
Abstract
This study assesses the likelihood of rearrest among a cohort of all adults (N = 1,438) released from the Massachusetts state prison system who received mental health services while they were incarcerated. All individuals were followed for 24 months. The analysis focused on four classes of variables: demographic characteristics, clinical history, criminal justice history, and postrelease supervision. These analyses showed that criminal history factors—a juvenile record and a history of multiple previous incarcerations—were significant risk factors, but that clinical factors, including a history of substance abuse, were not. Overall, the models developed here look much like the ones that would be observed in the general offender population. The implications of these findings for criminal justice and mental health policy are discussed.
Introduction
Concerns regarding persons with mental illness detained in correctional settings have been part of public policy discourse since Dorothea Dix’s observations of such individuals in the East Cambridge Jail in 1841 (Grob, 1973; Rothman, 1971). However, despite the proliferation of diversion programs, reentry programs, mental health courts, and other interventions targeting offenders with mental illness, as well as enhanced community mental health programs that provide services to the general population of persons with psychiatric illnesses, many of the same problems exist today that were identified by Ms. Dix more than 170 years ago. Some 20 years ago it was noted that the Los Angeles County jail system had become the largest institutionally based provider of mental health treatment, surpassing all psychiatric inpatient settings (Torrey, 1995; Torrey et al., 1992). Recent data from the Bureau of Justice Statistics (BJS; James & Glaze, 2006) indicate that an estimated 56.2% of state prison inmates met criteria for a “mental health problem,” defined as “receiving a clinical diagnosis or treatment by a mental health professional” at the time of the survey or in the previous 12 months. These rates appear to be substantially higher for female than for male inmates (73% compared with 55%). The diagnostic mix data indicate that many inmates met criteria for severe mental illnesses; 21% reported at least one symptom of mania, 26% at least one or two symptoms of major depression, and roughly 11% had at least one psychotic symptom. Sixty-three percent of state prison inmates with mental health problems had co-occurring drug use in the months prior to their arrest, a factor known both to exacerbate the symptoms of mental illnesses (Drake & Wallach, 1989) and increase the likelihood of arrest (Hartwell, 2004a, 2004b; Swartz & Lurigio, 2007). Translated into hard numbers, these figures suggest that roughly 705,600 state prison inmates had either a history of mental illness, were symptomatic at the time of the assessment, or both (James & Glaze, 2006).
A variety of factors contribute to excess correctional system involvement among persons with mental illness. Among them is their high arrest rate. Data from the Massachusetts Mental Health–Criminal Justice Cohort Study found that nearly 30% of individuals receiving services from the state’s public mental health system were arrested at least once over a 10-year period (Fisher, Roy-Bujnowski, Grudzinskas, et al., 2006). Similar results were obtained in a study of New York Medicaid recipients with psychiatric diagnoses (Cuellar, Snowden, & Ewing, 2007). The Massachusetts study also found that in virtually every offense category, the cohort members had significantly higher odds of arrest than demographically comparable Massachusetts residents (Fisher et al., 2011). As police researchers such as Bittner (1970) and proponents of the “criminalization perspective” (e.g., Abramson, 1972; Torrey et al., 1992) would predict, many of these arrests were for minor offenses, such as disturbing the peace, trespassing, minor shoplifting, and the like. Others, though, were serious felonies, involving property crimes, crimes against persons, and drug offenses involving more than simple possession that, if convictions were obtained on those charges, would carry significant state prison sentences (Fisher, Roy-Bujnowski et al., 2006; Fisher, Roy-Bujnoswski, Grudzinskas et al., 2007).
Criminal Recidivism Among Persons With Mental Illness
Many of the persons included in the Massachusetts cohort study were arrested multiple times during the observation period, including one individual who experienced 71 arraignments during the nearly 10-year observation period, suggesting that reentry and community reintegration are processes for which achieving success may in some cases prove difficult. Reentry and recidivism have been well studied, and a host of factors have been identified that appear to contribute to failure, notably serious mental disorders (Baillargeon, Binswanger, Penn, Williams, & Murray, 2009. As Travis (2005) described in the Urban Institute Report and book by the same name, But They All Come Back, the challenges faced by individuals exiting the correctional system are universally daunting, but are compounded for persons who have psychiatric and substance abuse problems.
Many reentering inmates feel ill-prepared for life outside prison. In interviews with soon-to-be-released inmates in the New Jersey Department of Corrections, Wolff, Maschi, and Bjerklie (2004) found that one in four male and one in five female interviewees reported their readiness for resuming life in the community as “poor” or “fair,” and half did not know whether they would be able to support themselves once they were released. Reintegration for persons with psychiatric illnesses may also prove difficult because of less than optimal psychiatric treatment provided in some prison settings. A 2003 Human Rights Watch report on correctional mental health care titled Ill Equipped: Mental Illness and US Prisons outlines numerous deficiencies in the way psychiatric treatment is provided in these settings. Leaving prison with a poorly treated psychiatric condition and, perhaps, minimal follow-up, is likely to compromise individuals’ likelihood of succeeding as they transition into their communities.
