
Abstract
Clinical supervision is a cornerstone of clinical training, and supervision experiences are associated with important outcomes (e.g., stronger working alliances and more trainee disclosures in supervision). Psychology has made strides in understanding how cultural processes unfold in supervision, with the multicultural orientation (MCO) model garnering increasing empirical support, but less is known about the dynamics that occur based on racial differences between supervisees and supervisors. Therefore, within cross-racial supervisory relationships, we examined the associations between cultural humility, cultural comfort, and supervisees’ satisfaction with supervision, disclosure in supervision, and the supervisory working alliance. Survey results from Black, Indigenous, and people of Color (BIPOC) trainees (N = 116) receiving supervision from White supervisors indicated that supervisees who rated their supervisors high in cultural humility and cultural comfort also reported higher supervision satisfaction and a stronger supervisory working alliance. Perceptions of supervisors’ cultural humility, but not cultural comfort, were related to a higher willingness to disclose in supervision.
Keywords
The results of the present study highlight the importance of cultural humility and cultural comfort in Black, Indigenous, and people of Color (BIPOC) supervisees’ experiences in clinical supervision with White supervisors. Cultural humility was also related to supervisees’ greater willingness to disclose in supervision. This further evidence for the multicultural orientation (MCO) framework in clinical supervision emphasizes the need for supervisors to foster their MCO.Significance of the Scholarship to the Public
The Relationship Between Cultural Humility, Cultural Comfort, and Supervision Processes and Outcomes for BIPOC Supervisees
My supervision experience included “blatant racism by psychologists.” (Anonymous BIPOC participant; Wilcox et al., 2022)
This quote is an unfortunate reality for many supervisees who are Black, Indigenous, and people of Color (BIPOC). Indeed, O’Hara (2014) found that incidences of supervisory microaggressions were highly correlated with a poor supervisory working alliance. Moreover, scholars (e.g., Monceaux et al., 2021; Wilcox et al., 2020) have found that psychotherapists overwhelmingly do not consider their clients’ sociocultural contexts and cultural identities during case conceptualization and treatment planning. Yet, scholars have long emphasized the importance of being oriented toward cultural dynamics and processes in psychotherapy, and ideally those lessons would be incorporated in supervision. In fact, the American Psychological Association (APA; 2002, 2017) is now on their second iteration of multicultural guidelines, both of which drew heavily from the tripartite multicultural competencies (MCC) model (Sue et al., 1982). The MCC model emphasizes the importance of knowledge, awareness, and skills in the provision of culturally-responsive psychotherapy and supervision (Sue et al., 1982, 1992). More recently, scholars have sought to extend the MCC model to include social justice competencies (e.g., Singh et al., 2020). However, there is an MCC theory-to-supervision practice gap, especially for the supervision practices of BIPOC trainees.
White clinicians represent the majority in psychology in the United States, accounting for approximately 83% of the psychology workforce (APA, 2022). Due to White hegemony in the mental health profession, it is highly probable BIPOC supervisees will work with White supervisors at some point throughout their clinical training. Previous research has demonstrated that when BIPOC supervisees are paired with BIPOC supervisors, it is facilitative of cultural discussions (Jernigan et al., 2010). However, BIPOC supervisees paired with White supervisors may encounter challenges associated with their racial and cultural differences (Constantine & Sue, 2007), interpersonal conflicts due to cultural differences (Sue et al., 2022), and obstacles related to their professional roles (Nilsson & Duan, 2007). This can be particularly concerning as it can negatively impact the supervisory relationship (or the supervisory working alliance) and result in an adverse supervision experience. Indeed, scholars have found that experiences of racism negatively impact clinical supervision for BIPOC supervisees (Jang et al., 2019), although MCC may alternatively contribute to positive outcomes in the supervision dyad (Vandament et al., 2022). Given the dearth of research specifically on cross-racial clinical supervision, it is important to examine supervision processes and outcomes specifically in cross-racial clinical supervision.
