
Abstract
Frontline-administrator misalignment in general evaluations of health can undermine efforts to improve correctional officer well-being. This study examined optimization bias in correctional leadership—administrators’ overestimation of officer well-being. Using paired surveys from (n = 308) officers and (n = 104) administrators, cross-role perceptions regarding relational access and well-being revealed disparities between both groups. For example, all administrators indicated staff could approach them when experiencing problems, whereas only 31.9% of officers felt the same. Administrators also rated staff physical health higher than officers. Additional discrepancies concerned health interventions, with administrators favoring communication-based programs, while officers emphasized structural conditions as conduits to improved well-being. Strategies to align these perceptual outcomes are proposed in light of these findings.
Keywords
Introduction
Correctional officers (COs) work in environments defined by constant stress, danger, and strain (Ferdik & Pica, 2024; Ferdik et al., 2025). Decades of research show correctional staff experience disproportionately high levels of burnout, sleep disruption, hypervigilance, and trauma exposure, among other health maladies (Finney et al., 2013; Regehr et al., 2019; Schaufeli & Peeters, 2000). These pressures manifest not only as psychological fatigue, but as serious physical health concerns, including elevated cardiovascular disease, chronic exhaustion, and impaired functioning (Schultz & Ricciardeli, 2024). Officers routinely report that the demands of overtime and understaffing leave little opportunity for rest or recovery—conditions that contribute to absenteeism, turnover, and diminished safety (Siqueira Cassiano & Ricciardelli, 2023).
Despite the consistency of these findings and the clarity of officers’ own descriptions of strain, correctional systems have struggled to implement wellness approaches that meaningfully address the realities of frontline work (Miller et al., 2022; Schaufeli & Peeters, 2000). Officers frequently express that wellness efforts feel disconnected from their lived experience, overlooking material needs such as recovery time, adequate staffing, workable schedules, and accessible health supports (Ricciardelli et al., 2018; Schultz & Ricciardeli, 2024). These concerns highlight not only the severity of occupational stress, but also a persistent disconnect between what officers say they need and what institutions appear to understand about their day-to-day conditions (Finney et al., 2013). A critical but understudied contributor to this disconnect is the way correctional administrators perceive officer well-being. Administrators occupy roles that shape policy, allocate resources, and set expectations for workplace climate (Finney et al., 2013; Miller et al., 2022). Existing work suggests staff feel leadership is distant, difficult to approach, or unaware of the pressures officers face, especially regarding relational support and health concerns (Ferdik & Pica, 2024; Siqueira Cassiano & Ricciardelli, 2023). When administrators view wellness through different assumptions than officers, frontline needs may remain obscured (Ricciardelli et al., 2018; Schultz & Ricciardeli, 2024).
These issues underscore the importance of examining how leaders make sense of officer well-being—how they perceive relational dynamics, how they appraise the physical and mental health of their workforce, and how accurately they understand the conditions officers describe. Without clarity on administrators’ perceptions, it becomes difficult to explain why longstanding health risks among correctional staff continue to be met with limited or insufficient organizational response (Forman-Dolan et al., 2022; Regehr et al., 2019). Exploring these perceptual gaps offers an opportunity to better understand why wellness efforts so often fall short of officer experience and to illuminate the cognitive and relational barriers that shape decision-making in correctional environments. To address these needs, the current study collected mixed-methods questionnaire data from correctional officers and administrators employed in a unified, statewide jail system in Tennessee to ascertain perceptions of relationships and health between both sides.
Occupational Stress in Correctional Settings and the Role of Leadership Perceptions
Correctional officer well-being cannot be understood solely through exposure to occupational stressors. Instead, it must also be examined in relation to how correctional administrators perceive, interpret, and respond to those stressors. Large reviews demonstrate COs experience high levels of job stress, burnout, and other mental health concerns driven by organizational and operational conditions (Finney et al., 2013; Miller et al., 2022; Schultz & Ricciardeli, 2024). Yet comparatively little work directly examines how leaders cognitively appraise these conditions, or how those appraisals guide wellness-related decisions. Scholarship on CO health and on leadership cognition together suggests that wellness needs may remain unmet partly because administrators’ interpretations of staff well-being diverge from frontline experience (Butler et al., 2019; Johnston et al., 2022; Miller et al., 2024).
COs experience some of the highest levels of occupational strain among justice and public safety workers, including chronic exposure to violence, organizational pressure, and emotional labor (Finney et al., 2013; Schaufeli & Peeters, 2000; Useche et al., 2019). Systematic reviews document elevated burnout, sleep disruption, trauma-related symptoms, and psychological distress, with organizational climate and structure emerging as central drivers of stress (Finney et al., 2013; Miller et al., 2022; Page & Robertson, 2022). Health consequences include increased cardiovascular and other physical health concerns as well as a broader “mental health crisis” among correctional staff (Schultz & Ricciardeli, 2024; Useche et al., 2019). These burdens translate into organizational problems such as absenteeism, presenteeism, turnover, and reduced job satisfaction (Ferdik & Pica, 2024; Vickovic et al., 2022).
Despite decades of evidence, wellness programs remain limited or poorly aligned with frontline realities (Ferdik & Pica, 2024; Ferdik et al., 2022; Ricciardelli & Adorjan, 2020). Reviews and qualitative research emphasize that interventions must target organizational structure, climate, and communication rather than only individual coping (Finney et al., 2013; Johnston et al., 2022; Schaufeli & Peeters, 2000). Officers frequently report management is “less connected” to field work and does not fully understand or acknowledge their mental health concerns, calling for improved manager–staff relations, schedule reforms, and accessible mental health services (Ferdik et al., 2022; Johnston et al., 2022). This perceived disconnect between staff experience and leadership response is echoed in broader evidence that lack of administrative and organizational support predict higher stress and burnout (Finney et al., 2013; Page & Robertson, 2022).