A number of factors work specifically against persons affected by mental health problems as they exit prison. Such individuals carry the double stigma of a mental illness and a criminal history. Many are forced to live in drug infested, high crime neighborhoods where available social capital may be limited to persons who engage in substance abuse and other criminal and antisocial behaviors (Alverson, Alverson, & Drake, 2001; Drake & Wallach, 1989; Drake, Wallach, & McGovern, 2005). Involvement with such groups may increase the likelihood that a releasee will violate the terms of parole or be rearrested (Hartwell, 2004a). In addition to finding housing and employment—tasks that can be difficult for many former inmates, persons who have mental illness must also connect with mental health and substance abuse services and, for those eligible, also establish or reestablish essential entitlements, particularly Medicaid, which for many will be the source of payment for psychiatric services (Morrissey, Cuddeback, & Meyer, 2007). The social histories of state prison inmates with mental health problems further complicate the reentry process. The BJS data cited earlier indicate that roughly 13% of mentally ill inmates had been homeless at some point prior to their arrest (James & Glaze, 2006).
The failure to prepare inmates for the transition from corrections into the community would seem to be an obvious recipe for high rates of recidivism, and this problem has been recognized by the federal government and addressed in the form of The Second Chance Act of 2008 that provided federal support for local reentry initiatives. Other legislation, including the Mentally Ill Offender Treatment and Crime Reduction Act of 2004, has targeted funding to local mental health and criminal justice system collaborations in support of the development of efforts to prevent arrest and rearrest of persons with mental illnesses. Some reentry approaches entail identifying inmates with mental illness who are slated for release and beginning transitional planning at that point, with the goal of having the essential elements needed for successful community reintegration, including housing, treatment and support services, and access to medication and entitlements, in place on release. The Massachusetts Department of Mental Health’s Forensic Transition Team operates on this principle (Hartwell & Orr, 1999). Another model, the Critical Time Intervention model, which is based on an intervention that worked successfully with persons who were homeless, identifies a time period during which maximum input of services is needed and then works intensively with released inmates during that period (Draine & Herman, 2007).
County Jails Versus State Prisons
As the preceding discussion suggests, a significant amount of attention has been paid to correctional inmates with mental illnesses. However, reentry transition as a focus of research should be different for persons exiting state prisons, as opposed to county jails. County jails house inmates who typically have committed minor infractions resulting in sentences served in jail rather than prison. For persons affected by psychiatric illnesses, exiting state prisons is arguably made more difficult by the fact that, unlike county jails, which are local and serve a geographic area that may also be served by an integrated mental health authority, state prison systems are often organized around levels of security. As a result, prison inmates may serve sentences in facilities some distance from their home communities and from the mental health providers from which they may previously have received services.
Moreover, the duration of state prison sentences, measured in years rather than in months, may make reestablishment of linkages with previously used mental health services extremely difficult. This problem is exacerbated by the fact that some inmates with mental illness may experience even longer than expected sentences. Difficulty following prison routines can increase the likelihood that persons in this population will experience lengthy spells in disciplinary housing, including solitary confinement, and they can be released directly to the street when completing their sentences. In doing so, they may be deprived of the benefits of transition through lower security housing and the enhanced discharge planning and preparation provided there (Human Rights Watch, 2003).
Several person-level factors may also contribute to the likelihood of rearrest in this population. As a focus of criminological research, we frame this question in terms of correlates of risk, suggesting what Everett Hughes (1945) long ago labeled a “master status”—a “complex of auxiliary characteristics” that here emphasizes either (a) the clinical status of persons affected by mental illness, evidence of which would be severity of diagnosis; or (b) standard criminal history factors, such as whether a person had a juvenile record, number of previous incarcerations, and type of charge; or (c) as an alternative, a status that is defined by a combination of both types of risk factors. As a public policy issue, the question of how “mental health factors” compare with “criminal justice factors,” is an important one for the mental health and criminal justice agencies that must work with members of this population and have an awareness of what factors, if any, reduce or exacerbate the risk of rearrest. This article addresses these issues using the experience of a cohort of individuals who had been “open mental health cases (OMHC)” while incarcerated in the state prison facilities maintained by the Massachusetts Department of Corrections (MDOC).
Method
Data and Sample
Data
This study was based entirely on administrative data, supported by a grant from the National Institute of Mental Health aimed at encouraging the use of such data. The portion of the study presented here uses data from the MDOC and, through MDOC, from the Massachusetts Criminal Offender Record Information service.