Multicultural Orientation Framework
To complement the model of MCC, scholars sought to capture the processes unfolding in therapy through defining a framework called multicultural orientation (MCO; Owen, 2013; Owen et al., 2011). The MCO framework includes three interrelated pillars: cultural humility, cultural opportunities, and cultural comfort. Cultural humility refers to an individual’s ability to foster an open, other-oriented stance toward others’ cultural identities and experiences. Cultural opportunities refer to behavioral expressions of cultural humility; they require cultural humility to recognize and skillfully engage culture within a session. Cultural opportunities are similar to what emotion-focused therapists refer to as “markers” (Elliott et al., 2004), interpersonal therapists refer to as “points of entry” (Teyber & Teyber, 2017), and what Yalom (2009) refers to as here-and-now occurrences that require the development of finely-tuned “rabbit ears” to catch and intervene in these fleeting moments. Finally, cultural comfort is an expression of cultural humility in how psychotherapists emotionally respond to clients and implies maturity in responding to cultural transference (and countertransference). Clinicians mature in this aspect of MCO respond to even difficult situations with a high degree of emotional attunement, flexibility, and paradoxical confidence as opposed to avoidance. Research has consistently shown that cultural humility, cultural opportunities, and cultural comfort are positively related to psychotherapeutic outcomes (Davis et al., 2018; Owen et al., 2016, 2017; Zhang et al., 2021). Building from this work, supervision scholars (e.g., Hook et al., 2016; Watkins et al., 2019; Watkins & Hook, 2016) have posited the significant influence of MCO on supervision processes and outcomes; however, only recently has research begun to examine these relationships empirically.
An MCO approach to supervision proposes that (a) the supervisor and supervisee are in a bidirectional educational relationship, (b) the supervisor is transparent about the attitudes and values that influence their behaviors and actions, (c) cultural processes are important for connecting with supervisees’ and clients’ cultural identities, and (d) a strong MCO motivates a desire to learn more about the supervisor’s, supervisees’, and clients’ worldviews (Watkins et al., 2019). Although in its nascent stages, a body of literature is emerging investigating the relationship between MCO and supervision processes and outcomes. Two recent studies found that supervisor cultural humility and cultural missed opportunities were significantly associated with supervisees’ satisfaction with clinical supervision (Drinane et al., 2021; Wilcox et al., 2022); however, the samples in these studies were predominantly White. Research has also demonstrated that BIPOC trainees experience detriments as a result of racism during their supervision and training (e.g., Alvarez et al., 2009; Nilsson & Duan, 2007; Pieterse et al., 2016; Wong & Jones, 2018), yet their experiences have not been comprehensively represented in the literature. It is therefore imperative to examine clinical supervisors’ MCO and its relationship with supervision processes and outcomes in cross-racial supervision between White supervisors and BIPOC supervisees.
The component of supervision considered to be most crucial for effective supervision is the supervisory working alliance (Schweitzer & Witham, 2018). The supervisory working alliance is defined as the relational bond between supervisee and supervisor, as well as agreement on the goals and tasks of clinical supervision (Bahrick, 1989; Bordin, 1983). The supervisory working alliance has consistently been found to be positively related to a host of important supervision outcomes, including trainee disclosure (e.g., Gibson et al., 2019), satisfaction with supervision, supervisee self-efficacy, and a stronger therapeutic working alliance between supervisees and their clients (e.g., Park et al., 2019). However, little empirical evidence exists regarding how cultural factors relate to the supervisory working alliance.
Wilcox et al. (2022) were among the first to empirically apply the MCO framework to clinical supervision. They examined the impact of supervisors’ cultural humility and cultural (missed) opportunities on supervisees’ satisfaction with supervision. They examined cultural humility and cultural opportunities along two levels: (a) as it pertained to the supervisees’ cultural identities and experiences, and (b) as it pertained to the supervisees’ clients’ cultural identities and experiences. They found that supervisors’ supervisee-focused perceptions of cultural humility were significantly and positively associated with satisfaction with supervision, and supervisors’ supervisee-focused cultural missed opportunities were significantly and negatively associated with satisfaction with supervision. Thus, supervisor cultural humility and engagement in cultural opportunities in supervision positively affected supervisees’ satisfaction with supervision. However, again, this sample was predominantly White.
Supervisees’ satisfaction with supervision is a frequently measured supervision outcome, defined as supervisees’ assessment of the quality of their supervision and the extent to which they feel as though their needs were met (Ladany et al., 1999). Satisfaction is considered important for supervisees’ engagement (Ladany et al., 1999), and research has demonstrated that satisfaction with supervision is inversely related to trainee nondisclosure (Ladany et al., 1996) and positively related to attention to culture in supervision (e.g., Green & Dekkers, 2010). In a recent study of MCO in clinical supervision (in a sample of predominantly White supervisees), Drinane et al. (2021) sought to examine the extent to which supervisees engage in cultural concealment, a process in which individuals subtly downplay or hide their cultural identities or experiences. Cultural concealment was examined on two levels: (a) whether the supervisee deliberately withheld sharing aspects of their own cultural identity, and (b) whether the supervisee concealed aspects of their clients’ cultural identities. They found that both supervisee-focused and client-focused cultural concealment were significantly and negatively associated with satisfaction with supervision and with the supervisory working alliance. Supervisees not only had lower levels of satisfaction with supervision, but also weaker working alliances with their supervisors–both of which could hinder their growth as therapists and, more importantly, hinder the therapeutic process with their clients (Drinane et al., 2021).
