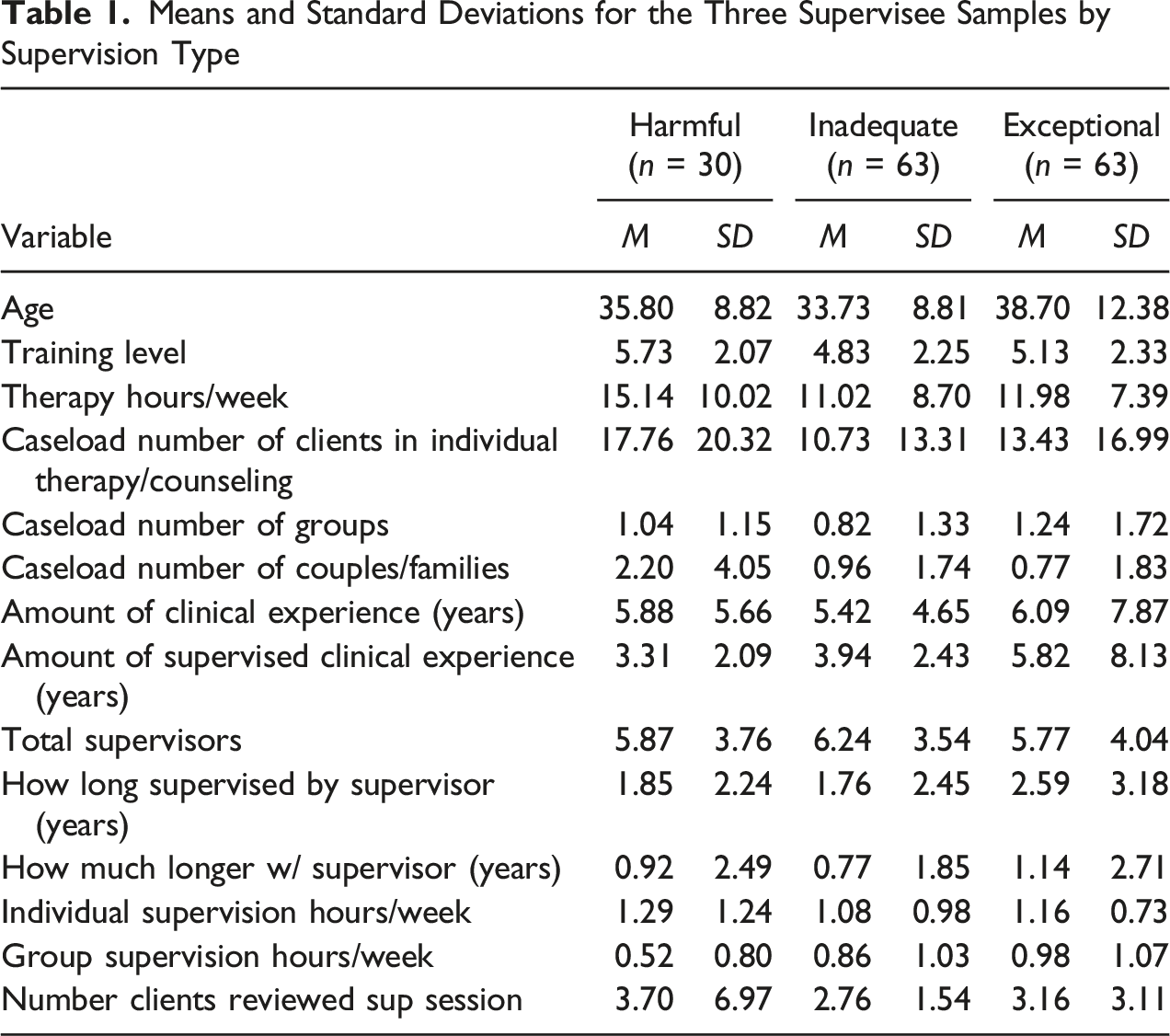
Means and Standard Deviations for the Three Supervisee Samples by Supervision Type
Percentages and Frequencies for the Three Supervisee Samples by Supervision Type
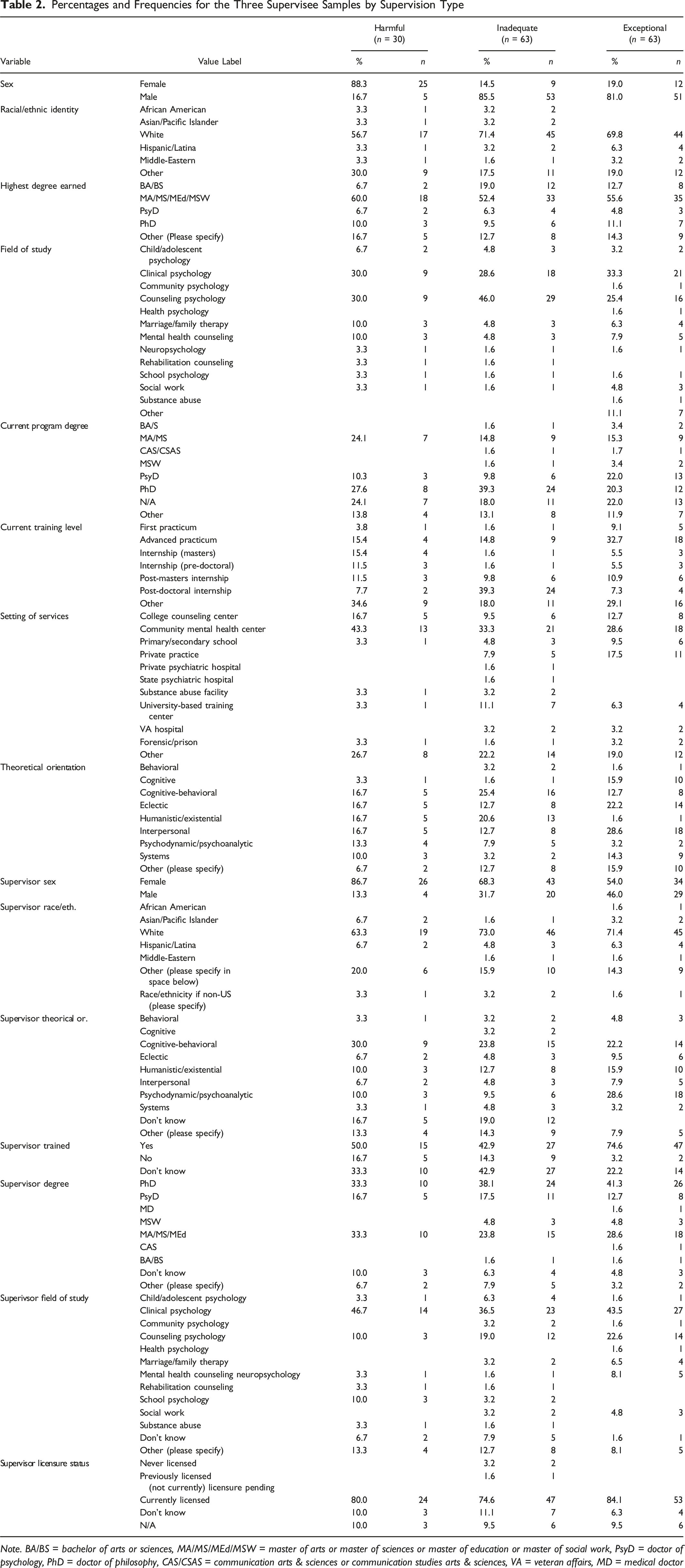
Note. BA/BS = bachelor of arts or sciences, MA/MS/MEd/MSW = master of arts or master of sciences or master of education or master of social work, PsyD = doctor of psychology, PhD = doctor of philosophy, CAS/CSAS = communication arts & sciences or communication studies arts & sciences, VA = veteran affairs, MD = medical doctor
Analytic Team and Researcher Assumptions
Two faculty members (a cisgender White heterosexual female assistant professor and a cisgender White heterosexual male full professor) and four cisgender doctoral students (a fourth-year Black/African American female, a second-year biracial Black/Hispanic female, a second-year White male, and a third-year White female) in counseling psychology programs located in public universities in the Northeast United States served as judges. Three separate coding teams, each with three individuals, analyzed the inadequate, harmful, and exceptional supervision data, respectively. Each team was consistent in terms of gender, race, and experience level. Only the first two authors had prior consensual qualitative research experience. Team members varied in their familiarity with the clinical supervision literature, ranging from having published extensively to being recently introduced to this research. However, all team members shared a basic understanding of inadequate, harmful, and exceptional supervision. In discussing our assumptions, we identified our own compassion for supervisees, and our commitment to preventing harmful and inadequate supervision. We also believed that exceptional supervision is empowering whereas harmful supervision often involves an abuse of power, stemming from our own supervision experiences. Finally, because our negative experiences were more accessible, we wondered if exceptional supervision was rarer. In acknowledging these assumptions, we strived to make their influence on the analysis transparent.
Measures
Information about participants and their supervisors (e.g., age, gender, race and ethnicity, years of clinical experience and supervised training) was obtained via a demographic questionnaire. Participants who self-identified as currently receiving inadequate, harmful, or exceptional supervision based on the Ellis et al. (2014) definitions were invited to elaborate on their experiences via open-ended questions. Specifically, after endorsing that they received inadequate, harmful, or exceptional supervision, participants were asked “what did the supervisor do?” to make the supervision experience inadequate, harmful, or exceptional. Participants who indicated that they received harmful supervision were also asked “how were you harmed?”
Data Collection
We invited participants, via emails to programs and professional organization listserv postings, to take part in a larger study “to develop and test a new measure of the clinical supervision relationship” (recruitment materials). Inadequate, harmful, and exceptional supervision were not mentioned. Materials included a cover letter with a link to a password-protected website, the informed consent, the questions presented in randomized order, and a demographics questionnaire, which included the inadequate, harmful, and exceptional supervision questions, and was always presented last. Over 93% completed the materials in less than 25 minutes. A $25 gift card to Amazon.com was awarded to one out of every 25 participants.
