
Abstract
Marginalized individuals often work within systems that invalidate their worth, identity, and contributions. These systems, whether in academia, healthcare, education, or corporate spaces, perpetuate psychological distress through microaggressions, gaslighting, exclusion, and structural oppression. In such environments, self-trust becomes not only difficult but radical. Thus, this article introduces the TRUST Model, a healing-centered, liberatory framework that explores how individuals—especially those from historically marginalized communities—reclaim and sustain trust in their internal voice and truth. Rooted in healing centered engagement theory and liberated cognitive behavioral theory, the TRUST model comprises five interrelated domains: (1) Tuning Into Invalidation, (2) Recognizing and Renaming the System, (3) Uncovering and Reclaiming Your Inner Voice, (4) Strategizing for Resistance and Protection, and (5) Tending to Healing and Reconnection.
Significance of the Scholarship to the Public
This article explains how people who experience exclusion and invalidation can learn to trust themselves again, even in harmful systems like workplaces, schools, and healthcare settings. It introduces a practical model (TRUST) that helps individuals recognize harmful dynamics, reconnect with their inner voice, and protect their well-being. This work is important because it offers clear, accessible tools for healing and empowerment, especially for people from marginalized communities.
Invalidation for people of color often reflects broader systemic patterns rather than isolated incidents, with each dismissal reinforcing historical and ongoing experiences of marginalization. It is a repeated and cumulative experience often embedded in the very fabric of institutions and systems that were never constructed to affirm the humanity, cultural identities, or lived realities of people of color and other historically marginalized groups (Sim & Bierema, 2025). From education and healthcare to corporate and legal structures, these systems reflect cultural norms that subtly and overtly devalue the perspectives, bodies, and voices of those who do not conform to Whiteness, cisnormativity, able-bodiedness, or other dominant identities (Quint et al., 2025; Stoll et al., 2025).
Individuals navigating invalidating systems often face chronic and layered forms of erasure (Coles & Pasek, 2020). These forms of erasure may include microaggressions that diminish one’s perceived competence, tone policing that silences one’s freedom of expression, institutional betrayal that fractures trust in leadership, and exclusion from decision-making spaces that reinforce feelings of invisibility (Bhattacharyya & Berdahl, 2023; Sue, 2011; Suh et al., 2024; Williams & Embrick, 2023). Although these acts may be dismissed as minor or unintentional by those in power, their cumulative effect is profound. System invalidation not only causes external harm but also seeps inward, teaching people to question their own feelings, mistrust their perceptions, and sometimes internalize negative messages, which warps the way they see and relate to themselves. Over time, this can lead to racialized trauma responses that chip away at self-trust, causing individuals to second-guess their judgment and intelligence, suppress their emotions, and question whether they truly belong (Carter & Pieterse, 2020; El Kassar, 2021; Howard & Hinton, 2016.
In response, purposefully cultivating self-trust becomes both a psychological tool of survival and a form of intentional resistance. Self-trust is not simply about boosting confidence, it is about reclaiming one’s truth in environments that deny it. The TRUST model was developed to map this psychological and relational journey. Rooted in healing-centered engagement (Ginwright, 2018) and liberated cognitive behavior therapy (Sawyer, 2023), the TRUST model offers a process-based, identity-affirming, and resistance-oriented framework for healing. It recognizes that restoring trust in oneself is a radical act—one that requires awareness, intentionality, and community. Through its five interrelated domains, the model guides individuals in identifying invalidating dynamics, reclaiming their internal wisdom, and practicing strategic self-advocacy in the face of systemic harm. The steps of the model include (1) Tuning Into Invalidation, (2) Recognizing and Renaming the System, (3) Uncovering and Reclaiming Your Inner Voice, (4) Strategizing for Resistance and Protection, and (5) Tending to Healing and Reconnection.
The remainder of the article begins with a review of the literature exploring the psychological toll of invalidating systems on diverse populations and the concept of self-trust. The TRUST model is then presented, first highlighting the theories undergirding the model, followed by the domains of the model. The article concludes with a discussion of implications.
The Psychological Impact of Invalidating Systems
Invalidating systems are those that deny the reality of discrimination and prejudice, minimize its impact, or blame victims for the consequences of their oppression (Bryant-Davis & Ocampo, 2006; Parmenter et al., 2024). One illustration of this can be seen in predominantly White institutions, where individuals from racially marginalized backgrounds often carry the invisible labor of representing diversity, educating peers, and suppressing their emotional responses to bias in order to appear “professional.” These conditions create what Hochschild (1983) termed “emotional labor,” magnified by race and systemic inequality. A convergence of research demonstrates that exposure to this type of invalidation contributes to measurable adverse psychological outcomes among individuals with historically marginalized identities (Comas-Díaz et al., 2019). Microaggressions, another type of invalidation, are also associated with adverse psychological outcomes among marginalized populations, including heightened stress, anxiety, depression, emotional exhaustion, suicidal ideation, and reduced quality of life (Choi et al., 2022; Kimber et al., 2026; Nadal et al., 2014; Sue et al., 2007). This is particularly relevant to the TRUST model when microaggressions occur in organizational settings, such as a workplaces, signaling to targets that their identities are viewed as threats and that they do not belong (Emerson & Murphy, 2014).
