
Abstract
This article examines the contemporary trends of therapy and life-‘skills’ training. Several interrelated implications are drawn for the understanding of contemporary modernity. There is a continued modernist belief in the attainability of complete control in life, and faith in knowledge/expertise and instrumental rational control. Hence, life’s contingencies are construed as eliminable or resolvable ‘problems’, instead of unavoidable and given. There is a disempowerment of individuals who are thus rendered dependent on ‘experts’; correlatedly, there is a diminution of individual agency (responsibility) concerning the consequences of life choices and decisions, and the handling of life’s contingencies. These implications are at odds with the theses on contemporary modernity advanced by Giddens, Beck and Bauman. Enhanced empirical research into the diminution of individual agency has both scholarly and practical significance.
Introduction
This article examines the contemporary trends of therapy and life-‘skills’ training in affluent societies to draw their implications for the understanding of contemporary modernity. There is continued modernist belief in the attainability of complete control in life, and faith in knowledge/expertise and instrumental rational control. Hence, life’s intrinsic contingencies are construed as eliminable or resolvable ‘problems’ instead of unavoidable and given. Individuals hegemonized by the discourses of therapy and life-‘skills’ training become disempowered and rendered dependent on ‘experts’. Correlatedly, individual responsibility concerning the consequences of the making of life choices and decisions and the handling of life’s contingencies is diminished.
Therapy 1 is categorized into treatment therapy (concerning mental disorder 2 ) and, for want of a better term, ‘positive therapy’ (which aims to produce happiness and mental growth). Based upon analyses advanced by medical sociologists and various clinicians, it is shown how the disciplines of psychiatry and psychology have often been abused in mental health practices. In treatment therapy, this abuse creates growing numbers of purported disorders and the pathologizing of more and more people, resulting in the creation of phony victims. The therapeutic discourse implies continued faith in knowledge/expertise and instrumental rational control, and phony victimization implies disempowerment of individuals, dependence on ‘experts’ and diminished individual responsibility. Disempowerment and dependence afflict even non-phony victims who are nonetheless hegemonized by the therapeutic discourse.
In ‘positive therapy’, the above abuse creates what one clinician refers to as ‘myths of psychological change’. ‘Positive therapy’ entails all the implications mentioned in the opening paragraph. Many qualitative aspects of life are being transformed into so-called ‘skills’ which are seen as formalistically trainable-learnable. Such ‘skills’ include self-esteem, parenting, critical thinking, etc. All of the above implications also follow from this trend.
The above implications are inconsistent with the theses on contemporary modernity advanced by Giddens, Beck and Bauman. While their theses do apply to certain contemporary trends, our analysis shows that there are large numbers of individuals who, instead of casting reflexive doubt on rationality, actually harbour ungrounded faith in the ability of rationality to attain complete control of life’s contingencies by means of knowledge/expertise and instrumental control; and who, instead of exercising reflexive and autonomous agency and assuming self-responsibility, are disempowered and rendered dependent with diminished responsibility. Enhanced empirical research into the diminution of agency has both scholarly and practical significance.
Finally, the present article is, to some extent, a sequel to an earlier paper of the author’s appearing also in this journal (Lau, 2009), with the title of ‘The contemporary culture of blame and the fetishization of the modernist mentality’. In the last but one section of that article, I discussed how the contemporary culture of blame casts serious doubts on the theses concerning contemporary modernity advanced by Giddens, Bauman and Beck. As noted in the present article, there is a similar critique of their theses. Together, these two articles demonstrate that numerous contemporary trends show that, contrary to Giddens, Bauman and Beck, the grip of the modernist mentality on contemporary people to the extent of its becoming fetishized is still very strong.
Rule of the therapeutic
In 1980, 10 million antidepressant prescriptions were written in America (Horwitz, 2002: 78), by 2008, this had increased to 164 million (Menand, 2010). In England, qualified NHS clinical psychology staff increased by 29.2 percent (from 5514 to 7122) between 2001 and 2005; the British Association for Counselling and Psychotherapy’s membership jumped 7.1 times (from 4500 to 32,000) between 2001/2 and 2010, in comparison to a 2 percent and 3.9 percent population growth in England/Britain from 2001 to 2005 and 2001 to 2008 respectively. 3 In the following, it is shown that the rapid rise of therapy has been accompanied by its increasing discursive influence in society.
We schematically distinguish between treatment therapy (concerning mental disorder) and therapy aiming to produce happiness (e.g. marriage counselling), personality growth (e.g. being ‘never moody’) and release of human potential (e.g. ‘optimal psychological functioning’) – hereinafter, for simplicity and want of a better term, ‘positive therapy’ – though they constitute a partially overlapping continuum rather than a strict dichotomy.
Concerning treatment therapy, the mental disorder handbook DSM (Diagnostic and Statistical Manual) was initially compiled in 1952 with 106 diagnostic categories; its fourth edition (DSM-IV) of 1994 includes 297 categories (Conrad, 2007: 118). The number of people purportedly having mental problems has also grown tremendously. Thus, two national surveys based upon the DSM have been conducted in America in 1985 and 2001–3. They respectively reported that 48 percent and 46.4 percent of the population would suffer from one or more disorder over their lifetime; within a given year, the ratios were respectively 29 percent and 26 percent (Horwitz, 2002: 87; Satel and Sommers, 2005).
Thus, according to the therapeutic discourse, treatment therapy has grown because there are, first, many more kinds of mental disorders than previously known; second, mental disorder is not, as previously believed, exceptional, but common, e.g. OCD (Obsessive-Compulsive Disorder) and SAD (Social Anxiety Disorder aka Social Phobia) have over the years officially changed from ‘rare’ to ‘common’ (Peele, 1989: 1; Pettus, 2006: 41).
Concerning ‘positive therapy’, Giddens (1991: 34) argues that self-actualization therapy (equivalent to ‘positive therapy’) is ‘an expression of the reflexivity of the self’. If Giddens is right, ‘positive therapy’ has grown because western society has entered the era of ‘high modernity’ populated by reflexive individuals. Unsurprisingly, both the therapeutic discourse and Giddens’ argument have been contested.
Since the 1960s, sociologists and others have been advancing the medicalization thesis from different perspectives. Foucault and the 1960s anti-psychiatry movement argue that mental disorder does not really exist and dismiss the discipline of psychiatry altogether as pure discourse. Some constructionist sociologists focus solely on the process of how particular disorder categories have been constructed and are not concerned about whether or not these categories constitute real disorders.
