
Abstract
The Australian health system requires novel strategies to implement widespread primary prevention to reduce the burden of chronic illness. One approach is for health sectors to draw on resources available in communities of place and to form partnerships which maximize the relevance and uptake of initiatives designed to promote healthy lifestyles. This article presents a typology of conceptual approaches to community and health sector partnerships, developed through an extensive literature search and empirically tested using in-depth case studies across regional Australia. The article finds that the health sector’s orientation to primary prevention is generally instrumental involving highly targeted outcomes and pre-defined programmes. Communities of place have multifaceted priorities that include building the social and economic sustainability of their community. While these approaches might appear incompatible, careful ‘manipulation’ and ‘massaging’ of instrumental objectives to adjust to community agendas and the presence of ‘boundary crossers’ can lead to successful primary prevention outcomes.
Introduction
A large proportion of the associated premature mortality and much of the morbidity of chronic illness is thought to be preventable (National Health Priority Action Council, 2006). In light of this Australia’s healthcare system has highlighted primary healthcare and prevention in its current reform agenda (Commonwealth of Australia, 2009). In Australia, as in many other resource-rich countries, the health system transformations involved in the reorientation from acute care to primary prevention and health promotion are multifaceted and difficult. The increasing complexity of acute care results in strategic objectives focused on balancing demands for cost containment with quality improvement rather than primary prevention. Furthermore, the social determinants of health, such as the societal processes that determine social class and act as risk factors for chronic illness, exist outside the health system (Minkler, 2005; Syme, 2004; WHO, 2010); the system, even with the best of intentions, has limited capability to respond.
In an attempt to overcome this problem, the most widely used public health strategy to promote participation in public health is for health systems to form partnerships with the community to jointly run preventative initiatives (Butterfoss et al., 2003). There is an increasing international literature about the role of non-government organizations (NGOs) in the reform of health systems (Owen and Kearns, 2006). This article adds research evidence about ‘communities of place’ working in partnership with the health sector. Using community interaction theory, a community of place can be understood in a sociological sense as a locality with more or less commonly agreed upon geographic boundaries and a local society in which people interact in order to meet social and business needs (Wilkinson, 1991).
While there are no universally agreed upon definitions, a partnership, collaboration or coalition can be understood as joint action to achieve mutually agreed upon goals. In public health, for example, the term ‘community coalition’ is used to describe an organization of diverse interest groups that combine their material and human resources to effect a specific change that members are unable to achieve independently. Partnerships between the health sector and communities are notoriously difficult to achieve. The body of work on factors that facilitate and inhibit community and health sector partnerships acknowledges that there is no ‘best way’ to implement partnerships and no one way of evaluating success (Butterfoss, 2006; El Ansari and Phillips, 2001; Israel et al., 1998; Lasker and Weiss, 2003; Roussos and Fawcett, 2000; Wandersman et al., 2005). In a review of published papers from 1980 to 2004 on relationships among coalition-building factors and indicators of coalition effectiveness, Zakocs and Edwards (2006) found that the factors associated with effective coalitions in resource-rich nations are unclear. This lack of evidence about the factors that might impede or facilitate community and health sector partnerships for primary prevention of chronic illness was the basis for the study reported upon in this article.
The study aimed to explore the types of partnerships formed between communities of place and the health sector and the motivations for them. It also examined the different perspectives brought by communities and the health sector and how perspectives changed over time. We present a typology of conceptual approaches and categorize partnerships, using the typology, in eight Australian case studies. Using empirical data, we describe the dominant themes in each of the partnership types and the instances of competing approaches and build concepts about how these approaches are aligned.
A typology of community and health sector partnership approaches
The typology of partnership approaches was synthesized from conceptual material about community participation in health activities including writing by Bracht and Tsouros (1990), Hildebrandt (1994), Laverack (2003), Laverack and Labonte (2000), Minkler (2005), Oakley (1989), Preston et al. (2010), Rifkin (1986, 1996, 2001), Rifkin et al. (2000), Taylor et al. (2006) and Williams and Labonte (2003) as well as seminal material about community participation generally, such as Arnstein (1969) and Midgley (1986).
