
Abstract
In response to negative media attention regarding gender affirming medical interventions (GAMI), the current manuscript explores the content of messages trans and nonbinary (TNB) individuals receive regarding the impacts of GAMI on gender dysphoria. Further, TNB individuals’ experiences of the effects of GAMI on gender dysphoria are described. A sample of responses from 105 TNB participants were analyzed utilizing qualitative content analysis. These qualitative results revealed that the messages participants received were split between trans negative and trans affirming aspects. Relatedly, participants’ experiences also reflected a dichotomy between current limitations and positive impacts of GAMI on gender dysphoria. The discussion focuses on how participants’ positive experiences with GAMI, which resulted in decreased gender dysphoria and psychological distress, challenge the current political discourse that attempts to ban GAMI. Clinical implications focus on how to translate the current findings regarding the limitations of GAMI into more fully informed consent processes.
Keywords
This study highlights the positive impacts of gender-affirming medical interventions (GAMI) on reducing gender dysphoria and psychological distress among transgender and nonbinary individuals, countering harmful societal narratives. By amplifying these lived experiences, the research informs public discourse and guides healthcare providers toward more inclusive and ethical informed consent practices.Significance of the Scholarship to the Public
As of August 18th, 2023 there were 451 anti-trans bills passed or up for debate in the United States, with a majority of these bills targeting health care for trans and nonbinary (TNB) individuals (Trans Legislation Tracker, n.d.). However, this rise in anti-trans legislation is not unique to the United States. India, Uganda, and numerous European countries’ legislative bodies have advanced bills aimed at removing the rights of TNB citizens (Evdokimova, 2023; Yurinova, 2023). This politicized attack on TNB lives has been linked to significant harm, including lack of access to life saving medical care (Alfonseca, 2023) and increased psychological distress (Hughto et al., 2021). In tandem to these political movements, media outlets have run numerous stories regarding what it means to be TNB and to medically transition. In response, TNB individuals are now likely to receive diverse, and at times conflicting, messages about gender affirming medical interventions (GAMI) and their impacts on gender dysphoria. The current qualitative study explores the content of such messages and how they compare to TNB individuals’ experiences of GAMI’s impact on their gender dysphoria.
Gender Affirming Medical Interventions
GAMI, or more colloquially referred to as medical transition, are interventions which masculinize or feminize primary and/or secondary sex characteristics towards an individuals’ affirmed gender composition (Tomita et al., 2019). The most common form of GAMI is hormone therapy, which involves the introduction of exogenous endocrines to generate changes in secondary sex characteristics (Hembree et al., 2017). GAMI also include gender affirming surgeries, among which mastectomy (i.e., chest reconstruction and masculinization) is more common than genital surgery (e.g., phalloplasty, metoidioplasty) for trans men and breast augmentation and genital surgery (e.g., vaginoplasty, clitoroplasty) are equally common among trans women. Nonbinary individuals utilize gender affirming surgeries less often than binary trans individuals (Nolan et al., 2019).
GAMI are reported to not only affect the physical bodies of TNB individuals, but also their psychological well-being through their impact on gender dysphoria. Gender dysphoria is frequently, although not always, experienced by TNB individuals, and can be defined as the distress or discomfort that can be experienced when an individual’s gender identity is different than what is socially expected based upon their sex assigned at birth (Coleman et al., 2022). Numerous previous quantitative studies have reported that the initiation of GAMI reduces scores on measures of gender dysphoria (e.g., van Leerdam et al., 2023) as well as improves scores on psychological well-being (e.g., Rowniak et al., 2019). However, little, if any, peer-reviewed qualitative reports on the impacts of GAMI on gender dysphoria and psychological well-being exist.
Knowing that GAMI reduces gender dysphoria when measured quantitatively is important, but it does not provide the nuanced context for how this reduction occurs or the potential connection to psychological well-being. Assuming the efficacy of an intervention based solely on quantitative changes does not allow nuanced understanding of the mechanisms in action and limits providers’ ability to improve care further. In addition, without understanding the experience, researchers, clinicians, and providers are limited in their ability to describe the necessity of GAMI to legislators looking to ban this care. Most importantly, such lack of information can harm TNB individuals, as they are not able to receive a fully informed consent of possible psychological experiences after starting GAMI.
Messages About Gender Affirming Medical Intervention
As described above, with the recent increase in legislative efforts to ban GAMI, TNB individuals are likely to be receiving far more messages regarding how GAMI supposedly impacts gender dysphoria. Recently, Dhanani and Totton (2023) found that TNB youth and adults spend on average 7 hours a week reading news related to anti-trans legislation, suggesting that these messages are actively sought out by TNB individuals. Importantly, the content of some of these messages contains inaccurate or false information resulting in numerous professional organizations (e.g., American Academy of Pediatrics, American Medical Association, American Psychological Association, World Health Organization, World Professional Association of Transgender Health) to release statements debunking GAMI myths. Frequent myths reported in media include that detransition and regret are common and that GAMI is unsafe, unresearched, and irreversible (National Association of Social Work, n.d.).
The impacts of false and misleading messages about GAMI were documented in a Swedish study that explored the relation between the airing of a two-part documentary series on detransition and regret on national television and corresponding referrals to a child and adolescent gender affirming clinic (Indremo et al., 2022). The results of this study indicated a negative relation, such that exposure to negative media coverage on GAMI was associated with a 25.4% decrease in the number of youths accessing gender-affirming health care over a 3-month period. Further, exposure to negative depictions of TNB individuals in the U.S. news media has been linked to increased symptoms of depression and anxiety (Hughto et al., 2021). Based on the impacts of inaccurate or incomplete messages around GAMI, it is important to understand the content of these messages from diverse sources (e.g., media, friends, family) and how they compare with TNB people’s experiences. Such information is crucial for combating false narratives and for ensuring fully informed consent-procedures.
Statement of the Problem
There is an earnest need to understand both the content of messages TNB individuals receive and the impacts of GAMI on their gender dysphoria. Without this information, TNB individuals must rely on word-of-mouth messaging that has the potential to be biased in either overly positive or negative ways. The impact of this bias could potentially be overly optimistic expectations of the potential ways in which GAMI can reduce their gender dysphoria, or conversely, fear to the extent that it keeps them from utilizing best practice treatments (i.e., GAMI; Coleman et al., 2022). A similar concern exists regarding the experience of GAMI’s impact, where not knowing the nuanced impacts causes researchers, clinicians, providers, and TNB individuals to face limitations with understanding the psychological relation between GAMI and well-being. In response to these concerns, qualitative research presents the opportunity to describe and document both the messages about and impacts of GAMI on gender dysphoria. The present qualitative study represents a community-based, nonclinical sample of TNB individuals, focuses directly on their freely described personal knowledge of GAMI, and addresses the following research questions: (a) What messages have TNB individuals received about the impact of GAMI on gender dysphoria? (b) What are TNB individuals’ experience of the impacts of GAMI on gender dysphoria? (c) How do the messages TNB individuals receive compare to their experience?