We believe that a more convincing medicalization position to take is a realist-cum-constructionist one. This perspective, on the one hand, accepts the existence of real disorders which can, with a reasonable degree of plausibility, be distinguished from unreal disorders (this is the realist position); on the other, it agrees that room exists for extra-discursive factors to pathologize some normal psychological disturbances in a process of construction. 4 This is the position more or less explicitly adopted by medical sociologist Allan Horwitz and social work professor Jerome Wakefield; and implicitly taken by mental health scholars and clinicians who critique the therapeutic discourse from within the disciplines of psychiatry and psychology. Thus, a realist-cum-constructionist critique respects the disciplines of psychiatry and psychology, but critiques the abuse of these disciplines in the pathologization of normality.
A critique of the therapeutic discourse needs to begin with a look at psychiatry’s history. 5 In the 19th century, psychiatry assumed the form of asylum psychiatry focusing on severe psychoses believed to be organically based such as schizophrenia. Freud initiated a paradigm change to dynamic psychiatry in the following ways: (1) psychoses were ignored and focus turned to neuroses believed to be psychically based; (2) pathology was posited to be continuous with normality, since normality such as dreams and Freudian slips derived from the same psychic mechanisms as neuroses; (3) this vastly widened the scope of psychiatric intervention to everyday life problems in outpatient practices; (4) aetiology was foregrounded and symptoms, posited to be non-specific manifestations of unconscious mechanisms, devalued.
Dynamic psychiatry enjoyed hegemony in America up to the late 1960s; the first two editions of DSM (1952 and 1968) were both premised upon it. However, a confluence of factors, from economic, cultural to medical-scientific, raised demands that dynamic psychiatry was unable to meet. Of interest to us is that by the 1960s, medicine had discarded the role of case studies and come to stress statistical analysis and empirically rigorous criteria (in diagnosis, evaluation, etc.). Not only is dynamic psychiatry based upon case studies, it is also averse to hard and fast operationalization. At the same time, interrater diagnostic reliability (different clinicians arriving at the same diagnosis on the same patient) was notoriously low. Thus, psychiatry was under immense pressure to safeguard its professional position within medicine.
Two allied groups of researchers based in New York and St Louis took up the challenge by returning to asylum psychiatry’s principles. 6 They proposed to tackle the reliability problem by devising structured interview schedules to standardize elicitation of information from patients, and by laying down strict symptom-based diagnostic criteria for each diagnostic category. Further, they devised a new statistic (called kappa) to measure reliability.
In 1974, Robert Spitzer of the New York group was appointed head of the Task Force to produce DSM-III. This third edition, published in 1980, represented an overnight paradigm change from dynamic psychiatry to asylum-psychiatry-inspired diagnostic psychiatry. Neuroses were deleted as a class and replaced by various specific categories. DSM users were advised to pay no attention to aetiology and focus solely on a category’s list of symptom-based diagnostic criteria. From DSM-II’s 182 categories over 134 pages, DSM-III expanded to 265 categories over 494 pages. Field trials were conducted using kappa, which purportedly showed the new paradigm’s superiority in reliability. There were claims that the ‘reliability problem has been solved’ (cited in Spiegel, 2005: 61).
In a book-length examination of DSM-III’s field trials and all the researches published before and after the manual’s publication, Kirk and Kutchins (1992) convincingly show that despite DSM-III’s efforts to improve reliability, ‘the DSM-III results could more accurately be described as . . . similar to earlier studies’ or ‘no worse than the 1950s and may be better’ (1992: 176–7). In 2005, Spitzer acknowledged: ‘To say that we’ve solved the reliability problem is just not true’ (cited in Spiegel, 2005: 62).
In returning to asylum psychiatry’s principles, DSM-III’s architects claimed that mental disorders were organically based. However, asylum psychiatry limited itself to psychoses, and in the original development of strict diagnostic criteria by the St Louis researchers only 14 disorder categories were enumerated. Psychoses do approach the general medical model of discretely differentiated, organically based pathologies. The same is not true of most of the conditions then being treated by practising clinicians. The overthrow of the dynamic paradigm already faced stiff opposition (see Lane, 2007 passim). Were asylum psychiatry’s principles to be strictly followed, most of the 182 categories listed in DSM-II would have to be eliminated, which was clearly out of the question. There was no choice but to inherit dynamic psychiatry’s legacy of multifarious categories. Spitzer subsequently admitted: ‘Because the DSM-III classification is intended for the entire profession . . . the Task Force has chosen to be inclusive rather than exclusive . . . [if a condition’s] identification is important in the clinical work, it is included’ (cited in Horwitz, 2002: 71). The recategorization of dynamic psychiatry’s legacy in accordance with diagnostic psychiatry’s principles, and the acceptance of new categories proposed (many originating from practising clinicians) expanded the number of categories from DSM-II’s 182 to DSM-III’s 265.
Further, dynamic psychiatry is not particularly known for research backing. Hence, in taking up its legacy, DSM-III is on extremely shaky evidential grounds. One Task Force consultant admitted: ‘There was very little systematic research . . . the majority of us recognized that the amount of good, solid science upon which we were making our decisions was pretty modest.’ Allen Frances, later to become head of DSM-IV’s Task Force, described DSM-III’s expansion as ‘wild growth and casual addition’ (cited in Spiegel, 2005: 58, 61 respectively).
In inheriting dynamic psychiatry’s legacy, DSM-III legitimized its intervention into normal everyday life problems. What’s more, because DSM-III claims to be based upon the medical model, this model was now applied not only to psychoses but across the board, thereby pathologizing normal psychological disturbances as conceptually comparable to psychoses. DSM-III’s architects did make an attempt to remedy this by providing a definition of mental disorder (missing in both DSM-I and DSM-II), specifying that disorder occurs only when symptoms are outcomes of internal dysfunction (cf. note 2). However, the definition leaves dysfunction undefined, and, even more consequentially, it is completely ignored when it comes to individual categories as users are advised to focus solely on the presence of symptoms in making diagnosis. This renders DSM’s validity as an instrument seriously problematic because meeting the symptoms required itself does not necessarily entail the presence of disorder. 7
Closely related to this is the setting of diagnostic thresholds: how many criteria need to be satisfied from a list set; how long the symptoms have persisted. As diagnosis is advised to be made without regard to the dysfunction issue, the setting of thresholds, as Kutchins and Kirk (1997: 36) point out, becomes ‘largely arbitrary’. Defenders of DSM have admitted as much (Kessler et al., 2003: 1118). It has been revealed that DSM-III’s Task Force initially desired to set high thresholds, but ‘to accommodate . . . concerns of the psychiatric community . . . the threshold for making a diagnosis was lowered’ (cited in Lane, 2007: 57). A lower threshold, of course, entails positive diagnosis for more people. DSM-III’s low thresholds have been maintained in DSM-IV (Satel and Sommers, 2005).