Leadership interpretations of need and support therefore become pivotal. Experimental research shows that servant leadership training can improve perceived organizational culture and reduce depression, anxiety, and burnout among officers, with effects partly mediated by culture perceptions (Ferdik et al., 2022). Other work links transformational or motivational leadership to higher perceptions of procedural justice among COs (Baker et al., 2014). At the same time, correctional executives’ self-perceptions of emotional intelligence and leadership efficacy suggest leaders may see themselves as effective and capable, potentially differing from staff views of support and understanding (Harper, 2015).
Collectively, this scholarship indicates COs and administrators may inhabit different perceptual worlds regarding stress, support, and wellness. Organizational reviews stress that improving communication between management and COs is a key pathway to reducing job stress and burnout (Ferdik et al., 2022; Ferdik & Pica, 2024; Finney et al., 2013; Johnston et al., 2022). Understanding the cognitive and role-based mechanisms underlying these perceptual gaps is therefore central to explaining why severe, well-documented health risks among correctional staff persist despite extensive empirical warning signs (Miller et al., 2022).
Cognitive and Role-Based Mechanisms Underlying Judgment Discrepancies
The idea that administrators may systematically overestimate officer well-being aligns with research on leadership judgment and cognitive bias. Leaders often display optimism and positive self-appraisal in implementing organizational systems, which can shape how they interpret performance and well-being information (Hristov et al., 2022). In correctional contexts, executives report relatively high self-ratings of emotional intelligence and leadership self-efficacy, suggesting confidence in their capacity to manage people and emotions (Harper, 2015). Such self-views may support stability and legitimacy, but may foster overconfidence in how well leaders address workforce needs.
Organizational and behavioral research underscores that decision-makers operate within distinct informational environments. Frontline officers’ judgments are grounded in daily exposure to risk, heavy workloads, and moral strain (Ricciardelli et al., 2024). Their sense of wellness is shaped by direct experiences of fatigue, perceived danger, organizational conflict, and limited support (Fusco et al., 2021; Useche et al., 2019). Administrators, by contrast, typically engage officer well-being through aggregated indicators—formal complaints, performance metrics, absenteeism data, or episodic consultations—rather than continuous embodied exposure. Finney et al. (2013) characterize correctional organizations as highly hierarchical and bureaucratic, with structural distance between management and line staff that can itself be a stressor. Qualitative accounts from correctional workers in Canada similarly describe management as removed from “field work,” leading to perceptions that mental health concerns are unnoticed (Johnston et al., 2022). Ferdik et al. (2022) add to these discrepancies when reporting officers can be admonished by administrators for what they perceive to be unfair standards of conduct. Collectively, these findings parallel broader organizational evidence on cognitive distancing, where decision-makers removed from operational contexts rely on simplified representations that can obscure frontline strain (Hristov et al., 2022).
This distance has concrete implications for wellness implementation. Systematic reviews emphasize most consistent correlates of CO stress and burnout are organizational climate, supervisor support, and communication (Finney et al., 2013; Page & Robertson, 2022). Yet officers report cultural norms that discourage emotional disclosure, and both fear stigma and ambiguity about whether management will respond constructively to distress (Fusco et al., 2021; Johnston et al., 2022; Schultz & Ricciardeli, 2024). When leaders appraise problems primarily as individual coping failures rather than systemic issues, interventions tend to focus on resilience training or individual therapy instead of staffing, scheduling, and cultural reform (Miller et al., 2022; Schultz & Ricciardeli, 2024). Taking all these points into consideration, empirical evidence suggests alignment between correctional staff and management is of utmost necessity to improve officer wellbeing—an issue the current paper directly addresses.
The Current Study
The present study examines whether correctional administrators and officers differ systematically in how they perceive core aspects of staff wellness. Building on prior research documenting substantial officer stress and persistent gaps in organizational response, we focus on three domains central to wellness-related decision-making within correctional institutions: (a) relational accessibility, or beliefs about whether officers feel comfortable approaching administrators for support; (b) health appraisals, including perceptions of officers’ physical and mental well-being; and (c) support for wellness interventions, reflecting the types of resources each group views as valuable or necessary. Across these domains, officers and administrators bring distinct informational backgrounds, interpersonal experiences, and role-based cognitive perspectives. Officers’ assessments are grounded in daily exposure to demanding working conditions, whereas administrators’ judgments often rely on indirect indicators of staff well-being and broader organizational considerations. These divergent perceptual environments may produce systematic differences in how each group interprets staff needs, particularly regarding relational support, workplace health, and the kinds of interventions perceived as meaningful.
This study evaluates these cross-role perceptions using paired survey data from officers and administrators. By examining relational, health-related, and intervention-related appraisals side-by-side, the study provides an opportunity to assess whether administrators consistently adopt more favorable interpretations of staff well-being and workplace conditions than officers. In addition to quantitative ratings, open-ended responses are analyzed to enrich understanding of the cognitive frames and interpretive assumptions officers and administrators use when evaluating wellness needs. These analyses allow for a direct assessment of cross-role perceptual differences and provide empirical grounding for understanding how leadership cognition may influence the alignment—or misalignment—of wellness policy with frontline experience.
Method
This study used a mixed-methods design to examine whether correctional officers and administrators differ systematically in their perceptions of three wellness-related domains: relational accessibility, health appraisals, and support for wellness interventions. Open-ended survey items first captured how each group described wellness problems, sources of strain, and existing supports, allowing respondents to articulate their perspectives in their own language. Standardized, parallel quantitative items then assessed cross-role differences in relational judgments, perceived officer health, and intervention support. Qualitative responses provided interpretive depth and grounded context, while quantitative comparisons revealed patterned differences across roles (Creswell & Plano Clark, 2018). This design centers role-based perceptual divergence and aligns directly with the study’s focus on administrator–officer differences in wellness judgments.