Method
Participants and Recruitment
The present study was part of a larger investigation regarding the messages TNB adults receive about GAMI and gender dysphoria. One prior study utilizing this dataset focused exclusively on messages related to gender dysphoria and explored their alignment or divergence from the experiences of TNB individuals (Lindley et al., 2024) . The questions addressed in that study were entirely independent and distinct from those being investigated in the current study. The questions asked of participants for the other study were: (a) What messages have you received from others about gender dysphoria? (b) Where did you hear this information about gender dysphoria? (c) How have your experiences of gender dysphoria been similar to these messages? and (d) How have your experiences of gender dysphoria been different from these messages?
Participant Demographics
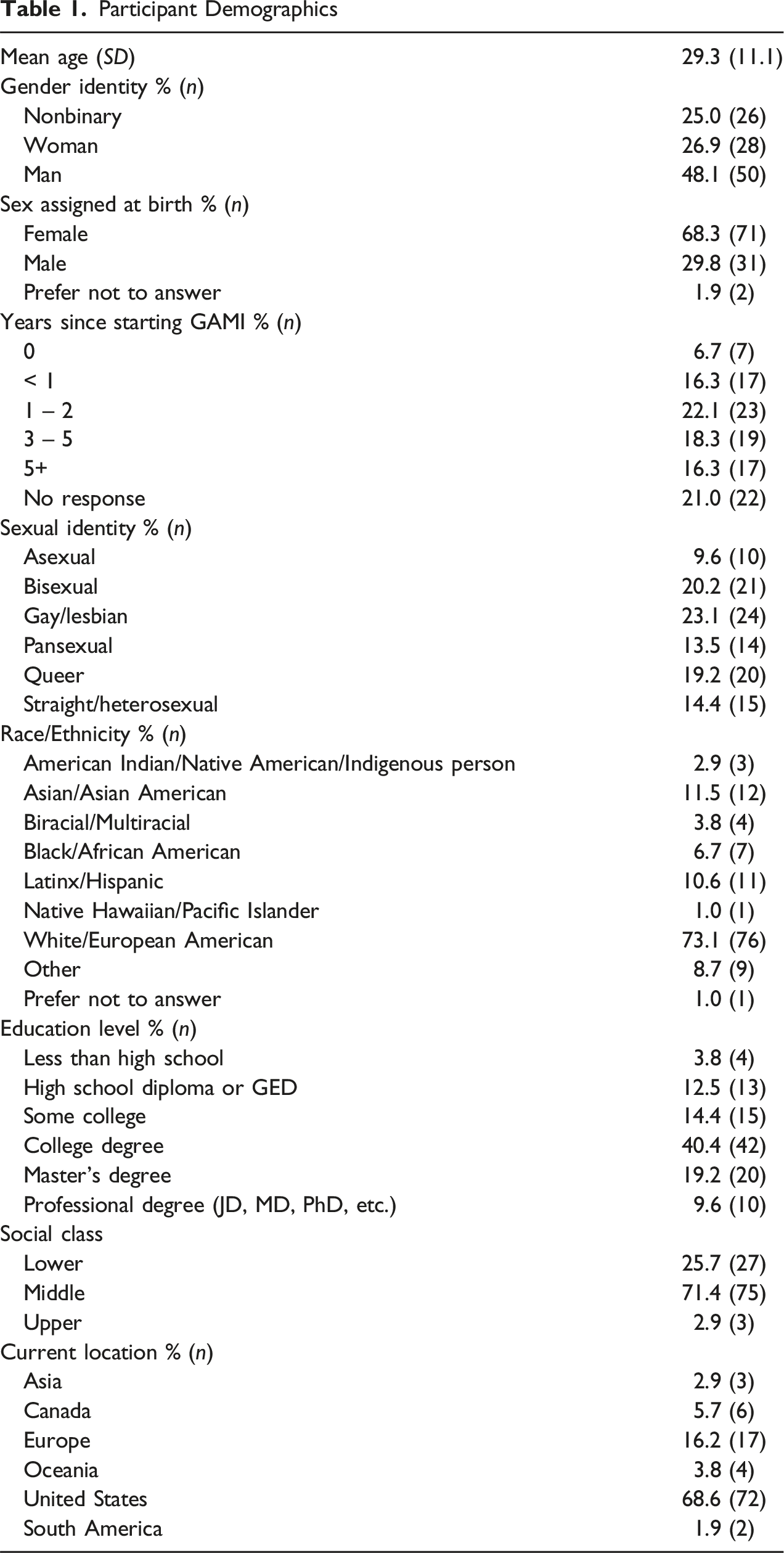
A total of 133 participants completed the survey; however, one participant was under the age of 18 and 28 participants did not provide a response for the prompts analyzed for this study and were removed. The only significant difference between participants who did and did not respond to the prompt was race/ethnicity, where participants who did not complete the prompts were more likely to endorse a white identity. The final sample size of 104 participants endorsed a range of gender identities, including: man (48.1%), nonbinary (25.0%), and woman (26.9%). Participants ranged in age from 18 to 74 years (M = 29.32 SD = 11.12) and had racial and ethnic diversity comparable to U.S. census data (U.S. Census Bureau, 2022) with 64.4% endorsing only a white identity, and 35.6% identifying as a racial or ethnic minority. Table 1 displays the demographics of the sample, including highest level of education and sexual identity.
Procedure
The study was approved by the Institutional Review Board at the University of Wisconsin-Madison. Participants completed an online survey via Qualtrics and at completion, were given a prompt thanking them for their participation, provided an opportunity to leave suggestions to improve future studies, and offered a list of supportive resources. No incentives were provided for participation. This study was not preregistered nor was the data deposited in a publicly accessible database.
Instruments
The online survey included demographic information, a series of 13 open-ended prompts, and quantitative measures of gender dysphoria, alcohol use, psychological distress, and social anxiety. Within the demographic section, participants were requested to provide their gender identity through both a write-in response and fixed choices (i.e., man, woman, or nonbinary). The fixed choice gender identities were utilized in the demographics table, whereas the write-in responses were employed to provide context to quotes. Participants were not limited in the length of the response to open-ended questions and could skip any item they did not wish to answer. Two prompts were used to ask about participants’ experiences with messages regarding GAMI’s impact on gender dysphoria: (a) What messages have you received from others about the impact of GAMI on gender dysphoria? and (b) How have GAMI impacted your experience of gender dysphoria (either actual experiences or your expectations of the impact)? The authors deliberately refrained from providing a specific definition of gender dysphoria to avoid influencing participants’ narratives.