Allen Frances, head of DSM-IV’s Task Force, made it extremely hard to add new categories to DSM-IV – DSM-III-R’s (revised, published in 1987) 292 categories expanded to 297 only in DSM-IV. However, as Frances revealed in private correspondence, his policy was also to retain DSM-III-R’s categories despite their shaky evidential basis (cited in Kutchins and Kirk, 1997: 171–2; cf. Horwitz, 2002: 79–80). DSM-IV also retained DSM-III’s definition of disorder, but likewise ignored it when it comes to making diagnosis. In a word, DSM-IV retains all the crucial problems afflicting DSM-III (validity [including low thresholds], reliability, lacking evidential support).
Horwitz (2002) argues that DSM-IV’s categories fall into four types: (1) psychoses which are valid disorders constituting diseases; (2) valid non-psychotic disorders which do not constitute diseases; (3) distress as normal response to transient stressful situations; and (4) social deviance. The last two categories are not outcomes of internal dysfunctions, hence do not constitute valid disorders. Horwitz and Wakefield 8 are leading critics of DSM from the realist-cum-constructionist angle. Remarkably, Robert Spitzer (2007), chief architect of DSM-III and III-R, has recently publicly endorsed their particular critique of DSM for pathologizing normality (while distancing himself from purely constructionist critiques).
Moreover, in the mental health market, disorder is extended beyond DSM (Dineen, 1996: 77–8). The case of PTSD (Post-Traumatic Stress Disorder) illustrates this. DSM-III-R defines traumatic experience in relation to PTSD as first-hand experience of ‘distressing events [such as war] that is outside the range of usual human experience (i.e. outside the range of such common experiences as simple bereavement, chronic illness, business losses, and marital conflict)’ (cited in Westervelt, 1998: 130). DSM-IV revises this to ‘the person experienced, witnessed, or was confronted with an event or events that involved actual or threatened death or serious injury, or a threat to the physical integrity of self or others [which extends coverage to rape and abuse cases]’ (Psychiatric News, 18 October 2002: 25). In other words, also counting now are more common experiences and, as Summerfield (2001: 97) notes, ‘second hand shocks’ such as ‘hearing the news [“confronted with”] that something bad has happened to someone to whom one is close’.
In DSM-IV, the traumatic event is at least in relation to actual or threatened death, serious injury or physical integrity. In the mental health market, however, practitioners have applied PTSD to cases such as: betrayal (Nolan, 1998: 64); parting with someone close, losing a pet, experiencing discrimination (Dineen, 1996: 67, 231); being kissed in public, being sacked, minor automobile accidents (McNally, 2003: 281); verbal sexual harassment, difficult labour (with healthy baby) (Summerfield, 2001: 96). 9
Various mental health researchers and clinicians have voiced support for the critique of DSM and its further extension in the mental health market. Clinicians such as Peele (1989) and Dineen (1996) have published book-length critiques. Though such lengthy treatises are exceptional, many have made critical remarks. To mention just a couple of more recent instances, in a 2005 interview, London-based psychiatrist Isaac Marks, who coined the term ‘social anxiety’ in 1969, said that psychiatrists have eroded the distinction between normal and acute anxiety, while much of the current literature constitutes an ‘advertising ploy’ for drug companies (Lane, 2007: 7, 13). Similarly, as already mentioned, in 2007 Robert Spitzer endorsed the critique of DSM as pathologizing normality.
Various social and cultural critics have also written on medicalization. Among recent academic medicalization studies, Conrad (2007: Ch. 3) argues that the extension of Attention Deficit/Hyperactive Disorder from children to adults merely medicalizes underperformance; Lane (2007) argues that shyness, a character trait, has been illegitimately medicalized into Social Anxiety Disorder; Horwitz and Wakefield (2007) argue that DSM fails to distinguish between normal sadness and Major Depressive Disorder.
In view of the above, how many people suffering only from normal psychological disturbances are diagnosed with a disorder because the therapeutic discourse pathologizes such normal disturbances? We refer to these people as phony victims. It should be noted that ‘phony’ here has nothing to do with fraud. Fraud involves conscious faking (on the part of the client) and/or reporting (on the part of the clinician) of symptoms. In the case of phony victimization, the symptoms required for making the diagnosis are met, hence both clinician and client are acting in good faith.
In two American surveys in the 1980s, half of those entering treatment therapy did not have a diagnosable DSM problem (Horwitz, 2002: 221–2). In the early 1990s, 15 percent of Americans received treatment therapy annually (Horwitz, 2002: 4). In the previously mentioned 1985 national survey, the conditions of 5.4 percent were serious by DSM’s criteria (Horwitz, 2002: 105). If, like Horwitz, we take for comparison’s sake this as somewhat closer to the real disorder rate, this implies a phony victimization rate of 28 percent ([7.5 percent – 5.4 percent]/7.5 percent). As noted, the pathologization of normal suffering extends beyond DSM in the mental health market. However, without further investigation, it is impossible to tell how far this would push the phony victimization rate further up.
In 2005, 10 percent of Americans were on antidepressants alone (Menand, 2010). According to the American Camp Association, which serves 3 million children campers, 25 percent of the children staying at their camps were on medication for various purported mental disorders (Gross, 2006). In the second national survey in the early 2000s, the proportion of individuals in serious condition was 6 percent (Satel and Sommers, 2005), almost the same as in 1985. Does it follow from the above that the phony victimization had shot up drastically in comparison to the early 1990s? It is impossible to tell since it is unknown how many of those on medication had been diagnosed with a DSM disorder. But a higher phony victimization today does appear likely.