Relatedly, supervisees’ willingness to disclose in supervision is another important supervision outcome. Supervisors are responsible for both the professional development of supervisees as well as client welfare; in order for supervisors to do their jobs effectively, they are reliant upon supervisees disclosing their internal processes as well as what is happening in psychotherapy with their clients (Amerikaner & Rose, 2012; Bernard & Goodyear, 2019). It is not unusual or inherently problematic for supervisees to withhold certain types of information from their supervisors (Mehr et al., 2010), especially if they feel as though their supervisor may not understand them (Farber & Hazanov, 2014), but it is important that supervisees disclose the things that matter to their work with clients. Hutman and Ellis (2020) recently found that supervisor multicultural competence was negatively related to supervisees’ nondisclosure. Yet to be determined, however, is the relationship between MCO and supervisee nondisclosure, especially among BIPOC supervisees.
The Present Study
With a sample of BIPOC supervisees who were working with White supervisors, we sought to examine the relationship between supervisor cultural humility and cultural comfort and supervisees’ satisfaction with supervision, willingness to disclose in supervision, and ratings of the supervisory working alliance. Based on the existing MCO research, we theorized that BIPOC supervisees would report having more positive supervisory experiences, a more positive supervisory relationship, and be less guarded in supervision if they perceived their supervisors as higher in cultural humility and cultural comfort. Specifically, we hypothesized that both cultural humility and cultural comfort would be positively related to (a) supervisees’ satisfaction with supervision, (b) supervisees’ willingness to disclose in supervision, and (c) the supervisory working alliance. We focused specifically on cultural humility and cultural comfort to examine therapist characteristics that may influence the supervisory process, rather than supervisor behavior (cultural opportunities).
Method
Participants
The sample consisted of 116 BIPOC-identified psychotherapists-in-training who were recruited via email through U.S.-based listservs as well as via emailing current graduate program directors. All participants were currently receiving clinical supervision from a White supervisor. Data collection occurred during fall of 2020 and spring of 2021; participant recruitment occurred toward the end of the fall semester and spring semester to help ensure that participants were not reporting on a new supervisory relationship. Given that this sample was collected during the COVID-19 pandemic, participants were asked about the format of their supervision; notably, 75.0% (n = 87) reported that their supervision was telesupervision-only, whereas 18.1% (n = 21) were receiving only in-person supervision, and 6.9% (n = 8) were receiving a combination of both. The majority of the sample identified as women (n = 98, 84.6%), followed by men (n = 14, 12.1%), and genderqueer or gender nonbinary (n = 4, 3.5%). In terms of race, participants identified as Black/African American (n = 41, 35.0%), Asian/Pacific Islander (n = 31, 26.7%), Hispanic/Latinx (n = 21, 18.1%), multiracial (n = 13, 11.2%), Middle Eastern/North African (n = 7, 6.0%), Native American/First Nation (n = 2, 1.7%), and an identity not listed (n = 1, 0.8%). The average age of participants was 29.23 years (SD = 7.49). The participants predominantly identified as heterosexual (n = 71, 60.3%), with 20.7% (n = 24) identifying as bisexual, 6.0% (n = 7) as pansexual, 4.3% (n = 5) as gay/lesbian, 5.2% (n = 6) as queer or questioning, 1.7% (n = 2) as asexual, and 1.7% (n = 2) as an identity not listed. Social class was measured using the social class ladders of the MacArthur Sociodemographic Scale (Adler et al., 2000), on which participants rate from 0 to 10 where they feel their social standing is compared to others in their community or the United States, respectively; participants reported being, on average, middle class (M = 5.67, SD = 1.58) as compared to others in the United States, with 52.7% (n = 61) rating themselves at 6 or above.
As for professional characteristics, on average, participants were in their third year of their graduate program and had 17.60 months (SD = 18.56) of supervised clinical experience. Most students were enrolled in a PhD (n = 52, 44.8%) or PsyD (n = 21, 18.1%) program, followed by MS (n = 18, 15.5%), MA (n = 11, 9.5%), MSW (n = 5, 4.3%), MFT (n = 5, 4.3%), and other master’s or doctoral programs (n = 4, 3.4%). Most participants were training in clinical psychology (n = 41, 35.3%) or counseling psychology (n = 38, 32.8%), followed by counseling or mental health counseling (n = 12, 10.3%), marriage and family therapy (n = 10, 8.6%), school psychology (n = 4, 3.4%), and other mental health programs (n = 11, 9.5%). Other than supervisor race, demographic characteristics of the supervisors were not obtained.