Sample
The sample used in this study consisted of all individuals released from MDOC facilities from 2007 through 2009 (N = 1,438) who, while incarcerated, were given a diagnosis of a psychiatric disorder and were receiving treatment, in some cases psychotropic medications, for that disorder. Each individual in this cohort was followed for up to 24 months.
Human Subjects Review
This study was reviewed and approved by the institutional review boards of the University of Massachusetts Lowell, the University of Massachusetts Boston, the University of Massachusetts Medical School, the MDOC, the Massachusetts Department of Mental Health, and the Massachusetts Department of Public Health.
Variables
Dependent variables
The intent of this study is to examine factors that may predict rearrest and time until its occurrence. Our first dependent variable is “rearrest within 24 months of release” from a MDOC facility. This variable is treated as a dichotomy (0 = not rearrested, 1 = rearrested within the observation period). The second dependent variable examines time to arrest. The manner in which we were able to construct this variable presented challenges. To address this question in a standard event history framework, we would ideally use an outcome variable such as “days to reincarceration.” But, because the data with which we are working include psychiatric diagnoses, the entire data set, including the criminal justice variables, becomes “protected health information (PHI)” once merged with diagnosis. The data also constitute PHI because the sample consists of a medically defined population. In such data, precise dates of events (e.g., month, day, and year of release of rearrest) are considered to be identifying information (Hartwell et al., 2012). We were therefore only allowed to keep month and year in the final data set. “Time to arrest” is therefore measured in months, with a range of 1 to 24.
Independent Variables and Hypothesized Effects
We identify four groups of variables that we hypothesize should be either risk or protective factors with respect to reincarceration.
Demographic variables include gender, age, race, and education, which we have operationalized as “having less than a high school education.” Consistent with the general criminological and sociological perspectives, we assume that males, persons of color (African, African American, or Hispanic), persons with less than a high school education, and younger individuals will be at higher risk of rearrest.
Clinical factors include psychiatric diagnosis and a history of substance abuse. We compare the two arguably most severe diagnoses, “mood disorders,” which include depression, bipolar disorder, and mania, and “thought disorders,” which include psychotic illnesses such as schizophrenia spectrum disorders with other diagnostic categories. We do so because these disorders are deemed so debilitating and treatment intensive that they are in fact ranked by the World Health Organization (WHO; 2004) among the top 10 medical conditions in their listing of global burden of disability. We should note that, although all thought disorders are generally considered to be “major mental illnesses” because of their impact on functioning and contribution to disability, not all mood disorders present in our sample, for example, dysthymia, would fit that definition. However, the overall number of cases with specific mood disorders was small, and it was therefore necessary to group them into one category.
We should also note that information on disorders used in this analysis were those present in the archival data made available to us by MDOC. These diagnoses were made by clinicians working in that system and based on inmates’ symptom presentation at the time of their assessment. No information was available as to whether individual inmates’ diagnoses might have changed over time; what role other factors such as substance abuse might have played in their symptomatology; whether specific diagnostic protocols were followed, and if so, how stringently; or any aspect of the assessment process itself. Given that diagnostic protocols are unknown, persons seeking to use our findings regarding the effects of specific diagnoses and recidivism should proceed with caution. With that caveat issued, we continue to use the term here for the sake of convenience.
An additional clinical factor, history of substance abuse, is included because of its well-established relationship with criminal involvement and because substance abuse can complicate the management of psychiatric illnesses (Hartwell, 2004a, 2004b). In fact, it is so potent a risk factor for justice involvement among persons affected by mental illnesses that for some combination of offense types, substance abuse completely mediates the relationship between mental illness and arrest (J. Swartz & Lurigio, 2007).
In the model we develop, we compare the two “major mental illnesses”—thought and mood disorders, with all others, because of their severity and difficulty in management—factors that could lead to decompensation, involvement in deviant and disruptive behavior, and possible rearrest and reincarceration. We hypothesize that persons with these disorders will be more likely to be rearrested and, perhaps, rearrested more promptly following release. In addition, for reasons described above, we regard a history of substance abuse as a potential risk factor for rearrest and reincarceration.
Criminal history
It is widely assumed that individuals’ previous criminal involvement may predict future offending (Moffitt, 1993; Nagin & Land, 1993). In this study, we include having a juvenile record and number of prior incarcerations as risk factors for rearrest and hypothesize that these will be positively related to the likelihood of rearrest and its promptness. We also include variables capturing the governing offense for the last conviction. Although there was a substantial number of offense categories represented in this sample, the numbers of individuals convicted on some offenses, such as arson and sex offenses, were small. We thus used four categories—property crime, crimes against persons (which included sexual assault, murder, and other violent offenses, all of which were present in small numbers but which together created a suitably large category), and drug-related crimes. An “other” category was also constructed that included a number of offenses, many of them “crimes against public order” and a handful of others that were not classifiable in the other three categories. Our overall hypothesis is that persons sentenced for more serious offenses, such as crimes against persons, will be more likely to be rearrested than those convicted on lesser charges including public order offenses.