Analytic Process
The analytic process for CQR-M parallels consensual qualitative research (Hill et al., 1997; Hill, 2012), albeit with some departures (Spangler et al., 2012). A team of coders and judges familiar with the constructs of inadequate, harmful, and exceptional supervision was selected. Next, the first author trained the coders in CQR-M and provided ongoing consultation. The open-ended questions defined the domains: inadequate, harmful, and exceptional. Coders on each domain team then independently condensed participant statements and met to achieve consensus. Disagreements about coding decisions were processed as a group to ensure that all members’ perspectives were considered and included. Doing so helped to mitigate against any experiences of disempowerment, particularly for those with less positional power, such as students (Hill, 2012). Next, coders independently reviewed each case to develop categories and subcategories, meeting to establish consensus at each step. Consistent with this methodology (Hill, 2012), categories facilitated an understanding of how the data clustered together thematically, and subcategories helped to describe the data further within larger categories. Per Spangler et al. (2012), core ideas were not constructed; given the simplicity of the data, they were put into categories directly. Consensus meetings involved lengthy discussions about whether the categories and subcategories accurately captured the meaning of participants’ experiences as reflected in their responses, as well as refining the categories and subcategories. Smaller categories were combined into larger ones where possible. A category was deemed sufficient if it reflected at least 10% of responses. A master coding table (participant identifier, condensed statements, categories, subcategories, and frequencies) served to organize the data. Consistent with CQR-M, we used proportions (vs. general, typical, variant).
Once each team achieved consensus, we met as a larger group to discuss the findings. We discovered that there was overlap in the category labels for the harmful and inadequate supervision categories (e.g., supervisor lack of support and supervisor unsupportive). To resolve the overlap, representatives from each domain team compared the responses within similarly named categories, and then offered suggestions with their respective domain teams, who refined or relabeled the categories. Although not required for CQR-M, this process served as an audit to ensure the integrity of the analytic process and bolster the trustworthiness of the findings.
Findings
We describe herein the categories that emerged from supervisees’ descriptions of their inadequate, harmful, and exceptional supervision experiences. We endeavored to stay close to the responses to avoid making assumptions about participants’ feelings, thoughts, and contexts. No more than one illustrative example was taken from each participant’s open-ended response. To avoid redundancy, we address triangulation in the Discussion section, per Hill (2012).