Analytic Methodology
The present study used an inductive approach in which participants’ received messages about and experiences of GAMI’s impacts on gender dysphoria were analyzed using qualitative content analysis. Inductive qualitative content analysis was particularly valuable in studying the impact of GAMI on gender dysphoria due to the dearth of existing research on messages about and experiences related to this phenomenon. This approach involves building understanding and identifying patterns from the ground up, making it well-suited for situations where comprehensive prior knowledge is insufficient or incomplete. Qualitative content analysis involves four primary and sequential steps: (a) familiarization with the data, (b) line-by-line coding, (c) development of categories, and (d) generation of higher order categories (Elo & Kyngäs, 2008). Prior to the initial coding stage, all coding members read through participants’ responses and made notes of their observations. Additionally, the coding team auditor divided participants’ responses into meaning units. In the initial coding stage, meaning units were independently coded line-by-line by each coding member. The coding team then met to discuss the line codes and reach a consensus on final line-by-line codes. Next, the two coding members independently placed the line-by-line codes into descriptive categories to begin to organize the data across participants. Again, the coding team met to collapse and/or combine these categories to consensus regarding the descriptive themes before entering the final stage, generating higher order categories. In this stage, all members of the coding team met together to discuss how the descriptive categories fit together and what higher category captured or explained these phenomena best.
During the coding phase, several steps were taken to increase the trustworthiness of the results. At the end of the survey, participants were given the chance to provide feedback regarding the study’s questions and provide additional context for the research team to understand their answers. A review of this feedback indicated that no participant wished to clarify their answers regarding the prompts analyzed for this study. Next, each category (i.e., subtheme) and higher order category (i.e., theme) was clearly defined and operationalized, following discussion by the coding team. Finally, each participant’s response was given a line-by-line code, ensuring that every participant’s experience was captured in the results.
To juxtapose external messages to TNB people’s experiences, we systematically compared the identified themes on external messages with those derived from participants’ experiences. This comparative analysis allowed us to identify overlaps, where reported messages mirrored participants’ experiences, as well as divergences, where discrepancies or contradictions emerged. Moreover, we paid close attention to nuances within the themes, exploring subtle variations or complexities between external messages and TNB people’s experiences.
Researcher Positionality
The research team consisted of individuals from a range of gender identities, including but not limited to TNB individuals, as well as individuals from diverse racial and national backgrounds, such as Asian and American. The multiplicity of these identities enriched the data analysis process, allowing for a more nuanced understanding of how our own positionalities may influence our interpretation of participants’ experiences. Prior to analyzing the data, the coding team met to discuss our expectations for the results and potential biases. This was an important step, as both members of the coding team (the third and fourth authors) and the coding auditor (the first author) were all trans/nonbinary masculine and white, which can limit our understanding and bias our coding. In this meeting, we discussed our positionalities as participant observers who had varying experiences with gender dysphoria and GAMI, which could contribute to insider knowledge or projecting our understandings onto the participants. In response, we named our potential biases (e.g., expecting transnegative messages, descriptions of positive effects of GAMI, desire for rapid changes) and discussed how to hold each other accountable when they came up (e.g., questioning assumptions, being more attentive to content related to Black, Indigenous, and people of Color or trans femme experiences). This allowed us to increase the rigor of our process and ensure trustworthiness of the results by allowing space for processing how our own identities may have impacted our understanding of participants’ experiences, and for reflection on how our respective social identities, as well as our power dynamics within our research group, may have impacted our process. The authors took notes of these possible biased expectations and frequently returned to them throughout the coding process to engage in bracketing. Finally, prior to and after each coding meeting, the coding team discussed their personal reactions to the data, to further process personal biases, understand our reactions to potential shared experiences with participants, and to engage in bracketing of our identities.
Results
Thematic Structure for the Messages Prompt
Thematic Structure for the Experiences Prompt
Receiving External Messages
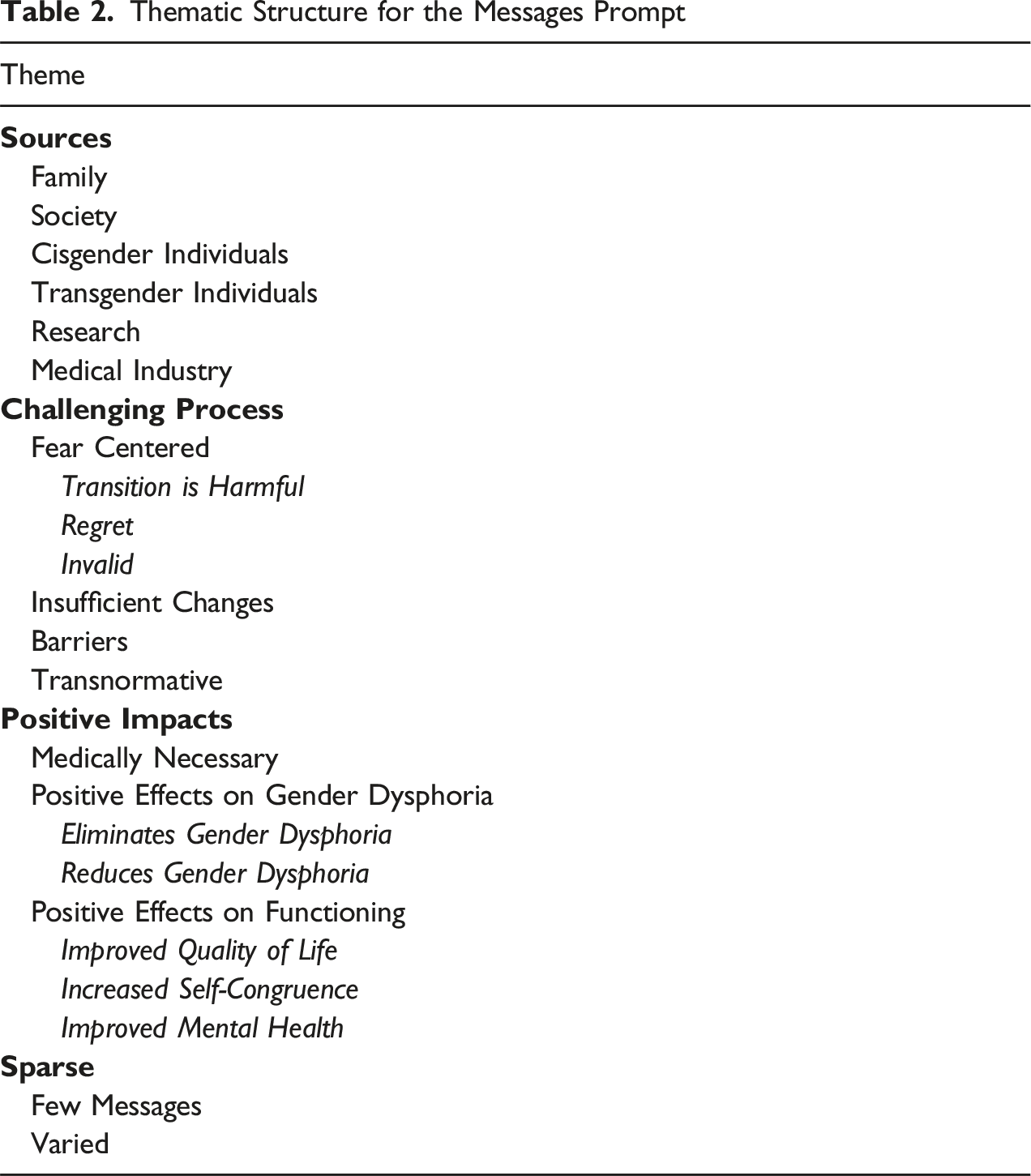
Qualitative content analysis of participants’ responses to the prompt, “What messages have you received from others about the impact of GAMI on gender dysphoria?” revealed four main themes: the sources of messages, messages around GAMI being a challenging process, messages affirming the positive impacts of GAMI, and sparse messages (see Table 2). Some participants’ quotes included all four themes. This indicated that some TNB individuals received mixed and/or multilayered messages regarding GAMI’s expected impacts on gender dysphoria.