Beyond covert experiences of invalidation such as invisible labor and microaggressions, historically marginalized groups also continue to experience overt, macro-level forms of discrimination and systemic invalidation that additionally contribute to psychological distress among these populations. Blatant discrimination in the form of derogatory language, bullying, or blocked career advancement, for example, reinforce messages of inferiority, exclusion, and unworthiness, diminishing one’s inner authority and compounding the emotional toll of systemic invalidation on mental health (Di Marco et al., 2021). In one seminal study, researchers found that exclusion in their sample of 3,400 employees was linked to job dissatisfaction and lower emotional well-being among women and racial/ethnic minorities (Barak & Levin, 2002). Similarly, institutional betrayal—defined as instances in which an institution that an individual relies on creates conditions that increase the likelihood of trauma or fails to respond appropriately after trauma occurs—has been associated with diminished well-being, including PTSD symptoms and depression, among university students of color, further underscoring the impact of systemic invalidation among stigmatized groups (Tamaian et al., 2024).
In sum, repeated experiences of microaggressions, institutional betrayal, and exclusion communicate to individuals that their perspectives and identities are undervalued or suspect. Over time, this cumulative pattern may even function as a form of chronic racialized and systemic trauma, not merely isolated stressors. Racial trauma by definition, is the effect of individual and systemic racism over time, which can often look similar to the symptomatology of PTSD (Carter, 2007; Comas-Díaz et al., 2019; Williams et al., 2018). Meta-analytic reviews further confirm that these harmful effects occur broadly across stigmatized groups (Costa et al., 2023; Lui & Quezada, 2019; Williams, 2020). Such trauma undermines a sense of safety and belonging and erodes confidence in one’s own judgment, resulting in chronic self-doubt, hypervigilance, and rumination. Studies have shown that this ongoing exposure to invalidation is associated with trauma-related symptoms, including elevated stress hormone levels (e.g., cortisol), intrusive negative thoughts, and feelings of alienation. These symptoms are in turn associated with mood alterations, including vulnerability to internalizing symptoms such as anxiety, depressive episodes, and emotional exhaustion, as well as externalizing responses such as disengagement or withdrawal from academic and professional settings (Bellamy & Hardy, 2015; Erby & Blustein 2026; Sylvain et al., 2022; Williams & Zare, 2022). These findings further substantiate that invalidating systems are not simply inconvenient or frustrating; they operate as persistent, trauma-inducing psychosocial stressors that directly compromise mental health, identity development, and overall well-being.
Self-Efficacy and Self-Esteem vs. Self-Trust
When individuals repeatedly encounter situations that call into question their competence, intelligence, or leadership capacity, they may begin to unconsciously adopt these narratives as truth (James, 2022; Speight, 2007; Steele & Newton, 2022). This process is particularly insidious because it erodes self-trust, undermining one’s ability to advocate, make decisions, or challenge unjust conditions (Reck et al., 2024; Roberson & Pieterse, 2021). Self-efficacy has been well researched as it relates to racism and oppression (Ahn et al., 2022; Patel et al., 2008; Soland, 2019; Spanierman, 2002); however, it is helpful to distinguish self-trust from self-efficacy, as the two are related but not identical. Self-efficacy refers to a person’s belief in their ability to successfully perform specific tasks or achieve particular goals (Bandura, 1977). It focuses on doing—on skills, strategies, and confidence in one’s capacity to handle a situation. For example, someone with strong self-efficacy might think, “I can figure out how to give this presentation successfully,” or “I know I can learn this new software.” Self-efficacy is often shaped by practice, mastery experiences, external feedback, and observing others succeed (Sitzmann & Yeo, 2013). Self-trust, on the other hand, may be defined as a person’s confidence in their own perceptions, decisions, and inner wisdom (El Kassar, 2021; Jones, 2012). It focuses on being and knowing rather than on specific tasks. Self-trust might sound like, “I trust my sense that something feels off in this situation,” or “I trust my decision, even if others doubt it.” It is cultivated through self-reflection, self-awareness, and experiences of validation or invalidation.