Harmful Supervision
Categories, Percentages, and Core Ideas
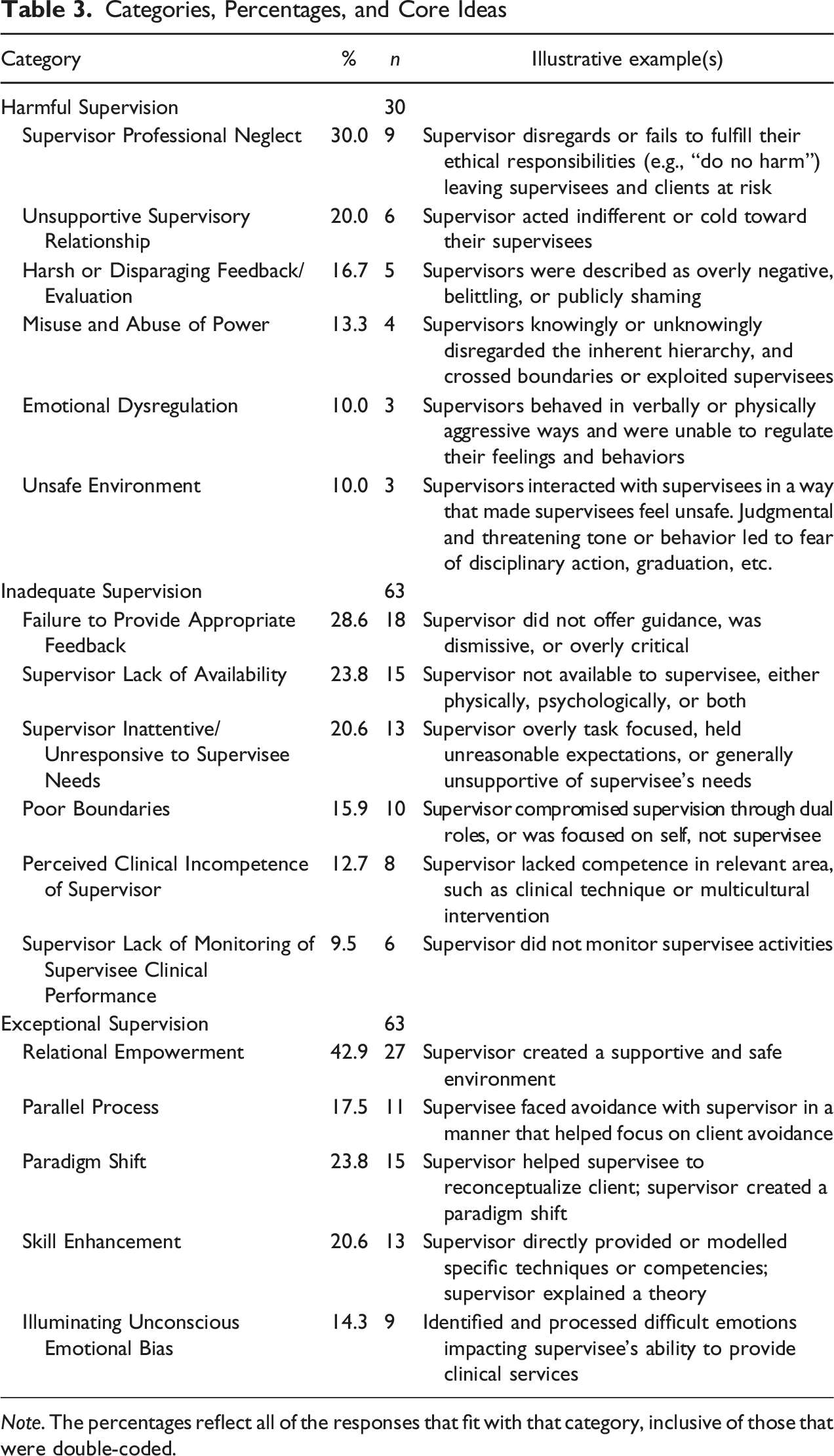
Note. The percentages reflect all of the responses that fit with that category, inclusive of those that were double-coded.
Supervisor Professional Neglect
Responses categorized as Supervisor Professional Neglect (30.0%) moved beyond supervisors who were simply not available to supervisors who completely disregarded or neglected to fulfill professional and ethical responsibilities, resulting in harm to the supervisee. Specifically, supervisors neglected their ethical duty to “do no harm” (APA, 2015), risking supervisee and client welfare. Distinct from the inadequate category of Supervisor Lack of Availability, these experiences were characterized by a pervasive supervisory absence, which consistently deprived supervisees of professional and emotional support, and often required supervisees to navigate novel clinical challenges on their own, compromising not just their development, but also their well-being and that of their clients. For example, one supervisee described how their supervisor neglected their professional and ethical responsibilities to provide critical clinical information in which the supervisee experienced a “physical assault resulting from the supervisor directing me to immediately see a client that had been double booked, me not knowing the client’s history/presenting problem, and ‘triggering’ the client’s PTSD [posttraumatic stress disorder] symptoms.”
Another participant described a supervisor’s “inappropriate allocation of some clientele in terms of my areas of skill/interest/competence” and an “inability to discuss methodologies as [the] supervisor has no prior application thereof” due to the supervisor favoring “non-evidence-based approaches.” The supervisor neglected their professional and ethical responsibility to provide clinical experiences and expertise that align with the supervisee’s training needs, thus neglecting the supervisee’s professional growth, and provoking a “sense of isolation” and the “inability to effect change to the perceived harmful dynamic” because they did not know how to treat a client in an empirically grounded way. The supervisor’s failure to teach empirically validated practices harmed the supervisee, leading them to seek “external supervision to address [the] harmful aspects of this situation.” Other instances of supervisors neglecting their professional duties resulted in similar patterns of harm. One supervisee experienced “shady billing practices, [and a] lack of supervision… [and] could not complete [their] post-doctoral position with this person and resigned,” whereas another was “unable to assist [in] my decision process [about treatment] with a severely depressed client… [and I] sought outside supervision.” The supervisors depicted here neglected their responsibility to promote supervisee growth. Thus, a persistent pattern of supervisory negligence or absence characterized supervision. Whether as an absence from their professional role, or an inability to provide education and guidance to support competency development, supervisors thwarted their supervisees’ development to the point of harm.
Unsupportive Supervisory Relationship
The second most prominent harmful supervisee experience (20.0%) described relationally and emotionally unsupportive supervisors. We differentiated Supervisor Professional Neglect (a failure to fulfill one’s professional responsibilities to provide supervision) from Unsupportive Supervisory Relationship (negative emotional experiences within the supervisory relationship and working alliance). In essence, supervisors were depicted as oblivious or insensitive to supervisees’ emotional needs, resulting in harm. For instance, one supervisor, “was not willing to work with a life-threatening medical illness that I had and reduce [my] workload for a period of time.” The supervisor’s unresponsiveness to the supervisee’s urgent medical needs precipitated ruptures in their alliance, conveyed a sense of callousness vis-à-vis the supervisee’s well-being, and “negatively impact[ed] the [supervisee’s] career trajectory.” Another supervisor “did not facilitate me to overcome challenges of giving an intervention to a client,” but instead advised them to “change the intervention entirely” and appeared “disinterested in supervision.” The lack of guidance for the supervisee’s choice of intervention left the supervisee “feeling more negative about the profession, [and] feeling more guilt/shame about the poor quality of the supervisory relationship.” Finally, one supervisee was placed on “sharp restrictions on contact during a time when [I] was also dealing with difficult personal issues” such that the supervisor “only communicated once a week when [they] had been available to communicate as needed throughout the week,” which “damaged trust in [our] supervisory relationship” and triggered feelings of “uncertainty in how [my] supervisor perceives me on a daily basis.” The supervisor created relational distance right when the supervisee needed more support than usual due to personal struggles, thus harming the supervisee.