Sources of Messages
Although participants were not directly asked to name where they received messages about the impact of GAMI on gender dysphoria, some participants included the source in their response. These sources included “family” (Chilean/Filipino American, man), “society” (Latinx, nonbinary), and from “cis community” (white, transgender male/male). Other participants noted that messages came from “within the [trans] community” (white, transgender male) and from “other who were further along [with medical transition]” (South-East European, Balcan, genderqueer). Finally, participants mentioned “research” (white, genderqueer) or “medical or mental health literature” (white American, transmasculine, genderqueer) and a “bitch medical industry fixated on cure” (white, a fucking nuisance but also genderqueer).
Messages Around Gender Affirming Medical Interventions Being a Challenging Process
The present theme involved descriptions of messages that centered on how medical transition can be a challenging process. Subthemes of these challenges included receiving messages: that centered fear about GAMI, that GAMI may lead to insufficient changes, described barriers in access, and contained transnormative content. Overall, participants described these messages as containing content aimed at discouraging individuals from pursuing or continuing GAMI.
Fear Centered
The subtheme of fear-centered messages involved “lots of fearmongering about negative impacts of medically transitioning” (white American, transmasculine, genderqueer). One aspect of this “fearmongering” included references to the supposed “harmful” (Chilean/Filipino American, man) aspects of GAMI that “hurt your body” (Latino, male). For example, “that getting bottom surgery without proper channels can make you homicidal” (white, woman, metabinary). Other participants indicated that folks in their lives expressed “‘concerns’ about ‘mutilation’” (white, trans man), with one participant sharing that his “own father has referred to it as ‘mutilation’ and told me it is a mistake” (white Irish, male). Finally, one participant shared that “antagonist claim … that it is ‘enabling self-harm’” (white, agender, nonbinary). Participants also described messages centered around regret. Key aspects of regret involved “stressing that hormones and surgery are irreversible” (Latinx, gender non-conforming transmasculine person/guy) and that “HRT [hormone therapy] ruins lives” (white, male). As a result, these messages indicated that TNB people “are unhappy and detransition” (Caucasian, man). A final aspect of fear-centered messages placed an emphasis on invalidation, that GAMI are “wrong” (Caucasian, Mohawk-Abenaki, two-spirit), “too strange” (European, male, trans man), or “a fad” (white Irish, male). Rather than seeking GAMI, these messages instructed participants to “wait” or “try to change [their] mind/feelings rather than [their] body” (Latino, male).
Insufficient Changes
The subtheme of insufficient changes describes messages received regarding the “medical limitations” (white, Scandinavian American, female) of current GAMI options. For example, participants reported receiving messages from others that GAMI are “not a cure at all” (white, German, female), “won’t always cure dysphoria” (Black, transmasculine nonbinary), and “that they don’t help” (Chinese Singaporean, male). Others noted “that there will always be some vestige of gender dysphoria left” (Scotch-Irish, transgender female) because medical interventions are “currently incapable of eliminating [gender dysphoria]” (white, female). Other messages highlighting the insufficiency of GAMI include “still [having] social problems to deal with” (white, woman), “feel[ing] dysphoria in new places” (white, trans man), or “never being able to have functioning male genitalia” (human, American, woman). One participant described these messages as centering on trying to convey that medical transition “isn’t convincing” (white, nonbinary).
Barriers With Access to Gender Affirming Medical Interventions
The barriers subtheme describes messages that centered how GAMI is “astronomically expensive and thus unavailable to the majority of trans people” (white/Hispanic, transgender female) or highlighted “the amount of time, money, and effort it takes to be able to access [GAMI]” (white American, nonbinary, maverique, autigender). Overall, participants received messages denoting “that it’s hard” (Asian, genderqueer) to receive or begin GAMI processes.
Transnormative Messages
The final subtheme of challenging messages involved messages that reproduced a key aspect of transnormativity, specifically, who is “really trans.” For example, content of messages included “that medical transition is a requirement to be ‘really trans’” (white American, transmasculine, genderqueer) and that “if someone genuinely has gender dysphoria, medical transitions will help alleviate it” (Caucasian, American, transgender man). Conversely, other participants’ messages contained the opposite message, “medical transition shouldn’t be seen as a ‘requirement’” (South-East European, Balcan, genderqueer, nonbinary) and “that you don’t need dysphoria to be trans” (white, male).
Messages Affirming the Positive Impacts of Gender Affirming Medical Interventions
In contrast to the challenging messages, trans-affirming messages involved descriptions of the positive impacts of GAMI. Subthemes of trans-affirming messages described GAMI as being medically necessary and the positive effects of GAMI on gender dysphoria and overall psychosocial functioning. Whereas challenging messages contained contentment intended to dissuade participants, trans-affirmative messages highlighted the positive impacts of GAMI and provided encouraging content.