Although different, self-efficacy and self-trust often reinforce each other. When a person has self-trust, they are more likely to attempt tasks that build self-efficacy. Likewise, when self-efficacy has been developed by mastering tasks, it can strengthen self-trust because there is tangible evidence that one’s decisions and efforts lead to success (Hsu et al., 2007). Together, they work hand in hand to support resilience, motivation, and a strong sense of self (Rahman et al., 2018).
In a similar fashion, self-trust and self-esteem are also related concepts but focus on very different aspects of the self. While self-trust refers to an inner belief that you can rely on your own perceptions, feelings, intuition, and judgment, especially when faced with external pressures or invalidation, self-esteem refers how positively or negatively one views oneself as a person (Rosenberg, 1979). Essentially, self-trust is an active, internal process of tuning into one’s own wisdom and honoring what one knows to be true of oneself, while self-esteem is more of a global evaluation. Self-esteem asks, “Do I believe I am a person of worth?” Self-trust, which is more moment-to-moment and contextual, asks, “Can I trust what I feel, think, or decide right now, even if others disagree?” Someone can have high self-esteem, feeling confident and worthy, while still having low self-trust, constantly second-guessing their own decisions because of external pressure or fear of making mistakes. Conversely, a person may have low self-esteem, struggling with feelings of inadequacy, but still possess a strong sense of self-trust, relying on their inner voice to guide their actions in challenging environments. For example, a Black professional may feel proud of their cultural identity and accomplishments, reflecting high self-esteem, yet still struggle with low self-trust when confronted with subtle racism at work. Even though they sense a colleague’s comment was racially charged, years of systemic invalidation may cause them to second-guess themselves, wondering if they are “being too sensitive.” Conversely, that same Black professional could experience low self-esteem due to ongoing exposure to racist stereotypes and workplace microaggressions, leaving them questioning their overall worth compared to White colleagues. Still, they may maintain high self-trust by believing firmly in their own perception of bias and confidently naming the racism when it occurs, even if others dismiss or minimize it.
Importantly, experiences of systemic invalidation often undermine self-trust even when self-esteem remains intact. A Latinx professional, for example, may possess a strong sense of self-esteem, grounded in pride in their cultural identity, accomplishments, and sense of personal worth. However, within predominantly White professional settings, repeated exposure to gaslighting and tone policing may gradually erode their self-trust. When a colleague responds to their concerns about inequitable treatment by saying, “I think you’re misinterpreting the situation,” or “You’re being too emotional about this,” the individual may begin to question their own perceptions, emotional responses, and judgment, despite still viewing themselves as capable and competent. In this context, self-esteem remains relatively stable, yet self-trust becomes compromised as external invalidation distorts one’s confidence in their internal reality.
Taken together, the literature reviewed thus far paints a compelling picture: systemic invalidation is a chronic, structural force with cumulative psychological and emotional consequences. These harms are not the result of personal failure or lack of resilience but stem from navigating environments where one’s full humanity is consistently denied or distorted. As such, they require interventions that go beyond traditional coping strategies to include self-trust, through avenues such as cultural reclamation, community connection, political consciousness, and structural critique (Adames et al., 2023; French et al., 2020; Jones, 2025; O’Keefe et al., 2021; Williams et al., 2019). Hence the need for the TRUST model, which is discussed below.
The TRUST Model
The TRUST model is grounded in the understanding that repeated exposure to systemic invalidation can result in cumulative harm that functions as trauma and other negative psychological outcomes (Osman et al., 2025). Situating the model within the broader literature described above underscores the need for integrative, culturally responsive approaches that move beyond symptom reduction to support agency, meaning-making, and personal growth. The TRUST model is therefore rooted in healing-centered engagement (HCE; Ginwright, 2018) and liberated cognitive behavior therapy (CBT-L; Sawyer, 2023), both of which emphasize the importance of affirming identity, fostering self-determination, and addressing the sociocultural conditions that impact psychological well-being. HCE is a strengths-based, culturally rooted, and politically grounded approach that, while trauma-informed, reframes healing as holistic well-being rather than mere trauma recovery. Accordingly, instead of focusing solely on pathology, HCE views healing as a process rooted in liberation, joy, and empowerment—an essential lens when working with individuals harmed by systemic oppression. Of particular relevance to the TRUST model, HCE more specifically provides fertile ground for the development of self-trust by shifting the question from “What’s wrong with you?” to “What is right with you?” through its primary principles: addressing systemic causes of distress, grounding healing in culture and identity, and emphasizing strengths and assets over deficits. The means through which these principles are implemented by clinicians include building empathy, encouraging hope, and building critical reflection that leads to social action (Freire, 1970; Ginwright, 2018).