Harsh or Disparaging Feedback or Evaluation
Supervisees (16.7%) described harmful interactions where supervisors excessively criticized, belittled, and/or publicly shamed or humiliated supervisees. Although constructive feedback is a vital component of training, these instances of harsh or disparaging feedback often resulted in supervisee self-doubt, insecurity, or self-silencing, rupturing the supervisory relationship and causing harm. One supervisee “[felt] constant criticism” and was not “provided with guidance or positive feedback.” They felt “deflated and insecure after each supervision session” and “unable to ask questions.” The supervisee was silenced and paralyzed by the supervisor’s unduly harsh feedback, resulting in ongoing injury to the supervisee’s confidence and leaving them unable to benefit from supervision. Similarly, one supervisee said, “I do not feel comfortable asking questions or asking for help from the supervisor” because the supervisor “publicly humiliated me in front of colleagues for asking a question.” The supervisee’s relationships with colleagues and willingness to seek guidance were also negatively impacted.
Harsh or disparaging feedback can leave supervisees doubting their clinical skills. Indeed, one supervisee indicated that “after a staff training [the supervisor] told me in supervision that she would never want any of us (the staff) to be her therapist because she felt we were all judgmental.” Even though the supervisee had been “trying to build my confidence in supervision, being told that made it really hard to believe what I am doing is any good.” Thus, harsh supervisor feedback can undermine supervisees’ self-efficacy and compromise their desire to seek further supervisory feedback and evaluation.
Misuse and Abuse of Power
Supervisors’ misuse and abuse of power (13.3%) stems from the inescapable hierarchy within pre-licensure clinical supervision. Supervisees described supervisors who intentionally or unintentionally abused the power differential by exploiting supervisees, crossing boundaries, and taking advantage of their positions of authority. For example, one supervisee noted that the supervisor “initiated a sexual relationship” with them. Another participant described an authoritarian supervisor, “it was her way or the highway,” noting that “even if I disagreed with how to manage a patient I went along with [the supervisor’s] suggestion out of fear of being negatively evaluated or terminated from the program.” This supervisee reported, “[the supervisor] was the principal and I was a learner waiting to be disciplined for incorrect work,” leaving the supervisee feeling “anxious and afraid of other supervisors before even being supervised by them.” Another supervisee indicated that their supervisor forced them to take an incomplete because “she refused to review and sign a testing report within an appropriate time-frame and when I tried to discuss this with her, she terminated supervision and sent a very negative evaluation to my practicum supervisor.” Here, the supervisor’s abuse of power directly and negatively impacted the supervisee’s career trajectory, forcing the supervisee to “engage in damage control to protect me from program disapproval.”
Emotional Dysregulation
Supervisors (10%) were described as unable to control and regulate their emotions, acting with verbal or physical anger and aggression toward the supervisee. Supervisees felt fearful of erratic, volatile, and unpredictable supervisors. One supervisee stated that “[the supervisor] would deny she was upset but throw things around her office until I broached the topic with her, and [then] she would discuss her insecurities about [my] intelligence and respect for her.” This supervisor’s inability to self-regulate their behaviors resulted in “extreme anxiety” for the supervisee, who “began taking medication before supervision to manage panic attacks.” Another supervisee noted “[my supervisor] projected her own issues on to me [and] failed to realize how she was projecting.” The supervisor spoke “with much contained anger in front of [the supervisee’s] colleagues.” As a result, they felt “so belittled I would shake during supervision.”
Unsafe Environment
Supervisees in this category (10.0%) explicitly identified threats to their safety. The unsafe environment often involved feeling shamed, and fearful of disciplinary action that permeated the supervisory experience. Distinct from other forms of harmful supervision, supervisees here indicated a need to be hypervigilant—their career was in peril. An unsafe environment entailed being berated or punished: “[my supervisor] attacked my perceptions of a group supervision session that made me uncomfortable… I felt judged and not safe to share such things in the future.” Often, the lack of safety was tied to their professional position being at risk. One supervisee opined, “[I am] afraid of her, afraid of doing something wrong, it doesn’t feel like a safe space to bring personal [and] professional issues.” For another supervisee, their supervisor was directly involved in staff cutbacks… [and] told on a number of occasions privately not to speak about it (i.e., the impact of staff cutback) as it got staff riled up… [I was] silenced and threatened with disciplinary action if I did not continue to concurrently accept an increase in my caseload [due to another staff’s maternity leave].
Elaborating on their lack of safety, this supervisee compared their experience to “playing chess in interactions with my supervisor.”
Inadequate Supervision
Inadequate supervision occurs when: [the] supervisor is unable, or unwilling, to meet the criteria for minimally adequate supervision, to enhance the professional functioning of the supervisee, to monitor the quality of the professional services offered to the supervisee’s clients, or to serve as a gatekeeper to the profession … or fails to provide the minimal level of supervisory care as established by his or her discipline or profession. (Ellis et al., 2014, p. 437)
Here, supervisees collectively described subpar experiences without the consequences of direct harm to them or their clients (cf. harmful supervision). The six emerging categories were: Failure to Provide Appropriate Feedback, Supervisor Lack of Availability, Supervisor Inattentive or Unresponsive to Supervisee Needs, Poor Boundaries, Supervisor Lack of Monitoring of Supervisee Clinical Performance, and Perceived Clinical Incompetence of the Supervisor. Five statements fit in multiple categories within this domain.
Failure to Provide Appropriate Feedback
Supervisees (28.6%) reported a lack of guidance (e.g., not receiving feedback when it was needed or receiving unhelpful feedback) or supervisors providing dismissive or overly critical feedback. Unlike the harmful Harsh or Disparaging Feedback/Evaluation category, supervisees did not report harm because of the (lack of) feedback. To illustrate, three supervisees, respectively, described their supervisors as (a) “not challeng[ing] me, agrees with everything, does not offer any advice or solutions to work with clients;” (b) “overly-challenging, sometimes vague in her responses;” and (c) “[d]idn’t let me get a word in edge wise and actually spoke over me when I started saying something. I brought up an issue and he didn’t ask my thoughts on it or take my opinion into consideration but simply told me what to do as a command.” In these cases, supervisors failed to provide appropriate feedback that was geared toward furthering supervisee professional competency development.