Gender Affirming Medical Interventions Being Medically Necessary
One aspect of the trans-affirmative messages described GAMI as “necessary to treat dysphoria” (white, transsexual woman). Participants described messages that medical transition is “the only way to “get rid” of dysphoria [and is] essential [for] transitioning” (white, transgender male). With one participant noting messages suggested that medical transition is “the only thing that will fix my gender dysphoria” (white, male).
Positive Effects of Gender Affirming Medical Interventions on Gender Dysphoria
Participants also described receiving messages noting positive effects of GAMI on gender dysphoria. These effects ranged from elimination to reduction of gender dysphoria symptoms. For example, on the elimination range, participants described encountering messages that GAMI “makes [gender dysphoria] go away” (Caucasian, transfeminine), “fixes everything” (white, nonbinary), and “cures dysphoria” (European, African, Asian, Native American, male). Whereas other messages noted that GAMI can reduce gender dysphoria, such as it “helps with alleviating [gender dysphoria]” (European, African, Asian, Native American, male) and “can reduce dysphoria” (white, trans feminine).
Positive Effects of Gender Affirming Medical Interventions on Functioning
Finally, although unprompted, participants described encountering messages about GAMI having positive effects on their overall functioning. For example, participants noted that messages indicated that GAMI “save lives” (Black, male) and “are imperative to live” (white/Hispanic, transgender female). Others reported messages describing the “life-altering” (white transgender male) and “life-changing” (white, male/transmasc) benefits. Finally, some participants noted that “medical transition can be a miracle” (white, transsexual male).
Participants also described messages that GAMI can result in increased self-congruence, for example allowing TNB people to “become who [they] are on the outside as well as the inside” (Australian, Caucasian, male). Others described these self-congruence messages as allowing TNB people to “feel at home in their bodies” (white, gender fluid, nonbinary, trans-masc) and “finally feel like themselves” (white, man) by “making your body more aligned with your gender identity” (Asian, male). Finally, participants received messages that GAMI positively impacts psychosocial functioning, such as “helping mental health as well” (white, man). These messages described GAMI as “cur[ing] the suffering” (Caucasian, female) through “reliev[ing] the stress I get from gender dysphoria” (Latino/white of Italian descent, male).
Sparse
The final theme of messages regarding the impact of GAMI on gender dysphoria was sparse, which reflected participants who indicated that they received few messages or that the messages they did receive were varied in nature. For example, one participant noted that “I haven’t really talked to others about [GAMI]” (white, male) and thus they had not received messages, whereas another indicated that “few comment on [GAMI]” (Black, Korean American, transman). Other participants indicated that messages they received were “varied” (white British, male) or “mixed” (white, transgender male/male). As a white trans woman explained, “information from other trans people varies *wildly* depending on their results, personal experience of dysphoria, and general mental health.”
Experiences of Gender Affirming Medical Interventions’ Impacts on Gender Dysphoria
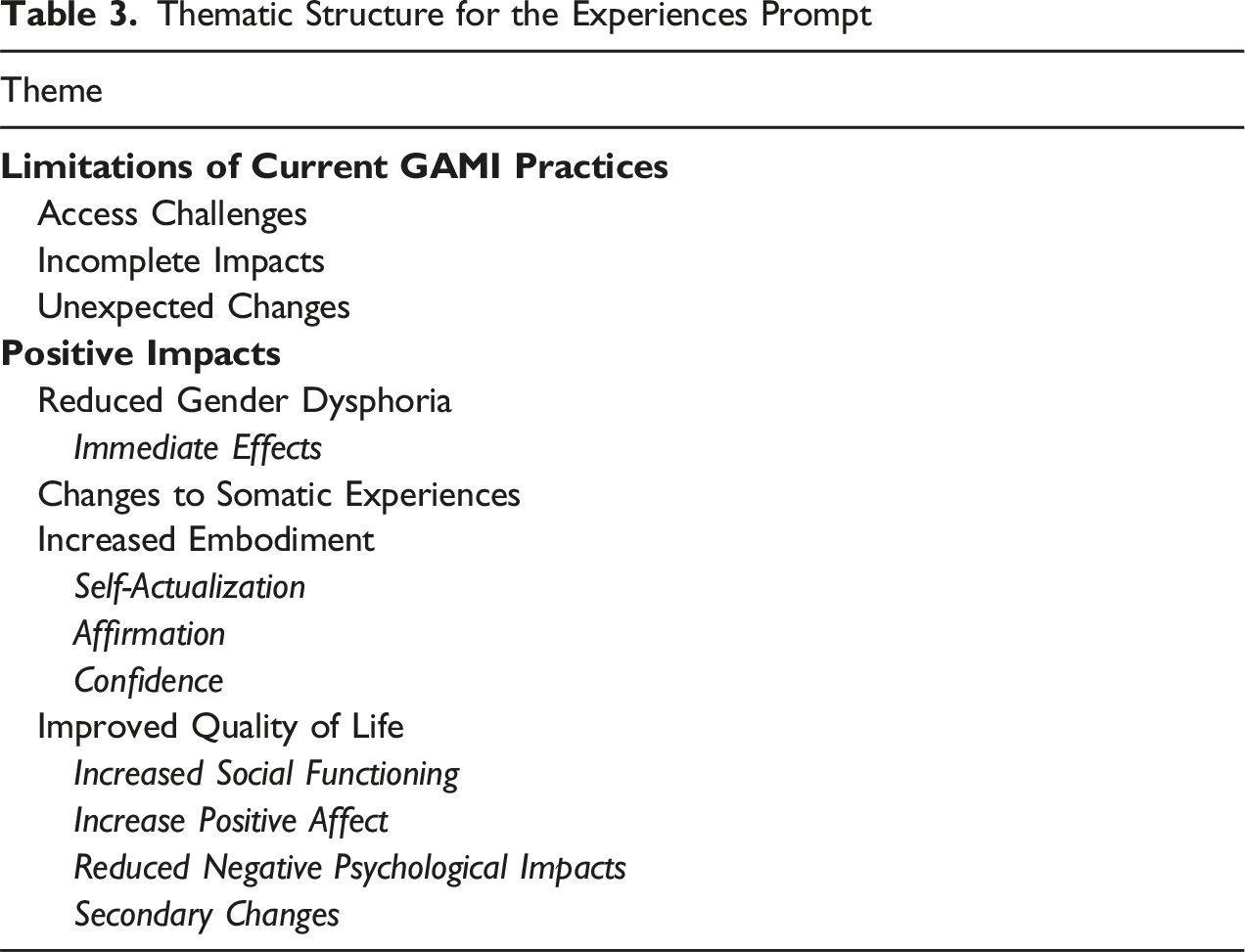
Qualitative content analysis of participants responses to the prompt “How have GAMI impacted your experience of gender dysphoria (either actual experiences or your expectations of the impact)?” uncovered two main themes: limitations of current GAMI practices and positive impacts of GAMI (see Table 3).