Of course, the above constitutes educated guesswork only. Evidence for Britain and elsewhere is especially lacking, though indications (e.g. the rise of counselling for pets dying [Furedi, 2004: 9]) suggest similar trends arising. Systematic evidence can most valuably be obtained at the clinical level, hence the value of book-length contributions from clinicians critical of the therapeutic discourse. However, existing works of this type date from the 1980s and 1990s; comparable up-to-date evidence is needed. Ethical considerations may apparently preclude direct access to clients by outside researchers; however, such possibilities do exist (see later).
In 2004, a survey by the British Association for Counselling and Psychotherapy found that 45 percent of the workforce would like confidential counselling from employers (Ecclestone and Hayes, 2009: 105). As seen, American data show that only a small percentage of individuals suffer from real mental problems, and the phony victimization rate is in the region of a few percentage points. If so, why would as many as 45 percent of employees see the need (though how strongly we do not know) for the provision of counselling? This suggests that many people who have not been diagnosed with a problem (either correctly or falsely) have nonetheless, to some degree, fallen under the influence of the therapeutic discourse which claims that mental problems are common on the assumption that humans are psychically vulnerable. 10
Nolan (1998, 2009) argues that in tandem with the rise of professional therapy, a therapeutic ethos has taken hold in America in civil law, political rhetoric, etc., and examines the spread of America’s ‘problem-solving court’, underpinned by the ethos, to the UK and other countries. Furedi (2004), Ecclestone and Hayes (2009), among others, have taken up Nolan’s concept. According to these scholars, the therapeutic ethos is a new sensibility that first foregrounds the emotive (from ‘I think therefore I am’ to ‘I feel therefore I am’ [Nolan 1998: 6]); and second, sees humans as emotionally vulnerable, and hence life events as readily damaging of people’s psyche. This second point is derived directly from the therapeutic discourse (mental disorder is common because humans are psychically vulnerable). Ecclestone and Hayes (2009) examine how the therapeutic ethos has now hegemonized British educational thought and policy. The increasing prominence of the therapeutic ethos, at least among policy-makers, advocacy groups and the like, is another indication of the therapeutic discourse’s increasing influence beyond phony victimization.
Victimization implies a deterministic model of action, while determinism excludes individual responsibility; hence the advocacy group Alcoholic Anonymous claim that the alcoholic is ‘powerless over alcohol’. Attention Deficit/Hyperactive Disorder (ADHD), Conrad (2007: 64–5, 139) argues, ‘shifts blame from the person to the body . . . provid[ing] a medical explanation for [the phony victim’s] underperformance. . . . A man who has come to see his ADHD as underlying the chaos in his life said, “I always thought I was stupid”.’ Promoters of the therapeutic discourse are fully aware of the exonerating effects of victimization: in 2001, the American National Mental Health Awareness campaign’s logo in one poster reads: ‘It’s not your fault’ (Lane, 2007: 132–3).
American courts have now accepted addiction to alcohol and gambling as exonerating ‘diseases’/‘disabilities’; charges ranging from homicide to welfare fraud have been defended or filed, to varying degrees of success, on the basis of Battered Women Syndrome, ‘urban survival syndrome’, ‘chronic lateness syndrome’, etc. (Peele, 1989: 27–8, 203–18, 220; Sykes, 1992: 3; Westervelt, 1998: Chs 1, 3 and 5). It is reasonable to assume that some of these cases involve phony victimization. The Americans with Disabilities Act affords individuals classified as having a disability certain rights, including immunity from dismissal for misbehaviour or poor performance. Thus, besides divesting individual responsibility, phony victimization also enables the seeking of state protection against consequences of life choices and decisions made by phony victims.
As noted, the phony victim acts in good faith, hence does not consciously shirk responsibility. Instead, the individual is now disempowered (by both self and society) for she is now regarded (by both self and society) as being incapable of solving her own problems, and instead made dependent on someone else to do it for her. This someone else is none other than the therapist. 11
Various clinicians have commented on this dual disempowerment–dependence of phony victims: ‘we are increasingly dependent on external agencies and less sure of our ability to manage our own bodies and our lives . . . more people today believe they are incapable of managing their lives and that some type of remedial experience [i.e. therapy]’ is needed (Peele, 1989: 245–6, 274). Harold Mulford, director of Alcohol Studies at the University of Iowa observes: ‘The alcoholism-disease way of thinking leads us to disown our responsibilities . . . it encourages us to relinquish our authority . . . to designated “experts” who are all too eager to assume the task’ (cited in Peele, 1989: 259). A study in the mid-1990s (cited in Horwitz, 2002: 172) found that the single most common precipitant for entry into treatment therapy is problems with social relationships. Assuming, as shown to be the case, that some of these are phony victims, it is clear that these individuals have disempowered themselves (regarding themselves as incapable of resolving normal life problems) and opted to depend on ‘experts’. 12 Wainwright and Calnan (2000) have coined the term ‘diminution of the self’ to refer to this dual disempowerment–dependence.
As noted, a 2004 survey in Britain found 45 percent of the workforce seeing the need for the provision of counselling from employers. Since most of them, as we have previously remarked, were neither real nor phony victims, this suggests that even non-phony victims who are nonetheless hegemonized by the therapeutic discourse are having a diminished view of themselves.
By taking up the role of a ‘victim’, the phony victim is thereby disempowered and made dependent. Hence, the occurrence of phony victimization necessarily entails disempowerment–dependence. Nonetheless, systematic evidence to demonstrate this in detail is clearly desirable. Again, such evidence is most valuably obtained at the clinical level: the above comments by Peele and Mulford are clearly informed by clinical observations. Opportunities do exist for non-clinicians to gain direct access to victims who may be phony ones. When Lane (2007: 205) presented his critique of Social Anxiety Disorder on various occasions, many in his audience’s reaction was ‘to express dismay over the growing number of students who press them each semester to be released from tests, exams [etc.] . . . on the grounds that they suffer from one or more disorders’. In other words, teachers relevantly equipped are in a good position to carry out systematic research, or systematic in-depth interviewing with teachers would likely provide valuable data.
As noted, there is evidence to suggest that even non-phony victims who are nonetheless hegemonized by the therapeutic discourse render themselves disempowered-dependent. Ecclestone and Hayes (2009: 44, 122–4, 164) worry that therapeutic education may produce diminished selves. Critiqued for lacking evidence, they report finding increasing echoes among teachers at seminars, etc. (2009: 146–7). However, for their worry to be substantiated, it will first have to be empirically established that students taught under such a regime are internalizing the therapeutic ethos, i.e. becoming hegemonized by it. Only if this is the case can we then go on to ask whether or not, as a result, students are rendered disempowered-dependent.