Supervisor Lack of Availability
Supervisees (23.8%) described supervisors that were physically and/or psychologically unavailable. One participant stated “[my supervisor] did not always keep supervision appointments, sometimes very sleepy, distracted during supervision, never invited discussion about the nature of supervision or my reactions to it.” This supervisor was physically unavailable by not providing supervision as scheduled. Another supervisee’s supervisor “skipped 6 weeks of supervision due to personal reasons, did not provide a replacement,” describing a lack of physical availability without arranging for alternative forms of support and oversight. Yet another supervisee recounted how the
[s]upervisor would cancel scheduled supervision appointments without notifying me. Supervisor would sit in supervision and allow herself to be distracted by staff interruptions, not being prepared for the meetings, unfocused, arrive late for supervision, or would only meet for five minutes.
As a result of this lack of availability, supervisees felt unsupported and lost in terms of how to intervene with their clients.
Supervisor Inattentive or Unresponsive to Supervisee Needs
Supervisors often (20.6%) failed to recognize or meet the supervisee’s needs. Supervisors were depicted as overly task-focused, holding unreasonable expectations, and/or as generally unsupportive. One supervisee stated “my supervisor left me with 2 days to score and write up each psychological report. I was always under severe pressure because of the inflexible time-table she imposed upon me.” This supervisee experienced stress because the supervisor did not provide support commensurate with the time pressure to finish the reports efficiently. Another supervisee described an excessively task-focused supervisor, this supervisor focuses only on getting done what is necessary and not on the process at all. Supervision is a series of box-checking to ensure that I am in compliance with rules, not to expand my ability and competency as a therapist.
Another supervisee reported “[my] supervisor did not adequately train me in the manual that I am providing and I had to seek other support to feel more comfortable providing the therapy.” The mismatch between what supervisees needed and what they were receiving from their supervisors was a common pattern within this category.
Poor Boundaries
Some supervisees (15.9%) described supervisor boundary violations, either the mismanagement of multiple roles, or an excessive focus on themselves and their needs (vs. supervisees). For example, supervisees recounted supervisors who “totally concentrated on their own agenda when they had a problem,” or how “[s]upervision was about her personal life challenges.” These supervisees were unable to receive supervision focused on them and their development. Another supervisee reported that their supervisor, who was also a staff manager, was not focused on my needs, specific to my case work or personal impact of the work and subsequent impact on client work. [My supervisor was] unable to contain [their] own issues and supervision became about solving organizational level concerns, [and] hearing of managerial related concerns of other staff.
The supervisee “[relied] on peers and external supervision that I supplement[ed] unofficially.” The supervisor mismanaged their dual roles, thus failing to demarcate clear boundaries between clinical work and administrative responsibilities.
Perceived Clinical Incompetence of Supervisor
Some supervisees (12.7%) described supervisors that lacked the skills and knowledge needed to provide competent supervision. One supervisee depicted a culturally insensitive supervisor: “she is not competent about exploring cultural differences and other forms of diversity… has revealed her prejudice when commenting on the marriage customs of an Indian client.” Another supervisee recounted a supervisor who was not challenging me, no wow moments, no bigger picture, future goals … I am in the process of changing supervision, I feel this one has reached its limit, I am also more qualified, trained than him, leaves me wanting more.
These examples illuminate supervisor deficiencies in both competence and credibility.
Supervisor Lack of Monitoring of Supervisee Clinical Performance
Several supervisees (9.5%) described a lack of supervisor oversight over their work with clients. Supervisees often described supervisors who were unfamiliar with their cases, or who were disconnected from what the supervisee was doing clinically. To illustrate, supervisees described supervisors who “didn’t review tape,” who were “not able to review all [my] cases,” those who “[took] my word for how things are going. Doesn’t double check assessment administration or scoring,” or were “not familiar with my patients, [he is the] supervisor because he’s [the] only PhD in [the] facility.” This lack of supervisor oversight and monitoring is concerning as supervisors can only support supervisees’ competency development and protect clients if they are tracking their supervisees’ clinical performance consistently.
Exceptional Supervision
A solid supervisory relationship is necessary, but insufficient. For exceptional supervision supervisors need to surpass the minimum standards for competency-based, adequate, supervision. The four categories within this domain were: Relational Empowerment, with a Parallel Process subcategory; Paradigm Shift; Skill Enhancement; and Illuminating Unconscious Emotional Bias. One supervisee’s statement was double-coded into more than one category (Hill, 2012).
Relational Empowerment
Supervisees described supervisors who used the supervisory relationship as a vehicle for empowerment that went above and beyond adequate supervision (42.9%). Relational empowerment reflected supervisors who: (a) provided a genuinely safe and collaborative supervisory environment, (b) validated supervisee experiences, and (c) optimized supervision based on their developmental needs. One supervisee noted, [my supervisor] validated my social justice/existential trauma theory and supported me [in] developing it further, supported me developing an intervention model, and supports/encourages me in evaluating its effectiveness… the emotional empowerment she has given me has been personally as well as professionally life-changing.
Another supervisee stated, “[m]y supervisor consistently supports my self-exploration and allows me to freely offer aspects of myself that interfere with my ability to be the best clinician I can.” Exploring one’s professional growth and biases was central to these exceptional supervision experiences. In addition, one supervisor “helped me connect personal areas of growth with my clinical work with a patient, but managed to help me develop compassion and curiosity about these areas without shaming me.” Because supervisors facilitated exploration within a safe and supportive supervisory relationship, transformational growth was possible.
Paradigm Shift
Supervisees described a profound, foundational conceptual change in their clinical work (23.8%), which often involved supervisees adopting new perspectives or gaining new insight regarding a client. For example, one supervisee recounted how “[my supervisor] helped me conceptualize cases and gain perspective in a way that I was having difficulty doing on my own.” Another shared that their supervisor “helped me look [at a] situation in a new way, suggested a new way of dealing with an issue, taught me something about my own bias [and] prejudice. Encouraged critical thinking [and] reflection of past behaviors.” Recognizing one’s biases and adopting an alternative lens exemplifies this exceptional supervision experience. Another supervisee noted the supervisor’s transformational approach: [my supervisor] helped me embody, understand, and articulate my role with traumatized clients, particularly in relationship to power struggles: “your job is not to give people what they never had, but to help them see that now is not then.”
This statement is describing not only a shift in how they conceptualized their clients, but a fundamental change in their understanding of this clinical population.