Postrelease supervision
In this cohort many individuals were released under terms of probation or parole. We consider both to be protective factors, compared with having no supervised status post release. In addition to the potential of supervision to reduce criminal reinvolvement, some individuals may have compliance with mental health treatment or at least avoidance of substance abuse as terms of their release, which we believe will reduce their risk of rearrest.
Statistical Analysis
Basic frequency distributions for the dependent and independent variables were estimated, and binary logistic regression was used to examine the effects of the above variables on the dichotomous variable “rearrest within 24 months.” In addition, we examined time to first rearrest, measured in months, as we described earlier. This was done by first examining this right-censored outcome using unadjusted survival and hazard functions, and then in a multivariable framework using a Cox proportional hazard model (Singer & Willett, 2003), incorporating the predictors described above and used in the logistic regression model. All analyses were carried out using SPSS Version 19.
Results
Frequencies on the above variables are presented in Table 1. As indicated, the number of cases on which analyses are based (n = 1,012) is smaller than the total in the MDOC sample due to listwise deletion of cases used in our various analytic techniques. A comparison of the final analytic sample with the total sample, using the covariate means that form the basis of our various analyses and those of the total sample, showed no particular bias in any direction, suggesting that the reduced sample size reflects a “missing at random” process and therefore an analytic sample that is essentially a representative subset of the total sample.
Characteristics of Persons Released From Massachusetts Department of Corrections Facilities in 2009 Who Received Mental Health Treatment While Incarcerated and the Subset Who Were Rearrested (n = 1,012 a ).
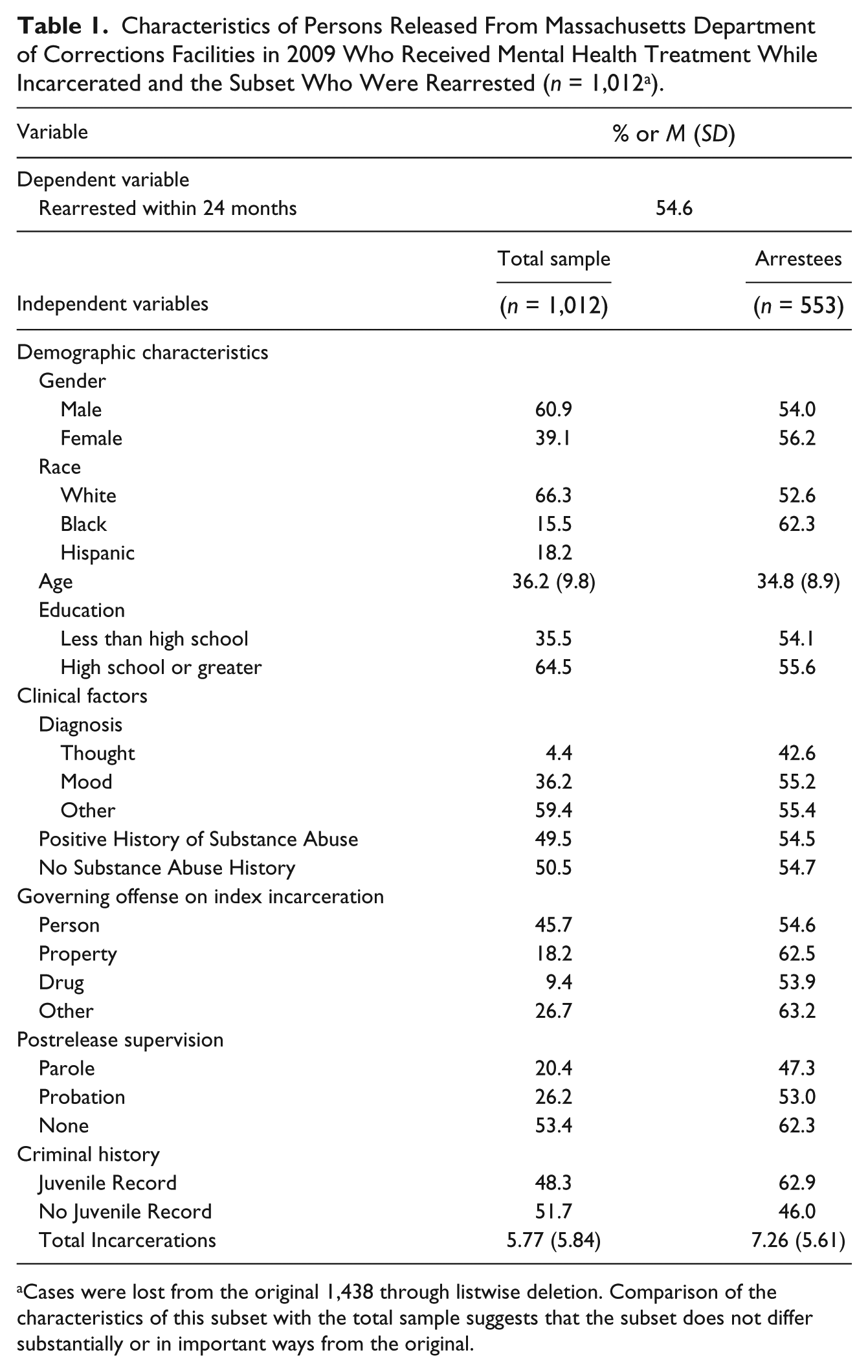
Cases were lost from the original 1,438 through listwise deletion. Comparison of the characteristics of this subset with the total sample suggests that the subset does not differ substantially or in important ways from the original.