One point concerning our disempowerment arguments needs stressing. We certainly do not deny that there are real victims who therapy might be able to help or empower (though see later on the issue of therapy’s effectiveness), i.e. individual cases of empowerment do occur in clinical situations. However, our disempowerment argument does not concern that. Rather, it first concerns phony victims who should have relied on their own resources to handle normal disturbances. Cases certainly exist in which therapy enables the phony victim to feel better; to the therapist, this would constitute evidence of empowerment, but in terms of our analysis, the phony victim has already been disempowered. Our argument also concerns non-phony victims who, suffering from no real disorder but being hegemonized by the therapeutic discourse, believe that they need to undergo therapy without having yet done so, as well as individuals generally hegemonized by the belief that people are emotionally vulnerable. This disempowerment lies beyond the therapist’s clinical horizon.
Concerning ‘positive therapy’, in psychology, the belief/claim that psychological knowledge is able to produce the optimal psychological human dates back a long time. In an advertisement around 1900 (Moskowitz, 2001: photo opposite p. 102), the advertising psychologist promises ‘a plain road to health, success, poise and power’ for those suffering from, inter alia, ‘lack of ambition . . . weakness’. BF Skinner stated: ‘what do you say to the design of personalities? . . . Give me the specifications, and I’ll give you the man!’, and the optimal psychological human would suffer from ‘no failure, no boredom’ (cited in Zilbergeld, 1983: 5).
Therapists have since described the optimal psychological state thus: ‘No More . . . Feeling of Inferiority . . . Guilt’; ‘living without anxiety’; ‘depression is not a . . . genuine . . . human experience. It is a phony, synthetic counterfeit’; after ‘primal therapy’, clients are ‘never moody’; anger, guilt and worry are all ‘useless emotions’ (cited in Moskowitz, 2001: 224; and Zilbergeld, 1983: 198). In short, ‘positive therapy’ states that psychological certainty is attainable because anxiety, moods, etc. are not unavoidable (psychological) contingencies of the human condition, but ‘useless’ and ‘phony counterfeits’ that therapy can eliminate. 13
At this point, it is necessary to comment on the modernist mentality. Weber examines the modernist mentality in terms of formal, instrumental rationality. Instrumentally rational action constitutes a means to attain set ends; whereas formal rationality refers to the use of rules, procedures, and, where possible, ‘quantitative calculation’, as being the most efficient instrumental means. The modernist mentality believes that humanity ‘can, in principle, master all things by calculation [or formal, instrumental rationality generally]’ (Weber, 1946: 139). Picking up from Weber, Bauman (1992) sees the modernist mentality as being characterized by ‘an incessant drive’ to attain ‘free[dom] from contingency’ by means of reason so as to attain complete rational control of the future. In other words, the modernist mentality believes that knowledge and expertise (i.e. reason) are able to devise formal, instrumental methods to eliminate life’s contingencies, thereby enabling complete control and certainty.
The belief that psychological certainty is attainable by eliminating psychological contingencies thus accords perfectly with the modernist mentality. Therapists state that (psychological) contingencies can be eliminated by means of formal instrumental rationality in the form of psychological ‘skills’ which are seen as formalistically teachable-learnable. One therapist says of unsatisfactory relationships: ‘it is amazing how little formal training any of us gets in coupling skills . . . relationship enhancement skills’; another states that optimal mental health is achievable in ‘seven easy steps’. Famed physician Lewis Thomas observes: ‘new books about dying . . . with . . . step-by-step instructions for performing the function that you’d think this was a new sort of skill’ (cited in Zilbergeld, 1983: 25, 92, 110).
Two obvious questions arise: can psychological contingencies really be eliminated/cured? Does ‘positive therapy’ work? We can only attempt a few comments here. Concerning the first question, Bauman (1991: 16) rightly observes that contingency is ‘a lasting human condition’. Clinician Zilbergeld echoes him by subtitling his critique of ‘positive therapy’, ‘myth of psychological change’. In other words, ‘positive therapy’ problematically construes life’s contingencies as ‘problems’ which are then said to be therapeutically solvable. Concerning the second question, the conclusion of research findings on therapy in general (Dineen, 1996: Ch. 4 and pp. 234–9; Horwitz, 2002: 196–207; Zilbergeld, 1983: Chs 7–10) is that generally therapy does not work or can even be counterproductive (on counter-productivity see also British psychiatrist Simon Wessely’s [2005] summary of findings on the increasingly routine use of post-trauma therapy); where and when it does, it works in a similar way to generic social support provided by relatives and/or friends (Peele, 1989: 260). In sum, contingencies including psychological ones are intrinsic to life; whereas individuals may be able to better cope with them with the social support of relatives/friends or therapist or simply through maturation, the claim that they are eliminable by means of psychological ‘skills’ must be regarded with great scepticism.
We have argued that the therapeutic discourse in relation to treatment therapy engenders divestment of responsibility, disempowerment and dependence. The same applies to the discourse in relation to ‘positive therapy’, because in believing in the discourse and depending on it, users no longer accept psychological contingencies as given and take up the responsibility to deal with them by relying on their own resources. Based upon his own clinical experience and formal research, Zilbergeld (1983: 216–18) observes: ‘Another great cost of the therapeutic sensibility is a loss of confidence in ourselves. If we are . . . not living as we should [as the discourse of “positive therapy” says], we need to depend on experts to set us straight. . . . Clients ask if they are making the right decision to take up a certain course of study, or a certain career, or even a certain investment . . . they could have received the reassurance from a friend or relative, but they believe in experts.’ Even Giddens (1991: 143), who endorses ‘positive therapy’, admits that many therapists encourage dependence by ‘hold[ing] that without regular contact with a professional counselor there is no hope of real personal change’. 14 What’s more, Zilbergeld (1983: Ch. 11) details how once under therapy, the user’s incompetence to achieve the therapeutic goal is emphasized, thereby further strengthening reliance, not necessarily on the same therapy, but on therapy as a whole. The irony of this is that, faith in therapy undiminished, users blame failure not on the ‘experts’, but on themselves, indicating the extent of their disempowerment.