The typology defines four approaches to community and health sector partnerships in communities of place: the ‘contributions’, ‘instrumental’, ‘empowerment’ and ‘developmental’ approaches. These approaches often overlap, and change over time, but generally there is an overriding approach. The contributions approach occurs when people and organizations in a community contribute by time, expertise, funds or community-based knowledge to a project voluntarily. This occurs without any involvement in decision-making about how the contributions will be used or about the overall direction of the project. The contributor or the instigator may not have a concept of ‘partnership’ (Oakley, 1989). In chronic illness prevention, for example, this would entail health professionals using volunteers to distribute information about the initiative to ensure that target groups are informed. Volunteers would not contribute to decision-making about the project.
An instrumental approach conceives of the partnership as a means to achieve health outcomes – or illness prevention – in line with a health sector strategic direction. Involvement of people in the community is seen primarily as a way to maximize community involvement in the activities and potentially community ownership. The interventions or programmes are predetermined according to the priorities of the health sector with only limited ability to incorporate community priorities (Rifkin, 1996). The empowerment approach, common in the health promotion literature, conceives of the partnership as a means to achieve a greater knowledge and capacity for people to take control over issues that affect individual and community health and well-being (Laverack and Labonte, 2000). There is an explicit transfer of information, knowledge and power generally from health professionals to community members. Health professionals may call this process ‘capacity building’ in individuals and communities. The developmental approach in a partnership evolves where members see the partnership as a means to achieve both specific and broad health and well-being outcomes for a community of place and address the social determinants of health (Laverack, 2003). All partners have a role in decision-making and knowledge and power transfer might occur. Collective advocacy for actions to improve health is usually involved.
Research design
The typology was tested through a prospective multiple site, embedded, case study design. Eight case studies were chosen in regional communities of place in two Australian states, South Australia and Queensland. It was thought that including cases from different states might enhance the possibility of transferring findings to other regional locations. Most of the case study sites had populations of between 10,000 and 20,000 people and most had high levels of relative social disadvantage using the Australian Socio-Economic Index for Areas (SEIFA) scores (ABS, 2006).The SEIFA is an index designed to enable comparison of the economic and social well-being of communities. Regional Australian service centres outside capital cities were chosen because they usually exhibit phenomena more clearly than in urban neighbourhoods where there are multiple levels of interactions with many systems both within and external to the community.
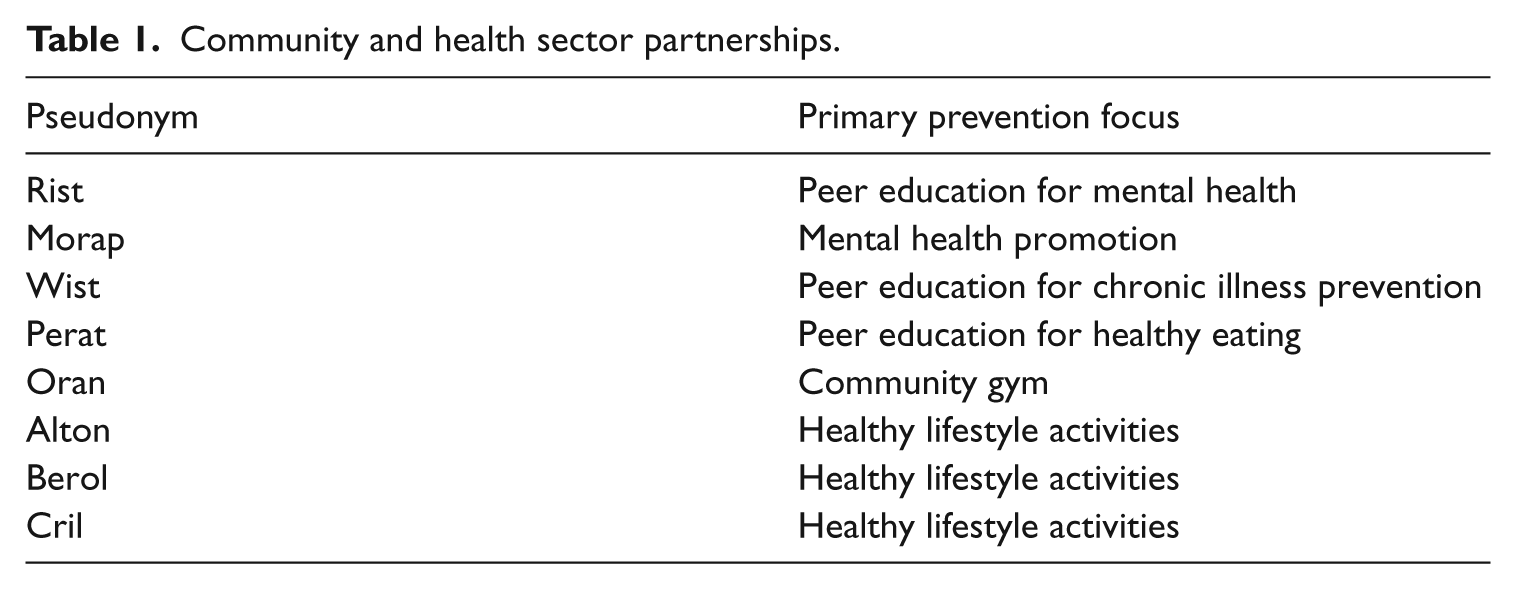
A ‘case’ was defined as a partnership between a community-based NGO, volunteers and/or citizens, and paid public or private health sector employees in a community of place The case included all those people knowledgeable about the partnership structures, processes, activities and outcomes at all stages of the life of the partnership. In each region expert panels were constructed composed of regional health, local government and community members, familiar with partnerships in the region. These panels identified potential cases. Purposive sampling, through a web-based search of partnerships, supplemented the expert panel’s suggestions. Eligibility criteria included current involvement in activities to prevent chronic illness, health sector and community members involved, and being located in a regional town (see Table 1). Ethics approval was obtained from four university and health department human research ethics committees.