Internalized oppression is when people from marginalized or stigmatized racial groups absorb and believe negative stereotypes, messages, or beliefs about themselves, leading them to doubt their worth, limit their potential, or unconsciously act in ways that reinforce their own disadvantage (Rosenwasser, 2002). HCE’s emphasis on shifting one’s perspective, building critical reflection, and taking empowered action reflects its cognitive focus on reauthoring internal narratives, challenging internalized oppression, and fostering a mindset rooted in agency—all key components of cognitive behavior therapy (Steele, 2024; Steele & Newton, 2022). As such, CBT also serves as a key theoretical component of the TRUST model, similar to other ethnopolitical approaches, for example, those grounded in womanist theory (Sanchez-Hucles, 2016), positive racial socialization (Steele et al., 2025), and mujerismo, a Chicana feminist framework that centers the lived experiences, cultural knowledge, spirituality and collective resilience of Latina women in the face of intersecting systems of oppression (Gloria & Castellanos, 2016). CBT posits that our thoughts shape our emotions and behaviors, and that by identifying and challenging distorted or unhelpful thoughts, individuals can improve psychological functioning. However, traditional CBT must be critically examined and expanded when working with clients navigating invalidating and marginalizing systems. Standard CBT frameworks can risk pathologizing thoughts that are actually accurate responses to oppressive realities. Therefore, CBT-L is applied in the current framework to move beyond individualistic conceptions of healing by addressing the sociopolitical roots of psychological distress and expanding the role of cognition to include critical consciousness (Sawyer, 2023).
According to Sawyer (2023), CBT-L, which draws from liberation psychology (Martín-Baró, 1994), is based on the premise that traditional CBT often assumes that systems are healthy. Traditional CBT, therefore, risks cultural gaslighting by encouraging clients to adapt to oppressive conditions. Cultural gaslighting refers to the systemic dismissal of marginalized people’s lived experiences, leading them to question the validity of their perceptions, emotions, and cultural knowledge (Sawyer, 2023). Within the TRUST model, this means that CBT is not intended to be used to reframe or minimize the traumatic realities of systemic oppression, but rather to offer culturally responsive tools that support meaning-making and healing. Instead of challenging the validity of invalidating experiences, the therapist works collaboratively with the client to explore how internalized messages from those experiences can be disentangled from their core sense of self and their perceived ability to enact change within these environments (Steele & Newton, 2022).
Importantly, it should be noted that HCE and CBT-L are both rooted in critical consciousness (Freire, 1970), which underlies their shared emphasis on sociopolitical awareness and transformation. Critical consciousness emphasizes sociopolitical awareness, reflection, and action to challenge inequitable systems and has been recognized within counseling psychology as an empowering process for individuals from historically marginalized communities. HCE and CBT-L extend this tradition by integrating critical awareness with psychological healing, attending not only to external structures of power but also to the internal processes shaped by chronic invalidation. Building on this foundation, the TRUST Model implicitly centers the intrapsychic and emotional mechanisms that sustain critical awareness over time, foregrounding self-trust as essential for believing one’s perceptions, emotions, and judgments when those realities are routinely questioned or dismissed. In this way, self-trust functions as a bridge between critical consciousness and sustained engagement, buffering against gaslighting and tone policing while supporting resilience and healing.
Domains and Associated Interventions Within the TRUST Model
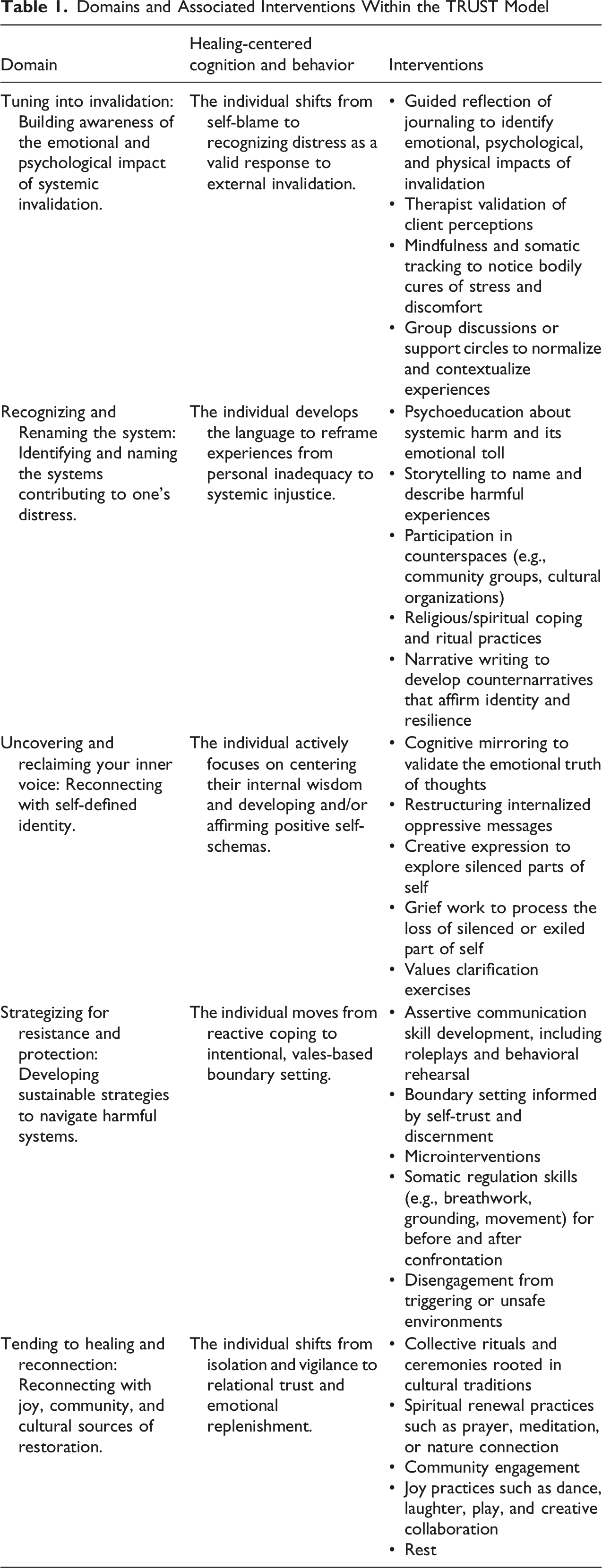
Tuning Into Invalidation