Measures
Supervision Cultural Humility Scales
Correlation Matrix and Descriptive Statistics
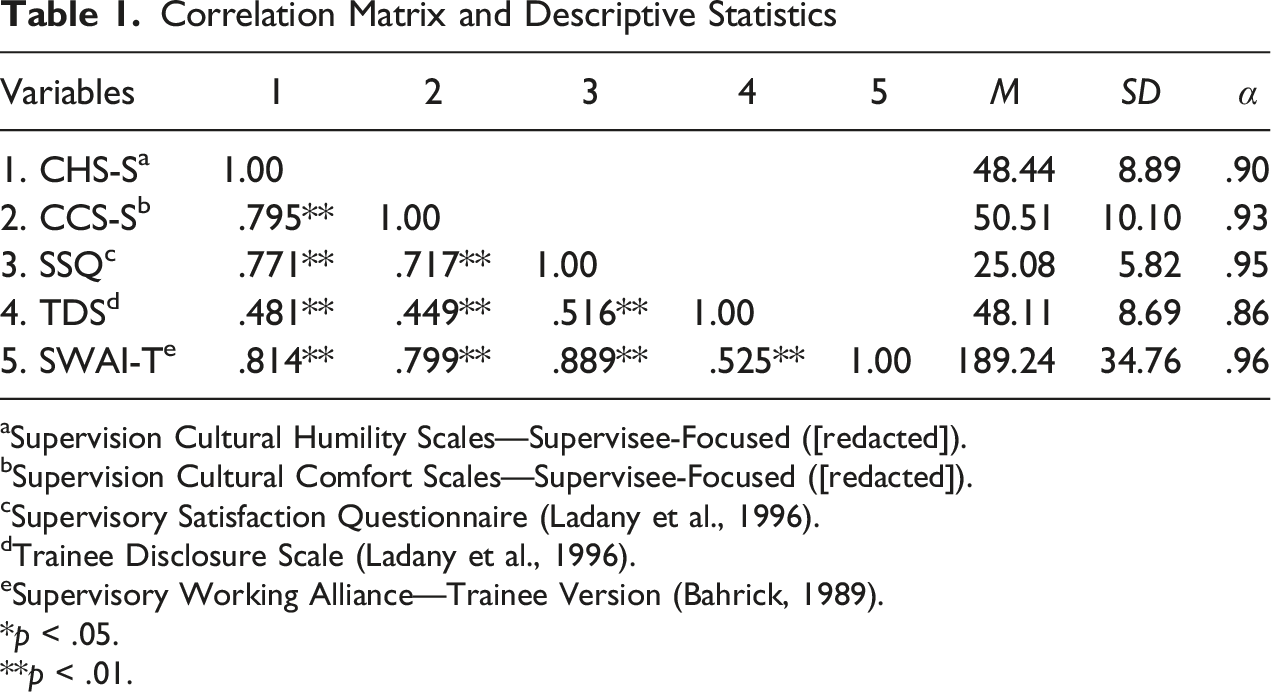
aSupervision Cultural Humility Scales—Supervisee-Focused ([redacted]).
bSupervision Cultural Comfort Scales—Supervisee-Focused ([redacted]).
cSupervisory Satisfaction Questionnaire (Ladany et al., 1996).
dTrainee Disclosure Scale (Ladany et al., 1996).
eSupervisory Working Alliance—Trainee Version (Bahrick, 1989).
*p < .05.
**p < .01.
Supervision Cultural Comfort Scales
The Supervision Cultural Comfort Scales (CCS-S) is an adapted version of Pérez-Rojas et al.’s (2019) Therapist Cultural Comfort Scale. Similar to the CHS-S, the CCS-S is a set of two 13-item self-report measures, one supervisee-focused and one client-focused. All items are answered on a 5-point Likert-type scale, from 1 (Strongly Disagree) to 5 (Strongly Agree), with a potential range of 13 to 65; higher scores indicate greater supervisee-perceived supervisor cultural comfort. The Therapist Cultural Comfort Scale was adapted for the clinical supervision context by editing the prompt rather than each item, such that the prompt for the scale read (for the supervisee-focused measure), “When important parts of my culture come up or are discussed, my supervisor…” Sample items include “Stumbles with words” and “Appears anxious.” Similar to the CHS-S, both CCS-S were administered, but only the supervisee-focused scale is described. The original Therapist Cultural Comfort Scale demonstrated good internal consistency (.97) as well as convergent and incremental validity (Pérez-Rojas et al., 2019); however, this was in a sample of predominantly White psychotherapy clients.