Community and health sector partnerships.
Three sources of data – semi-structured interviews, non-participant observations and document reviews – were collected by one researcher during field trips between 2008 and 2010. Eighty-six interviews exploring partnership objectives and outcomes, motivations for involvement and partnership processes were conducted. Interviews were audio-recorded, transcribed, and a summary report about the partnership was returned to partners. One researcher, as a non-participant, observed partners’ interactions at partnership meetings, NGO board meetings and activities where primary prevention occurred. There were eight observations of partnership or board meetings and 15 observations of partnership activities. Documentation about the partnership such as annual reports, information flyers, evaluations, meeting minutes, strategic plans and press releases were also reviewed.
Analysis was conducted both within cases and across cases in accordance with established techniques (Miles and Huberman, 1994). Data were entered into NVIVO (a software programme marketed by QSR International for the coding of qualitative data), creating a project for each case. An analysis of the three sources of data (interviews, observation and document analysis) about partnership objectives and motivations resulted in preliminary categorization of the partnership type. The type was categorized for both the health sector and communities at the commencement of the partnership and at the time when data were collected. The overall partnership type was derived by three of the authors reading node reports from NVIVO and each making an independent judgement. There was a lack of consensus about the categorization of one partnership and further analysis of data and discussion occurred. Across cases analysis was undertaken to systematically examine the themes emanating in the instrumental, empowerment and developmental partnership types. There was no contributions type partnership. Themes were developed about each partnership type and how different approaches were aligned.
One researcher conducted all of the interviews and document analysis and also made the observations. The potential for interviewer bias was dealt with by consistent debriefing with the research team. The investigation used purposive sampling of partnerships which differed from each other and therefore extensive claims about the transferability of findings cannot be made. However, the partnership typology was able to be applied in all cases in spite of these variations and in the developmental and empowerment partnerships consistent themes emerged about how communities and the health sector aligned their objectives and made decisions designed to lead to effective primary prevention outcomes. ‘Reactivity’, as the influence of the researcher on the setting in the process of collecting information (Maxwell, 1998: 92), could not be eliminated in this research design. Partners often clarified their views about the partnership during the interview and made decisions to implement changes in theirs or their organization’s approach.
Conceptual approaches to communities and health sector partnerships
This section of the article presents empirical analysis of the conceptual approaches found in the partnerships and the themes that were apparent in the instrumental, empowerment and developmental type partnerships. It became apparent early on in the analysis that the health sector and the communities brought different perspectives to the partnership and that these perspectives changed over time. It was also clear that some partnership types coexisted, although there was no clear pattern to this. To ensure anonymity pseudonyms are used for cases study sites and quotations from participants are identified simply as ‘community’ or ‘health sector’.