Data Collection Procedures
The study was conducted within a unified statewide jail system in Tennessee comprising 120 county jails operating under a single regulatory authority: the Tennessee Corrections Institute (TCI). TCI establishes operational standards, conducts facility inspections, coordinates training, and maintains cross-facility communication, creating a shared administrative environment in which correctional staff experience broadly comparable organizational structures (personal communication with TCI Officials, 2024). This system-level uniformity provides a consistent context for examining differences in wellness perceptions between officers and administrators across facilities. Participants included (n = 308) frontline correctional officers and (n = 104) correctional administrators employed in all of Tennessee’s county jails. Officers served as custody personnel responsible for daily carceral resident supervision, while administrators included jail administrators, commanders, chief jailers, lieutenants, captains, majors, assistant administrators, and facility administrators responsible for oversight, policy implementation, and staff management.
Prior to collecting any data, a human subjects review panel at Austin Peay State University approved the ethical procedures of this study. Two parallel Qualtrics survey links were disseminated statewide: one to frontline correctional officers and one to jail administrators. Survey invitations were distributed by research team members to the work-based email addresses maintained by TCI of all jail-based personnel in the state. Data collection took place between 1 August 2024 and 1 February 2025. Once the digital survey link was clicked, this prompted respondents to a cover letter informing them of the voluntary and anonymous nature of the study, the identity of the investigators, the purpose of the study, and that all data would be reported in aggregated format to protect respondent privacy (Dillman et al., 2014). By-monthly emails were submitted by research staff reminding officers to complete the questionnaire, while all 120 jails posted flyers about the study in breakrooms. Monetary incentives were not possible in the current study due to limited funding, yet sample members were told their responses would aid in improving their health.
Data collection procedures produced, at best, modest CO response rates (308/5,544; 5.5%), yet fairly robust administrator ones (104/120; 86.7%). Such asymmetry is common in correctional research given chronic understaffing, rotating shifts, and mandatory overtime that constrain frontline availability (Ferdik et al., 2014; Ferdik & Pica, 2024). Rather than treating this difference solely as a methodological limitation, it is interpreted as substantively meaningful, reflecting the differential organizational capacity and time access that each structure how actors navigate health pathways.
Demographic breakdowns of each sample are reported in Table 1. Correctional officers were, on average, younger (M = 38.04 years) and had slightly less tenure (M = 6.82) than administrators (M age = 49.40; M tenure = 8.42). Educational attainment differed across roles, with officers most commonly reporting a high school diploma or some college (74.8%), whereas administrators were more likely to report postsecondary degrees, including two-year, four-year, or graduate education (55.8%). The officer sample was nearly evenly split by sex (50.9% male; 49.1% female), while administrators were predominantly male (64.4%). Racial composition was similar across groups, with White respondents comprising the majority of both officers (74.2%) and administrators (71.2%). Hispanic ethnicity, finally, was rare in the sample.
Sample Demographics for Correctional Officers (n = 308) and Correctional Administrators (n = 104).
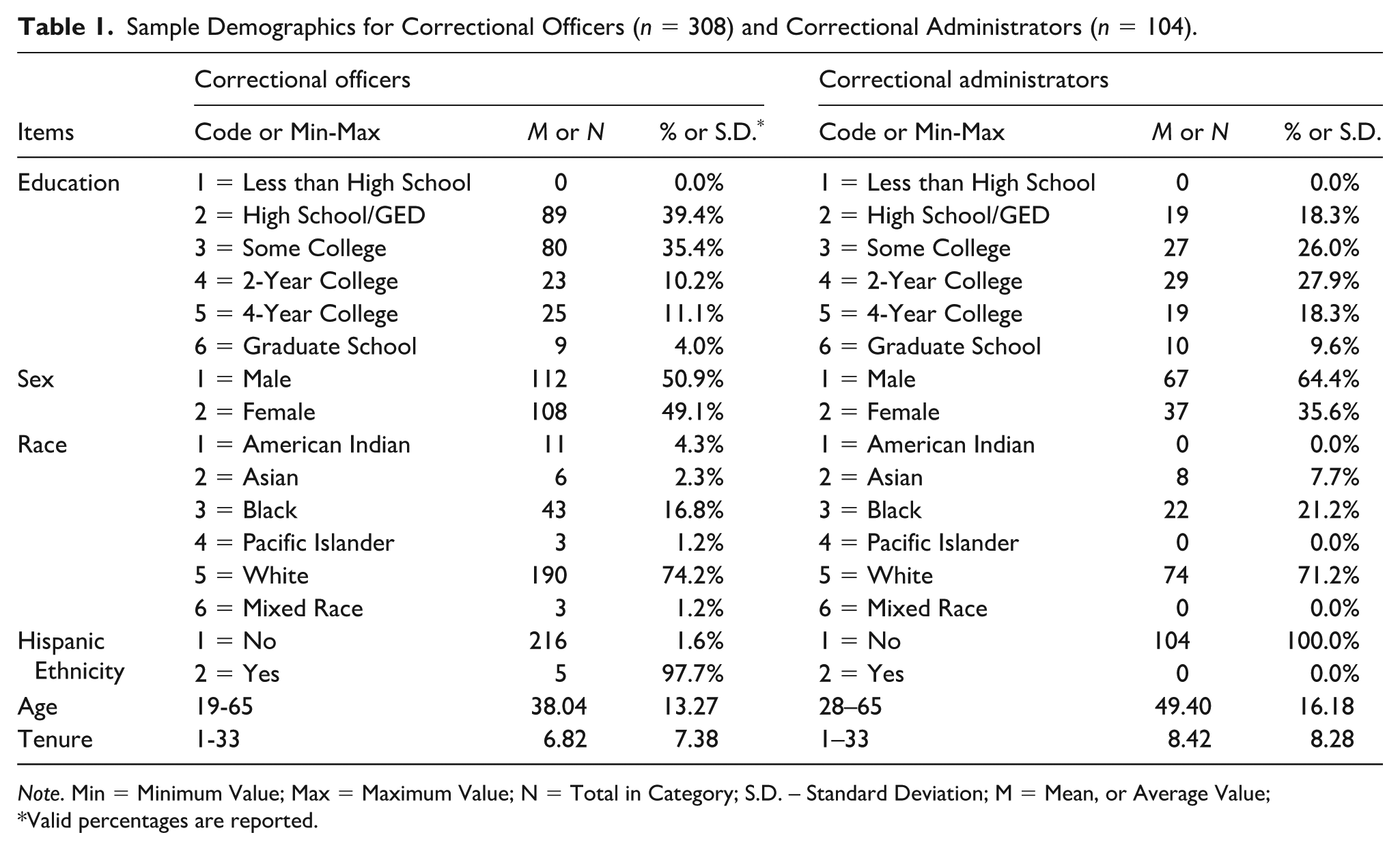
Note. Min = Minimum Value; Max = Maximum Value; N = Total in Category; S.D. – Standard Deviation; M = Mean, or Average Value;
Valid percentages are reported.