As the frequency distributions in Table 1 indicate, this group featured significant variation with respect to both clinical and criminal history factors. The combination of thought and mood disorders indicates that roughly 40% of the cohort carried diagnoses of what were described earlier as “major mental illnesses.” Moreover, a substantial portion of the cohort had significant criminal justice histories; nearly one half of this cohort had a juvenile record, and others had significant numbers of incarcerations prior to the one from which they were reentering.
Comparison With the General MDOC Population
Before considering the findings of our analyses, it would be useful to examine briefly how the characteristics of OMHCs summarized in Table 1 differ from the general inmate population. We can assess some of these differences using data from MDOC (2012). A brief overview of these trends shows that the persons who were OMHCs are indeed a different population. First, the male/female differential is greatly diminished among OMHCs, among whom the gender differential is roughly 60/40 compared with 94/6 among the general population. This is consistent with national data from the BJS (James & Glaze, 2003) that highlight the far greater prevalence of mental health issues among females. Mental health recipients also differ with respect to race/ethnicity, with a substantially greater representation of Whites. They also differed with respect to governing offenses. A greater proportion of OMHCs were convicted on drug charges (26.7% compared with 14%) and property crimes (18.2% compared with 7%), but a smaller proportion were convicted on charges of “crimes against persons” (45.7% compared with 62%). Mean age for both groups was nearly equal at roughly 34. In assessing these similarities and differences, it should be noted that they compare a release cohort with the MDOC sentenced population and do so for slightly different time periods (2009 vs. 2011). (The latter is probably unimportant, but the former, because it includes individuals in the incarcerated population serving very long sentences for serious violent crimes, may skew the general population offense distribution toward greater representation of persons convicted of crimes against persons.) Overall, these data paint a picture of a subpopulation defined by their status as OMHCs that differs in important ways from the larger offender population, but whose rearrest potential is nonetheless governed by criminal justice, rather than by mental health attributes
Dependent variables
As indicated, 46.6% of the releases remained arrest free at the end of the observation period. (We should note that our data only capture events occurring in Massachusetts. Records of arrests in other states were not available for this study.) The Kaplan–Meier survival function developed as a preliminary step in this analysis indicated that the median time to rearrest was approximately 19 months. Moreover, the unadjusted hazard function, which describes the probability of rearrest in a given time interval following release for persons remaining at risk at the beginning of that interval, and which thus links the likelihood of rearrest with time at risk, indicates little, if any, trend, suggesting that increasing time at risk neither substantially increases nor decreases an individual’s chance of rearrest.
Multivariate model of arrest within 24 months
The variables described above were entered simultaneously in a binomial logistic regression model with “rearrest within 24 months of release” as the dichotomous dependent variable. As shown in Table 2, demographic variables, age and male gender were both associated with risk of rearrest. Male gender was a significant positive predictor of rearrest, but age was a negative predictor. Diagnostic factors were not associated with risk of rearrest. Persons whom we deemed to have the most significant and arguably most disabling conditions, those with mood and thought disorders, were neither more nor less likely to be rearrested. Criminal history factors were significant, however. Persons with juvenile records were roughly at 36% greater odds of rearrest than those without such histories during their 24-month observation period. Similarly, the number of total convictions (entered here as a logged variable due to its positively skewed distribution) was significantly and positively associated with rearrest. The variables measuring governing offenses on which individuals were convicted, which compared drug, person, and property crimes with a category of “other crimes,” were not significant predictors of rearrest. Parole was a significant negative predictor of rearrest; parolees were only about two thirds as likely to be rearrested as nonparolees. Probation appeared to have little effect in this regard.
Logistic Regression Model for Any Rearrest During 24-Month Observation Period.

Note. CI = confidence interval.
95% CI does not include one and is therefore assumed to be significant at the .05 level.
Modeling time to arrest
Results of the Cox proportional hazards model used to assess the effects of the set of variables that had been incorporated into the logistic regression “rearrest model” on time to rearrest are shown in Table 3. These data suggest that the factors associated with time to rearrest are slightly different from those associated with whether an individual is rearrested during the observation period. Here, age and being on parole appeared to delay rearrest, but the number of total incarcerations appeared to hasten it. These are consistent with the findings of the logistic regression. However, juvenile history, a moderate predictor of rearrest in the logistic regression, was not significant here, suggesting that this factor predicts recidivism but not its timing relative to release.