Instrumental approach
In each of the eight partnerships the health sector, at some stage, used an instrumental approach to the partnership. The way the health sectors were structured, with clearly defined programmes emanating from state or national-level priorities, demanded this approach. There was one partnership where the instrumental approach dominated throughout the life of the partnership. The Rist partnership, initiated and managed by the health sector, had clearly defined strategies to meet the goals and objectives and limited community involvement. A structured peer education programme for young people to raise awareness about, and prevent, mental illness was provided through coursework and a residential camp. Components of the programme were provided by other agencies, for example the local police provided material about the risks of alcohol misuse. At the time of the study there were no formal partnership meetings and all decisions were made by a programme coordinator. The programme had been operating for a number of years and became consolidated through ongoing relationships.
The Morap partnership involved the development of a wellness centre, established through a health sector and community partnership. Both the health sector and the community members initially had a developmental approach in order to establish the centre as a place where people might make social connections, participate in activity programmes as well as specific mental health promotion programmes. The partnership had resulted in an NGO becoming incorporated and the NGO managed the centre. However, the governance model was resourced through the publicly funded community health sector. At the time of the case study there was a major state-level health sector reorganization and the centre was then funded and managed through the publicly funded mental health programme. Although the partnership had elements of a developmental partnership initially, a move to an instrumental approach occurred with a strong focus on the strategic directions of the mental health programme:
There is a change from the early days when the centre was set up with a wellness focus rather than an illness focus. It provided support to a lot of different people living here. It moved past the rhetoric of de-stigmatizing mental health to actually doing it. It might not have ‘made the books’ in mental health from the strategic perspective – but it is a very important place. Now I think we might focus on mental illness. (Health sector Morap)
The state health sector will always bring specific targets and objectives when they fund initiatives. In the case of primary prevention of chronic illness it may focus on risk factors, specific diseases and interventions (Syme, 2004). Therefore, in partnerships with communities of place a ‘top-down’ approach with the dominance of instrumental objectives and professional knowledge might be expected to prevail. Moreover, the health sector will generally operate within an ‘expert’ model and the structures and management systems evident within the sector contribute to the continuation of this model (Kruske et al., 2006).
In the Morap partnership it is likely that moves to comply with the strategic focus of the mental health programme might mean that the partnership will shift to more targeted programmes for those with mental illness rather than retain a preventative approach. The original approach of the partnership, initiated by community people, was to provide a ‘welcoming’, friendly and safe place where there would be opportunities for all to gain mutual support, information, education and connection with others. A flexible approach, meeting needs as they arise, stands in contrast to a structured programme and there is inevitably tension in bringing these approaches into alignment. Furthermore, the public mental health sector in this state is funded to provide services to those with serious mental illness and there is a limited focus on primary prevention.
Empowerment approaches
There were two partnerships, Perat and Wist in South Australia, which had predominantly empowerment approaches. The Wist partnership was initiated by a university as part of a nationally funded chronic illness management project with the aim to create an incorporated community group to conduct peer education for the prevention and management of chronic illness. The university initiator of the partnership had an explicit intention to give up or transfer power through helping the volunteer group become independent and make decisions:
I guess first and foremost my aims were really to set up a peer-led community group because we recognized that health professionals have very limited time and sometimes education – they tend to stick to their specialties. We recognized that there was so much more that community people could contribute rather than just completely rely on a health professional input. But it was a skills transfer as well. Then eventually I could step away so that this group of people could make decisions. (University Wist)
Fawcett et al. (1995: 679) have identified community empowerment in health promotion as ‘the process of gaining influence over conditions that matter to people who share neighborhoods, workplaces, experiences, or concerns’. Using Fawcett et al.’s categories, the empowerment in this partnership is at the individual and group level and the relationship is between an ‘empowering agent’ (the university) and ‘empowering recipients’ (community volunteers). As a community member acknowledged:
Well the change [in the direction of the partnership] started I think very quickly. Some of the consumers involved in the partnership were asked if they would like to attend a conference to provide community members with the knowledge and the concepts of what the project was about. I think that was the sort of turning point. We use the word ‘empower’ a lot, but I think all those that attended that conference came back feeling empowered consumers. We knew a lot more about consumerism in the health service than we sort of ever dreamed of. (Community Wist)
In the Wist partnership the empowerment was at both an individual and a group level and at the time of study, it had resulted in an incorporated NGO with up to 20 volunteer qualified trainers in chronic illness self-management and prevention. The volunteers recognized ways in which their lives had changed through involvement in the partnership:
I think that one of the things – the greatest thing and it’s perhaps what people have commented on most – is I went into the partnership lacking confidence and over the years I’ve grown in confidence. I can now confidently and comfortably talk to people. (Community Wist)
While the university initiator of the Wist partnership used an explicit empowerment approach, the locally based hospital and community health sector was not supportive and was not actively involved. Over time, the perspective of the health sector changed to recognize the potential benefits of having volunteers train in chronic illness prevention. Consequently, a new relationship opened up, consolidated by the NGO moving its activities into the hospital. The health sector brings an instrumental approach to the partnership and there are tensions in aligning the empowerment and instrumental approaches. However, community members feel sufficiently ‘empowered’ to maintain their own objectives and identity while being seen as part of the health system:
We are now an accepted part of the [health sector] but retaining our own identify is getting harder. We don’t want to be seen as just a part of it. We want to remain an independent part of it. We have to work on that quite hard. Some of our volunteers see us as just as –a part of the hospital. (Community Wist)
In the Perat partnership both the health sector and community volunteers shared an empowerment approach and this continued throughout the life of the partnership. The health sector recruited volunteers to be trained as peer educators to deliver ‘healthy eating’ messages in their communities. The programme was state-wide and had clear goals and objectives but these were flexibly implemented at the local level and in this way the partnership fell more into the empowerment than the instrumental type. The overall aim was to increase the knowledge and skills of volunteers so that they could provide community training programmes about healthy eating:
I really enjoy being involved. Just seeing the change in people from when they first come to the training to the end is just incredible; especially, because most of them were unemployed and to see them at the end was just really good. (Health sector Perat)
Community capacity building was the term used by the local community health sector; this involved providing support and training to volunteers, building their self-esteem and reaching a broader audience through the volunteers:
I guess from the way I see it is very much a community engagement, community capacity building type programme. So, I guess we are increasing the skills of the actual volunteers, but then hopefully that will extend further into the community. The programme reaches audience that we wouldn’t. (Health sector Perat)
The most apparent theme in the empowerment partnerships was the changes in the lives of the volunteers who had learnt new skills, built self-esteem and had new opportunities. This was empowerment at an individual level first and in the Perat partnership the empowerment rested at this level. The volunteers thought it valuable to learn new skills that would assist them and their families and the community more broadly. They could acknowledge that they had more self-esteem and this affected their families:
Well, look I think it actually allows us to feel good about ourselves and our knowledge and I think we have a bit more pride in ourselves or self-esteem. I think we have a lot more connections in the community now and because we are involved in the healthy canteen stuff we meet more parents. And in the beginning I was too shy too – to do anything. But now, I have got more get up and go. I think it has helped with our kids as well. If we have self-esteem our kids will have self-esteem if they see it in us. (Community Perat)
Developmental approaches
The remaining four partnerships were predominantly of this type; Oran in South Australia, Alton, Cril and Berol in Queensland. The Oran partnership, of eight years, was a health sector initiated health promotion committee of which a subgroup had become incorporated and developed and managed a community gym. There had been one-off funding for gym equipment and in-kind support from the health sector and community organizations, but no ongoing funding. Cril and Alton were well-established funded NGOs with a mandate of community development and social care service delivery. With specific funding from the health sector, these NGOs had moved to include health promotion and primary healthcare access as they thought these components would add to the development of their communities. The services provided by these organizations included health lifestyle programmes and access to primary healthcare for outlying communities. The Berol partnership was eight years old and based in an NGO established through a partnership with the health sector, specifically for health promotion activities. A range of health-related activity programmes were provided including a ‘community champions’ programme focused on healthy eating and exercise and the organization worked in conjunction with local government and other agencies to implement healthy public policy.