Limitations of Current Gender Affirming Medical Interventions Practices
The present theme described experiences that involved some form of hindrance in participants’ experience with GAMI in addressing gender dysphoria. This hindrance was described in three subthemes: challenges in accessing GAMI, incomplete impacts of GAMI on gender dysphoria, and unexpected changes.
Challenges in Accessing Gender Affirming Medical Interventions
Participants who were yet to access all of their desired GAMI noted that some GAMI were
Incomplete Impacts of Gender Affirming Medical Interventions on Gender Dysphoria
Within this subtheme, participants explained how GAMI had an incomplete impact on their gender dysphoria. For example, participants noted that “hormone treatment has significantly decreased my dysphoria in some ways, while others remain” (white, trans-masc, nonbinary). For some participants, this remaining gender dysphoria reflected a shift; their gender dysphoria redirected to new locations or sources of distress after initiating GAMI. Participants indicated that although GAMI resulted in reduced gender dysphoria in certain areas, it became more intense in other parts of their bodies. For example, “things like hip dysphoria have gotten worse since top surgery since I don’t have to focus on the worst of it, my chest” (white, trans man). A white trans woman described a “felt increased need to voice train, get laser hair, get facial feminization surgery, and so on” after seeing the positive effects of hormone therapy. Overall, participants’ experiences of redirected gender dysphoria involved “draw[ing] attention to other dysphoric features” (South Asian, transfeminine).
For others, GAMI’s incomplete impacts on gender dysphoria resulted in “still occasionally experiencing [gender dysphoria]” (white, trans woman), often due to not having accessed genital gender affirmation surgeries yet. Some participants indicated that their “dysphoria is not gone entirely” (white, male) and that they “still have a lot of bad body dysphoria even though I pass” (white, transfeminine, trans woman). Finally, some participants described GAMI as incapable of creating the desired changes they wanted. For example, “there is no medical way for me to achieve a look that would make me happy and relieve my physical dysphoria” (white, nonbinary trans guy).
Unexpected Changes
Participants also described how they experienced unexpected and undesired changes because of GAMI. As described by a white transgender male, “I have a higher voice even on HRT, and I have hypertrophic top surgery scars, so it’s done a number on me.” Another participant noted that “GAMI increased my dysphoria when I was getting hrt changes I did not want” (white Australian, nonbinary). For these participants, GAMI had the opposite effect than what was desired (i.e., increased distress).
Positive Impacts of Gender Affirming Medical Interventions
Positive impacts of GAMI described participants’ experiences that involved increased well-being. These positive impacts were described in four subthemes: reduction in gender dysphoria, changes in somatic experiences, increased embodiment, and improved quality of life.
Reduction in Gender Dysphoria
As could be expected, participants named that GAMI reduced their symptoms of gender dysphoria. This reduction was described as “dramatic” (white American, transmasculine, genderqueer), “great” (white, trans feminine), and “significant” (Latinx, trans woman), with folks indicating that “overall, I feel less dysphoria” (white, trans masc nonbinary). With some participants indicating that both the
Immediate Effect
Importantly, participants also indicated that this reduction to gender dysphoria could occur immediately following the first administration of GAMI. For example, a white trans masc nonbinary participant indicated that “as soon as I began T [testosterone], it is hard to describe, but I had an immediate reduction in dysphoria because something just felt right inside.” Another participant went on to explain how this rapid reduction felt psychologically, “just the change in hormones present in my system resulted in a dramatic reduction of my feelings of dysphoria” (Scotch-Irish, transgender female). Participants who described an immediate change noted that the reduction in gender dysphoria happened prior to any physiological changes: “I suddenly felt a wave of calm and mental peace 8 hours into first T shot for the first time since before puberty, despite no visible physical changes” (Chinese Singaporean, male) and “after starting HRT, the majority of my dysphoric depression was gone within a week, before any visible changes” (white German, female).
Changes to Somatic Experiences
Participants also described the impact of GAMI on their physical body, specifically how it changed their relationship with their body. For example, Chest surgery had a much stronger impact than I expected it to. I didn’t think that it was that important to me until I had it, but after I did, I felt much better about my body overall … it made me feel like my whole body was more masculine, and that I was more masculine. (white, European American, male, FtM)
Another explained it as “I’m comfortable enough in my body now that it doesn’t bother me near as much when I do have a period … testosterone’s effects on clitoral growth mostly relieved the sensation of a ‘phantom penis’” (white, female-to-male). Participants who had not initiated or were desiring more GAMI noted what they expected to happen, such as “I’ll be more comfortable in my body” (Asian, male) and “after all my surgery, I think I will be able to see my whole body in the mirror, use the bathroom comfortably, and shower comfortably” (white, male, trans male).
In addition, participants described positive secondary changes from GAMI, such as “I’ve got facial hair, which I dreamt to grow since I was about 4 y/o” (Latino, male) and how these changes “have alleviated the feeling I used to have of being distressingly bare, like a feeling of always being ‘naked’” (white, female-to-male). Participants whose voice changed because of GAMI indicated that “my voice is not holding me back from participating in class or talking to store clerks anymore” (white, male).
Increased Sense of Embodiment
In addition to the expected physical changes from GAMI, participants also described how these interventions improved their sense of embodiment. Participants described how they experienced increased self-actualization. Often, participants noted that they “LOVE that I am becoming who I am” (Caucasian/white, transman) and “love everything about myself so much more now, and that is more true every day” (no race provided, trans, genderfluid, demi-guy). Further participants described being able to “recognize myself in the mirror” (white, trans man) and “see myself with all of my senses” (European, African, Asian, Native American, male) which has allowed them to “become who I envisioned” (Black, male), and “get near my physiological image of myself” (white European, female).
Affirmation was another salient aspect of increased embodiment. Participants noted that GAMI allowed them to “look like me” (white, trans man) and “feel far more connected to my body” (South Asian, transfeminine). Further, GAMI helped participants to “accept and validate myself” (Caucasian/white, female/mtf) and provide the “body I was ought to always have” (Russian, white, male).
Finally, participants indicated that embodiment was also available to them through feeling “a lot more confident wearing whatever I want” (Latinx, gender non-conforming transmasculine person/guy) or expecting to “wear what I want to without feeling like I have a chest” (Caucasian, genderfluid, nonbinary). A white nonbinary, transmasculine participant explained it best, “knowing that I actually CAN wear all my feminine things at the same time as I show off chest hair and a beard? … yeah. That helps a lot.”