Instrument Development and Analytical Approach
The analytical approach combined instrument development, survey administration, and mixed qualitative–quantitative analysis to evaluate cross-role differences in wellness perceptions. The survey instrument was developed through a researcher–practitioner model in close collaboration with TCI where all parties contributed to item generation to ensure constructs reflected operational realities and role-based perspectives. Since no validated measures exist for cross-role assessment of correctional wellness perceptions, all items were research-generated following best practices for scale development in emerging domains (Creswell & Plano Clark, 2018; DeVellis & Thorpe, 2021). The final instrument included parallel items for officers and administrators across three domains central to the study: relational accessibility, health appraisals, and wellness-intervention support. Relational accessibility was assessed using matched 4-point Likert items that captured either administrators’ self-perceived approachability or officers’ comfort seeking help (e.g., “If my staff are experiencing problems, they can come to me”; “I feel comfortable going to administrators with problems”). Health appraisals were measured with parallel 4-point items assessing perceived officer physical and mental health, including whether officers were experiencing ongoing health problems. Officers evaluated the general health of their peer group, whereas administrators evaluated the health of staff they supervised. Intervention support was assessed through ratings of 15 wellness interventions on a 1–10 scale, including communication counseling, peer mentoring, critical-incident debriefing, suicide-prevention resources, mindfulness programs, servant-leadership training, family therapy, and structural supports such as regenerative breakrooms. In addition to these closed-ended items, the instrument incorporated open-ended questions inviting respondents to describe wellness concerns, resource needs, and perceptions of institutional support, providing qualitative depth to understand role-based interpretations of wellness.
Open-ended responses were analyzed using reflexive thematic analysis (Braun & Clarke, 2006), drawing on grounded-theory–informed procedures for coding, constant comparison, and memo-writing to support analytic rigor (Charmaz, 2014; Saldaña, 2016). Two coders independently reviewed all responses, generated initial codes, and iteratively refined themes to capture how officers and administrators described wellness challenges, interpreted physical and mental strain, and identified available or needed supports. Officers frequently emphasized embodied stress, fatigue, workload pressure, and material resource scarcity, whereas administrators more often emphasized procedural, communication-focused, or policy-oriented interpretations of wellness. Coding proceeded until thematic saturation was reached—bibr13-00111287261459989defined as the point at which additional data yielded no new conceptual insights across either role group (Hennink et al., 2017). Peer debriefing and iterative comparison enhanced the credibility and stability of thematic interpretations.
Using SPSS, quantitative analyses assessed cross-role differences within the three wellness domains. Likert-type items were dichotomized into agreement versus disagreement to facilitate direct comparison. Intervention ratings were dichotomized using a ≥7 threshold to indicate high support, consistent with decision-making cut points used in organizational and correctional wellness research (Agresti, 2021). Descriptive statistics summarized levels of endorsement for officers and administrators, and two-proportion z-tests evaluated group differences. Analytical attention focused on the direction and consistency of cross-role divergence, assessing whether administrators tended to provide systematically more favorable assessments of relational accessibility, officer health, or intervention value relative to officers. Integration of qualitative and quantitative results allowed qualitative themes to contextualize quantitative patterns, clarifying how officers’ and administrators’ conceptualizations of wellness problems and supports aligned—or conflicted—with their relational evaluations, health appraisals, and intervention preferences. This combined approach provided a comprehensive assessment of cross-role perceptual differences in wellness-related judgments.