The implications of ‘positive therapy’ for understanding contemporary modernity are: (1) a belief in the attainability of (psychological) certainty in life because life’s (psychological) contingencies are seen as eliminable ‘problems’; (2) faith in instrumental rational control in the form of psychological ‘skills’ which are seen as formalistically teachable-learnable; (3) disempowerment and dependence on ‘experts’; (4) users’ self-divestment of responsibility to deal with life’s psychological contingencies by means of their own resources. Points (1) and (2) are what the discourse of ‘positive therapy’ is about; the extent of its influence can be gauged from existing studies such as Moskowitz (2001), though more systematic evidence (e.g. the growth in the number of ‘positive therapy’ clients), especially in societies other than America, is desirable; Zilbergeld has provided solid evidence of points (3) and (4) at the clinical level, but there is clearly a need for more such evidence.
The skillization of life: Formalized training of so-called life-‘skills’
What is called psychological competence refers to psychological ‘skills’ of handling life situations which are said to be formalistically trainable-learnable; these ‘skills’ are taught not only to therapy users, but also to non-users such as children. Popular ‘skills’ include anger/stress management, emotional ‘skills’, adversity ‘skills’ and so on. Ecclestone and Hayes (2009) provide a survey of the teaching of such ‘skills’ in UK schools. In the previous section, we have discussed ‘skills’ of ‘positive therapy’ taught by therapists; in this section we cover one skill of this nature (self-esteem) taught to students, and other kinds of life-‘skills’.
What we argue in this section is that qualitative aspects of life, such as the extent to which an individual develops a sense of self-esteem or how to discharge the responsibilities of being a parent, can only be acquired/learned in a contingent process through the experience of an individual’s own active engagement with life. They cannot be turned into formalistically trainable-learnable ‘skills’. The trend of doing exactly that carries the same implications for understanding contemporary modernity as the therapeutic trend. Thus, although self-esteem is tied to the therapeutic ethos, that ethos is irrelevant in this section. Our focus here is on the turning of qualitative aspects of life into so-called ‘skills’ per se. 15
Self-esteem theory argues reductionistically that social and personal problems ranging from drug addiction to poor grades all derive from the lack of self-esteem; that self-esteem is a ‘skill’ that can be taught-learned by means of formalistic techniques; and hence teaching school children this ‘skill’ can solve all the above problems. In America, self-esteem constitutes a veritable social movement (Nolan, 1998: 157) and its place in the curriculum now ranks alongside reading, writing and mathematics; in British schools, it constitutes a ‘core skill’.
According to the theory, guilt/shame feelings are counterproductive, hence children should never be made to feel guilt/shame. To achieve this, the child should always be told, in the words of one theorist, ‘over and over again how bright and talented he or she is’ (cited in Hewitt, 1998: 75) as well as made to feel that she is important and special, regardless of what she does or how she performs. To facilitate this, teachers and parents should create success, make failure improbable and praise the child for ‘doing well’. There are specific methods, step-by-step procedures and exercises for attaining these objectives (Hewitt, 1998: Ch. 4; Nolan, 1998: 164–5). In one typical exercise (Hewitt, 1998: 79), the teacher is asked to write ‘No matter what you say or do to me, I am still a worthwhile person’ on the board, to have the class copy it several times and then to start insulting the class in a good-natured manner. The class is instructed to respond to each insult by reciting the phrase in chorus. This would supposedly make children internalize the phrase and become immunized from guilt/shame feelings.
From the social psychological view, self-esteem is developed differentially between different individuals over the longer-term in the process of role-taking, social comparison and self-evaluation and in the context of an individual’s commitment to culturally endorsed values and activities (Swann, 1996). It is an outcome of active substantive engagement with life (Damon, 1995). This is why educator Mike Schmoker (1989) titled his critique of self-esteem theory ‘Self-esteem is earned, not learned’. Lasch (1992: 32) agrees: ‘Children need to risk failure and disappointment, to overcome obstacles. . . . Self-respect cannot be conferred, it has to be earned . . . [self-esteem theory] hopes to manufacture self-respect without risk.’
Without failure, self-esteem can only, as Lasch (1992) points out, result in an inability to value ideals and standards. It is only in this light that we can make sense of the celebrated case of William Hung. 16 In 2004, Hung auditioned for the American Idol television series. An adjudicator told Hung: ‘You can’t sing, you can’t dance, so what do you want me to say?’, to which Hung, who said he wanted ‘to make music my living’, replied: ‘I’ve done my best and I have no regrets’. The episode was posted on the Internet, whereupon Hung became an instant celebrity, inspired a cult following and landed a recording deal. With ideals and standards being devalued, it is unsurprising that not only does research evidence show no beneficial effects of teaching self-esteem, it shows rather demotivating effects (Furedi, 2004: 157; Hewitt, 1998: 58–60; Nolan, 1998: 169, 177).
Furedi (2002: 19) rightly observes that parenting ‘is a qualitative [matter] that cannot be improved by the application of a technical formula’. However, it has now been turned into a ‘skill’ which requires special formalistic training to learn. The parenting discourse enjoins parents to learn communication and listening ‘skills’, otherwise ‘communication channels may begin to close’. Detailed instructions are given on how to decode the child’s emotions, how to determine ‘whether any situation is growth-producing or not’, what words to use in response to negative behaviour and so on. Dos and don’ts are specified. According to University of Wisconsin professor Jack Westman, licensing should be introduced for parents because parenting is a complicated and demanding ‘skill’ (Furedi, 2002: 79, 85–7, 102). However, as in the case of self-esteem, research findings on the usefulness of teaching parenting ‘skills’ are decidedly unfavourable (Furedi, 2002: Ch. 9 and pp. 178–9).
To consider just one more illustration how qualitative aspects of life are being turned into ‘skills’, at an academic forum on university education several years ago where this author lives, a prominent public figure remarked in his address: ‘Intellectual curiosity, the ability to maintain a thirst for knowledge, and to look at things critically are skills we must impart to youth’ (South China Morning Post, 10 June 2006). No longer are intellectual curiosity and looking at things critically dispositions, attributes and aptitudes that people develop, to varying degrees, over the longer-term as the differential outcome of nature, nurture and contingency (e.g. meeting an inspiring person at the right time and place), they are rather ‘skills’ that could be taught-learned algorithmically.