The most apparent theme in these four partnerships was that the communities, and to some extent the health sector representatives, viewed health development as interrelated with the development of the community as a whole. This did not mean that primary prevention objectives were subsumed into overall community objectives, rather the former were contextualized in a community of place and the interrelationship of relevant health determinants was noted. People understood that enabling healthy lifestyles involved action to ensure access to employment, opportunities for activity and emotional well-being. This was particularly so in Oran, the smallest regional centre studied. This region had seen a decline in service provision, movement of young people away from the region to obtain employment and education and a serious drought. Residents, through the health promotion committee, were determined to keep the services they had and address the problems they faced:
We wanted to keep on the committee to get that feedback for the community. We are trying to act as a voice for the ordinary person as the mildest form of lobby group. The health promotion committee highlights what the problems are in our community and goes about, in a very subtle way, to address the problems, meeting needs or even pre-empting a need where we could see one was emerging. (Community Oran)
The aim of the community gym, established by the health promotion committee, was to ensure all residents had access to affordable exercise options including specific programmes for older residents. The broader objective was to enhance community sustainability:
I think it’s just a better place for the community to live in, and more opportunities to do the things that they want to do and also [through the community gym]. I think it leads to a healthier community with a better sense of well-being, in my opinion. (Community Oran)
In Cril there was an explicit intention to use the health promotion programmes to benefit the community as a whole:
I have always really admired the work they have done here [the NGO] with being passionate about the community and really fulfilling need in the community. Even though there are separate programmes under one umbrella we all do try to very much work together and cross over because what we had in mind is the outcomes for the community and the need in the community. We can add value to what other groups are already enjoying because physical activity and healthy eating benefits everybody. It also brings about that sense of community when we are all doing it together through different ventures. (Community Cril)
From a sociological perspective, expressing connection to community through collective social interactions is commonplace and the substance of community development. Collective action on behalf of a community, whether health or social development, validates the self as an active contributor while producing results that are seen to be in the communities’ interests (Wilkinson, 1991). Conceptually, the development of the community’s health and the broader community development are related themes (Minkler, 2005). For example, communities are often aware of the broad social determinants of health that operate in their community and they bring this awareness to the partnership. Most interviewees gave examples of how they saw the inseparable connections between well-being and community life. Here is an example of how a participant in the study saw this operating:
If you don’t network with one another, you can’t empathize with people. There was an example yesterday – there was a farmer reaping in a paddock and he had a gap between when the load needed to be taken away and his neighbour was reaping nearby. He thought ‘I am going to hop in the header [a piece of machinery to harvest wheat] with him.’ So he walked across to his paddock and spent an hour and a half sitting in the cab with him going around and around the paddock and they would have talked about the reaping, the weather, the kids – eventually got on to how he is coping [his wife had passed away]. (Community Oran)
Using existing theory about community participation in health it is apparent that these four partnerships are ‘ground-up’ expressing the commitment of communities to see positive health development (Rifkin, 1996; Roussos and Fawcett, 2000). However, the health sector representatives are not coming entirely from a ‘top-down’ perspective. The majority of health sector partners involved in developmental partnerships considered themselves in some ways as ‘part of the community’ and they contributed in a like manner to community well-being:
So basically we don’t sit apart as health – health is part of the community, so it didn’t matter what was on, we had a presence. And now we have the community’s trust. They come to us even for the funniest things and we’re pretty well part of every bun fight in town. (Health sector Berol)
Aligning partnership perspectives
In understanding effective partnership functioning, it is the conceptualizing of the integration of the approaches taken by communities and the health sector that is important. There are two important concepts emerging from this study.
The first involves aligning strategic health objectives with those of communities and the health sector ‘massaging’ or ‘manipulating’ their objectives to enable a ‘fit’ with those of communities.
The second concept is the presence of ‘boundary crossers’, who are part of and have the trust of both the health sector and community domains (Kilpatrick et al., 2009).