Cox Proportional Hazard Model of Rearrest During the 24-Month Observation Period.
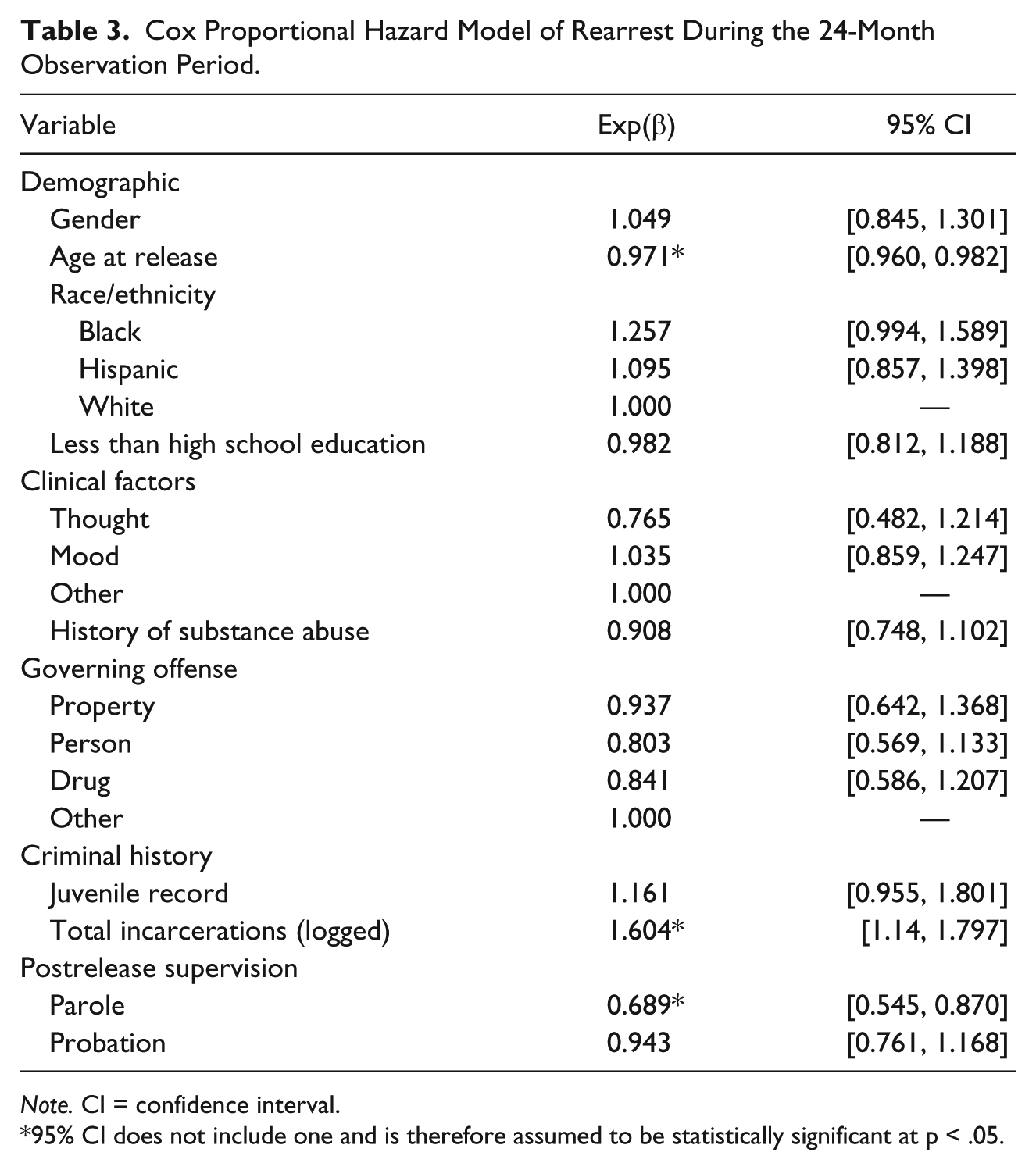
Note. CI = confidence interval.
95% CI does not include one and is therefore assumed to be statistically significant at p < .05.