Supervisory Satisfaction Questionnaire
The Supervisory Satisfaction Questionnaire (SSQ; Ladany et al., 1996) is an 8-item, Likert-type scale that measures supervisees’ satisfaction with their clinical supervision. Anchors on the Likert-type scale are specific to the item being answered, such as “Did you get the kind of supervision that you wished?” or “If you were to seek supervision again, would you come to this supervisor?” Participants may answer from 1 to 4, resulting in a potential range of scores from 8 to 32. Higher scores on the SSQ are indicative of greater satisfaction with clinical supervision. Internal consistency was reported as .96 by Wilcox et al. (2022) and .92 in a sample of international student trainees (Mori et al., 2009). It has been found to be related to supervisor multicultural competence (Inman, 2006; Mori et al., 2009) and the supervisory working alliance (Inman, 2006).
Supervisory Working Alliance Inventory—Trainee Version
The Supervisory Working Alliance Inventory—Trainee Version (Bahrick, 1989) is a 36-item self-report inventory of trainees’ experience of their working alliance with their clinical supervisor based on Bordin’s (1983) alliance framework. Items are rated on a 7-point Likert-type scale, from 1 (Never) to 7 (Always); participants are asked to rate how often they think or feel a certain way about their supervisor. The potential range of scores is from 36 to 252, with higher scores indicating a stronger supervisory working alliance. Example items include “I feel uncomfortable with [my supervisor],” and, “[My supervisor] and I respect each other”.
Trainee Disclosure Scale
The Trainee Disclosure Scale (Walker et al., 2007) is a 13-item self-report inventory that assesses for supervisees’ willingness to disclose in clinical supervision. Respondents are asked to endorse to what extent they would have been likely to discuss certain topics in their most recent clinical supervision session. Items are answered on a 5-point Likert-type scale, from 1 (Not at all likely) to 5 (Very likely). Scores are summed and may range from 13 to 65, with higher scores indicating a supervisee’s greater willingness to disclose in supervision.
Results
Although 261 participants began the survey, 87 discontinued almost immediately. Three did not meet inclusion criteria (currently enrolled in a mental health training program, identified as BIPOC, currently seeing clients, currently receiving supervision from a White supervisor). Of the 171 that remained, 52 discontinued the survey before completing all measures or did not complete at least 80% of all primary study measures. Thus, the initial sample was 119. Little’s MCAR was performed to analyze missing values; it was nonsignificant for the SSQ and CCS-S (client-focused); it was significant for CHS-S (supervisee-focused; χ2 = 47.02, df = 2, p = .001) and the SWAIT-T (χ2 = 308.41, df = 206, p < .001), however, less than 5% of data were missing per item. Thus, expectation maximization was used to impute missing values. Three multivariate outliers were removed (Mahalanobis distance > 13.82), resulting in the final sample of 116. Skewness and kurtosis values for all variables were within acceptable limits (skew < ± 2, kurtosis < ± 7; Byrne, 2010). No significant differences were observed on the variables of interest by any demographic or situational variables, including format of supervision.
Given the conceptual overlap, first, variance inflation factor (VIF) and tolerance values were examined for the supervisee-focused versus client-focused CHS-S and CCS-S. VIF values above 5 and tolerance values below 0.20 are generally cause for concern (Menard, 1995). Although all VIF values were below 10 and most tolerance values were above 0.2, supervisee-focused CHS-S in particular demonstrated values of concern (VIF = 5.61, tolerance = 0.178), and the remaining ranges for VIF were 3.97 to 4.73 and for tolerance were 0.21 to 0.25. Preliminary analyses demonstrated similar results as those demonstrated in Wilcox et al. (2022): Once the supervisee-focused perspective was accounted for, the client-focused perspective was no longer significant. Therefore, and to be consistent with prior research, the results reported here are only for supervisee-focused CHS-S and CCS-S. Multicollinearity was also assessed between the CHS-S and the CCS-S given the relationship between these two facets of MCO; although the two variables are highly correlated, multicollinearity was not observed to be an issue (VIF = 2.72, tolerance = 0.368). Preliminary analyses were then performed to assess for significant between-group differences on all study variables by race, gender, sexual orientation, socioeconomic status, and master’s versus doctoral students. No significant differences were found on any study variable by any of these demographic characteristics.