Results
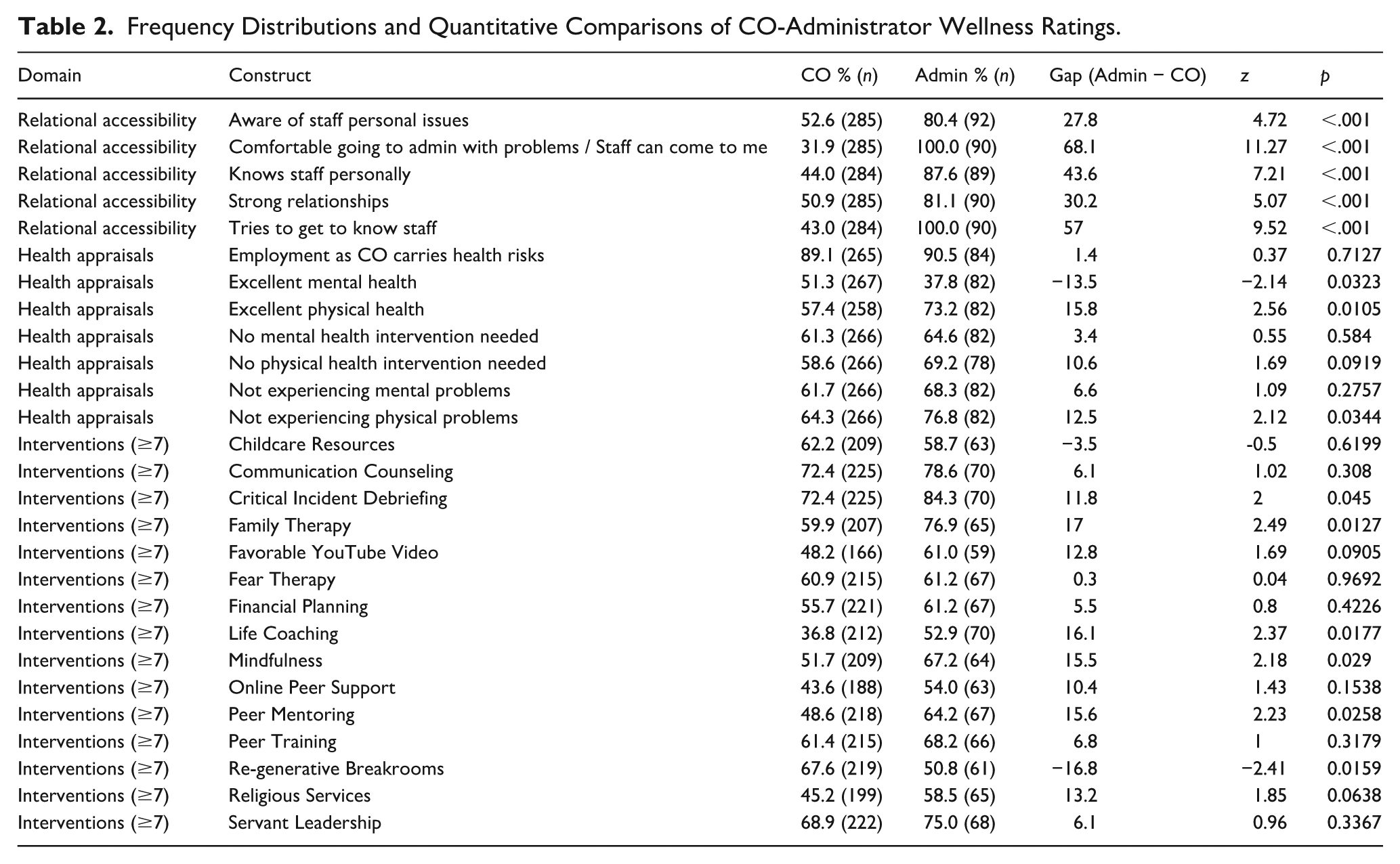
Table 2 displays results from the frequency distribution and quantitaive comparisons of correctional officers and administrators. Analyses identified clear quantitative and qualitative differences between administrators and officers across relational accessibility, health appraisals, and support for wellness interventions. In the area of relational accessibility, administrators consistently reported markedly higher agreement than officers on every item assessing approachability and relationship quality. Administrator agreement ranged from 80.4% to 100%, whereas officer agreement ranged from 31.9% to 52.6%. For example, all administrators (100.0%, n = 90) indicated that staff could come to them with problems compared to 31.9% of officers (n = 285), a 68.1-point difference (z = 11.27, p < .001). Administrators also unanimously agreed (100.0%, n = 90) that they try to get to know staff, compared with 43.0% of officers (n = 284), a 57-point difference (z = 9.52, p < .001). Similar gaps were observed for knowing staff personally (87.6% vs. 44.0%, z = 7.21, p < .001) and perceiving strong relationships (81.1% vs. 50.9%, z = 5.07, p < .001).
Frequency Distributions and Quantitative Comparisons of CO-Administrator Wellness Ratings.
Administrators’ written comments frequently emphasized daily interaction, intentional communication, and personal rapport. In addition to statements such as “Talk to them one on one,” “Talking and finding similar interest,” and “We talk daily. . . and are an outlet when we need time to vent,” administrators added: “I greet every staff member when I come in,” “I always check in to see how they’re doing,” “They know I’m there for them—my door is open all day,” and “I make rounds on all shifts so people see me and know I’m available.” Others highlighted supportiveness: “If someone needs advice, I stop what I’m doing,” “Staff know I’ll listen with no judgment,” and “We’re like a family here—I’m approachable anytime.”
Officer comments contrasted sharply, describing difficulty accessing administrators, limited presence, and inconsistent engagement. Alongside earlier statements (“Admin stays in their offices most of the time,” “Spend more time with the night shift,” “Have an open-door policy and make time to hear problems”), officers also wrote: “We barely see them unless something has gone wrong,” “They don’t come out unless it’s for paperwork,” “If we do approach them, it feels like we’re bothering them,” “They tell us their door is open, but they’re hardly there,” and “Most of the time they’re busy in meetings, so we don’t get the chance to talk to them.” Additional quotes included: “They don’t know our names,” “We are just bodies to them,” and “They don’t understand what the night shift goes through because they’re not here.” These qualitative comments were consistent with the large numerical gaps across relational items.