Discussion
Caveats
This analysis examines attributes of persons who had received mental health treatment during their period of incarceration in Massachusetts MDOC facilities to determine which variables and “classes” of variables—demographic, diagnostic, criminal history, or postrelease supervision—were associated with rearrest as an event and with the period of time elapsed between release and rearrest. Before we discuss the implications of these findings, it is important to acknowledge numerous limitations. The Nagelkerke R2 of the model, .158, indicates that, roughly speaking, about 16% of the “variation” in odds of rearrest is explained by the set of variables available for inclusion in the model. The limitations on variables that could be included reflected our reliance on administrative data. We do not, for example, have information on these individuals’ use of mental health services post release nor do we have rates of compliance with medication and other treatment protocols among persons who did access services. We also have no data describing postrelease living arrangements or employment outcomes. These factors likely affect both the probability of rearrest and the amount of time individuals remained arrest free following release. We also had no information on the charges for which individuals were rearrested. It is likely that information on these factors would have increased the explanatory power of our models.
Limitations also extend to the interpretation of the effects associated with variables that were available and included in our analyses. As we noted in our “Method” section, the diagnoses available for these analyses were those included in inmates’ records and were based on assessment by MDOC clinical staff of inmates’ symptom presentations when they were assessed. These are not based on a formal diagnostic protocol, such as that used by Steadman and colleagues in their prevalence study of mental illness in jail settings (Steadman, Osher, Robbins, Case, & Samuels, 2009). Thus, the lack of effects associated with diagnoses in this study cannot be said categorically to support the conclusion that psychiatric diagnoses have no effect. It is also important to recognize that the behaviors associated with clinical diagnosis can vary widely across individuals. Some individuals’ symptoms, for example, paranoid delusions that lead to violence or manic episodes in which individuals engage in high-risk behaviors, can lead to rearrest. Others, those with major depression or bipolar disorder, may be too functionally incapacitated to engage in most criminal activities. Such variation may, in fact, contribute to the lack of significant effects observed with respect to diagnostic categories.
Implications
With these caveats in mind, we consider the implications of these findings. Perhaps the major finding here is that more than half of this cohort’s members had remained arrest free for 24 months after release, despite histories of substance abuse, serious mental illnesses, and prior criminal involvement. It is noteworthy that, although published literature suggests that persons with psychiatric illnesses experience more complicated reentry processes than do persons without such conditions (cf. Blitz, Wolff, Pan, & Pogorzelski, 2005; Morrissey et al., 2007; Travis, 2005; Wolff & Draine, 2004), the nature and severity of individuals’ behavioral health problems were, within this population and with the caveats issued above, not significant predictors of rearrest. Having a mental illness may complicate reentry but the nature of the illness itself may not.
Equally noteworthy, perhaps, is the fact that the profile of the person who is rearrested (and rearrested more promptly) is weighted almost entirely toward criminal justice factors. Persons with juvenile records and more extensive histories of incarceration were, within this psychiatrically affected population, still the most likely to be rearrested. This is consistent with findings from other studies of samples similar to ours (Skeem, Manchak & Peterson, 2011). Even the one significant demographic factor, a negative effect of age on likelihood on rearrest, is consistent with the pattern of desistence from offending that has been noted in previous studies (Moffitt, 1993). In short, this model looks a great deal like a recidivism model one might observe in a general population of released inmates and is consistent with an earlier meta-analysis of studies by Bonta, Law, and Hanson (1998). It is important to note, however, that the charges on which inmates in this sample were sentenced were not significant predictors of recidivism; rather, it was inmates’ histories of criminal justice involvement that had the greatest effects. Overall, criminal involvement itself, rather than the type of crimes individuals commit, is the most robust predictor of subsequent criminal involvement. As Walters (1990) has noted with respect to the general population of offenders, chronic, protracted criminal justice involvement is associated with a lifestyle marked by low socioeconomic status and exposure to a host of socioenvironmental factors that may be highly criminogenic. A long tradition of research has noted that persons affected by mental illnesses are disproportionally located in lower socioeconomic areas. Chicago School sociologists Faris and Dunham (1939) observed this pattern in the early 20th century, and the phenomenon appears to persist into the 21st (Alverson et al., 2001; Drake & Wallach, 1989; Drake et al., 2005; Silver, Mulvey, & Swanson, 2002). Continual exposure to such environments following release from prison promotes a high level of risk for reoffending and rearrest. This appears to be the case even among persons with mental health disorders and is likely a contributing factor to their substantially elevated arrest rate (Fisher et al., 2011).
The pattern of findings reported here—the null effect of major mental illnesses and the predominance of criminal history factors—has implications for how criminal justice involvement among persons with mental illness is viewed by the disciplines that study and treat them. As we noted in our introduction, the past four decades have seen an enormous amount of research, much of it described in the psychiatric and psychological literatures, focusing on treating and providing services for persons with mental illness who become involved with the justice system. For this community, the “master status” often assigned to the psychiatrically involved arrestee, detainee, correctional inmate, defendant, or releasee is that of a person with mental illness who inadvertently and sometimes inappropriately has become entangled in the justice system. The remedy that has been proposed has been one that emphasizes the provision of appropriate mental health services as both curative and preventive (Fisher, Silver, & Wolff, 2006). This perspective has led to the alteration of traditional criminal justice entities and the development of new ones. These have included jail diversion programs, such as police-based crisis intervention teams (DuPont & Cochran, 2000) and mental health courts (Barr, 2003; Redlich, Steadman, Monahan, Petrila, & Griffin, 2005; Steadman, Redlich, Callahan, Robbins, & Vessilinov, 2011), special approaches to probation and parole (Lamberti, Deem, Weisman, & LaDuke, 2011; Skeem & Louden, 2006), and enhanced approaches to the management of releasees (Hartwell & Orr, 1999; Lamberti, 2007; Lamberti, Weisman, & Faden, 2004). All could arguably be categorized as emphasizing the “psychiatric” aspects of the individual’s status, with the extent of focus on criminal history sometimes less clear.