In the developmental partnerships a high level of skill was shown by the majority of health sector representatives, who could support the partnership outcomes required by the communities while also achieving health sector goals and objectives. They could incorporate and transcend the strategic agenda. One health sector representative referred to this as ‘massaging’ health sector objectives:
For us you always have goals or objectives that you have to meet for a programme. And often times when you are working with an NGO it doesn’t quite match their goals and objectives and their operandi. So you have to massage them so that they fit in with both; that you can meet your reporting requirements and the outcome objectives and they can fit in with their sort of way of working as well. (Health sector Berol)
This process of ‘massaging’ objectives involves careful negotiation of the goals and outcomes of the partnership which generally is achieved only through a long-term trusting relationship. Long-term partnerships between people are difficult from both the health sector and community perspectives. Health system objectives, programmes and funding change continually so the ability to focus on a particular partnership objective over time is limited. On the other hand, community agencies also change staff and objectives change to meet community emerging needs.
The Berol, Alton and Cril partnerships all demonstrated well-managed integration of objectives from both the health sector and the community partners. The community partners were well aware of their value to the health sector:
We also work along with the [health sector] initiatives so we’ve been able to facilitate their uptake much better in our local community. Because otherwise they probably just hit the desk and I’m not sure what would happen to them. We did a large focus for a long time over the Go for 2&5 Campaign [a programme designed to increase vegetable and fruit intake], lots with Smart Choices around – we had our tuck shops changing before Smart Choices came along so they were receptive to that. In terms of [health sector] initiatives we usually try and piggy back them and get more happening at our local level than normally would happen. (Community Berol)
Another way to bring potentially competing approaches into alignment is through the use of ‘boundary crossers’. A boundary crosser is someone who is a member of a community of place and is aware of the interests of that community as well as being an employee of the health sector (Kilpatrick et al., 2009). In Oran and Alton, health sector members of the partnerships were boundary crossers and they had the interests of their community, in addition to their professional role in mind:
The other thing from a personal point of view is I live here, I work here; this is my area, my community, so I have got a vested interest as a community member as well to be involved and I know others would share that same sentiment. (Health sector Oran)
The dual role of community member and health professional is one which enables the instrumental objectives of the health sector to be portrayed in such a way as to be relevant in a particular community of place. Like the massaging approach, this requires a high level of skill to be successful. However, even skilled boundary crossers hit difficulties when trying to implement unpopular health sector reforms. In addition, the closeness of interactions between professional and personal roles places health sector staff under the spotlight:
The work that your team does and that you do is under the spotlight from the community so if you put a foot wrong and you don’t involve the community in decisions and things like that you soon know about it. So there’s greater pressure. (Health sector Oran)
Conclusions
The outcomes of these partnerships between community-based NGOs and the state health sector were considerable. They included targeted exercise programmes for older adults at a community gym, the establishment of walking and exercise programmes with all age groups, vegetable growing projects, outdoor gyms and peer educators for the prevention and self-management of chronic illness. These are compelling reasons to promote community and health sector partnerships to contribute to the prevention of chronic illness and maintain a healthy community. However, at the local level, when beset by problems of maintaining a management committee, staff turnover and insecure and inadequate funding, it is easy to lose this bigger perspective. Consequently, local NGOs may benefit from connection to a larger regional or state-wide organization interested in health promotion, in order to support their efforts, advocate on their behalf and gain a voice in policy debates.
Better conceptualization of some of the competing priorities and approaches that are involved in partnerships between the health sector and communities or community-based NGOs may result in more explicit acknowledgement of both the benefits of partnerships and their challenges. The typology employed in this article provides a way to conceptualize approaches to partnerships and, although there are insufficient data to suggest that one type of partnership is more beneficial than another, concepts have been developed about how approaches are integrated in order for partners to achieve outcomes. Using this typology may assist in the negotiations that must inevitably occur when the health sector wishes to implement a managerial approach to achieve goals and communities want to develop and contribute to their community. It is not surprising that these two orientations may be in conflict. This finding, and the ways that approaches are aligned, adds to partnership theory.
Finally, partners, communities and NGOs as well as the health sector must be able to substantiate and measure the benefits of these partnerships both specifically in relation to partnership outcomes and more broadly in addressing the social determinants of health. Analysing the access and uptake of primary prevention activities and the ways in which these factors may ameliorate health inequalities may be one approach to this. NGOs and communities need to substantiate the benefits of these partnerships in order to claim a legitimate place in the Australian primary healthcare system.
Footnotes
Acknowledgements
The contributions of the communities and organizations involved in this study are acknowledged. Judy Taylor receives a Primary Health Care Research Fellowship from the Australian Government Department of Health and Ageing.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.