Skill Enhancement
Supervisees (20.6%) also described supervisors enhancing their knowledge and application of specific clinical competencies. Here, supervisors offered incisive feedback that allowed supervisees to thrive clinically. One participant recalled when their supervisor “explained client-centered therapy in a way that was helpful and powerful for me personally and professionally.” Another stated “the supervisor gave me an intervention to use with a minor—dramatizing how to carry his sadness and leave it down.” A third supervisee shared that “[my supervisor] used immediacy within the session to explore the dynamic between us. This role modelled [the] very skillful use of immediacy, which I then used with clients.” Similarly, another supervisee described their supervisor’s modeling: my supervisor has also brought great insight of patterns of [behavior] that clients are mirroring in their life. This has been immensely beneficial. Her use of her clinical skills within supervision and her congruence, unconditional positive regard, and empathy have been also a great role model for me to use with my clients.
Illuminating Unconscious Emotional Bias
Some supervisees (14.3%) identified and worked through transference and countertransference issues. Supervisors illuminated supervisees’ emotional reactions to clients to increase clinical effectiveness. One supervisee stated that their supervisor: helped me find compassion for a client who I was finding challenging. My supervisor was saying something like how the client was showing up the best they could, making contact the only way they knew how, and my heart opened…
Another shared that their supervisor “helped me work through deep personal block[s] from past trauma that [were] getting in the way of me being fully present with clients in session.” Similarly, another supervisee described how their supervisor facilitated me to see how I was being manipulated by my client and how I was influenced by projective identification from her part and… how my client reminded me of something in particular of my mother I wasn’t aware of before that.
Supervisors in this category conveyed support and empathy as they brought these issues into the supervisee’s awareness, helping supervisees to authentically and competently navigate their emotional reactions to clients.
Discussion
We sought to describe supervisees’ experiences of inadequate, harmful, and exceptional clinical supervision, and to triangulate our findings with Ellis et al.’s (2014) taxonomy and quantitative data. Collectively, the findings offer a more nuanced understanding of the three domains of supervision (cf. Cook & Ellis, 2021; Ellis et al., 2014, 2015a)—the categories (Table 3) tease out aspects of each supervision domain that are heretofore largely undocumented. We structured our discussion of the findings along the three research questions and where appropriate, the Benchmarks (Fouad et al., 2009) and Guidelines (APA, 2015).
Descriptions of Harmful, Inadequate, and Exceptional Supervision Experiences
Harmful and Inadequate Supervision
The pain our supervisee participants experienced is palpable—experiences all too common, as highlighted by supervisees’ narratives of harmful clinical supervision (Ellis, 2017), as well as the occurrences of specific harmful supervision descriptors noted by other researchers (Cook & Ellis, 2021; Ellis et al., 2014, 2015a), and consistent with other accounts (e.g., Ladany et al., 1999; Gray et al., 2001). Similarly, paralleling our findings, the literature attests to the occurrence and deleterious effects of inadequate supervision (e.g., Gray et al. 2001; Hendricks & Cartwright, 2018; Inman, 2006; Nelson & Friedlander, 2001; Worthen & McNeill, 1996). The harmful and inadequate supervision experiences reported herein clearly contradict most of the Guidelines (APA, 2015) and supervision competency Benchmarks (Fouad et al., 2009). We discuss these discrepancies in greater depth next.
A key finding emerging from supervisees' lived experiences is the overlap between inadequate and harmful supervision. Of note, 17 (27.0%) supervisees who identified receiving inadequate supervision also identified receiving harmful supervision from the same supervisor. The descriptions of inadequate supervision suggest that a threshold exists wherein supervisors providing inadequate supervision can become harmful to supervisees and their clients. Given that all harmful supervision is, by definition, inadequate supervision (Ellis et al., 2014), there appears to be a point at which inadequate supervisory behaviors become harmful to supervisees. Thus, there is some overlap in the supervisor's (in)actions between inadequate and harmful supervision. Such overlap emerged during the analytic process when our two coding teams for these domains independently came up with similar category labels (e.g., supervisor unsupportive and lack of supervisor support), reflecting commonalities among these two kinds of experiences. A better understanding of this threshold warrants further investigation, such as investigating supervisee resilience, the quality of the supervisory relationship, and/or other contextual factors.
Exceptional Supervision
As theorized, exceptional supervision appears to necessarily involve a strong supervisory relationship (e.g., Breese et al., 2012; De Stefano et al., 2017; Nelson et al., 2008). That is, the exceptional supervision experiences reported here entailed strong supervisory relationships where (a) supervisees felt safe, validated, and empowered; (b) supervision sessions focused on complex, relational, and process-oriented clinical training issues; and (c) went above and beyond facilitating basic supervision competencies (APA, 2015; Fouad et al., 2009). Consistent with Breese et al. (2012), exceptional supervision seems to further supervisees’ professional development and clinical competencies within a safe and empowering relational context.
What Supervisor (In)Actions Are Harmful, Inadequate, and Exceptional?
Harmful Supervision
Paralleling previous research (e.g., Ramos-Sánchez et al., 2002), harmful supervisors seem to evidence professional competence issues across multiple functional and foundational Benchmark competency domains (Fouad et al., 2009), and a failure to adhere to the Guidelines (APA, 2015; Ladany, 2014). Specifically, professional competency concerns were most often observed in four functional domains of supervision (relationships, reflective practice and self-awareness, ethical and legal standards, and individual and cultural diversity), and others (assessment, intervention, and consultation). Indeed, our most frequent categories pertained to problematic relationships (supervisor professional neglect, unsupportive supervisory relationship, and an unsafe environment), ethical-legal competencies (misuse and abuse of power and supervisor professional neglect), and reflective practice—self-assessment competencies (emotional dysregulation). Not surprisingly, these harmful supervision experiences reflected supervisor competence issues in all seven of the Guidelines domains (APA, 2015). Reviewing the specific Guidelines where supervisors fell short is beyond the scope of this manuscript; even so, we encourage readers to consider how the supervisees’ harmful experiences across the five harmful categories correspond to the 28 Guidelines (APA, 2015).
Inadequate Supervision
Inadequate supervision involved supervisors not fulfilling their responsibilities. Supervisors (a) did not offer feedback, or the feedback was dismissive, overly judgmental, or not based on observations of supervisees’ clinical performance; (b) were unavailable, inattentive, or unresponsive to supervisees needs, including setting unreasonable expectations; (c) compromised interpersonal boundaries or mismanaged their multiple roles; and (d) evidenced professional competence issues (e.g., supervising outside their areas of expertise or cultural competence). As Ladany (2014) argued, such supervisor (in)actions are ingredients for supervisor failure, and as these examples highlight, the consequences of receiving inadequate supervision were significant.