The first domain of the TRUST model, Tuning Into Invalidation, is a foundational domain in which individuals begin to consciously recognize the psychological, emotional, and sometimes physical toll of existing within systems that routinely distort, minimize, or erase their truth as a function of oppressive conditions. This domain often marks the moment where lived experience and internal awareness begin to align, breaking through long-held coping mechanisms like denial, over-functioning, or silence (Steele & Newton, 2022). A defining feature of this domain is the emergence of dissonance between one’s internal sense of identity and the way that identity is perceived, dismissed, or devalued by others. For example, a Black woman may feel confident in her knowledge and leadership skills, yet find herself constantly interrupted in meetings, passed over for promotions, or described as “aggressive” for expressing ideas with clarity. Over time, the discrepancy between how she sees herself and how she is treated becomes too glaring to ignore. This growing disconnect between lived truth and external messaging is often what sparks deeper reflection.
Within the TRUST model, this internal questioning, though painful, is used as an impetus for critical insight that can be promoted through reflection. This reflection, achieved through a variety of modalities, helps individuals begin to name their emotional experiences and connect them to broader patterns. For some, therapy becomes a space where they are validated and encouraged to explore the roots of their unease. For others, journaling provides an archive of emotional patterns that, over time, make the invisible visible. The overall goal through this reflection is to assist individuals with moving beyond self-blame and toward recognizing that something deeper, something structural, is contributing to their distress (Ginwright, 2018; Sawyer, 2023). This is essential, as invalidating systems often teach individuals to question their perceptions. Gaslighting, tone policing, and silencing can leave individuals unsure whether their experience “counts” as harm (Irigaray et al., 2023; Tobias & Joseph, 2020). Thus, coming into awareness is both liberating and destabilizing. It also represents the first movement toward self-trust: the brave and necessary act of saying, “Something here is not right, and it’s not just me.” It does not require the individual to have answers, solutions, or strategies. It only asks that they pay attention to the signals from their mind, body, and spirit. It is the opening portal of the TRUST model, the space where consciousness is awakened, and where the journey toward reclamation begins.
Finally, given that it is the first domain within the TRUST model, it is important to note that in some cases, tuning in emerges abruptly after a critical incident such as a blatant act of racial discrimination, a triggering conversation, or a professional betrayal that lays bare the reality of the system’s limitations. In other cases, it arises quietly through the steady realization that joy has been replaced by dread, or that one’s voice has been shrinking in order to survive. Accordingly, awareness of invalidation does not always appear suddenly; rather, it may unfold gradually over time through the accumulation of unresolved discomfort, ambiguous tension, or repeated moments of emotional injury. Tuning into invalidation involves noticing harm and beginning to sense its systemic origins, a process that can be emotionally painful because it disrupts coping strategies rooted in minimization or avoidance. Movement beyond this domain depends on relational safety, validation, and support; when these conditions are absent, continued disengagement is understood as an adaptive and self-protective response rather than a lack of readiness. In clinical settings, individuals may report persistent symptoms such as chronic anxiety, insomnia, intrusive self-doubt, exhaustion, irritability, or a growing sense of alienation from one’s workplace, educational institution, or social environment. These symptoms are frequently misdiagnosed or misunderstood as signs of burnout, depression, or imposter syndrome, when in fact they are deeply linked to systemic harm and environmental invalidation (Bressi, 2024; Dancy & Jean-Marie, 2014; McGee et al., 2022; Quint et al., 2025). Therefore, it is critical that therapists support clients in recognizing these patterns not as individual pathology, but as valid responses to systemic invalidation; hence, the next domain of the TRUST model.