In the domain of health appraisals, administrator ratings were generally more positive for physical-health items, while mental-health items showed a mix of significant and non-significant differences. Administrators endorsed excellent physical health at 73.2% (n = 82) compared to 57.4% of officers (n = 258), a significant 15.8-point gap (z = 2.56, p = .011). Administrators were also more likely to state that officers were not experiencing physical problems (76.8%, n = 82) compared with officers (64.3%, n = 266), a 12.5-point difference (z = 2.12, p = .034). Officers, however, were more likely to report excellent mental health (51.3% vs. 37.8%, z = –2.14, p = .032). Other mental-health-related items revealed smaller, non-significant differences, including “not experiencing mental problems” (68.3% vs. 61.7%, z = 1.09, p = .276) and “no mental-health intervention needed” (64.6% vs. 61.3%, z = 0.55, p = .584). Both groups strongly agreed that correctional work carries health risks (Admin = 90.5%, CO = 89.1%; z = 0.37, p = .713).
Administrator comments often reflected broad or generalized assessments of staff well-being. In addition to statements such as “Most staff handle the stress well” and “We address issues when they arise,” administrators wrote: “Physically they’re in good shape overall,” “The job is tough but we manage it,” “Mental-health issues get taken care of when reported,” “Everyone is doing fine unless they tell us otherwise,” and “Stress happens but they know the job.” Some administrators highlighted reassurance from staff behavior: “No one has come to me with major concerns,” “They would reach out if they needed something,” and “I think morale is good given the workload.” Officers’ qualitative responses provided a different perspective, emphasizing ongoing physical strain, insufficient rest, and cumulative stress. In addition to earlier statements (“The job wears you down physically and mentally,” “We are constantly exhausted,” “Short staffing is killing our health”), officers wrote: “My knees and back hurt every single shift,” “We walk miles a day with no breaks,” “The mental stress piles up and we don’t have time to recover,” “People cry in their cars before work,” “We are burned out but can’t take sick days,” and “Most of us are just trying to survive the shift.” Additional comments included: “We hide injuries out of fear of losing overtime,” “There’s no time for mental-health appointments,” and “Administration doesn’t see what long shifts do to us.”
In the domain of support for wellness interventions, endorsement levels varied across intervention type. Administrators expressed significantly higher support for several procedural, programmatic, or interpersonal interventions. High-support endorsement for Critical Incident Debriefing was 84.3% among administrators (n = 70) versus 72.4% among officers (n = 225; z = 2.00, p = .045). Suicide-prevention training also showed higher administrative support (Admin = 84.3%, CO = 71.1%, z = 2.20, p = .028). Significant differences also appeared in support for Peer Mentoring (64.2% vs. 48.6%; z = 2.23, p = .026), Mindfulness (67.2% vs. 51.7%; z = 2.18, p = .029), Life Coaching (52.9% vs. 36.8%; z = 2.37, p = .017), and Family Therapy (76.9% vs. 59.9%; z = 2.49, p = .013). Several interventions showed high support from both groups, though administrators typically reported higher ratings. Some differences, while not statistically significant, were descriptively relevant. For childcare resources, 62.2% of officers (n = 209) endorsed high support compared with 58.7% of administrators (n = 63); although the –3.5-point difference was not statistically significant (z = –0.50, p = .620), officers frequently emphasized the importance of childcare access in qualitative responses.
Administrator comments describing intervention support frequently emphasized communication, reflective practices, and professional development. In addition to earlier statements (“Talking and finding common ground helps staff,” “Communication counseling would improve morale,”), administrators added: “Peer mentoring builds teamwork,” “Mindfulness could help reduce tension,” “Debriefings let people process tough events,” “Leadership training always benefits staff,” and “Counseling services are what staff need to talk things out.” Some framed interventions as opportunities for engagement: “It gives them tools,” “It helps them talk through issues,” and “Workshops bring people together.”
Officers presented a different emphasis, focused on time, space, recovery, and structural supports. Alongside earlier statements (“We need a place to decompress,” “A quiet room would help us more than another training,” “More space and breaks would help us more than another class”), officers added: “Breakrooms would help us reset during stressful days,” “We need resources that actually give us rest,” “Programs are good, but we need staffing to make them possible,” “Time is the issue—we can’t leave our posts,” “Long shifts drain us more than anything,” and “We need real support, not more trainings.” Regarding childcare, officers frequently noted: “Childcare would help with scheduling,” “It’s hard to find daycare with our hours,” and “Childcare support would reduce stress for many of us.” Across all three domains, the numerical results showed significant disparities on several items and additional non-significant but descriptively meaningful differences. The expanded qualitative comments offered a more detailed depiction of how respondents articulated relational accessibility, workplace health, and the perceived usefulness of various types of wellness interventions.
Discussion
This study proposed and tested optimization bias in correctional leadership—defined here as administrators’ systematic tendency to overestimate frontline officer wellbeing and relational accessibility (Ricciardelli & Adorjan, 2020)—and found strong evidence of cross-role perceptual divergence across relational accessibility, health appraisals, and wellness-intervention preferences. Rather than isolated differences, results revealed a consistent pattern: administrators offered markedly more favorable judgments about (a) how approachable they are, (b) how physically well officers are, and (c) the value of primarily communication- and program-oriented wellness supports, whereas officers emphasized the need for structural supports (e.g., rest, time, space, staffing) and described relationships with leadership as more distant and inconsistent than administrators perceived. These findings give empirical form to a longstanding concern in correctional health research: that the persistence of officer strain may be driven not only by exposure to operational stressors, but also by organizational barriers that shape what leaders “see,” believe, and therefore prioritize.