A book titled Critical Thinking Skills (Cottrell, 2005) is typical of its kind. Critical thinking is said to be a ‘complex process’ including the following, enumerated in bullet-point format: ‘identifying other people’s positions, arguments and conclusions; evaluating the evidence . . .; weighing up alternative arguments and evidence fairly; being able to read between the lines . . . identifying false or unfair assumptions; . . . ’. We are further told that ‘critical analysis of other people’s reasons can involve’ (enumerated in the same format): ‘identifying their reasons and conclusions; analyzing how they select, combine and order reasons to construct a line of reasoning; . . .’. Critical thinking ‘is not about natural traits or personality; it is about a certain set of methods’ (Cottrell, 2005: 2–3). The book provides 250 pages of ‘easy-to-follow, step-by-step approach to developing a range of critical thinking skills’ (back cover), all written in the manner of an instructional manual complete with exercises. True, individuals who have over the longer-term developed a critical mind do identify other people’s positions, etc., but they do so spontaneously, not as so-called ‘steps’. No ‘set of methods’ can turn individuals who haven’t developed such an aptitude into critical thinkers.
Qualitative aspects of life cannot be made subject to instruction-manual-like formalized training. We propose to call the transformation of them into ‘skills’ the skillization of life. Its implications for understanding contemporary modernity are: (1) it regards uncertainties in (the qualitative aspects of) life, such as whether or not a sense of self-esteem is developed, as rationally solvable ‘problems’; (2) it harbours faith in instrumental rational control: a belief that qualitative aspects of life can be transformed into formalistic life-‘skills’; (3) it involves dependence on ‘experts’ in handling qualitative aspects of life, hence disempowerment and, by the same token, self-divestment of responsibility. Points (1) and (2) are what the skillization discourse is about. That many people believe in the discourse is evident in self-esteem’s immense influence, because, as said, on top of its underpinning by the therapeutic ethos, it epitomizes a belief in the transformability of a qualitative aspect of life into a ‘skill’. Reading through Ecclestone and Hayes (2009), one is struck by how authorities and educators alike conceptualize all aspects of education in terms of ‘skills’. Point (3) follows logically from the argument that qualitative aspects of life pertain to self-engagement with life. Actually, individuals who, as a result of learning self-esteem, are unable to value ideals and standards, and who (as research has shown) lack motivation to do substantive learning, constitute disempowered individuals. Nonetheless, much more work does need to be done to empirically substantiate point (3), such as with participants in parenting training.
Conclusion: Understanding contemporary modernity through the trends of therapy and the skillization of life
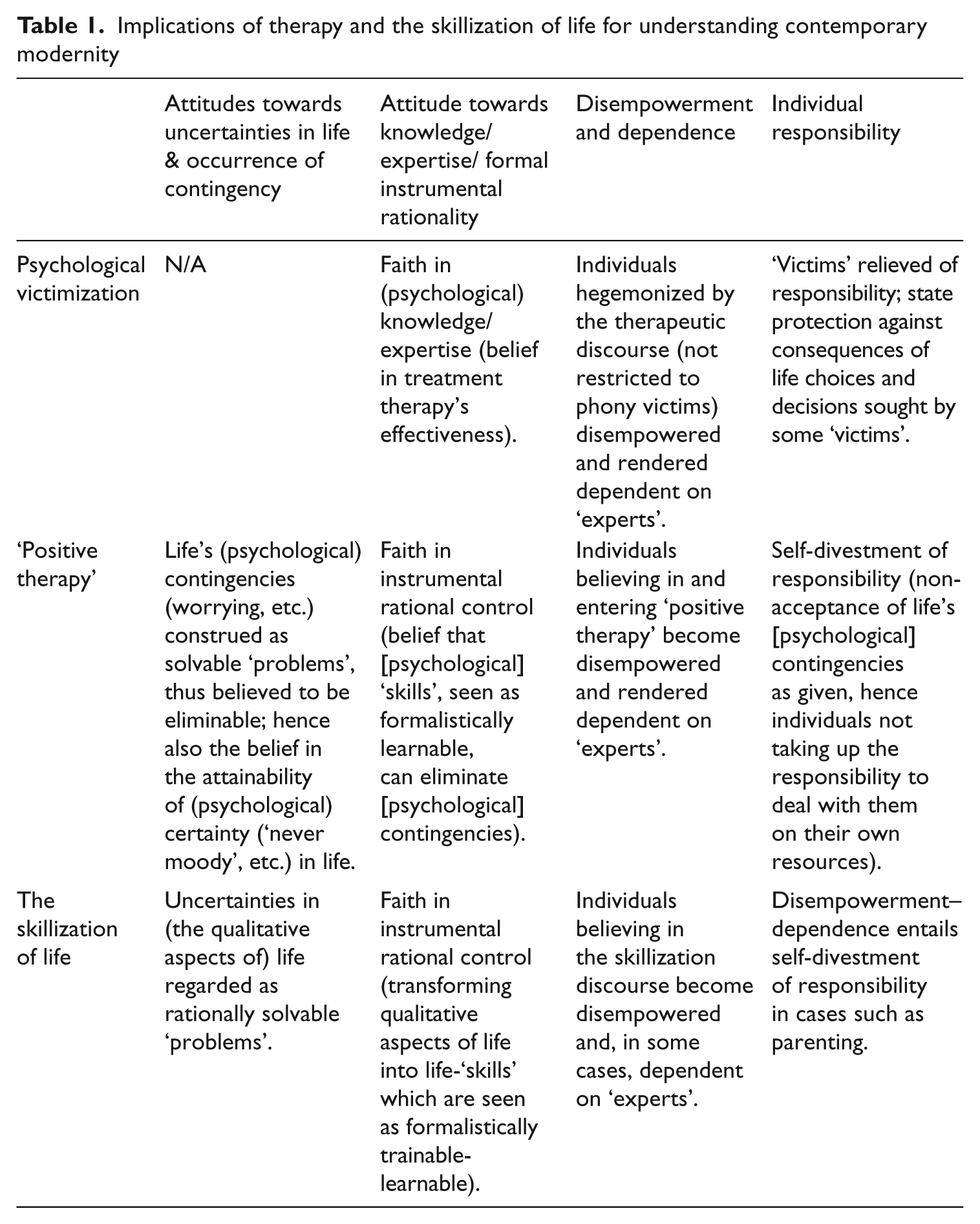
The implications of the trends of therapy and the skillization of life for understanding contemporary modernity are summarized in Table 1.
The modernist mentality remains entrenched today in its faiths in the attainability of complete control in life (first column), and in knowledge/expertise and formal instrumental rationality which are seen as capable of assuring complete control (second column). From this angle, we examine the analyses of contemporary modernity of Giddens, Beck and Bauman.