A multivariate multiple regression was performed to test the hypotheses, with supervisory satisfaction, the supervisory working alliance, and trainee willingness to disclose as the dependent variables, and supervisee-focused supervisor cultural humility and cultural comfort as the independent variables (see Figure 1 Conceptual model and results of multivariate multiple regression of cultural supervision processes and outcomes for BIPOC supervisees.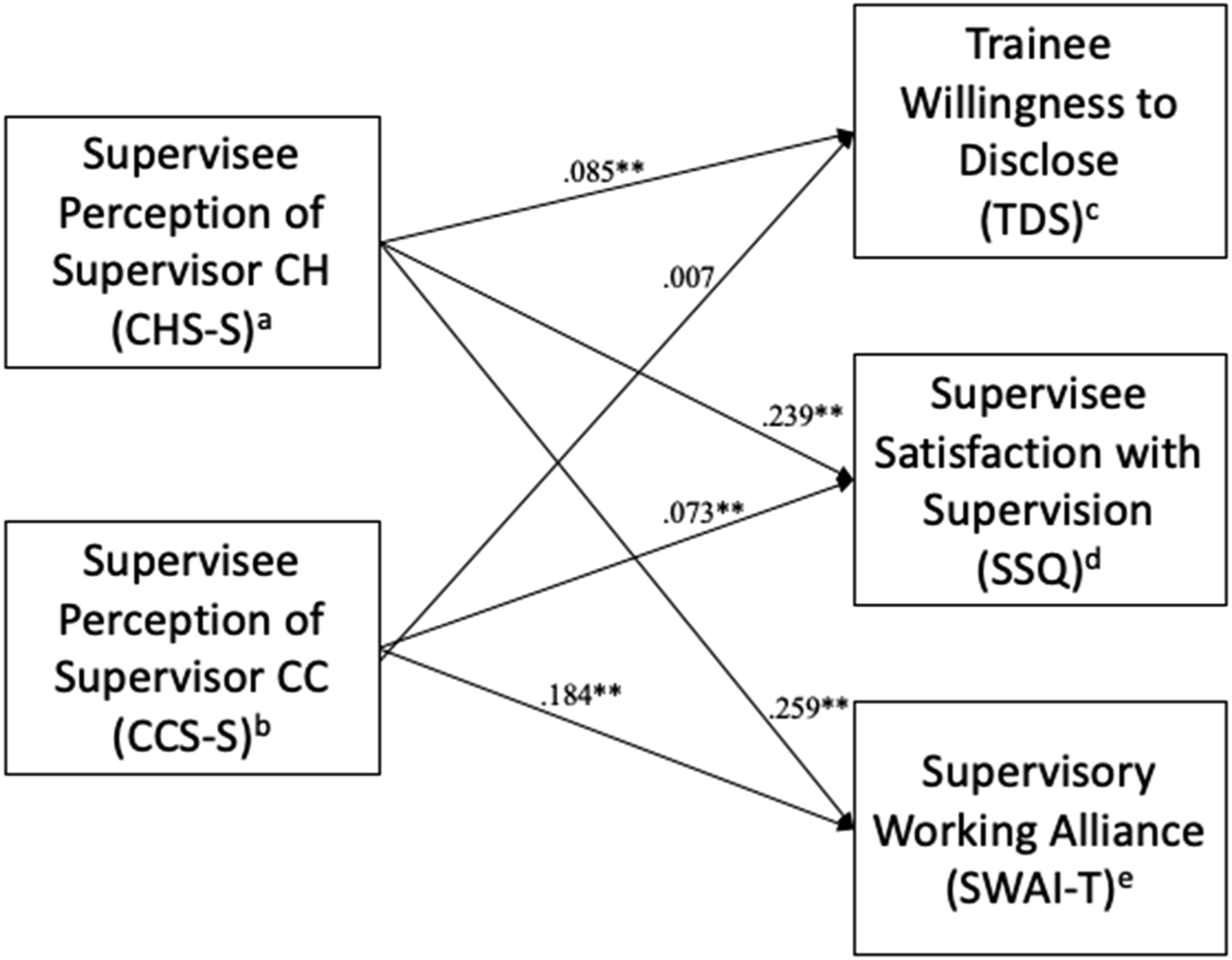
Discussion
The present study was one of the first to examine the relationship between MCO and clinical supervision processes and outcomes specifically for BIPOC supervisees receiving clinical supervision from White clinical supervisors. Most hypotheses were supported, consistent with the burgeoning literature demonstrating that MCO is important for clinical supervision processes and outcomes. Specifically, BIPOC supervisees who rated their White supervisors higher in cultural humility and cultural comfort reported a better supervisory working alliance and greater satisfaction with supervision. Those who rated their supervisors higher in cultural humility reported greater willingness to disclose to their supervisor about difficult supervision issues; however, cultural comfort was not found to be related to willingness to disclose. The results of the present study add to the body of literature that suggests that MCO, specifically cultural humility and cultural comfort, are important to culturally-responsive supervision.