An Agenda for Criminologically Based Research on Offenders With Mental Illness
The findings of this study and those just cited point to the need for a new research agenda within criminology focusing on persons who have mental illnesses and who become involved in the justice system. First, we need to learn more about the prevalence and nature of criminal histories among persons in this population. Previous research focusing on criminal justice involvement among persons with serious mental illnesses has shown that arrest rates for a variety of offenses are much higher across the board than those for the general population (Fisher et al., 2011). A logical next step, then, would be to compare criminal histories and trajectories of persons “with and without” mental disorders. Any such effort would, of course, confront significant definitional issues with respect to “who does and does not have mental illness.” But, once these problems were addressed, such research could examine the prevalence and effects of the many criminogenic risk factors long noted by criminologists, such as those subsumed under the major predictors of criminal behavior referred to as the “Central Eight” risk/needs factors (Andrews & Bonta, 2006; Andrews, Bonta, & Wormith, 2006) as they apply to these subgroups. Only recently have these factors come to the attention of researchers focusing on offending among persons with mental illness (see Morgan, Fisher, & Wolff, 2010, for an overview of this issue), but they should become a major focus of both future research and the design of preventive interventions for this population. Research is also needed on how service entities, such as mental health courts and other diversion and reentry programs use such information in planning services and identifying appropriate settings and other factors that might reduce risk of rearrest.
Given the important effects of criminal histories in this study, a second research agenda might focus on the composition of these histories. There has been a significant body of research in criminology focusing on the question of specialization (e.g., Sullivan, McGloin, Pratt, & Piquero, 2006), and in developing methods for appropriately measuring the extent to which individuals’ offending records consist mainly of repeated incidents of the same type, such as burglary or drug dealing, or whether offense histories are more heterogeneous. Applying the conceptual principles and methodological tools developed by criminologists to investigate this question could be useful in examining similar patterns among individuals who have recognized psychiatric illnesses.
A related issue is that of patterns of offending over the life span. In this study, juvenile history was a powerful predictor of rearrest (although not of its timing). As we noted, developmental criminologists have examined this factor in great detail in general offender populations (e.g., Moffitt, 1993; Nagin & Land, 1993; Sampson & Laub, 1993) in the context of addressing the question of whether persons who are arrested during childhood or adolescence are likely to persist into adulthood or desist and forego adult offending and what factors are associated with persistence and desistence from offending at various stages of the life course (Sampson & Laub, 1993). But locating criminal histories in a causal framework that involves mental illness is complicated. Some diagnoses observed among this cohort, such as anxiety and personality disorders, reflect behavioral patterns that may have their origins in childhood or adolescence. Others, such as schizophrenia, although in some cases, originating in the late teens, often have their onset in early adulthood—too late, in many cases, for the disorders to have directly affected persons’ offending behavior in childhood or adolescence, unless prodromal symptoms appearing in the late teens began to cause problems leading to arrest. As Desai, Lam, and Rosenheck (2000) noted in their discussion of early offending among persons with mental illness who were homeless, arrest in this population is viewed by the mental health services community as “largely situational,”—that is, arising from circumstances related to failed mental health treatment and supports, and not as part of a longer trajectory that may date back to childhood or adolescence. Understanding the interaction between mental illness and early-onset offending in shaping risk for adult offending could be a useful focus of research for criminologists and could directly benefit the development of more refined recidivism risk assessments.
Persons with mental illnesses who are involved with the justice system, including those experiencing reentry into the community following sometimes lengthy periods of incarceration, present important policy challenges to the mental health community and to virtually all segments of the criminal justice system. They also are an interesting subset of the offender population, but one that has to date received little attention from the criminological research community. Applying criminological theories, methods, and perspectives to understanding the offending patterns of persons in this population offers a rich and largely unexplored set of opportunities for the criminological research community (Fisher, Silver, & Wolff, 2006).
Footnotes
Acknowledgements
The authors wish to acknowledge the assistance of the Department of Corrections in data compilation.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a National Institute of Mental Health (NIMH) Grant 1RC1MH088716-01, Stephanie Hartwell, PhD., Principal Investigator.