Recognizing and Renaming the System
The second domain of the TRUST model is Recognizing and Renaming the System. This domain is pivotal in shifting the emotional burden of harm away from the individual and toward the systems and structures that perpetuate it (Jones, 2012). In this domain, individuals begin to recognize that the distress they feel, while deeply personal in its impact, is not personal in its origin. Rather, it is the predictable outcome of navigating environments shaped by historical and ongoing systems of oppression such as racism, sexism, heteronormativity, ableism, and classism. Through this lens, what may have previously felt like isolated incidents (e.g., being interrupted in meetings, receiving vague or biased feedback, being described as “too much” or “not a good fit”), are recontextualized as systemic patterns of exclusion and control (Cross, 1971). The harm is no longer located within the self but in the social, cultural, and institutional norms that shape one’s environment.
Consistent with HCE, a powerful transformation begins to occur in this domain. The internal question shifts from “What did I do wrong?” to “What is this system doing that repeatedly undermines my sense of self and safety?” This reframing is critical because as suggested by CBT-L, invalidating systems often operate through gaslighting, where individuals are subtly or overtly led to believe their experiences are exaggerated, imagined, or irrational. Naming the system interrupts that distortion and reclaims narrative power. Importantly, this process of naming is not solely intellectual—it is emotional, political, and embodied. Naming the system interrupts distortion and reclaims narrative power because it affirms lived truth in ways that engage not only the mind but also the heart, identity, and body, transforming resistance into an art of healing and empowerment. At this level, individuals may report feeling a profound sense of relief, grief, or anger when they finally recognize that the problem is not a personal deficit but a pattern of injustice. Others experience a kind of awakening, what liberation theorist Freire (1970) might describe as critical consciousness, which allows them to see with new clarity the ideological forces that have shaped their environment and internal world. The psychoeducation that occurs at this domain often involves developing a new vocabulary to describe one’s experiences. Individuals may begin learning terms such as “microaggressions,” “racial battle fatigue,” or “institutional betrayal” (Steele, 2024). With this language comes power—the power to tell the truth, to articulate harm, and to resist internalizing systemic messages.
Interventions at this domain beyond psychoeducation primarily focus on activities that support the development of counternarratives; that is, stories that resist dominant explanations and affirm lived experience. For example, culturally affirming practices such as storytelling (Chioneso et al., 2020), spending time in counterspaces (Chapman-Hilliard & Beasley, 2018Chapman‐Hilliard & Beasley, 2018), and religious coping (Turner et al., 2022) provide opportunities for individuals to make meaning of their experiences, reclaim their truth, reinforce a coherent sense of identity in the face of systemic invalidation, and plant seeds to reestablish self-trust. Other therapeutic strategies drawn from culturally adapted cognitive therapy for PTSD (Steele, 2024) such as narrative writing (Ehlers & Wild, 2020) can also be used to help individuals process difficult experiences, identify negative self-appraisals shaped by systemic harm, and author new interpretations that honor their pain and build self-trust. Essentially, at this domain, individuals begin focusing on telling their story differently, not as a tale of overreaction or inadequacy, but as evidence of resilience and clarity in the face of injustice.
Uncovering and Reclaiming Your Inner Voice
The third domain of the TRUST model, Uncovering and Reclaiming Your Inner Voice, is a transformative domain where individuals engage in the intentional work of realigning with their core values. Having named the systems that distort, diminish, or deny their truth, individuals now begin the process of healing the internalized narratives those systems have left behind. This domain marks a critical pivot: a focus turns inward, with clarity that the self has been shaped by external forces that must now be deconstructed and rebuilt with intention. At the heart of uncovering and reclaiming one’s inner voice is the affirmation of self-defined identity (Jones, 2012). Individuals begin to ask, sometimes for the first time, “Who am I when I’m not trying to fit into a system that invalidates me?” This may involve rediscovering parts of themselves that had been silenced, repressed, or culturally erased in the effort to survive professionally or socially. They may begin exploring the aspects of identity that feel most authentic, whether racial, cultural, spiritual, gendered, or artistic, and giving those parts more space, voice, and visibility.