Clinical supervision is the primary method of psychotherapy training (Bernard & Goodyear, 2019), which is in part theorized (and empirically demonstrated) to occur through parallel processes (Tracey et al., 2012). Thus, better understanding what constitutes culturally-oriented supervision may help the field of psychotherapy to better foster culturally-oriented psychotherapists. Perhaps more importantly, given that professional psychology remains overwhelmingly White (APA, 2022), and that many BIPOC trainees experience racism during their training (Basma et al., 2021), better understanding culturally-responsive clinical supervision for BIPOC supervisees will help to support BIPOC trainees’ pathways into the professional psychology workforce. Especially given the results of the present study, it is important that supervisors (and supervisors-in-training) have opportunities to foster their cultural humility and cultural comfort, such as through didactic training and clinical supervision opportunities with MCO-oriented supervisors.
Supervisees’ perceptions of supervisors’ cultural humility were associated with their levels of nondisclosure, but there was no significant association found between supervisors’ cultural comfort and nondisclosure. Given that trainee nondisclosure has significant clinical and supervisory implications, more research is needed to explore possible mechanisms explaining the link between cultural humility, and cultural comfort, and nondisclosure. Trainees may opt to not disclose information, particularly around cultural processes, if they perceive that their supervisor cannot hold space for, or value, complex or difficult cultural conversations. Some have suggested that supervisor cultural humility is required to repair ruptures in the supervisory working alliance (Watkins et al., 2019); it is possible that supervisees may anticipate or assume supervisors’ inability to engage in conflict prior to adequately repairing the relationship.
Strengths and Limitations
It is important to consider the study results in the context of its limitations as well as its strengths. The first major limitation is that this was an ex post facto survey study from the perspective of supervisees. Other than what was reported by the supervisee participants, little is known about the supervisors themselves, nor was the supervisory relationship able to be examined over time. It is also unknown how long supervisees were in supervision with the supervisor on whom they were reporting; and, we relied on supervisees’ perceptions of their supervisor’s racial identity. Second, our sample was among the first to examine MCO in the context of BIPOC supervisees’ experiences; and although preliminary analyses suggested no significant differences between racial groups, this may be due in part to small subsample sizes. It is possible that Black, Indigenous, Latinx, Asian, Southeast Asian, Middle Eastern/North African, and other supervisees of Color may have different experiences in clinical supervision. Further, we only examined the experiences of BIPOC supervisees receiving supervision from White supervisors; it is also possible that supervision could unfold differently in important ways for BIPOC supervisees with BIPOC supervisors, White supervisees with BIPOC supervisors, and White supervisees with White supervisors.
Intersectionality was also not accounted for; it is possible, for example, that women, trans and gender nonbinary supervisees of Color have different experiences in clinical supervision than men of Color or that lower socioeconomic status BIPOC supervisees have different experiences than upper socioeconomic status BIPOC supervisees. Indeed, research suggests that Black women experience specific types of microaggressions associated with greater detriment (Lewis et al., 2013, 2017). Black people experience racism differently at different socioeconomic levels (Cavalhieri & Wilcox, 2021), and Latinx sexual minority men report discrimination at the intersection of their racial/ethnic and sexual orientation identities (Zelaya et al., 2021). As the field advances its understanding of culturally-responsive clinical supervision, it will be imperative for future research to examine MCO and clinical supervision in the context of the different types of racism experienced by individuals from different racially-minoritized groups, as well as in the context of intersectional complexity. Finally, the correlations between cultural humility and cultural comfort were observed to be rather high; future research examining the conceptual differentiation between cultural humility and cultural comfort will be important.
As for strengths, this study was amongst the first to examine the role of MCO in clinical supervision specifically with BIPOC supervisees working with White supervisors. Our sample was adequate in size and diverse in terms of racial identity, sexual orientation, and professional characteristics. As well, we assessed for differences in supervision format, finding no differences between telesupervision and in-person supervision on study variables. Given the increasing shift to telehealth, the lack of differences between supervision formats is an important contribution.