As with harmful supervision, supervisors providing inadequate supervision evidenced problems with professional foundational competencies and within the functional domain of supervision (Fouad et al., 2009) and among the seven Guidelines domains (APA, 2015). Specifically, supervisors displayed competence deficiencies in assessment, evaluation, and feedback as well as in monitoring supervisees, relationships, ethical-legal standards and professionalism, reflective practice- and self-assessment, and supervisor competence. Thus, inadequate supervision experiences tended to include deficits in multiple areas, with the supervisor often failing to fulfill their responsibilities to the supervisee and their clients in complex and multifaceted ways.
Exceptional Supervision
Although scant information exists about exceptional supervision (e.g., Breese et al., 2012), our findings suggest that exceptional supervisors facilitated a fundamental paradigm shift, offered skill enhancement that was optimally attuned to supervisees’ professional development and training needs, and illuminated and processed supervisees’ emotional reactions. Although intuitive, these aspects of exceptional supervision have not been well codified. As might be expected, supervisors providing exceptional supervision evidenced few, if any, problems of professional competence. In fact, exceptional supervision often entailed supervisors clearly exceeding the expectations outlined in the Benchmarks (Fouad et al., 2009) and Guidelines (APA, 2015).
Our participants described exceptional supervision experiences against a backdrop of strong collaborative supervisory relationships, in combination with safe, supportive, and growth-fostering supervisory environments tailored to their developmental needs (Bernard & Goodyear, 2019). A quality supervision relationship, although essential, is insufficient for exceptional supervision (Ellis et al., 2015a); supervisor functional competencies (Fouad et al., 2009) that reflect supervisor skills, expertise, and credibility, are also important. Interestingly, one component of the relational empowerment category that emerged was working through issues with parallel processes, wherein supervisors capitalized on their awareness of these issues, and modeled effective resolution (e.g., Bernard & Goodyear, 2019). Thus, exceptional supervision appears to involve supervisors who center the relationship, are attuned and responsive to relational issues as they come up, and have the skills and expertise to promote supervisee competency development. Indeed, supervisees also described supervisors using their skills and expertise to help them shift their perspectives and approaches to clinical work (Ladany et al., 2013). These “Aha!” moments were transformational for supervisees and their clients.
How Do Our Qualitative Findings Map Onto Ellis and Colleagues’ Studies?
The findings align with Ellis et al. (2014) and Ellis, Creaner, et al.’s (2015) theoretically-based and empirically-derived framework and taxonomy inasmuch as the three domains (types) of supervision appear to hold up conceptually to supervisees’ experiences at the extremes. Recalling that supervisees in our study self-identified the types of supervision they were receiving (vs. endorsing de facto, objective, behaviorally-based criteria), a few supervisees identified that they were currently receiving, from the same supervisor, both harmful and inadequate supervision (n = 17), consistent with Ellis and colleagues taxonomy or framework; others indicated receiving both exceptional and inadequate supervision (n = 2), or harmful and exceptional supervision (n = 1), or all three (n = 2), inconsistent with the framework.
Percentages of Supervisees Within Each Domain Classified Per the Taxonomy
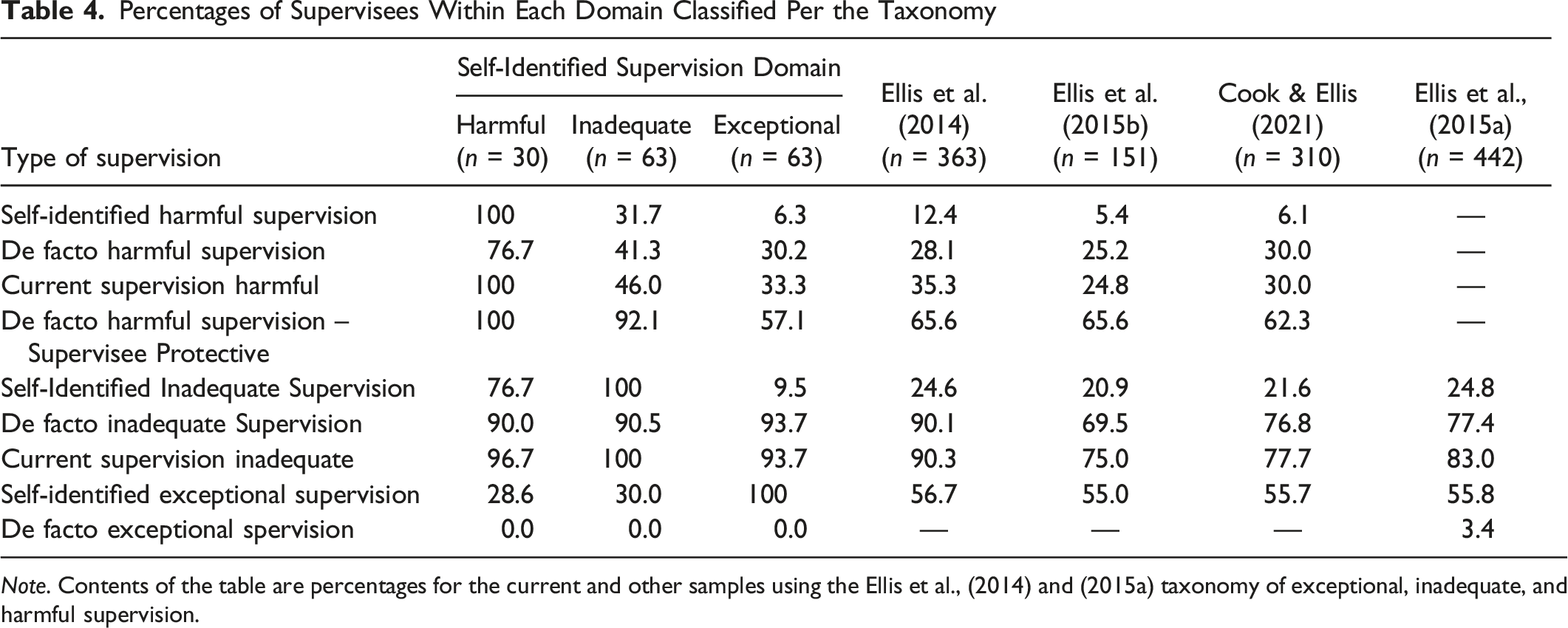
Note. Contents of the table are percentages for the current and other samples using the Ellis et al., (2014) and (2015a) taxonomy of exceptional, inadequate, and harmful supervision.