The most striking differences emerged in relational accessibility. Across every relational item, administrators endorsed far higher agreement than officers, with the single largest discrepancy concerning approachability. These are not small “differences in opinion”; they indicate that the two groups are describing different organizational realities. The qualitative data deepen the implications of these numbers. Administrators frequently described routine check-ins, open-door availability, and daily communication, whereas officers commonly reported limited presence, difficulty accessing leadership, and perceptions that administrators remain in offices, appear primarily when problems arise, and are disconnected from night shift conditions. In organizational terms, these results suggest that administrators may be using intent (“I’m available,” “my door is open”) as a proxy for impact (whether officers actually feel comfortable approaching them), while officers evaluate approachability through repeated, situational experiences—timing, visibility, responsiveness, and perceived safety in raising concerns. This is precisely the kind of cognitive mechanism that could sustain optimization bias (Ricciardelli & Adorjan, 2020; Wang et al., 2025): leaders infer relational accessibility from their own behaviors and self-concept, while frontline staff infer it from the costs and outcomes of seeking help.
These relational findings align with prior scholarship emphasizing the centrality of organizational climate, supervisor support, and communication to correctional officer stress and burnout (Ferdik & Pica, 2024; Ferdik et al., 2022; Johnston et al., 2022; Ricciardelli & Adorjan, 2020). Systematic reviews indicate that organizational stressors—and not only operational dangers—are robust predictors of burnout and distress, often mediated through perceived support and climate (Evers et al., 2019). Research also shows that perceived leadership practices (e.g., transformational, procedural justice–oriented supervision) relate to staff outcomes such as stress, fairness perceptions, and organizational commitment (Ferdik et al., 2025). In this context, the present results extend existing work by showing that the challenge is not merely “leaders should communicate better,” but that leaders may believe communication and accessibility are already strong—reducing the likelihood of organizational change because the problem is not recognized as such.
Cross-role differences were also evident in health appraisals, although in a more nuanced way. For instance, qualitative officer comments emphasized fatigue, cumulative pain, and physical wear-and-tear (e.g., back and knee problems, constant exhaustion), often linked to understaffing and long shifts. Administrators, by contrast, tended to describe staff as “doing fine unless they tell us otherwise,” a framing that implies a reporting-dependent model of health awareness: if officers do not raise concerns, leaders assume concerns are minimal. This finding is consistent with correctional health scholarship documenting physical health risks (including sleep disruption and broader physiological consequences) among correctional staff and the role of organizational conditions (overtime, staffing shortages, rotating shifts) in producing chronic strain (Evers et al., 2019). Where this study adds value is in identifying a plausible organizational mechanism: administrators may not observe the daily bodily toll of the job (or may interpret absence of formal complaint as absence of strain), fostering a rosier appraisal of physical wellbeing that can dampen urgency for structural reforms.
Mental health results were more mixed. Officers were more likely than administrators to report that officers have excellent mental health. At first glance, this seems to contradict an “administrators always more optimistic” narrative. But there are multiple plausible interpretations that still fit the optimization-bias framework. One possibility is that officers’ “excellent mental health” endorsements reflect identity and occupational culture dynamics: corrections work is characterized by norms of toughness and emotional control, and some staff may interpret mental health through a lens of resilience, coping, or “handling it,” even while describing exhaustion, burnout, and distress in open-ended responses (Ferdik et al., 2024). Another possibility is that administrators—given their responsibility for liability, performance, and staff stability—may be more attuned to mental health as an institutional risk and therefore less willing to endorse “excellent” ratings even while believing intervention is not needed. Indeed, the groups were relatively similar on items like “no mental health intervention needed” and “not experiencing mental problems,” where differences were small and not statistically significant. Regardless, the broader message remains: cross-role appraisals of health are not simply mismatched—they are grounded in different informational environments and different thresholds for what counts as “doing well,” which can yield inconsistent signals for wellness planning. Prior reviews emphasize that correctional worker wellbeing must be understood as a system-level issue shaped by organizational structure and culture, not only individual coping capacity. The present study supports that conclusion by showing that leaders and frontline staff may not even share the same diagnostic picture of where the primary health problems lie.
The third domain—support for wellness interventions—illustrated a clear misalignment in what each group sees as most valuable. Administrators reported significantly higher support for multiple communication and counseling-oriented interventions, including critical incident debriefing, suicide-prevention training, peer mentoring, mindfulness, life coaching, family therapy, and related services. Officers, in contrast, repeatedly emphasized the constraints that make many interventions feel unrealistic or symbolic: “time is the issue,” “we can’t leave our posts,” and “we need real support, not more trainings.”
Qualitative data reinforced this pattern, with officers describing a need for spaces to decompress, opportunities for rest, and staffing levels that permit breaks. This reflects a broader theme in the correctional wellness literature: interventions that focus only on individual resilience or programmatic add-ons often fail when the fundamental organizational conditions—staffing, schedules, overtime, operational tempo—remain unchanged (Ricciardelli & Adorjan, 2020; Siqueira Cassiano & Ricciardelli, 2023). Systematic reviews and mixed-method syntheses similarly emphasize that organizational reforms targeting climate, communication, and working conditions are essential, and that wellness initiatives can be perceived as disconnected from reality when they ignore structural strain (Evers et al., 2019). Importantly, this does not mean administrators’ preferred interventions are “wrong.” Many of the administrator-endorsed items (e.g., critical incident debriefing, suicide prevention training, family supports) are consistent with documented occupational exposures to trauma and distress among correctional staff and the need for supportive services. Rather, the issue is priority and feasibility: officers appear to view structural supports as prerequisites for other programming. Without sufficient staffing, schedule predictability, and protected time, even well-designed counseling or peer supports may be underutilized, inaccessible, or experienced as performative.