Improved Quality of Life
The last subtheme, improved quality of life, discusses participants’ descriptions of the ways GAMI positively impacted their functioning. Overall, participants described GAMI as “totally chang[ing] my life” (white, transgender male). This was often due to becoming a “functional person” (white, trans man) who was “able to do a lot of things I couldn’t do before” (Black, trans male) by “[making] it easier to engage in daily life” (white, male/trans male). The improved quality of life subtheme was described across four categories: increased social functioning, increases in positive affect, reduction of negative psychological impacts, and experiencing secondary changes.
Increased Social Functioning
Participants noted that GAMI improved their social lives through making it easier “to engage in social interactions” (white, agender, transgender, non-binary) and “and no longer feel[ing] like a fly on the wall” (European, African, Asian, Native American, male). A white trans woman indicated that this improvement was related to “socially presenting and passing as female” which “has provided immense relief from a great deal of my dysphoria” and another explained that for her it was related to a decreased “fear people will misgender me as much.”
Increase in Positive Affect
Changes to participants’ psychological affect were also described. For instance, participants’ described feeling “confident and comfortable” (white, male/transmale), as if they “can go anywhere with confidence of being seen appropriately” (Black, Korean American, transman). Others noted feeling “happier” (white, female) or expecting to “be happy someday” (white, nonbinary, transmasculine). For others, GAMI provided hope for the future. For example, “most immediately, it gave me hope for the future” (white, transgender man), which as a Caucasian French man put it, “I often feel desperate [because of gender dysphoria] but with what is possible today, I have hope.”
Reduction of Negative Psychological Impacts of Gender Dysphoria
Related to improved psychological affect, participants additionally described how GAMI impacted their mental health by reducing the impacts of gender dysphoria. Most importantly, participants noted that GAMI lessened their suicidal ideation. A Russian white male participant stated that simply “finding out about surgeries and hormones made me stop my plans to commit suicide because it gave me hope.” For another participant who had “struggled with suicidal ideation, anxiousness and lack of motivation” through engaging with GAMI “most of this has been improved” (white, female).
Participants also described that their “head space changed” (Scotch-Irish, transgender female) and that they “can think straight” (white, trans man) and “their brain feels clearer” (Latinx, trans woman). For some participants, GAMI also affected them emotionally, such as creating “the capacity for the full range of emotion and expression” (white, man) and “regulating my emotional responses” (white, trans man). One participant exclaimed that “my mood improved by an almost unbelievable amount for the first few months” (Asian American, white, male). Finally, participants noted “it also improved my overall mental health far more than I thought it would” (white American, transmasculine, genderqueer) and “my overall mental health has significantly improved” (South Asian, transfeminine). For one participant, “even just getting the confirmation that I will see a gender therapist after 2 years of waiting has made me significantly less depressed” (white Irish, trans man).
Experiencing Secondary Change
Lastly, participants
Comparison of External Messages to Experiences
Participants’ reported messages regarding the impact of GAMI on gender dysphoria exhibited a complex relationship with their experiences. In certain cases, these reported messages mirrored participants’ lived realities, whereas in other instances, discrepancies or subtleties emerged, reflecting a more nuanced understanding of their experiences. Notably, participants’ experiences with barriers associated with GAMI echoed the challenges highlighted in the messages, emphasizing issues such as high costs and the significant time, money, and effort required for access. Conversely, although certain messages attempted to instill fear about the negative impacts of GAMI, such as its supposed harmful effects, concerns about mutilation, and claims that GAMI could lead to self-harm, none of the participants in this study reported experiencing regret, mutilation, or harm. Instead, many participants highlighted positive experiences, such as alleviated gender dysphoria, improved mental health, increased self-esteem, and a stronger sense of authenticity.
In terms of GAMI’s impact on gender dysphoria, external messages varied from claiming no effect to suggesting complete eradication. Participants’ experiences reflected this range, with some reporting partial relief and others complete elimination of gender dysphoria. Notably, the experiences of participants added nuance, revealing why GAMI may not eliminate gender dysphoria for all participants. Although GAMI alleviated distress related to specific body parts for some, it sometimes resulted in other aspects of gender dysphoria becoming more prominent. Additionally, some participants found that currently available GAMI were unable to create desired physical gender characteristics or resulted in undesired changes. These nuanced differences likely explain the range of effects participants reported receiving in messages, as their experiences demonstrate the complex and varied outcomes of GAMI.
Furthermore, participants’ accounts of their own experiences shed light on how the positive messages regarding the benefits of GAMI on functioning were manifested in reality. Participants reported increased social functioning, elevated positive mood, reduced negative psychological effects, and secondary changes that facilitated a more comprehensive engagement in social interactions. Collectively, these secondary impacts of GAMI, beyond addressing gender dysphoria, are likely what contribute to the life-saving narrative reported in some messages. In summary, the examination of participants’ reported messages alongside their experiences regarding the effects of GAMI on gender dysphoria reveals a dynamic interplay between societal narratives and personal realities.
Discussion
The present study aimed to (a) explore the external messages that TNB individuals encounter regarding the impacts of GAMI on gender dysphoria, (b) understand their experiences related to the impact of GAMI on gender dysphoria, and (c) compare the messages they received to their experience. Amidst a surge of anti-trans legislation and media coverage on the significance (or perceived insignificance) of GAMI in enhancing the lives of TNB individuals, our goal was to amplify the experiences of TNB people concerning the influence of GAMI on gender dysphoria.
Although some TNB individuals indicated they had not encountered external narratives about the effects of GAMI on gender dysphoria, others were exposed to diverse and occasionally conflicting information. Challenging narratives surrounding GAMI essentially acted as gatekeepers to TNB identities, implying that the need for GAMI to address gender dysphoria is a prerequisite to legitimately identifying as TNB. These narratives embody transnormativity, asserting that TNB individuals can only validate their identities through utilizing GAMI and adhering to binary frameworks (Bradford & Syed, 2019). Prior scholars have documented how transnormative messages impact TNB individuals’ decision making, as they grapple with whether or not they are “trans enough” to engage in GAMI (Murawsky, 2023). This underscores the importance of addressing and challenging transnormative perspectives to promote a more inclusive and supportive environment for TNB individuals with their healthcare decisions (Murawsky, 2023).
On the other hand, participants received external messages that aligned with contemporary scientific findings that GAMI is medically necessary (Coleman et al., 2022), reduces impacts of gender dysphoria (see van Leerdam et al., 2023), and increases psychosocial functioning (Rowniak et al., 2019). Given that factual and evidence-based information should be at the forefront of public discourse for medically necessary care (Brownson et al., 2009), messages about GAMI that are based on scientific evidence should be further distributed and amplified. This approach reinforces the efforts of professional organizations in actively publishing statements that debunk inaccurate information about GAMI, ensuring a more informed and accurate public understanding.