Implications for Practice, Education and Training, and Research
The results of our study suggest that White supervisors’ cultural humility and cultural comfort are particularly important in supervision with BIPOC supervisees. Cultural humility appears to be especially important in BIPOC supervisees’ willingness to disclose in clinical supervision. Therefore, it is important that learning about and fostering cultural humility and cultural comfort be emphasized in education and training, including specifically during supervisory training. Given that the preponderance of supervision is provided by psychologists who have already graduated, continuing education in particular will be an important avenue for supervisors to further develop their cultural humility and cultural comfort. It is incumbent upon supervisors to intentionally develop their MCO and their ability to engage in discussions related to racism and Whiteness from a curiously humble and open stance.
It is important for White supervisors to recognize that both Whiteness and their professional role contribute to the power imbalance in supervision with BIPOC trainees; it is the responsibility of all supervisors to foster a supervisory environment characterized by safety, comfort, and the ability to have difficult conversations about culture and positionality within the supervisory dyad itself. Much of this work is process-oriented, rather than content-oriented. A supervisor can elect to attend continuing education seminars that focus on multicultural competency; but, in order to further their humility and comfort they must be intentional about reflecting on how they experience such training. For example, if a supervisor feels uncomfortable in culturally-responsive training, why? Such continuing education is important, and should also be supplemented with deeper, interpersonal work. We recommend that supervisors identify and develop consultation groups with trusted colleagues, where they can unpack their assumptions, identify points of cultural discomfort, and practice receiving feedback openly. Supervisors may also solicit anonymous feedback from multiple supervisees, and notice their own reactions in reviewing feedback (i.e., cultural humility).
Finally, supervisors may want to reflect on who approaches them for supervision: Do BIPOC or other underrepresented supervisees work with them? Does it seem as though White supervisees disclose more to them than non-White supervisees? Based on the findings of this study, supervisors who find that BIPOC students tend to disclose less frequently in supervision than their White peers may want to use this as an opportunity to reflect on what cultural dynamics are at play in cross-racial supervision. Although beyond the scope of this study, supervisors should also notice how they may be explaining these differences (e.g., do supervisors perceive their White supervisees as more conscientious or self-aware?) and how cultural factors may be a more meaningful explanation (e.g., a supervisee of Color perceives their supervisor as low in cultural humility).
This study’s results also have implications for how training programs might socialize their students from underrepresented groups when it comes to selecting supervisors. Training program faculty can name cultural processes, such as humility and comfort, as important factors associated with training outcomes and emphasize that trainees evaluate the extent to which a potential supervisor is culturally humble or comfortable. Coaching on how to ask potential supervisors questions about this is important: programs can encourage students to ask potential supervisors about how they address culture in supervision or how supervisors view the supervisory relationship. Often, supervisors’ answers to these will give the trainee some clues as to how the supervisor may solicit feedback from trainees or how the supervisor conceptualizes the importance of culture (e.g., does the supervisor name culture as important within a supervisory relationship or focus only on culture related to clients?).
Future research should examine MCO in cross-racial clinical supervision in the context of longitudinal, dyadic studies that better capture the complexity of clinical supervision. This remains a limitation from past research, owing at least in part to the logistical difficulties of recruiting and retaining supervisory dyads (and, even more so, client–supervisee–supervisor triads) to study at all, much less over time. Developing the infrastructure to do so is difficult but would address a substantial need in this area of research. It will also be important for future research to examine how MCO in supervision may function differently based on supervisees’ or supervisors’ intersectional identities, different types of dyads (e.g., BIPOC supervisees with BIPOC supervisors, White supervisees with BIPOC supervisors, White supervisees with White supervisors). Given the importance of supervision to the practice of psychotherapy and the assumption that supervision influences supervisees’ psychotherapy, future research should also examine MCO in the triadic context, studying clients, supervisees, and supervisors over time. Finally, future research should examine more complex relationships between MCO and supervision processes and outcomes; for example, it is possible that more complex mediational or moderated relationships exist.
In conclusion, our results suggest that greater cultural humility and cultural comfort on the part of White supervisors is related to a better supervisory working alliance and greater satisfaction with supervision for BIPOC trainees, and that White supervisors’ cultural humility is also positively related to BIPOC supervisees’ willingness to disclose difficult supervision issues. Our results add to the growing literature demonstrating the importance of MCO. It is evident in clinical training and practice, fostering cultural humility and cultural comfort are key to culturally-responsive care.