Policy Implications
The present study contributes relevant policy implications in three primary ways. First, it shifts attention from documenting officer stress (which is already well established) to documenting the cross-role perceptual gap that may explain why evidence does not translate into policy. Second, by operationalizing leader–staff differences across relational, health, and intervention domains, it demonstrates that misalignment is not confined to a single area but may reflect a more general cognitive-organizational pattern. Third, the mixed-method design reveals that the gap is not merely quantitative; it is experiential and interpretive, with administrators and officers emphasizing different mechanisms of wellness and different constraints on change.
In doing so, the findings echo, but also extend, the broader organizational justice and corrections leadership literature. Leadership models such as transformational and procedural justice frameworks emphasize that perceived fairness, voice, and supervisor legitimacy influence staff attitudes and stress (Ferdik et al., 2025). What this study adds is evidence that leaders may misperceive the very relational conditions (voice, accessibility, approachability) necessary for those leadership models to function in practice. If officers do not experience administrators as accessible, then procedural justice and supportive leadership may not be “received” regardless of leader intent. This helps explain why some wellness and culture reforms underperform: the barrier may not be program design alone, but the perceptual gap that shapes whether frontline staff believe the system is responsive and safe to engage.
The findings therefore imply that effective correctional wellness policy must begin by treating perceptual alignment as a policy target—not merely an interpersonal ideal. When administrators hold unanimously positive views of relational accessibility while most officers report discomfort approaching leadership, wellness decision-making is likely to be guided by incomplete or distorted information. Agencies should institutionalize mechanisms that reduce optimization bias by creating routine, structured, and protected feedback loops that do not depend on officers individually taking relational risks (e.g., anonymous pulse surveys, third-party climate assessments, confidential listening sessions across shifts, and systematic reporting on “barriers to seeking help”) (Ferdik et al., 2022). Importantly, these feedback systems should be designed to reach night shift and high-overtime staff, since officer comments highlighted perceived administrative absence and uneven visibility across shifts.
Second, wellness policy should adopt a “structural-first, services-second” sequencing model. Officers’ emphasis on time, recovery, and staffing indicates that counseling, debriefings, peer supports, and trainings may be most effective when agencies simultaneously provide operational conditions that allow participation and follow-through. The significant officer preference for regenerative breakrooms, alongside qualitative calls for decompression space and rest, suggests that relatively pragmatic environmental changes—paired with staffing and scheduling reforms—may increase perceived legitimacy of wellness efforts and reduce cynicism toward “another training” (Ferdik et al., 2022; Ricciardelli & Adorjan, 2020). Third, agencies should treat leadership development as both a cultural and cognitive intervention. Prior evidence indicates leadership training (including servant leadership interventions) can improve culture perceptions and reduce burnout-related outcomes (see Ferdik et al., 2025), which makes leadership an actionable lever. However, the present findings imply that training should explicitly address cognitive bias and perception calibration—helping administrators test assumptions about approachability and staff wellbeing against frontline data, and requiring leaders to demonstrate accessibility through measurable practices (e.g., documented rounds across shifts, response-time standards, and formal mechanisms to close the loop on staff concerns).
Limitations and Future Research
Several limitations should be considered when interpreting these results. First, the study relied on self-report survey data, which can be influenced by social desirability, role-based incentives, and differences in how constructs are interpreted. This is particularly relevant to sensitive domains like mental health and leader approachability, where respondents may answer in ways consistent with identity, or perceived expectations. Relatedly, the cross-sectional design captures perceptions at one point in time and cannot establish causal pathways. Second, response-rate asymmetry is an important consideration. Officer participation was modest (308 of 5,544; 5.5%), while administrator participation was high (104 of 120; 86.7%). Although low response rates are common in correctional research due to understaffing, overtime, and shift demands, the possibility of nonresponse bias remains. Officers who responded may differ systematically from those who did not (e.g., more engaged, more dissatisfied, or more health-conscious), which could affect estimates of officer perceptions. At the same time, the magnitude and consistency of the relational gaps—especially the large differences on multiple items—suggest that the overall conclusion of perceptual divergence is unlikely to be an artifact of minor sampling variation, even if precise percentages could shift with higher participation. Third, measurement limitations apply. Because validated cross-role instruments for these constructs are limited, items were research-generated and then dichotomized for comparison. Dichotomization facilitates interpretability but can reduce nuance and statistical power by collapsing response categories. Future work would benefit from developing and validating multi-item scales for optimization bias and relational accessibility in correctional settings, and from triangulating survey data with behavioral indicators (e.g., administrator rounds, help-seeking patterns, EAP utilization, grievance trends, absenteeism) to strengthen inference about alignment and its organizational consequences.
Concluding Remarks
This study examined whether correctional administrators and officers differ systematically in perceptions of relational accessibility, CO wellbeing, and wellness-intervention priorities. Results revealed consistent cross-role gaps, particularly in relational accessibility, alongside more optimistic administrative appraisals of physical health and stronger support for communication-based interventions, whereas officers emphasized structural constraints. These patterns align with the concept of optimization bias and help explain why wellness initiatives often remain misaligned with frontline experience. Future research should develop validated measures of optimization bias, test whether perceptual alignment predicts downstream outcomes, and evaluate interventions designed to reduce leadership–staff perceptual gaps.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available on request from the corresponding author.
Data Declaration
The data are not publicly available due to their containing information that could compromise the privacy of research participants. Data reported in this study were not presented at any other venue, including other journal outlets, or at conference presentations. The findings from this study have exclusively been reported to this journal alone. Further, none of the data were posted on public forums such as listervs, or other websites as this would have violated the terms of the Institutional Review Board requirements.