TNB people’s experiences of the positive impacts of GAMI on gender dysphoria corroborates substantial prior research findings that indicate GAMI significantly lowers gender dysphoria and psychological distress (e.g., van Leerdam et al., 2023). Importantly, participants’ qualitative descriptions specified the ways in which GAMI impacted both their gender dysphoria and psychosocial well-being, including suicidal ideation, indicating a strong psychological impact. Participants reported that GAMI significantly improved their embodiment, increased social capacity, and hope towards the future, underscoring the critical role of gender in identity and social well-being. This adds depth to existing literature, shifting the myopic focus on physical changes post-GAMI to the medical necessity of GAMI in facilitating individuals’ holistic realization of their self.
Notably, our study findings on TNB people’s descriptions of challenging experiences uniquely add a nuanced and important understanding of how GAMI practices might not fully address every aspect of gender dysphoria. Within political discourse, experiences of imperfection or dissatisfaction are often used to gatekeep TNB people’s access to GAMI despite overwhelming evidence of its medical necessity (Marrow, 2022). Our study participants provided valuable insights into the potential origins of unsatisfactory GAMI experiences, highlighting scenarios where individuals could access one form of GAMI (e.g., hormone therapy), but faced barriers in accessing another type (e.g., genital surgery). Aligned with numerous prior findings, such barriers in access included lack of insurance coverage and prohibitive costs (e.g., Puckett et al., 2018).
Participants also noted that undergoing certain GAMI procedures sometimes intensified their gender dysphoria in other areas of their body. This phenomenon may be attributed to an increased alignment with their gender in certain body aspects, subsequently highlighting incongruities in areas that were not affected by GAMI (e.g., voice). Scholars have recently proposed that gender dysphoria is fluid and dynamic, noting that it can change across time, context, and locations on the body (e.g., Lindley et al., 2023). The participants’ experiences of shifting gender dysphoria likely signify changes in the focus of body discordance rather than implying that GAMI is ineffective in holistically reducing gender dysphoria.
Collectively, these findings emphasize that, contrary to political narratives that advocate for banning TNB individuals from receiving medically necessary care, dissatisfaction often arises more from insufficient TNB-affirming care than from the act of transitioning itself. For example, within prior research, TNB individuals reported their dissatisfaction with GAMI was related to discontent with cosmetic results, pain, and surgical complications such as scarring (Frederick et al., 2017; van de Grift et al., 2018). Further, reported pooled prevalence of regret for gender affirming surgeries is < 1% (Bustos et al., 2021). This underscores the importance of allocating more resources to TNB-affirming care to enhance quality of care rather than to ban it. The results further emphasize how crucial it is to prioritize client needs, goals, and access to improve GAMI experiences for TNB individuals.
Limitations and Future Directions
The findings of this study should be contextualized within its methodological limitations. Both recruitment and the survey were conducted online using a convenience sampling approach. As a result, a significant proportion of our respondents were young, white, assigned female at birth, highly educated, TNB adults based in the United States. This demographic skew might have influenced the types of messages they received and their personal experiences concerning the impact of GAMI on gender dysphoria, thus limiting the study’s generalizability to the broader TNB population. In subsequent research, it will be critical to explore how TNB people of Color experience impacts of GAMI on gender dysphoria, as they navigate a white supremacist and racist society where bodies of Color are regarded differently in value. Furthermore, in the current study, we broadly examined the impact of GAMI on gender dysphoria. However, future research would benefit from delving into how specific types of GAMI affect distinct forms of gender dysphoria (e.g., body, social, mental), building upon the insights from this study. Such focused exploration will offer a more nuanced understanding of the experiences of TNB individuals.
Implications for Practice, Advocacy, Education and Training, and Research
The present study elucidates external messages that TNB people receive on the impacts of GAMI on gender dysphoria and their experiences of this relation. It is noteworthy that some messages cautioned against the initiation of GAMI, recommended delays in treatment, or framed GAMI as a harmful mutilation of the body. Such messages perpetuate myths that have been consistently refuted by professional organizations. Further, prior research has indicated that such inaccurate and biased information correlates with reduced referrals to gender affirming health centers (Indremo et al., 2022), which can lead to delays in care linked to worsened mental health outcomes and increased suicidality (Jarrett et al., 2021). It is vital for healthcare professionals to recognize the widespread presence of these inaccurate narratives and proactively intervene by sharing evidence-based information, while policymakers should focus on diminishing barriers in access to GAMI. Considering that this data was collected in 2021, prior to the full impact of recent anti-trans bills, the results emphasize the escalating need to decrease obstacles for TNB individuals to access essential medical care.
Participants in the current study experienced lower satisfaction from GAMI than they had anticipated when there was a lack of sufficient existing surgical techniques or inadequate disclosure of risks and benefits by clinicians prior to GAMI. The World Professional Association of Transgender Health Standards of Care (8th edition) requires that TNB patients be fully informed of any potential side effects of GAMI prior to initiating care (Coleman et al., 2022, p. 8). However, participants who mentioned experiencing unwanted or unforeseen changes from GAMI often cited side effects inherent to the procedure. Thus, it is crucial to increase clinician competency when providing comprehensive informed consent both before and after GAMI procedures. During the informed consent process, clinicians should engage in detailed, yet affirming, discussions about the potential risks and benefits of specific GAMI procedures. Acting as a companion within the medical system, clinicians should address and assist with any client concerns or potential challenges that may arise pre- or post-GAMI. Throughout the process, it is essential to foster an affirming environment that establishes safety and trust between clinician and client, ensuring that clients feel comfortable voicing their concerns (Budge et al., 2023).
Healthcare professionals and clinicians involved in GAMI services should be aware of the potential for heightened or redirected gender dysphoria among TNB clients during specific types of GAMI. Instead of invalidating these emotional experiences, it is important to delve into the feelings, supporting clients in their journey towards acceptance and embodiment. Clinicians must be aware of ways to explore such shifting experiences with clients while also expanding access to essential GAMI procedures. To enhance their competency, clinicians should familiarize themselves with trans-specific strategies for coping with gender dysphoria (see Lindley & Budge, 2022; Lindley et al., 2023). This includes understanding the unique challenges TNB individuals may face and discussing effective strategies to alleviate distress during and after GAMI. By fostering open communication and addressing emotional well-being, healthcare providers can play a vital role in supporting TNB clients throughout their gender-affirming journey.
Lastly, drawing from the findings of the current study, we advocate for future research to delve deeper, using qualitative methods, into how external messages directly influence TNB individuals’ experiences with GAMI and impact their mental health. This is particularly pertinent in the current political environment where numerous negative narratives about GAMI prevail.