Implications of therapy and the skillization of life for understanding contemporary modernity
In Giddens’ view, 17 late-modernity is populated by late-moderns possessing heightened reflexivity. Late-moderns are enlightened individuals who (consequent upon the failure of social engineering and burgeoning environmental degradation) are aware that in late-modernity there is no certainty, that no knowledge is able to produce certainty, and that rational ordering of social and natural environments have proven to be unattainable. There is, in other words, widespread awareness of the limits of expertise, and the belief that much that goes on in life and society is open to contingency and beyond rational instrumental control. Radical doubt now filters into most aspects of daily life and risk awareness seeps into the actions of almost everyone. Accepting risk (which arises from uncertainty) as risk is an orientation that is more or less forced on late-moderns. The conclusions drawn in our analysis are hence contrary to Giddens’ view.
Giddens states that while casting radical doubt on knowledge/expertise, few if any late-moderns could disengage from the entire system of expertise. For instance, a person having back pain not trusting physiotherapy might try acupuncture instead. Giddens terms this ‘transfer of faith’. Does choosing between different types of ‘positive therapy’ constitute an instance of ‘transfer of faith’? It should be noted that for Giddens, doing so, as is ‘transfer of faith’ in general, constitutes a reflexive choice (evaluating competing expertise) of risk-taking (the chosen therapy might fail). However, contrary to Giddens, the majority of ‘positive therapy’ users, instead of taking risk in choosing a particular therapy, actually belief that risk (psychological contingencies) is categorically eliminable. Moreover, as Zilbergeld (1983: 119–20) shows, for reasons such as reducing cognitive dissonance, many users, instead of reflexively reflecting on what they got from a therapy which has failed, refuse to admit that it has.
In Beck’s view, up until the 1960s, ‘science could count on an uncontroversial public that believed in science but today its efforts and progress are followed with mistrust’ as a result of the unintended risks (hazards) produced by industrial society (1992: 169). Facing these risks: ‘will the new manufactured incalculability and disorder be opposed according to the pattern of instrumental rational control, that is by recourse to the old offerings of industrial society . . . ? Or is a rethinking and a new way of acting beginning here, which accepts and affirms the ambivalence [emphasis added] . . . one could call . . . the latter reflexive’ (1994: 11–12). In other words, for Beck, in today’s ‘reflexive modernization’, reflexivity in this respect means the acceptance of uncertainty (‘ambivalence’) as given (‘affirms’) and the recognition of the limits (‘rethinking’) of instrumental rational control. It is worth noting what Beck exactly refers to by science: ‘With reflexive modernization, public risk consciousness and risk conflicts will lead to forms of scientization of the protest against science . . . the critique is supported scientifically’ (1992: 161). Thus, science that departs from the precautionary principle is not mistrusted but embraced; the science being mistrusted is science that believes in instrumental rational control. Again, Beck’s theses are at odds with our conclusions.
The same applies to Bauman, who argues that with modernity’s transformation into liquid modernity, contemporary agents accept as given that they ‘are bound to [emphasis added] live with contingency (aware of contingency, face to face with contingency)’ (1991: 16). Abandoning the modernist illusions of ‘a state of complete control . . . free from contingency’, this contemporary acceptance of contingency constitutes ‘the exact opposite of what Max Weber anticipated . . . the impending triumph of “instrumental rationality” . . . perfecting the means’ (2000: 59; 2001: 104).
Returning to Table 1, fourth column, there is a general retreat of individual responsibility today concerning the consequences of life choices and decisions and the handling of life’s contingencies. State protection against such consequences is sometimes sought by ‘victims’. Contrarily, Giddens, Beck and Bauman all argue that contemporary modernity is characterized by individuals actively assuming responsibility for their own life choices and decisions, and facing the risks/consequences accordingly.
For Giddens, ‘The self today is for everyone a reflexive project’; ‘The self is seen as a reflexive project, for which the individual is responsible. . . . We are not what we are, but what we make of ourselves’ (1992: 30; 1991: 75); the construction of self (life-style) is open-ended because ‘an indefinite range of potential courses of action (with their attendant risks) is at any given moment open’ (1991: 28–9). In a word, late-moderns assume the responsibilities and risks of how they make of themselves. Beck (1992: 88, 90, 131) similarly argues: ‘These surges of individualization . . . class biographies, which are somehow ascribed, become transformed into reflexive biographies which depend on the decisions of the actor . . . one has to choose and change one’s social identity as well and take the risks [implying bearing the responsibility] in doing so’. In Bauman’s view, enjoying new individual freedoms, liquid-moderns have come to believe in the rightness of the ‘privatization of ambivalence’. In other words, they accept that the new freedoms come with new responsibility, and seek individualized solution to social contradictions (2001: 47, 70, 88). ‘Under the postmodern condition grievances translate into self-reflexivity of the agents . . . the resumption by agents of moral responsibility . . . autonomy turns into the defining trait of postmodern agents’ (1992: 197, 202).
In Giddens’, Beck’s and Bauman’s theses, contemporary individuals exercise reflexive and autonomous agency. However, our analysis (Table 1, third column) shows that large numbers of individuals (phony victims; non-phony victims who are nevertheless hegemonized by the therapeutic discourse; individuals believing in the ‘positive therapy’ and skillization discourses) are disempowered and rendered dependent on ‘experts’.
We think Giddens’, Beck’s and Bauman’s theses do apply to certain contemporary trends. However, the trends analysed here and their implications are at least as significant, if not more so. Instead of a population of individuals casting reflexive doubt on rationality, large numbers of individuals harbour ungrounded faith in rationality and instrumental control. Instead of a population of individuals exercising reflexive and autonomous agency and assuming self-responsibility, large numbers are disempowered, rendered dependent and divested of responsibility. We have commented on the varying degrees to which our various arguments possess empirical support (some better grounded, some more provisional), as well as suggested ways in which more systematic evidence can be acquired. Scholars such as Furedi, along with numerous social and cultural critics both in America and Britain, are especially concerned about the diminution of agency. Ecclestone and Hayes worry that therapeutic education may produce entire generations of diminished agents; such worries need to be substantiated by systematic evidence to become more convincing, in both scholarly and policy-making terms.
Footnotes
Acknowledgements
I am grateful to the anonymous reviewers for their helpful comments; the usual caveat applies.
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.