Although supervisees’ inaccurate grasp of supervision may partially explain the findings—it does not do so fully, hence meriting further study. It is also possible that supervisors are providing more than adequate clinical supervision and also (fail to) act such that it harms the supervisee, yet is unbeknownst to the supervisor, and thus, left unaddressed. For example, a supervisor might assign a case that appears to be appropriate for the supervisee’s skill level but triggers a trauma response from the supervisee based on past experiences that have not been shared with the supervisor. Or, consider supervisors who offer exceptional supervision and due to situations outside their control, cannot meet the minimally adequate supervision standards (e.g., due to COVID-19 restrictions). Technically, these occurrences would be classified as inadequate supervision, but without consideration of the contextual factors at play. Finally, for many supervisees, a very strong supervisory relationship might overshadow inadequate, or even harmful supervisory behaviors. Thus, when assessing exceptional, inadequate, and harmful supervision, one needs to consider: (a) contextual factors that may lead to inaccurate classifications when implementing the de facto criteria (Ellis et al., 2014), and (b) the extent to which supervisees feel able to take risks in speaking up in supervision when things go awry.
Strengths and Limitations
The current study has several strengths. Notably, we purposefully sampled and strived to listen to the perspectives of supervisees in order to obtain a rich description of the phenomena of interest. Consistent with CQR-M (Spangler et al., 2012) and well-established standards of qualitative methods of inquiry (Denzin, 1978), we used several judges to reduce the disproportionate impact of any one judge on the data analysis. The diverse coding teams allowed for a trustworthy data analytic process informed by multiple perspectives. Moreover, prior to the data analysis, we had lengthy discussions about the power differences among us, and our assumptions and biases surrounding harmful, inadequate, and exceptional supervision. Doing so allowed us to be transparent about our expectations and then bracket them to minimize any undue influence on the ways in which we were making sense of the findings.
This study also has some important limitations. Although electronically-transmitted open-ended questions allowed us to reach a large participant pool and access a wide range of experiences, interviews would have provided deeper, more contextualized understandings. Interviews could also illuminate the ways in which the broader system might perpetuate or support different kinds of supervision experiences (e.g., an agency with a high sense of urgency that values efficiency above all else might make it difficult for supervisors to give supervisees sufficient time to complete an assessment report). Some participants provided detailed responses and noted numerous negative or positive supervision experiences, whereas others may have reported one of many experiences. Without the opportunity to query and probe further into their experiences, we were unable to clarify some details or assess the extent to which participants chose to describe one of many supervision experiences. We hope that our findings can inform the development of interview protocols that permit a more in-depth exploration of these constructs in future research. Although we aimed to recruit diverse trainees from multiple disciplines, and who represented differing levels of development, as with any qualitative study, generalizability was not our focus. That said, it is important to note that our sample was predominantly White and female. Although this is consistent with the extant research in this area, it is possible that individuals with different identity group memberships would have provided different responses. Moreover, we did not collect demographic data around sexual orientation, social class, religion, or citizenship status, as well as other identity data. Having access to a more holistic understanding of our participants’ and their supervisors’ backgrounds would further contextualize our findings.
Implications for Supervisory Practice, Education, Training, and Advocacy
Our findings suggest that training systems (e.g., programs, sites) could be more vigilant in instances of inadequate and harmful supervision as well as reward exceptional supervision. Given the hierarchical relationship and supervisees’ reluctance to raise concerns about the supervision they are receiving, training directors might need to advocate for supervisees, and investigate even minimal signs of wrong-doing in clinical training through regular visits to and ongoing communication with sites. This seems especially important for supervisees with marginalized identities, as the power differential might be further amplified if the supervisor has multiple areas of privilege relative to the supervisee (Ladany, 2014; Nelson et al., 2008). Another possible focus for advocacy work would be for programs to develop systematic training and supervised experiences for supervisors (collegially referred to as “sup of sup”). Training supervisors about the Guidelines (APA, 2015) and encouraging faculty to refer to them when making pedagogical and training choices promotes a competency-based approach to preventing harmful and inadequate supervision. Conducting systematic and routine evaluations of sites and supervisors in ways that do not put trainees at further risk could also be helpful. For example, programs can collect feedback across supervisees and semesters and aggregate these data to protect supervisee anonymity and prevent retaliation. If evidence suggests inadequate or harmful supervision exists, training programs and agencies have an obligation to intervene and protect supervisees (Kangos et al., 2018).
In addition, supervisors and training programs could educate supervisees about the roles, expectations, and responsibilities in clinical supervision (e.g., via a supervision informed consent; Bernard & Goodyear, 2019) and offer role inductions (e.g., Ellis et al., 2015c), particularly at the beginning of supervisees’ clinical training, as they are acclimating to supervision. Per the Guidelines (APA, 2015), supervisors, by virtue of their position of power, bear the responsibility to educate supervisees about supervision and the criteria by which to evaluate it. It is also recommended that supervisors regularly solicit feedback about supervision and convey their commitment to addressing any emerging concerns (Kangos et al., 2018).
Implications for Research
Returning to the research question, the categories found in this study (see Tables 1) suggest that Ellis et al. (2014) and (2015b) taxonomy may benefit from further differentiation within each domain of supervision to examine the specific categories (e.g., create subtypes). In fact, most of the de facto criteria for harmful, inadequate, and exceptional supervision appear to map onto the categories as subcategories within the respective domains. Doing so may allow for investigations of the predictors and impacts of the various subtypes of harmful, inadequate, and exceptional supervision—research that may lead to remedial and preventive interventions for harmful and inadequate supervision, and equip supervisors with the tools for exceptional supervision.
Researchers could also interview supervisees who identify as receiving exceptional, inadequate, and harmful supervision from the same supervisor. In addition, researchers could use mixed methods research designs to further explore and assess these constructs. As this is the first study to collectively examine supervisees’ subjectively described exceptional, inadequate, and harmful supervision experiences, replication is recommended. For example, it would be valuable to examine if the observed findings apply to a more racially and ethnically diverse sample, as well as to supervisees in non-English speaking countries, and non-Western cultures. In so doing, a more comprehensive understanding of how harmful, inadequate, and exceptional supervision are experienced by supervisees with diverse identity group memberships would be possible.
Conclusion
This study built on the research of Ellis and colleagues by obtaining a rich description of supervisees’ lived experiences of harmful, inadequate, and exceptional supervision. The findings, although consistent with these studies and more recently, Cook and Ellis (2021), offer a more nuanced and multifaceted understanding of the phenomena of interest. We hope that they inform supervision research and practice that prevents harmful and inadequate supervision, and promotes exceptional supervision experiences.
Footnotes
Aknowledgments
We are grateful for the insightful comments from Erica Ellis on several drafts of the manuscript.
Author Note
An earlier version of the article was presented at the 127th annual meeting of the American Psychological Association, Chicago, IL.