The Uncovering and Reclaiming Your Inner Voice domain is where CBT-L and cultural practices most explicitly converge during therapy. From a CBT perspective, individuals at this domain engage in thought work; that is, challenging the internalized messages and distorted beliefs that have resulted from long-term exposure to oppressive systems. Contrary to traditional CBT, however, in CBT-L this process if not about disputing thoughts for their accuracy or logic alone, but engaging in cognitive mirroring, a practice that centers the client’s internal wisdom (Sawyer, 2023). For example, a queer individual in a conservative environment may internalize the thought, “Maybe I am too sensitive, and this really isn’t a big deal,” after repeatedly hearing homophobic remarks dismissed as jokes. With cognitive mirroring, the therapist recognizes this thought as a survival response rooted in an invalidating environment and a signal of eroded self-trust. Therefore, instead of attempting to correct the belief, the therapist reflects the emotional truth behind the thought, naming the discomfort as valid and affirming their perception (Ginwright, 2018). In the current example, a cognitive mirroring response might sound as follows: “It makes sense that part of you is wondering if you’re overreacting, especially when the people around you treat these comments like they are harmless. But I also hear another part of you that feels hurt and unseen. That pain is real, and it’s telling us something important about your environment.”
As individuals begin to reclaim their inner voice, they can further support self-trust by continuing to emphasize cultural reconnection as a vital source of restoration. Individuals may turn to ancestral wisdom, spiritual practices, rituals, music, storytelling, art, or community traditions as a way to remember who they are outside of systems of domination (Steele & Newton, 2022). This reconnection often reintroduces a sense of rootedness and continuity, reminding individuals that they are not starting from scratch but returning to a self that has always existed beneath the surface. It is important to note, however, that the process of inner reclamation is both liberating and emotionally complex. Individuals may report a mix of grief, pride, fear, and relief. Grief may emerge for the years lost to self-doubt, the silence once maintained to stay safe, or the parts of the self that were exiled to survive (Nicholls & Elliot, 2019). Nevertheless, that grief is often accompanied by pride for having endured, for choosing self-recovery, and for finally being able to say, “This is who I am.” This shift often creates a powerful emotional breakthrough, what some describe as a “homecoming to self” (Bryant-Davis, 2022).
Strategizing for Resistance and Protection
The fourth domain of the TRUST model is Strategizing for Resistance and Protection. This is an action-oriented domain where individuals begin to implement tangible, intentional practices to guard their mental, emotional, spiritual, and even physical well-being in systems that continue to be harmful or unreformed. Having developed insights and new self-schemas in the earlier domains, individuals are now equipped to engage with the world more deliberately, discerning when to resist, when to disengage, and how to preserve their inner sense of self and worth. Crucially, this domain does not advocate disengagement as retreat or surrender. Instead, it frames resistance and protection as acts of strategic wisdom, a knowing cultivated by those who understand that self-preservation is not selfish, but necessary for long-term survival, clarity, and thriving. For instance, research conducted by Roberson and Carter (2022) suggest that for people of color, symptoms such as avoidance or increased arousal may be an adaptive coping strategy used to navigate racially charged situations and increase safety. Unfortunately, while adaptive, this strategy reflects Hochschild’s (1983) notion of emotional labor of monitoring, filtering, and reshaping one’s expression to survive in invalidating spaces. It is moreover constant for individuals navigating oppressive systems. Accordingly, without boundaries and tools for sustainability, even the most self-aware individuals can experience burnout, retraumatization, or resignation.
Given these risks, this domain emphasizes using self-trust to guide decisions about when and how to advocate for oneself within invalidating systems. The goal of the individual at this domain, therefore, focuses on refining the skill of discernment; that is, choosing when to speak and when to be silent, when to show up fully and when to conserve energy, when to call out harm and when to redirect energy elsewhere. These choices are not made from fear or avoidance, but from an internalized clarity about one’s own limits, values, and priorities. Central to this task is recognizing bodily cues such as tension, fatigue, or unease as early warning signs that boundaries may be needed. To support this process, Gutiérrez (2022) suggests regularly practicing embodied awareness through breathwork, movement, or mindfulness. This not only sharpens internal attunement but also prepares individuals to act on these signals with greater confidence and self-trust.
When boundaries are needed, they can be enacted through practices such as assertive communication, disengagement from triggering environments, or the use of microinterventions, which are defined as brief, intentional responses that affirm one’s truth without requiring full emotional disclosure or debate (Sue et al., 2019). For example, drawing from CBT-L, assertive communication may include identifying beliefs that make boundary setting difficult, developing statements that state needs, limits, or harms without hostility, and practicing protective responses with a therapist or other trusted social support (Steele et al., 2025). From an HCE perspective, this may also include engaging in techniques to regulate oneself before or after confrontation. Similarly, disengaging from triggering environments may also assist with resistance and protection by providing a restorative break, while microinterventions provide concrete strategies such as calling attention to bias, clarifying intent, or offering information to challenge assumptions, which can help individuals assert their inner voice in the face of system invalidation (Sue et al., 2019).
Tending to Healing and Reconnection
Finally, the fifth and culminating domain of the TRUST Model is Tending to Healing and Reconnection, a relational domain that centers the emotional, spiritual, and communal repair necessary to sustain self-trust over time. In this domain, individuals ground themselves in healing practices that replenish the parts of them that systems have attempted to deplete—their joy, intuition, purpose, and sense of belonging (Sobande & Amponsah, 2025). Although the earlier domains of the TRUST model focus on awareness, resistance, and reclamation, Tending to Healing and Restoration is where integration and renewal firmly take root. This domain is based on the understanding that healing cannot, and should not, be done in isolation (Ginwright, 2018). Oppression is a collective wound; therefore, restoration must also be collective and culturally rooted (Chavez-Dueñas et al., 2019). Individuals do not simply bounce back from trauma by thinking differently or setting boundaries; they heal by being held, witnessed, and nourished emotionally, spiritually, and relationally. Restoration is not the same as “returning to normal” or seeking comfort in systems of oppression. Rather, it is about cultivating spaces and practices where one’s wholeness is affirmed without compromise. This can include everything from collective rituals and ancestral practices to laughter-filled conversations, creative expression, spiritual renewal, and physical movement (Gutiérrez, 2022). These practices are not secondary to the healing process, they are the healing process. They provide a counterweight to systems that thrive on urgency, extraction, and detachment.
In this domain, self-trust becomes relational. The inner voice that was once silenced or uncertain is now echoed and reflected back through community, through sacred practices, and through relationships that affirm, “You are not alone. You are not wrong. You are worthy” (Ginwright, 2018). As such, this domain draws heavily from the work of Black, Indigenous, and queer activists and healers who understood that systems of oppression not only harm the mind but fracture the spirit. This is also where the Ubuntu philosophy (“I am because we are”) is deeply resonant (Turner et al., 2022). Restoration and reconnection are not about finding comfort in systems that dehumanize but about remembering and re-rooting in our interdependence. For people who have been forced to individualize their survival in toxic systems, this domain can be both profoundly healing and countercultural. It invites individuals to rest not just in solitude, but in solidarity. Emotionally, this domain may evoke feelings of gratitude, release, relief, and even surprise. Some individuals may initially struggle to trust joy or rest, especially if they have lived in a state of vigilance for extended periods. Learning to feel safe in joy, connection, and softness becomes its own journey. This process often includes unlearning the belief that care must be earned or that rest must be justified.
Implications
The TRUST Model offers a liberatory framework for promoting psychological wellness among historically marginalized communities. Grounded in healing-centered engagement (Ginwright, 2018) and liberated cognitive behavior theory (Sawyer, 2023), it affirms identity, restores agency, and disrupts internalized systemic harm. In clinical practice, it expands therapy beyond symptom reduction to include empowerment and contextual awareness, reframing clients as survivors of invalidating systems. In education, it fosters reflective, culturally responsive environments—especially in graduate programs where systemic insight and personal growth intersect. Within organizations, it guides trauma-informed, equity-centered policies and supervision, helping leaders identify embedded harm and promote psychological safety and inclusion.
Conclusion
Although conceptually compelling, the TRUST Model requires empirical validation. Future research should assess its effectiveness across clinical, educational, and organizational contexts, focusing on outcomes such as psychological safety, identity development, and systemic resilience. Mixed-method and longitudinal studies could illuminate its transformative potential and guide its refinement. Empirical evaluation of the TRUST Model would likely proceed in phases, beginning with the development and pilot testing of TRUST-informed practices that operationalize the model’s domains into direct interventions. Subsequent studies could examine whether these practices are associated with changes in self-trust, boundary setting, and reduced internalized oppression across clinical and organizational contexts.
Nevertheless, the TRUST Model reorients practice around collective healing and structural resilience. It encourages practitioners, educators, and leaders to validate lived experiences and co-create pathways for emotional regulation, boundary setting, and self-trust. Trusting oneself in an invalidating system becomes an act of resistance, a reclaiming of identity and a return to wholeness. Through cycles of awareness, resistance, and restoration, individuals and communities affirm their worth, voice, and capacity for joy and liberation. This approach is especially critical for BIPOC, LGBTQ+, and neurodivergent individuals whose experiences have often been minimized or pathologized in dominant paradigms.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declare that they have no conflicts of interest.
Data Availability Statement
There is no data set associated with this manuscript.